Paeds · genetics-dysmorphology-and-metabolism
Ethical issues in genomic diagnosis and cascade testing
Also known as Ethics of paediatric genomic testing · Predictive and cascade genetic testing in minors · Secondary findings and the right not to know · Consent and disclosure in genomic medicine · The child's right to an open future
A fellowship approach to the ethics of genomic diagnosis and cascade testing in children: apply the AAP, ACMG, and ASHG framework that governs consent, predictive testing, secondary findings, and disclosure; defer predictive testing for adult-onset disease and carrier status to preserve the child's right to an open future; manage the ACMG secondary-findings list with genuine opt-in consent; and coordinate cascade testing of at-risk relatives while respecting confidentiality and the right not to know — because the genomic result belongs to the child, the family, and the future adult the child will become.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The mark goes to the candidate who separates four conversations that parents, and sometimes clinicians, collapse into one. The first is diagnostic testing of a sick child, where the ethical balance favours testing because the result changes management now. The second is predictive or carrier testing of a healthy child, where the balance usually favours waiting, because the child gains nothing in childhood and loses the right to decide as an adult. The third is the secondary finding, an actionable variant unrelated to the reason for testing that is returned only if the family opted in. The fourth is cascade testing, the obligation and the mechanism for offering testing to at-risk relatives once a pathogenic variant is confirmed in the proband. The candidate who can name which of the four is on the table, and apply the right rule, will pass this topic. [1] [2]
Overview & Definition
Ethical issues in genomic diagnosis and cascade testing arise whenever sequencing a child produces information that affects more than one person, more than one point in time, or more than one health decision. A genomic result travels in three directions at once: it informs the child's own care today, it predicts disease in the future adult the child will become, and it implicates parents, siblings, and relatives who share the variant. Each direction carries its own ethical weight, and the clinician must weigh them explicitly rather than default to "test everything and report everything." [1] [3]
The 2015 ASHG and ACMG "Points to Consider" statement, led by Botkin, is the current consensus framework for paediatric genetic testing. It updates the original 1995 ASHG/ACMG document and sits alongside the joint AAP and ACMG policy statement and technical report from 2013. Together these documents establish that parents may consent to testing that benefits the child, but that they should generally defer testing whose only value is adult — whether that is knowing one will develop an adult-onset disease, or knowing one is a carrier for a recessive condition. The guiding concept is the child's right to an open future: keep the child's options open until the child can make the decision personally. [1] [2]
Cascade testing is the structured process of offering testing to at-risk relatives once a pathogenic variant is confirmed in the proband. It is one of the highest-value interventions in clinical genetics, because identifying an affected or carrier relative before symptoms appear can enable surveillance, prevention, or reproductive planning. But cascade testing collides with confidentiality — the proband's identity cannot be shared with relatives without consent — and with the right not to know, because some relatives do not wish to learn their status. The clinician's job is to offer cascade testing, document the proband's consent, and respect each relative's choice. [3] [4]
Classification
The classification that unlocks this topic sorts genetic tests by the ethical demand they place on the clinician and the family. The decisive questions are who is giving consent, whether the child should be tested now or the test should wait, and whether the result changes care today or only in a future adult. The same laboratory technology — exome or genome sequencing — can fall into any class depending on why it is ordered. [1] [3]
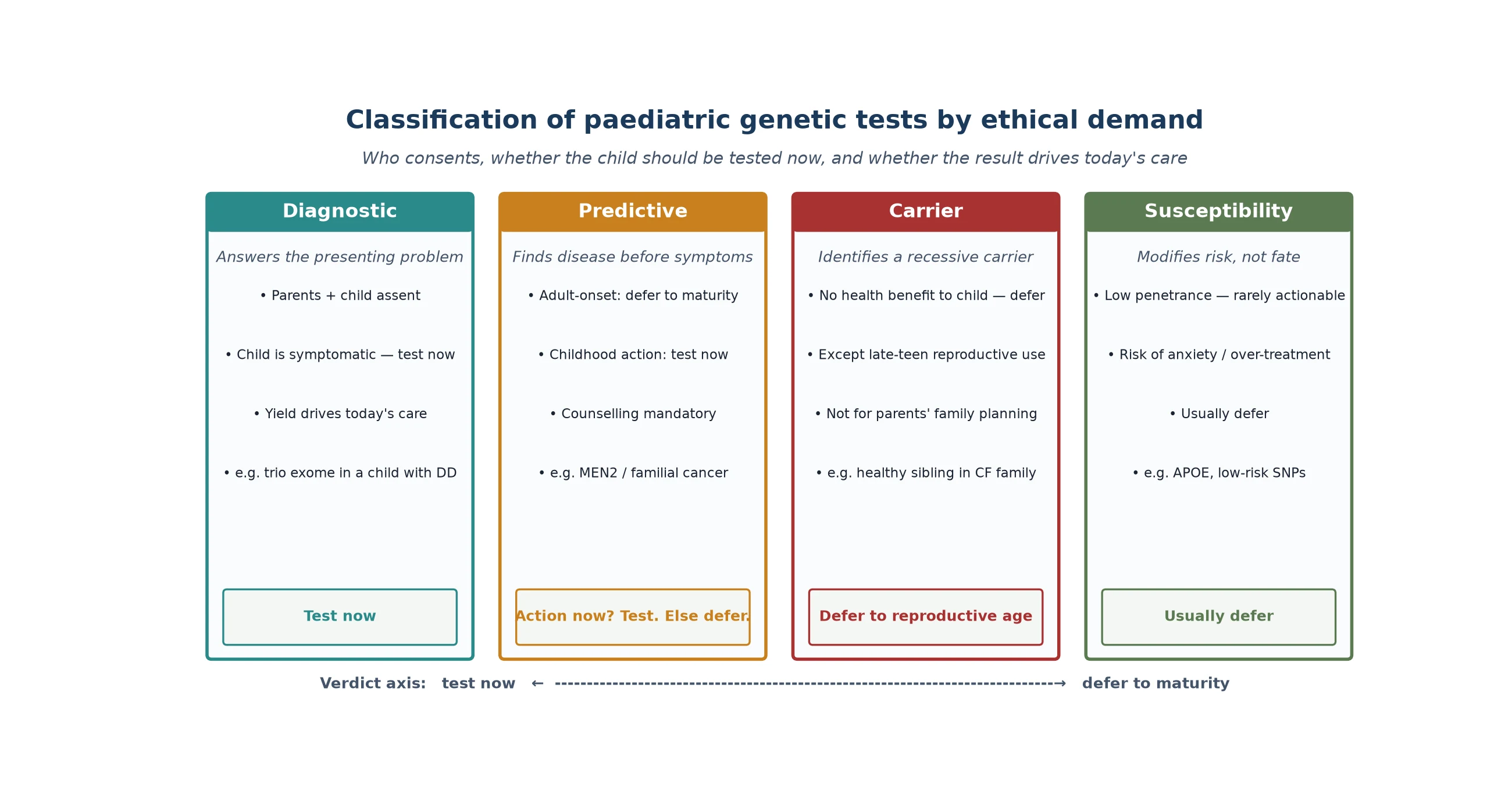
Diagnostic testing is ordered because the child has symptoms, and the result answers the clinical question driving today's management. Parents consent, the assenting child is included where able, and the balance falls clearly toward testing because the child stands to benefit. Predictive or presymptomatic testing is ordered for a child who is well but carries a familial variant; the ethical verdict turns on whether action in childhood changes outcome. Testing for multiple endocrine neoplasia type 2, where prophylactic thyroidectomy in early childhood prevents medullary thyroid cancer, is justified, because the benefit is immediate. Testing for Huntington disease or hereditary breast and ovarian cancer is not, because no childhood intervention changes outcome and the child loses the right to decide as an adult. [1] [4]
Carrier testing identifies a healthy child as a heterozygous carrier of a recessive or X-linked condition. It offers no health benefit to the child in childhood; its value is reproductive, and that value arrives at reproductive age. Consensus is to defer carrier testing unless a young person faces an immediate reproductive decision. Susceptibility testing for low-penetrance, common variants is almost never appropriate in children, because the risk information does not drive action and carries a real chance of anxiety, stigma, or over-treatment. [2] [3]
Epidemiology & Risk Factors
The scale of the ethical problem has grown with the reach of sequencing. As exome and genome sequencing have moved from research to first- and second-tier clinical tests, the number of children receiving a result with ethical weight — a secondary finding, a variant of uncertain significance, or a familial variant that implicates relatives — has risen in parallel. The diagnostic yield of genome sequencing in rare paediatric disease now reaches 40 to 50 percent, and each diagnostic result generates an obligation to consider cascade testing of the wider family. [6] [7]
The prevalence of medically actionable secondary findings is roughly 1 to 3 percent of adults and children undergoing exome or genome sequencing for any indication. That means in a service sequencing even a few hundred children a year, a small but real number will carry an actionable variant in a gene such as one of the hereditary cancer or cardiomyopathy genes on the ACMG SF list. These findings are only returned because a clinician looked for them, and only with prior consent. [5] [8]
The risk factors for an ethically charged encounter are the contexts in which the four domains collide. A critically ill infant in the NICU raises rapid-sequencing consent under time pressure. A family with a known adult-onset variant raises the predictive-testing question for the healthy sibling. A child of a donor or adoptive conception raises incomplete family history and identity questions. A family from a population under-represented in variant databases raises the risk that a rare variant is falsely called pathogenic. Each of these is common in tertiary paediatric genetics, and each demands a deliberate ethical conversation rather than a reflex test order. [1] [9]
Pathophysiology
The "mechanism" of this topic is not cellular; it is the structure of ethical reasoning that converts a clinical scenario into a defensible decision. Four principles from biomedical ethics — respect for autonomy, beneficence, non-maleficence, and justice — compete in every genomic result, and over them sits a fifth, paediatric-specific principle: the child's right to an open future. The clinician's task is to name which principles are in tension and resolve them in favour of the child's best interests. [1] [4]
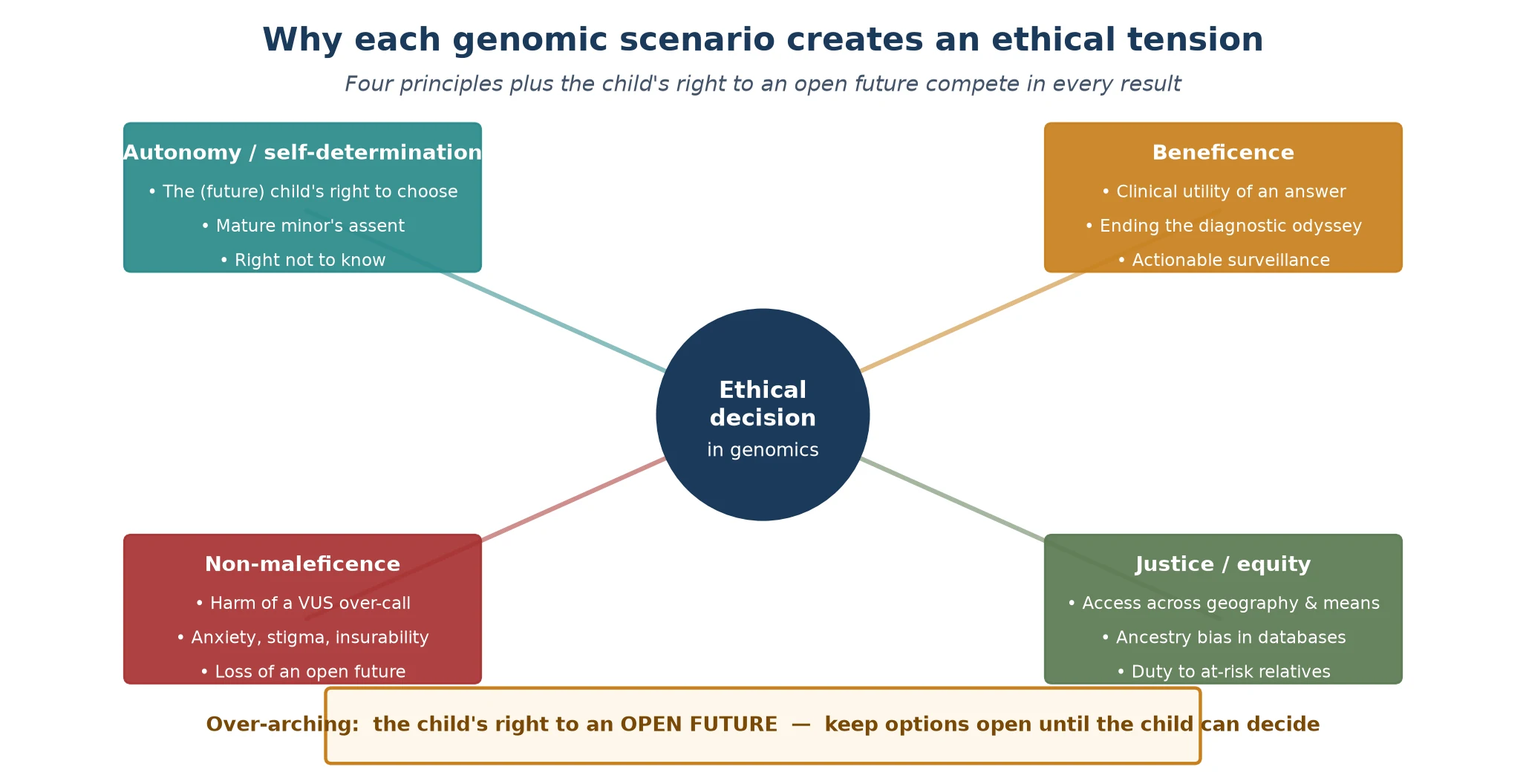
Respect for autonomy is complicated in paediatrics because the child cannot yet exercise it. Parents act as proxy, but their authority is not unlimited; it is bounded by the child's present and future interests. A mature adolescent's assent carries real weight, and an older adolescent may have the capacity to consent or refuse on their own behalf. Beneficence pulls toward testing when the result changes management now. Non-maleficence pulls against testing when the likely harms — anxiety, stigma, loss of insurability, foreclosing the future — outweigh the benefit. Justice asks whether access to testing and to the benefits of a diagnosis is distributed fairly, and whether ancestry bias in variant databases produces unequal harm. [1] [2]
The right to an open future, articulated by Ross and embedded in the ASHG/ACMG points-to-consider framework, resolves many of these tensions. It holds that a child has a right to make certain consequential decisions — whether to know a late-onset diagnosis, whether to learn carrier status, whether to share genetic information — for themselves when they reach maturity. Testing in childhood that serves no childhood purpose takes that decision away from the future adult, and that is a harm even when the parents would prefer to know now. [1] [4]
Clinical Presentation
The ethical scenarios "present" in clinic not as abstract dilemmas but as concrete family conversations. The candidate should recognise the recognisable clinical situations that each carry a distinct ethical demand, because the management follows directly from the situation that is on the table. [2] [3]
The diagnostic-odyssey child is the commonest: a child with unexplained developmental delay, intellectual disability, autism with dysmorphism, or multiple congenital anomalies, whose family has spent years without an answer. Here the ethics favour testing — microarray, then exome or genome sequencing — because a diagnosis can end the odyssey, direct surveillance and treatment, inform reproductive planning, and connect the family to a community. The ethical work is in pre-test counselling: explaining yield, the chance of a variant of uncertain significance, the option of secondary findings, and data sharing. [6] [9]
The known-variant family presents when a parent or sibling carries a confirmed pathogenic variant and the question is whether to test the healthy child. If the condition is adult-onset with no childhood action, the answer is to defer. If the condition has a childhood intervention that changes outcome — prophylactic thyroidectomy in MEN2, surveillance in familial adenomatous polyposis — the answer is to test. The candidate must know which familial conditions fall on which side of that line. [1] [4]
The incidental or secondary finding presents when the laboratory reports an actionable variant unrelated to the indication. The Green 2013 ACMG recommendations established a list of genes for which findings should be offered, and the policy has been refined through the Kalia 2017 v2.0 update (which made the list opt-out rather than mandatory) and the Miller 2021 v3.0 list. The clinical question is whether the family consented to receive these findings, and the answer determines whether and how the finding is returned. [5] [6] [7]
Differential Diagnosis
The "differential" here is the set of distinct ethical judgements a candidate must distinguish, because they look similar but demand opposite actions. Conflating them is the source of most errors and most lost marks. [1] [3]
The first distinction is between a pathogenic variant that warrants action and a variant of uncertain significance that does not. A pathogenic or likely pathogenic finding in a gene matching the phenotype drives management and cascade testing. A VUS, by definition, carries insufficient evidence to call either way, and acting on it — surveillance, prophylactic intervention, family testing — is an error. The VUS prompts further investigation (segregation testing, functional studies) and periodic re-analysis, never treatment. [1] [9]
The second distinction is between a diagnostic finding and a secondary finding. A diagnostic finding answers the clinical question and is returned as part of the diagnostic result. A secondary finding is unrelated to the indication and is returned only under the ACMG SF framework with prior consent. The two travel different consent pathways and carry different obligations, and confusing them leads either to over-disclosure (returning a secondary finding without consent) or under-disclosure (failing to return an actionable diagnostic result). [5] [7]
The third distinction is between a familial variant that is actionable in childhood and one that is not. This distinction governs predictive testing. A child at risk of MEN2 benefits from testing now because prophylactic thyroidectomy in early childhood is life-saving. A child at risk of Huntington disease gains nothing from testing now, because no childhood intervention changes outcome. The candidate must place each familial condition on the correct side of this line. [1] [4]
Clinical & Bedside Assessment
The ethical bedside assessment is a structured conversation, not a checklist of tests. It establishes what the family understands, what they value, and what they want to know, and it converts those into a documented consent and a defensible testing plan. The candidate who can run this conversation — in a viva, a DCE, or a communication station — demonstrates the ethical competence the examiners are testing. [2] [9]
Begin with the family's understanding and health literacy. What do they already know about the condition, the test, and the possible results? What have they been told by others, and what do they fear? Use plain language, check understanding by asking the family to repeat back the key points, and bring in a trained interpreter for any family whose preferred language is not English — family members are not appropriate interpreters for a consent conversation. [2] [3]
Move to the values and preferences that shape the decision. Does the family want to know everything the test can find, including secondary findings and uncertain variants, or do they want only the answer to the clinical question? Some families want maximal information; others find uncertainty and unsolicited findings burdensome. There is no correct answer, and the clinician's role is to elicit the family's view and honour it. Document the secondary-findings decision (opt-in, opt-out, or deferral) explicitly, because it will determine what happens when results return. [5] [6]
Close with the implications for the wider family and the future. Explain that a confirmed pathogenic variant may have implications for parents, siblings, and relatives; discuss how cascade testing is offered and how the proband's confidentiality is protected when relatives are contacted; and address insurance, employment, and reproductive implications with reference to the legislative protections that apply in the family's jurisdiction. A family that leaves the room understanding the result, the uncertainty, the family implications, and the right to decline has been properly consented. [1] [3]
Investigations
The "investigation" of an ethical question is the consent process itself, supported by the documents and conversations that make a testing decision defensible. Done well, it produces a record that withstands scrutiny; done poorly, it produces an actionable result with no agreed pathway for disclosure. [2] [9]
The pre-test consent conversation must cover the realistic diagnostic yield of the planned test, the possibility of a non-diagnostic result, the possibility of a variant of uncertain significance, and the option of secondary findings under the ACMG SF list. It must address what will happen to the data and the sample — storage, sharing with databases, and future re-analysis — and it must document the family's decisions on each. The genetic counsellor is central to this conversation, and the general paediatrician should view the documented consent as a clinical investigation in its own right: ordered, recorded, and reviewed before any result is disclosed. [5] [9]
What the consent record must contain before a result returns
A defensible pre-test record documents: the test ordered and the clinical question it answers; the discussion of diagnostic yield and the possibility of a non-diagnostic result; the discussion of variants of uncertain significance and the plan to investigate and re-analyse rather than act on them; the opt-in or opt-out decision for ACMG SF secondary findings; consent for data sharing and sample storage; and a plan for how and when results will be disclosed. Without these, an actionable or uncertain result arrives with no agreed pathway — the most common failure mode in genomic ethics.
[5][7]When a result returns, the investigation continues into the result itself. A pathogenic finding is confirmed against the phenotype, the inheritance is established by testing parents, and the cascade-testing plan is set. A variant of uncertain significance is reviewed for reclassification potential — parental testing to establish phase and de novo status, functional data where available, and segregation in the extended family. A secondary finding is disclosed only if the family consented, with disease-specific counselling and a management plan. Each of these is an investigative step that converts a laboratory call into a clinical action. [1] [7]
Management — Resuscitation
The resuscitation-context ethics arise in the critically ill infant in the NICU or PICU with a suspected but undiagnosed genetic disorder, where rapid trio genome sequencing can deliver a result in 7 to 14 days and directly change acute management. Here the usual deliberative pace of consent is compressed, and the clinician must balance the urgency of the clinical question against the integrity of the consent process. [10]
The intersociety policy on whole-exome sequencing in the critically ill newborn establishes that rapid sequencing is ethically justified in this setting because the diagnostic yield is high and the result can change acute decisions — guiding surgery, transplantation, escalation or withdrawal of intensive care, and palliative planning. The consent is conducted under time pressure but is not waived: the family is informed of the purpose, the rapid timeline, the possibility of secondary findings (usually deferred to a later, less pressured conversation), and the option of a result that may inform end-of-life decisions. [10]
The genetic counsellor plays a central role in supporting the family before, during, and after disclosure, because the disclosure of a life-limiting diagnosis to a family in crisis is one of the hardest conversations in paediatrics. The result must be communicated with clarity, empathy, and a concrete plan — whether that plan is disease-specific treatment, withdrawal of intensive care, or palliation. A rapid result that excludes a genetic diagnosis is also valuable, because it can redirect the investigation and reduce the harm of undirected testing. [10]
Management — Definitive & Stepwise
The definitive ethical framework runs as a five-step pathway that a candidate can recite and a general paediatrician can coordinate: counsel and consent before testing, order the right test, disclose the result in context, coordinate cascade testing, and plan re-analysis and re-contact. Each step has a specific ethical deliverable. [1] [2]
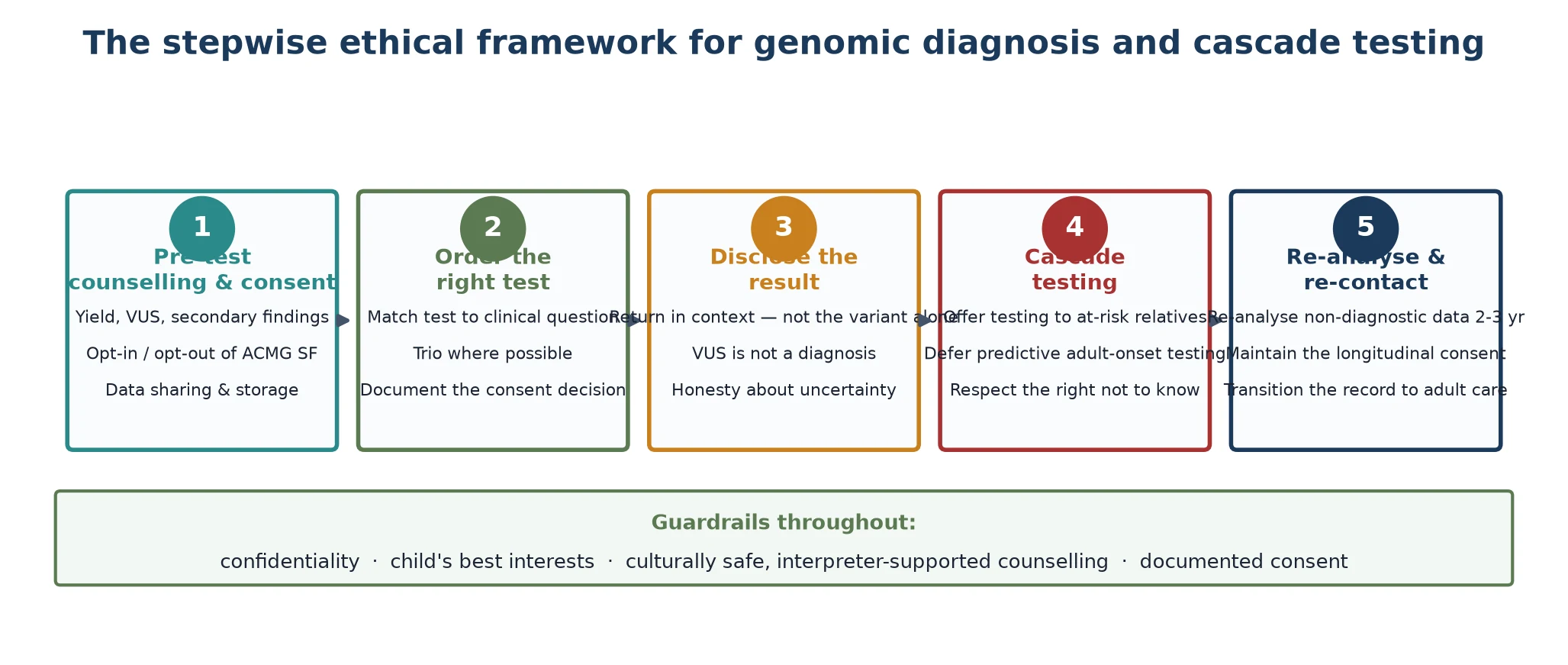
Step one, pre-test counselling and consent, sets the entire pathway. The conversation covers yield, the possibility of a variant of uncertain significance, the opt-in or opt-out decision for secondary findings, data sharing, and the implications for relatives. The decisions are documented so that disclosure follows an agreed pathway. Step two, order the right test, matches the technology to the clinical question — microarray, gene panel, exome, genome, or trio — and documents the consent decision alongside the order. [5] [9]
Step three, disclose the result in context, returns the finding as a clinical narrative rather than a laboratory call. A pathogenic result prompts a discussion of the diagnosis, natural history, management, reproductive implications, and the cascade-testing obligation. A variant of uncertain significance prompts a discussion of the uncertainty, the plan to investigate and re-analyse, and the principle that management follows the clinical picture. A secondary finding is disclosed only with prior consent, with disease-specific counselling. Step four, cascade testing, offers testing to at-risk relatives with the proband's consent to share identity, defers predictive testing for adult-onset conditions in minors, and respects the right not to know. Step five, re-analysis and re-contact, keeps non-diagnostic results alive by re-analysing every two to three years and re-contacting the family when new knowledge changes the answer. [1] [7]
C.O.D.E.R. — the ethical genomic pathway
Specific Subtypes & Scenarios
The four domains generate recognisable scenarios that examiners use to test whether a candidate can apply the right rule. Each scenario has a characteristic ethical tension and a characteristic correct answer. [1] [4]
The predictive-testing request for an adult-onset condition is the classic. A parent who carries, or whose sibling has, Huntington disease, hereditary breast and ovarian cancer, or another adult-onset condition asks to test the healthy child. The correct answer, grounded in the open-future principle and the AAP/ACMG consensus, is to defer testing to the age of maturity so that the future adult can decide. The clinician explores the parent's reasons — often anxiety, a desire to plan, or guilt — offers psychosocial support, and explains why international consensus is to wait. [2] [4]
The predictive-testing request for a childhood-actionable condition is the exception. A child at 50 percent risk of MEN2 should be tested, because prophylactic thyroidectomy in early childhood prevents medullary thyroid cancer. A child at risk of familial adenomatous polyposis should enter surveillance. The decisive feature is the existence of an intervention in childhood that changes outcome; where it exists, testing is justified, and deferring would deny the child effective prevention. [1]
The secondary-finding disclosure scenario tests whether the candidate remembers the consent pathway. An actionable variant in a hereditary cancer or cardiomyopathy gene is found. The first question is whether the family opted in. If yes, the finding is returned with counselling and a management plan. If no, the situation is managed carefully — the clinical geneticist and counsellor discuss the finding, its significance, and the option to receive it now — rather than returning it unilaterally. The original Green 2013 policy made the list mandatory; the Kalia 2017 update moved to opt-out; current practice treats it as opt-in with opt-out allowed. [5] [6] [7]
The cascade-testing scenario tests confidentiality and the right not to know. A pathogenic variant is confirmed in the proband, and at-risk relatives should be offered testing. The clinician offers the proband support in communicating with relatives, may provide a family letter that does not name the proband, and respects that some relatives will decline. Carrier testing of the proband's healthy younger siblings is deferred to reproductive age, and predictive testing for an adult-onset familial variant is deferred to maturity. [3] [4]
Complications & Pitfalls
The complications of genomic ethics are the errors that harm children and families and that cost candidates marks. They fall into cognitive traps and practical failures, and the candidate should be able to name and avoid each. [1] [3]
The first pitfall is predictive-testing a healthy child for an adult-onset condition with no childhood benefit. This is against international consensus, it forecloses the future adult's right to decide, and it remains the single most reliable way to lose marks on this topic. The correct answer is to defer, to explore the parent's reasons, and to offer support. The second pitfall is acting on a variant of uncertain significance as though it were pathogenic — ordering surveillance, prophylactic intervention, or family testing on the strength of a call the evidence cannot support. A VUS is investigated and re-analysed, never acted upon. [1] [9]
The third pitfall is returning a secondary finding without prior consent. The family must have been asked, and the decision must be documented, before any actionable variant is returned. If a finding surfaces without prior consent, the clinical geneticist and counsellor manage the situation deliberately rather than disclosing unilaterally. The fourth pitfall is breaching confidentiality in cascade testing — contacting relatives using the proband's identity without consent, or testing a sibling without the proband's agreement to share the result. The proband's confidentiality governs how relatives are approached, and a family letter that does not name the proband is one accepted mechanism. [3] [5]
The fifth pitfall is failing to re-analyse a non-diagnostic result as new genes are discovered and classification criteria evolve. The family should be offered re-analysis every two to three years, and the result should be reviewed whenever the phenotype changes. A non-diagnostic result is not the end of the diagnostic odyssey; it is a pause pending new knowledge. [6] [9]
Prognosis & Disposition
The prognosis of an ethically managed genomic encounter is good in two senses that the candidate should articulate. Clinically, a well-conducted consent and disclosure process delivers the maximum benefit of a diagnosis with the minimum harm of uncertainty and unwanted information. Relationally, it preserves trust between the family and the clinical service over the long arc of care. [1] [3]
The disposition is shared, longitudinal care. The clinical geneticist owns the variant interpretation and the re-analysis schedule. The genetic counsellor owns the consent, the disclosure, and the cascade-testing coordination. The general paediatrician owns the coordination of care, the preventive health, and the safeguarding of the child's interests across the transition to adult services. Each role is distinct, and the candidate should be able to describe the handover between them. [2] [9]
The transition from paediatric to adult care is a high-risk point for loss of continuity in genomic surveillance and in the re-analysis schedule. The future adult should enter adult care with the genetic record, the re-analysis plan, and — where a predictive or carrier test was appropriately deferred — the offer to make that decision now that they have the capacity to do so. The disposition is therefore not a single clinic visit but a lifelong relationship that the paediatric team hands on. [1] [10]
Special Populations
The same ethical framework behaves differently across populations, because access, equity, cultural safety, and representation in variant databases are unevenly distributed. The candidate should be able to describe how the framework adapts rather than assume a single universal application. [1] [2]
In remote and Indigenous communities, the barriers include geographic distance from genetic services, the cost of testing, the need for culturally safe counselling, and the ethics of sample storage and data sharing. Biological material may carry cultural significance that conflicts with the assumptions of biobanking, and data-sharing consent must be discussed respectfully and in the family's language. Culturally safe practice uses a cultural broker or interpreter where needed, coordinates with Indigenous health services, and recognises that the concept of an "individual" result may extend to kinship and community in ways that standard consent forms do not capture. [1] [2]
In migrant, refugee, and asylum-seeking families, the testing pathway may be complicated by incomplete family histories, consanguinity that raises the likelihood of autosomal recessive disease, different prior testing records from the country of origin, and language barriers. A trained interpreter must be used at every key consultation. The under-representation of non-European populations in variant databases is a particular concern, because a variant rare in European populations but common in the patient's ancestral population may be falsely classified as pathogenic, producing a false-positive diagnosis with downstream ethical and clinical harm. [1] [9]
In children in out-of-home care and donor or adoptive conceptions, the family-history gap and the question of whose consent governs predictive testing demand careful handling. In adolescents transitioning to adult care, the deferred predictive or carrier test now becomes a decision the young person can make for themselves, and the transition is the moment to offer it. In families managing complex disability, a confirmed molecular diagnosis can unlock coordinated care plans, disability funding, and community support, and the ethical value of the answer is high even when no disease-specific therapy exists. [2] [3]
Evidence, Guidelines & Regional Differences
The evidence base for the ethics of paediatric genomic testing rests on a set of consensus statements and policy documents rather than randomised trials, because the subject is normative as well as empirical. The candidate should know the key documents and what each establishes. [1] [3]
The ASHG and ACMG "Points to Consider" (Botkin 2015) is the current consensus framework for genetic testing in children and adolescents, updating the original 1995 document and embedding the open-future principle. The joint AAP and ACMG policy statement (Committee on Bioethics 2013) and its companion technical report (Ross 2013) set the North American paediatric consensus, and Ross's analysis of the best-interest standard (2013) clarifies how that standard should and should not be applied to predictive testing. Together these documents converge on the same core position: test symptomatic children, defer predictive and carrier testing where there is no childhood benefit. [1] [2] [3] [4]
The ACMG secondary-findings recommendations (Green 2013, Kalia 2017, Miller 2021) shaped the return of medically actionable findings through the SF list, which evolved from a mandatory original list, through the v2.0 opt-out update, to the v3.0 list. The Bennette 2015 cost-effectiveness analysis established that returning incidental findings can be cost-effective under certain assumptions, lending economic support to the policy. The Smith 2015 survey of genetic counsellor practices documented how the 2013 recommendations were incorporated into real-world counselling, and the Borghesi 2017 intersociety statement addressed the ethics of whole-exome sequencing in the critically ill newborn. [5] [6] [7] [8] [9] [10]
In Australia and Aotearoa New Zealand, genomic testing is publicly funded through the Medicare Benefits Schedule for specific indications, and state clinical genetics services deliver counselling and coordinate cascade testing, including by telehealth for rural and remote families. Legislative protections against genetic discrimination include Australia's Disability Discrimination Act 1992 and the privacy framework overseen by the Office of the Australian Information Commissioner, with the life-insurance moratorium agreed by the Financial Services Council; New Zealand's Human Rights Act 1993 provides analogous protections. The Australian Health Ethics Committee and the National Health and Medical Research Council guidance on genetic testing and insurance should be consulted for the current thresholds, because these protections have specific exclusions and are subject to review. Always confirm the current position before counselling a family on insurance implications.
[1][3]Exam Pearls
A fellowship candidate answering on the ethics of genomic diagnosis and cascade testing should land five anchor points and avoid four classic traps. The anchors are the test-type classification (diagnostic now; predictive, carrier, and susceptibility usually deferred), the open-future principle as the governing rule for predictive and carrier testing, the ACMG SF list as an opt-in (with opt-out) framework for secondary findings, the VUS as a call that must never drive action, and the cascade-testing pathway that respects the proband's confidentiality and each relative's right not to know. [1] [4]
The traps are predictive-testing a healthy child for an adult-onset condition, acting on a VUS as if pathogenic, returning a secondary finding without consent, and breaching confidentiality when contacting relatives. The candidate who can name the domain on the table, apply the right rule, and articulate the principle behind it will handle any scenario the examiner constructs. The five-step framework — counsel and consent, order correctly, disclose in context, cascade-test with consent, and re-analyse over time — carries the answer from the consent conversation to the long-term follow-up. [2] [7]
References
- [1]Botkin JR, Belmont JW, Berg JS, Berkman BE, Bombard Y, Holm IA, et al. Points to Consider: Ethical, Legal, and Psychosocial Implications of Genetic Testing in Children and Adolescents. Am J Hum Genet, 2015.PMID 26140447
- [2]Committee on Bioethics, Committee on Genetics, and the American College of Medical Genetics and Genomics Social, Ethical, and Legal Issues Committee. Ethical and policy issues in genetic testing and screening of children. Pediatrics, 2013.PMID 23428972
- [3]Ross LF, Saal HM, David KL, Anderson RR, American Academy of Pediatrics, American College of Medical Genetics and Genomics. Technical report: Ethical and policy issues in genetic testing and screening of children. Genet Med, 2013.PMID 23429433
- [4]Ross LF. Predictive genetic testing of children and the role of the best interest standard. J Law Med Ethics, 2013.PMID 24446947
- [5]Green RC, Berg JS, Grody WW, Kalia SS, Korf BR, Martin CL, et al. ACMG recommendations for reporting of incidental findings in clinical exome and genome sequencing. Genet Med, 2013.PMID 23788249
- [6]Kalia SS, Adelman K, Bale SJ, Chung WK, Eng C, Evans JP, et al. Recommendations for reporting of secondary findings in clinical exome and genome sequencing, 2016 update (ACMG SF v2.0): a policy statement of the American College of Medical Genetics and Genomics. Genet Med, 2017.PMID 27854360
- [7]Miller DT, Lee K, Chung WK, Gordon AS, Herman GE, Klein TE, et al. ACMG SF v3.0 list for reporting of secondary findings in clinical exome and genome sequencing: a policy statement of the American College of Medical Genetics and Genomics (ACMG). Genet Med, 2021.PMID 34012068
- [8]Bennette CS, Gallego CJ, Burke W, Jarvik GP, Veenstra DL. The cost-effectiveness of returning incidental findings from next-generation genomic sequencing. Genet Med, 2015.PMID 25394171
- [9]Smith LA, Douglas J, Braxton AA, Kramer K. Reporting Incidental Findings in Clinical Whole Exome Sequencing: Incorporation of the 2013 ACMG Recommendations into Current Practices of Genetic Counseling. J Genet Couns, 2015.PMID 25403901
- [10]Borghesi A, Mencarelli MA, Memo L, Ferrero GB, Bartuli A, Genuardi M, et al. Intersociety policy statement on the use of whole-exome sequencing in the critically ill newborn infant. Ital J Pediatr, 2017.PMID 29100554