Paeds · growth-development-and-behaviour
Behavioural assessment and functional analysis
Also known as Functional behaviour assessment · ABC chart behavioural assessment · Functional analysis of problem behaviour · Positive behaviour support assessment · Challenging behaviour formulation
Fellowship guide to paediatric behavioural assessment and functional analysis: operational definitions, medical and communication screens, multi-setting ABC data, four maintaining functions, descriptive versus experimental FA, PBS and FCT linkage, limited medication after formulation, and multi-agency plan leadership.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A childcare worker says a five-year-old “just snaps.” A school email asks for “something for aggression.” A parent wants a tablet increased because shower time is a war. Your job is not to name a villain. Your job is to run a behavioural assessment that finds what the behaviour does for the child, what medical or communication problem sits underneath, and what support will change the contingency rather than only the volume of the noise. [1] [10] [11]
Challenging behaviour is a description of impact — intensity, frequency or duration that risks safety or seriously limits ordinary life — not a DSM diagnosis by itself. Psychiatric disorders may coexist and need their own criteria. Emerson’s total-population work framed challenging behaviour as a common service-level problem in intellectual disability, not a rare curiosity. [9]
Functional assessment asks: under what conditions does this behaviour occur, and what consequence keeps it going? Experimental functional analysis (FA) tests those hypotheses under controlled conditions, classically associated with Iwata’s work on self-injury. Decades of FA research show that most identified functions are social (attention, escape, tangible), with a meaningful automatic/sensory subset. [1] [2] [3]
This leaf owns assessment method and formulation. Condition-specific treatment depth lives on linked pages for tantrums, oppositional behaviour, school refusal, ASD, ADHD and intellectual disability. Cross-link them. Do not hide a second disorder textbook here. [10] [14]
Assessment spine in one clinic block
Is anyone unsafe now?
Injury risk, medical emergency or safeguarding converts the visit.
Define the behaviour
What exactly happens, how often, how hard, where and with whom.
Medical and communication screen
Pain, sleep, seizures, sensory load, hearing, speech/AAC.
ABC data multi-setting
Home, school, care — not a single bad day story.
Function hypothesis and matched plan
PBS, FCT, caregiver training; medication only if residual severe risk.
Classification
Classify three layers before you open a prescribing chart: the job of assessment, the function class, and the intervention intensity. [1] [2]
Assessment levels
| Level | What it is | Who usually leads | Output |
|---|---|---|---|
| Operational definition | Clear topography, frequency, intensity, duration, context | Medical home with family/school | Shared target behaviour |
| Descriptive functional assessment | Multi-informant history + ABC charts across settings | Paediatrician with psychology/behaviour support | Function hypothesis |
| Experimental functional analysis | Controlled conditions testing maintaining contingencies | Specialist behaviour analysis teams | Confirmed function when safe/ethical |
| PBS plan | Function-linked proactive and reactive strategies with quality-of-life goals | Multi-agency team | Written plan, data review, restraint reduction |
General paediatric practice usually starts with descriptive assessment and medical screening. Experimental FA is powerful and resource-intensive; decades of literature support its utility, but protocols, safety and ethics belong with trained teams. [2] [3]
Four classic maintaining functions
- Attention — behaviour reliably produces social response (reprimand, comfort, laughter, eye contact).
- Escape/avoidance — behaviour reliably ends or delays demand, task, transition or aversive sensory event.
- Tangible — behaviour reliably produces preferred item, food, screen or activity.
- Automatic/sensory — behaviour produces its own sensory consequence and may persist when the child is alone. [1] [2]
Mixed functions are common. Rank the primary maintaining contingency for the target behaviour you are treating first. [2] [3]
Related but different jobs
Screening tools find children who need developmental or behavioural evaluation; they do not replace functional analysis of a named behaviour. Diagnostic labels (ASD, ADHD, anxiety) change probability and supports, but they do not tell you why this shower-time punch continues. [10] [11]
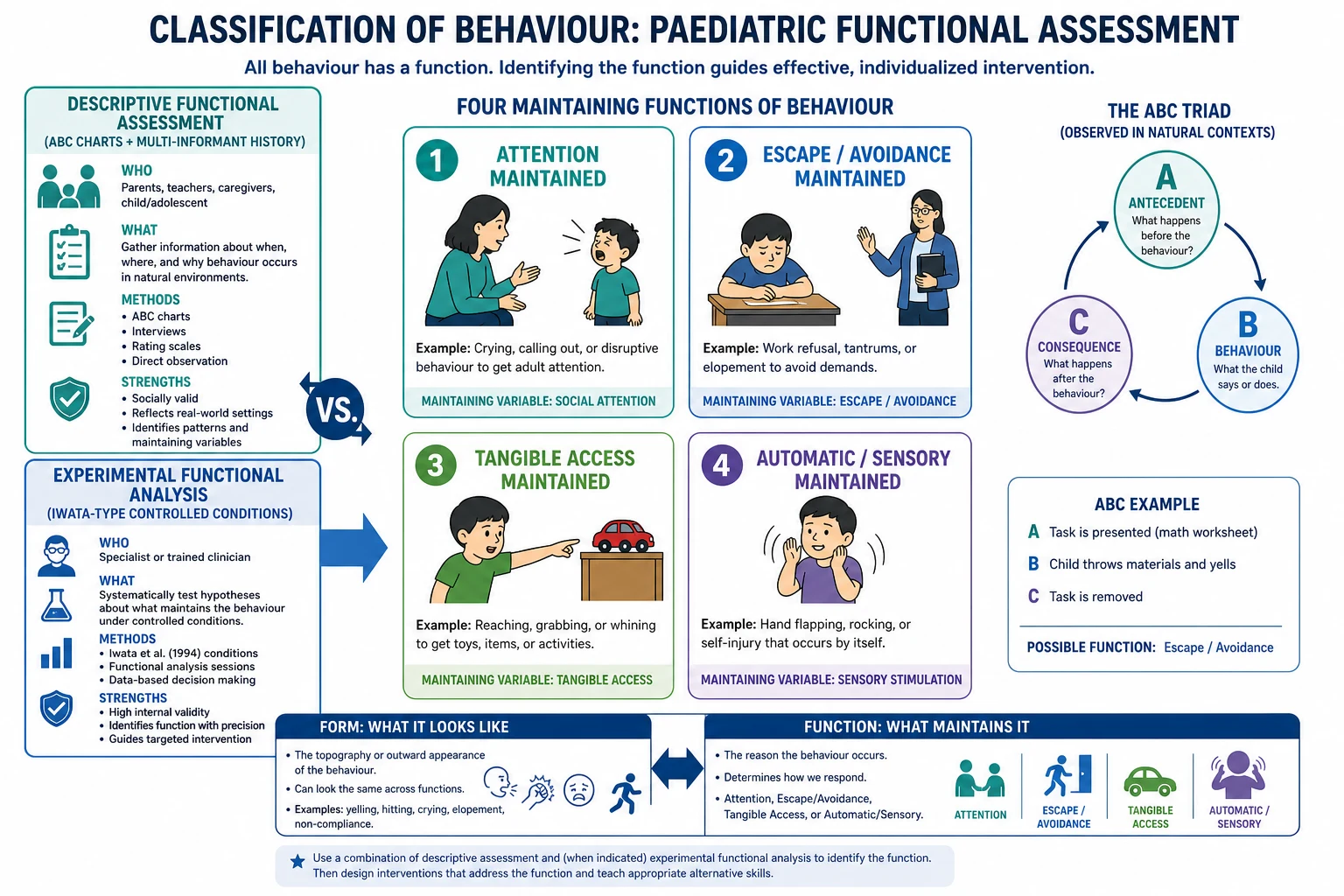
Read the figure like this: if you only collect stories, you get blame. If you only run controlled FA without medical context, you miss pain. The paediatric job joins both. [1] [10]
Epidemiology & Risk Factors
Challenging behaviour is patterned. Emerson’s total-population framing in intellectual disability showed that severe problem behaviour is common enough to demand systematic service design, not one-off crisis scripts. Autism populations carry high rates of co-occurring psychiatric and behavioural problems; Simonoff’s population-derived sample is a classic comorbidity anchor, and Hyman’s AAP report expects medical homes to manage behaviour pathways without equating autism with “untreatable behaviour.” [9] [10]
Early childhood emotional and behavioural problems are also common enough for the medical home to lead. Gleason’s AAP clinical report places more than 10% of young children in the clinically significant mental-health problem range and stresses limited early psychopharmacology evidence — so assessment and therapy access matter more than default medication. [11]
Risk concentrates where communication is limited, sensory load is high, sleep is short, pain is unrecognised, caregiving is inconsistent, and services are fragmented. Poverty, overcrowding, racism in care systems, language discordance and out-of-home care reduce assessment quality and plan fidelity. Population data on psychotropic use in intellectual disability show substantial prescribing for challenging behaviour and mental illness — a reminder that formulation gaps become tablets. [15] [16] [18]
Pathophysiology
Think in contingencies, not character. A behaviour that once started from pain, fear or overload can later be maintained by what happens after it. If aggression ends a hard task, escape is reinforced. If self-injury produces adult rush and touch, attention is reinforced. If screaming produces a tablet, tangible access is reinforced. If hand-mouthing produces sensory input even when alone, automatic reinforcement may maintain it. Iwata’s experimental conditions were built to separate these processes. [1] [2]
Intermittent reinforcement is sticky. Inconsistent adult responses — sometimes give in, sometimes punish harshly — can strengthen behaviour more than a steady plan. That is why multi-setting inconsistency (home soft, school hard, respite different again) keeps clinics full. [2] [3]
Medical drivers feed the loop. Dental abscess, otitis, constipation, reflux, fracture, migraine, dystonia, seizure clusters and sleep apnoea can present as “behaviour,” especially in non-verbal children. Treat the biology and reassess the operant picture. [10]
Communication failure converts unmet needs into topography adults notice. Functional communication training works because it installs a socially efficient alternative that still achieves the function. [4]
Toxic stress and trauma alter arousal regulation and threat detection. Garner’s framing is not a diagnosis of every meltdown as PTSD, but it explains why safety, predictability and relationship repair sit inside behavioural work. [18]
Medication without function change can reduce intensity while the contingency remains. When the drug is stopped or tolerance appears, the topography returns — expected if escape still works better than asking for a break. [8] [13] [16]
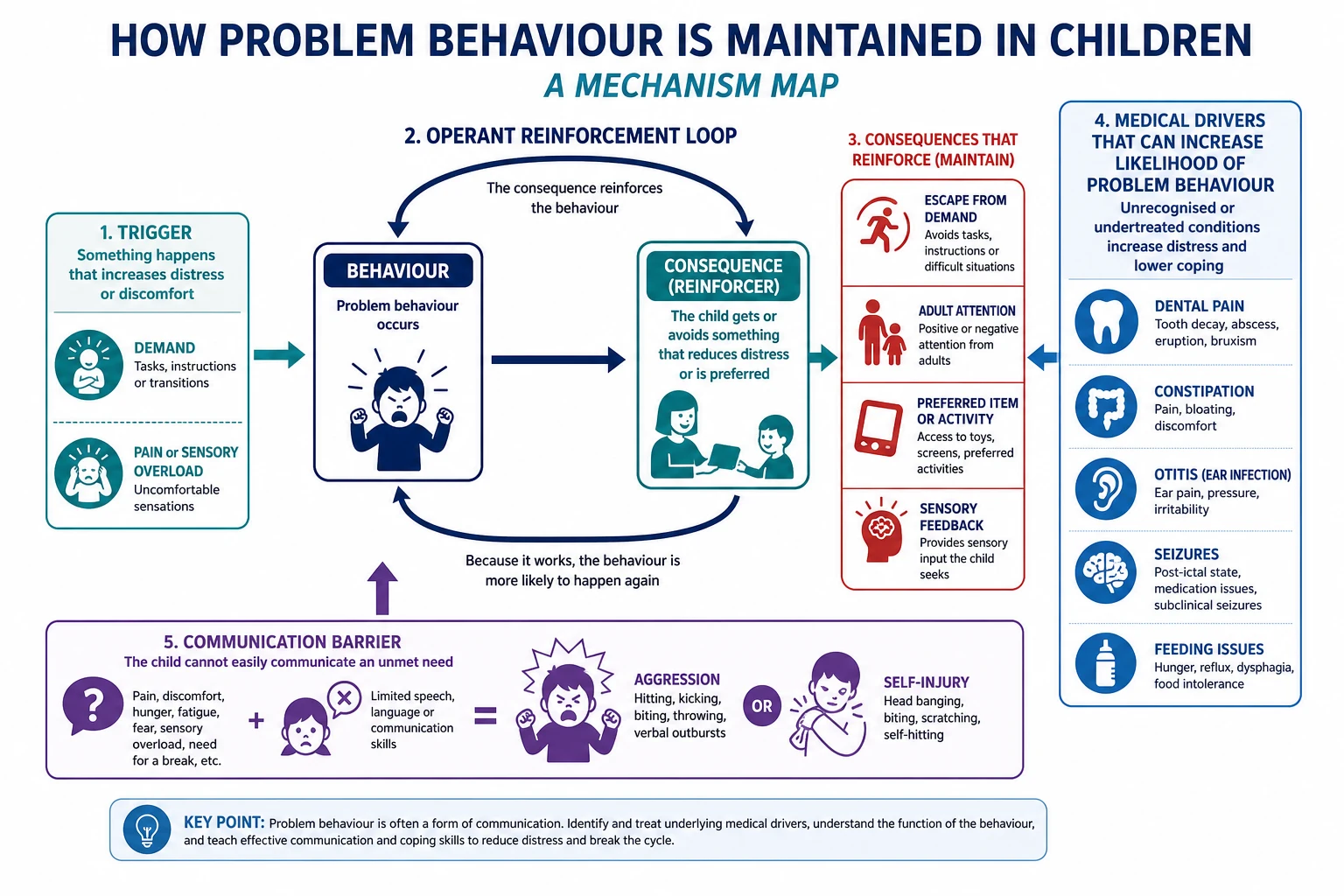
Read the figure like this: your plan must interrupt the maintaining arrow, not only scold the middle box. [1] [4]
Clinical Presentation
Families and schools rarely present with function labels. They present with scenes. [10] [11]
Common entry tickets
- “He hits when we say no to screens.”
- “Shower and teeth are impossible.”
- “She is fine at home and melts down at school.”
- “He bites his hand when left alone.”
- “Staff want the risperidone increased.”
- “He used to manage transitions; something changed last month.”
Function-linked patterns you should recognise
Attention-maintained. Peaks when adults are busy or conversations exclude the child; reprimands still “work” as attention; alone time is quieter. [2]
Escape-maintained. Peaks at demand onset (homework, hygiene, therapy, classroom tasks); settles when the demand is removed; may include running from the room. [1] [2]
Tangible-maintained. Peaks when preferred items are denied or removed; ends when the item is restored. [2]
Automatic/sensory. May continue when alone; less sensitive to social contingencies; always screen for pain and medical causes before accepting “pure sensory.” [1] [2]
School refusal as behaviour. Kearney’s profiles are a worked functional analysis: avoid negative affectivity; escape aversive social/evaluative situations; gain attention/proximity; gain tangible reinforcement outside school. Mixed functions are common. Full return-to-school therapy lives on the school-refusal leaf; the method lives here. [12]
When the presentation is the wrong clinic label
Sudden escalation with fever, reduced alertness, new seizures, refusal to weight-bear, or facial swelling is medical until proven otherwise. Regression of skills needs a developmental-neurology pathway, not only ABC charts. [10]
Differential Diagnosis
The differential is not “naughty versus neurodiverse.” It is which drivers and which functions explain this pattern. [10] [14]
| Pattern | Prefer first | Also consider | Do not assume |
|---|---|---|---|
| New aggression in non-verbal child | Pain, dental, ENT, constipation, fracture, seizure | Escape or attention function still present | “Personality change” without exam |
| Classroom disruption only | Escape from academic demand; learning disorder; bullying | ADHD, anxiety, hearing loss | Home “spoiling” as sole cause |
| Night-time self-injury | Pain, sleep disorder, automatic function | Trauma nightmares | Immediate antipsychotic |
| School non-attendance with panic | Kearney functions; anxiety disorders | Truancy pattern, depression, ASD overload | Pure “school phobia” label without function |
| Chronic antipsychotic for “behaviour” | Overshadowed medical/communication need; unassessed function | True psychosis or severe mood disorder | Lifelong drug as first diagnosis |
| Post-dose restlessness and worse aggression | Akathisia or paradoxical effect | Escape function still active | Higher dose by default |
Clinical & Bedside Assessment
Start with safety and the child’s body
Ask about injury, weapons, wandering, restraint use and caregiver capacity. Examine for pain sources. Review sleep, bowels, teeth, ears, medications and recent changes. If the child is acutely unwell, convert. [10] [11]
Operationalise the target
Write one sentence everyone can measure: “Open-hand hit to adult arm during personal care, 0–8 times per shower, lasting under 10 seconds, past 6 weeks.” Vague “aggression” cannot be charted or treated consistently. [2]
Multi-informant, multi-setting history
Interview caregivers separately from school/care staff when possible. Ask what happens before, during and after. Use professional interpreters when language discordance exists. Include the child or young person with developmental adaptations. [17]
ABC charts
Ask teams to log antecedent, behaviour and consequence across days and settings. Look for reliable patterns, not single dramatic stories. Descriptive assessment is the paediatric workhorse; experimental FA refines hypotheses when available and safe. [1] [2]
Communication, sensory and developmental context
What can the child request? Is AAC available and used? Which sounds, textures, crowds or transitions are aversive? What is the developmental age for demand setting? Behaviour plans fail when demands ignore developmental level. [4] [10]
Document like a system
Record operational definition, settings, function hypothesis, medical findings, safety risks, plan owner and review date. Care coordination is part of the assessment product. [17]
Investigations
Behavioural assessment is mostly structured clinical data. Investigations follow red flags, not a “behaviour blood panel.” [10]
Descriptive data. ABC logs, incident reports, restraint logs, attendance calendars and sleep diaries are first-line. [2]
Experimental FA. Specialist teams may use demand, attention, alone/ignore and play/control conditions (and modern variants). Beavers and Melanson-type reviews summarise decades of FA outcomes and common social functions. Do not invent a corridor protocol or claim you ran FA when you only took history. [1] [2] [3]
Medical tests. Targeted: dental review, ENT, constipation work-up, sleep assessment, EEG only with seizure suspicion, imaging for trauma or focal neurology. Avoid shotgun genetics because a child hit a teacher once. [10]
Sensory checks. Hearing and vision pathways when communication or learning demand is implicated. [10]
Rating scales. Irritability or problem-behaviour scales can track change; they do not replace function. Do not invent proprietary cut-offs in a viva — name the local tool and principle. [13] [14]
Low-value moves. Repeating “try harder discipline” without ABC data. Escalating antipsychotics without medical screen. Ordering broad panels to postpone hard conversations about escape function. [8] [15]
Management — Resuscitation
Most behavioural assessment is outpatient. These convert immediately: [10] [11]
- Active severe aggression or self-injury with injury risk — protect airway and others; least-restrictive safety; emergency services if needed.
- Medical emergency — seizures, encephalopathy, severe pain, anaphylaxis, trauma.
- Safeguarding or family violence — statutory pathways supersede behaviour coaching.
- Caregiver collapse with child at imminent risk — safety plan and crisis supports.
- Suspected serious medication adverse effect (for example acute dystonia or severe akathisia) — urgent review; do not “push through.” [13]
Say the conversion out loud: “We are treating safety and medical risk first; the behaviour plan continues after that.” [17]
Management — Definitive & Stepwise
- Confirm safety and medical/communication screen are done or in parallel. [10]
- Share the function hypothesis in plain language with family and school. [2]
- Proactive/antecedent strategies. Predictable routines, visual schedules, demand fading, reduced aversive load, preferred breaks earned, environmental redesign of high-risk routines (for example adapted washing methods). [4] [10]
- Functional communication training. Teach a request that serves the same function — “break,” “help,” “stop,” item request — and honour it while thinning later. FCT has a large efficacy literature moving toward effectiveness questions. [4]
- Differential reinforcement. Reinforce the alternative and other appropriate behaviour; minimise intermittent pay-offs for the problem topography. Consistency across adults is the active ingredient. [2] [4]
- Parent and carer training with practice. Bearss showed parent training superior to parent education alone for disruptive behaviour in children with ASD — skills practice beats handouts. [5]
- Write a PBS plan. Person-centred goals, proactive strategies, least-restrictive reactive strategies, data review, multi-agency ownership, explicit reduction of restrictive practices. [15] [17]
- Medication only after formulation when serious risk persists or while intensive programmes start, with named target behaviour, lowest effective dose under specialist guidance, metabolic/EPS/prolactin or akathisia monitoring as relevant, and a review/stop date. Risperidone (RUPP) and aripiprazole have trial evidence for irritability in autism, not for core social deficits and not as routine first-line for all challenging behaviour. Tyrer’s adult ID trial found risperidone and haloperidol not superior to placebo for aggressive challenging behaviour — use that as a caution against automatic antipsychotic escalation culture. [6] [7] [8] [13] [16]
- Close loops. Track school implementation, therapy access, medication reviews and no-shows. Care coordination is treatment. [17]
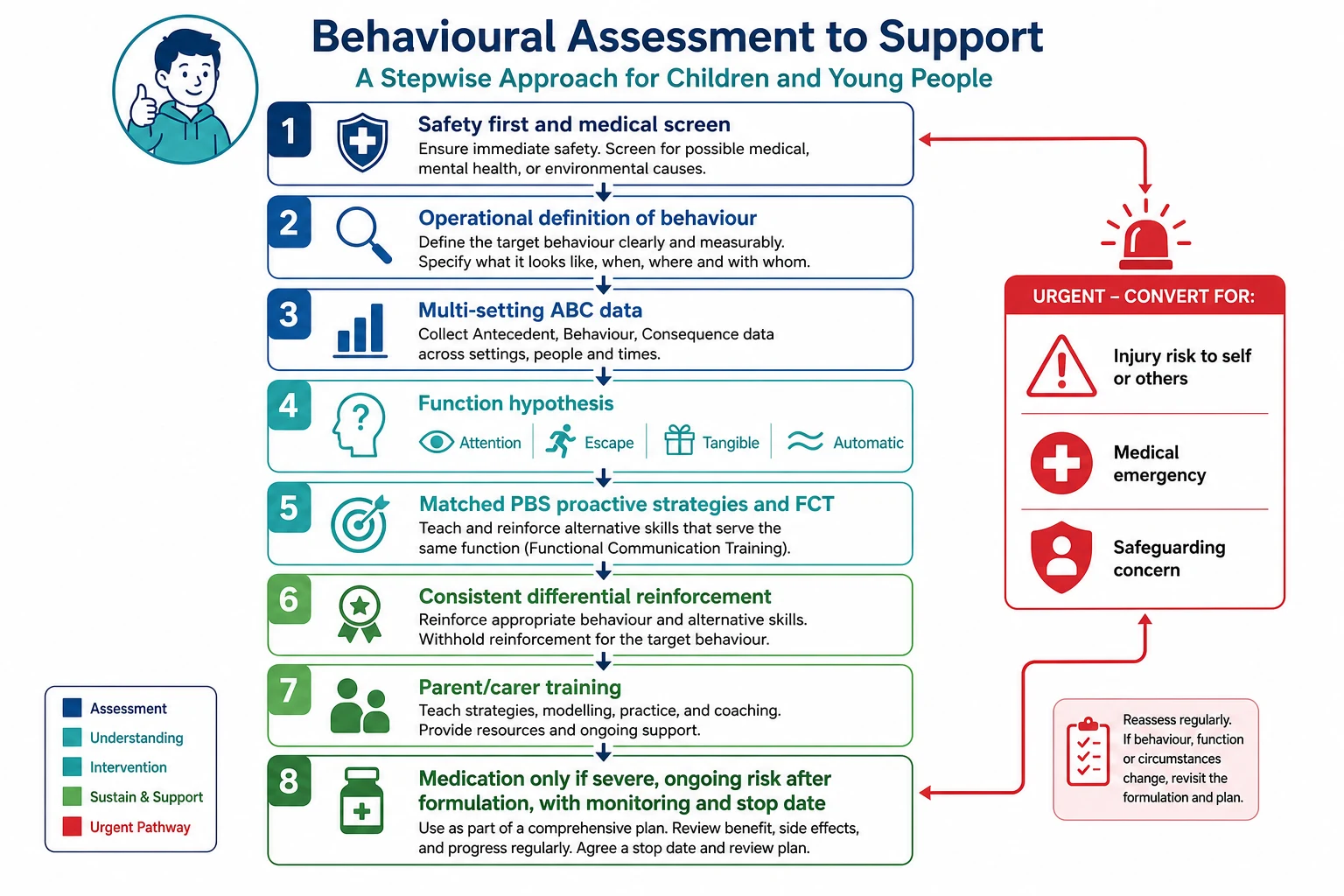
Read the figure like this: medication sits at the bottom of a ladder that most children never need if the function work is real. [5] [8] [13]
Specific Subtypes & Scenarios
Escape during personal care. High classic for demand avoidance plus sensory aversion. Redesign the routine, teach “stop/help,” reduce forced duration, reinforce cooperation steps. Do not only “hold still and increase risperidone.” [1] [4]
Tangible screen aggression. Contingency management, predictable access schedules, and replacement requests; caregiver consistency is the treatment. [2]
Automatic self-injury when alone. Medical pain screen first; environmental enrichment; protective equipment as temporary safety when specialist-supported; do not assume pure sensory forever. [1] [2]
ASD with severe irritability. Hyman and AACAP pathways: behavioural and environmental care first; consider risperidone or aripiprazole for severe irritability after formulation, with monitoring. [6] [7] [10] [14]
ID with long-term antipsychotic for “behaviour.” Reassess indication. Prefer PBS and supervised reduction when risk allows, consistent with deprescribing evidence and over-prescription epidemiology. [8] [15] [16]
School refusal. Apply Kearney functions; graded return lives on the dedicated leaf; do not prescribe for attendance alone without anxiety formulation. [12]
Toddler limit-testing. Developmental normal range is wide; Gleason frames medical-home leadership without medication-first care for early childhood. [11]
Rural long waits. Start descriptive assessment, medical screen, interim PBS coaching and safety-netting now; refer without waiting for perfection. [17]
Complications & Pitfalls
- Medication-first for staff convenience. [8] [15]
- Treating form without teaching a replacement skill. [4]
- Missing pain in non-verbal children. [10]
- Diagnostic overshadowing in ASD/ID. [10] [14]
- Inconsistent multi-setting responses creating intermittent reinforcement. [2]
- Punishment-only or restraint culture without proactive strategies. [15]
- Open-loop psychology referral with no interim plan. [17]
- Skipping safety assessment of self-injury severity. [1]
- Language-discordant history without interpreter.
- Cloning disorder chapters instead of teaching assessment method. [10]
Prognosis & Disposition
Function-matched intervention with caregiver fidelity improves day-to-day safety and participation for many children. Unaddressed maintaining contingencies predict persistence. Antipsychotic suppression without plan change predicts relapse at dose reduction. [4] [5] [16]
| Scenario | Disposition | Must include |
|---|---|---|
| Mild, clear function, safe | Medical-home PBS coaching + review | Written strategies and data plan |
| Multi-setting, moderate risk | Specialist behaviour support / psychology / developmental team | Multi-agency PBS, school plan |
| Severe injury risk or medical red flags | Urgent specialist + safety pathway | Same-week senior plan |
| On chronic antipsychotic without indication clarity | Formulation + deprescribing-capable review | Monitoring and PBS intensification |
Disposition is not “refer and forget.” Give families something to do this week while systems move. [17]
Special Populations
Non-verbal and AAC users. Communication access is treatment, not optional therapy later. [4]
ASD and intellectual disability. Higher CB prevalence; formulation mandatory before chronic drugs. [9] [10]
ADHD. Distinguish impulsivity from escape/attention functions; treat ADHD on its pathway when indicated without skipping ABC work. [10] [11]
Trauma and out-of-home care. Safety, relational repair and predictable adults sit inside the plan. [18]
Indigenous families. Culturally safe assessment and local supports are part of validity. [17] [18]
Migrant and refugee families. Interpreters and trauma-informed pacing. [17]
Medical complexity. Procedure-related and pain-related behaviour are common; coordinate with specialty teams. [17]
Adolescents. Include self-report, capacity and peer context; plan transition of behaviour supports. [10] [17]
Rural-remote. Telehealth ABC coaching and interim plans while specialist access is slow. [17]
Evidence, Guidelines & Regional Differences
Iwata’s functional analysis of self-injury remains the conceptual foundation for experimental FA. Beavers (30-year) and Melanson (40-year) reviews summarise the mature FA literature and the predominance of identifiable social functions. [1] [2] [3]
Ghaemmaghami and colleagues review functional communication training from efficacy toward effectiveness — replacement communication is not a slogan. [4]
Bearss and colleagues showed parent training superior to parent education for disruptive behaviour in ASD. [5]
RUPP risperidone and Owen aripiprazole provide core irritability pharmacotherapy evidence in autism; Fung’s meta-analysis supports pharmacologic options for severe irritability after behavioural care framing. These do not treat core autism. [6] [7] [13]
Tyrer 2008 is the exam-critical null trial for antipsychotics in aggressive challenging behaviour in adults with intellectual disability. Deb’s international guide and Sheehan’s deprescribing and population work push against open-ended chemical restraint culture. [8] [15] [16]
Hyman (AAP ASD), Volkmar (AACAP ASD parameter) and Gleason (early childhood emotional-behavioural problems) locate the medical home’s leadership role. NICE NG11 (official source) is the UK psychosocial-first anchor for learning disability and challenging behaviour — cite as jurisdiction guidance, not global statute. [10] [11] [14]
Use local disability supports, PBS frameworks, school behaviour pathways and specialist developmental/CAMHS services. Cultural safety and interpreter access are part of valid assessment. Map trial evidence to local formulary and consent rules rather than importing US clinic protocols as law. [10] [17]
NICE NG11 prioritises psychosocial and environmental interventions informed by assessment; medication only when behaviour poses serious risk and non-drug approaches are insufficient or while programmes are established, with regular review. Defend the principle; look up local operational forms. [8] [15]
AAP ASD guidance and AACAP parameters dominate exam answers for autism-related irritability pathways; ABA access and insurance structures vary widely. Still require function-informed care before chronic antipsychotics. [6] [10] [14]
Provincial pathways for developmental and mental-health services vary; the same nested model applies: safety, medical screen, function hypothesis, PBS/FCT, limited medication. [10] [17]
Controversies. Experimental FA resource and ethics debates; intensity and goals of ABA-type programmes versus neurodiversity-affirming limits on compliance-only targets; antipsychotic overuse; restraint reduction; waitlist ethics. Name the tension; do not invent false certainty. [3] [8] [16]
Exam Pearls
References
- [1]Iwata BA, Dorsey MF, Slifer KJ, Bauman KE, Richman GS Toward a functional analysis of self-injury. Journal of applied behavior analysis, 1994.PMID 8063622
- [2]Beavers GA, Iwata BA, Lerman DC Thirty years of research on the functional analysis of problem behavior. Journal of applied behavior analysis, 2013.PMID 24114081
- [3]Melanson IJ, Fahmie TA Functional analysis of problem behavior: A 40-year review. Journal of applied behavior analysis, 2023.PMID 36892835
- [4]Ghaemmaghami M, Hanley GP, Jessel J Functional communication training: From efficacy to effectiveness. Journal of applied behavior analysis, 2021.PMID 32929757
- [5]Bearss K, Johnson C, Smith T, et al. Effect of parent training vs parent education on behavioral problems in children with autism spectrum disorder: a randomized clinical trial. JAMA, 2015.PMID 25898050
- [6]McCracken JT, McGough J, Shah B, et al.; Research Units on Pediatric Psychopharmacology Autism Network Risperidone in children with autism and serious behavioral problems. The New England journal of medicine, 2002.PMID 12151468
- [7]Owen R, Sikich L, Marcus RN, et al. Aripiprazole in the treatment of irritability in children and adolescents with autistic disorder. Pediatrics, 2009.PMID 19948625
- [8]Tyrer P, Oliver-Africano PC, Ahmed Z, et al. Risperidone, haloperidol, and placebo in the treatment of aggressive challenging behaviour in patients with intellectual disability: a randomised controlled trial. Lancet, 2008.PMID 18177776
- [9]Emerson E, Kiernan C, Alborz A, et al. The prevalence of challenging behaviors: a total population study. Research in developmental disabilities, 2001.PMID 11263632
- [10]Hyman SL, Levy SE, Myers SM; Council on Children with Disabilities, Section on Developmental and Behavioral Pediatrics Identification, Evaluation, and Management of Children With Autism Spectrum Disorder. Pediatrics, 2020.PMID 31843864
- [11]Gleason MM, Goldson E, Yogman MW; Council on Early Childhood; Committee on Psychosocial Aspects of Child and Family Health; Section on Developmental and Behavioral Pediatrics Addressing Early Childhood Emotional and Behavioral Problems. Pediatrics, 2016.PMID 27940734
- [12]Kearney CA, Albano AM The functional profiles of school refusal behavior. Diagnostic aspects. Behavior modification, 2004.PMID 14710711
- [13]Fung LK, Mahajan R, Nozzolillo A, et al. Pharmacologic Treatment of Severe Irritability and Problem Behaviors in Autism: A Systematic Review and Meta-analysis. Pediatrics, 2016.PMID 26908468
- [14]Volkmar F, Siegel M, Woodbury-Smith M, King B, McCracken J, State M; American Academy of Child and Adolescent Psychiatry (AACAP) Committee on Quality Issues (CQI) Practice parameter for the assessment and treatment of children and adolescents with autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 2014.PMID 24472258
- [15]Deb S, Kwok H, Bertelli M, et al. International guide to prescribing psychotropic medication for the management of problem behaviours in adults with intellectual disabilities. World psychiatry, 2009.PMID 19812757
- [16]Sheehan R, Hassiotis A Reduction or discontinuation of antipsychotics for challenging behaviour in adults with intellectual disability: a systematic review. The lancet. Psychiatry, 2017.PMID 27838214
- [17]Council on Children with Disabilities and Medical Home Implementation Project Advisory Committee Patient- and family-centered care coordination: a framework for integrating care for children and youth across multiple systems. Pediatrics, 2014.PMID 24777209
- [18]Garner AS, Shonkoff JP; Committee on Psychosocial Aspects of Child and Family Health; Committee on Early Childhood, Adoption, and Dependent Care; Section on Developmental and Behavioral Pediatrics Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics, 2012.PMID 22201148