Paeds · growth-development-and-behaviour
Cerebral palsy: early recognition and classification
Also known as Cerebral palsy diagnosis · Early detection of cerebral palsy · GMFCS classification · CP motor type and topography · High probability cerebral palsy
Fellowship approach to early recognition of cerebral palsy, motor phenotype and topography, functional classification systems (GMFCS, MACS, CFCS, EDACS), early detection tools and first-step intervention planning.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A parent says, “She only uses her left hand,” or “His legs feel stiff when I change the nappy.” Your job is not to wait politely until the second birthday. Your job is to decide whether this child has a high probability of cerebral palsy, what pattern of motor disorder you are seeing, how the child functions day to day, and what must start now. [1] [16]
This page owns early recognition and classification. Ongoing hip surveillance, advanced tone management, feeding programmes and lifelong multidisciplinary care live on the companion page for CP surveillance and management. Cross-link developmental surveillance and dedicated GMA/HINE teaching rather than hiding full specialty manuals here. [1] [17]
C.L.A.S.S. early CP
Overview & Definition
Cerebral palsy is not one disease. It is a group of permanent disorders of the development of movement and posture. The cause is a non-progressive disturbance that happened in the developing fetal or infant brain. The motor disorder is often accompanied by epilepsy, sensation problems, perception issues, communication difficulty, behaviour challenges and secondary musculoskeletal problems. That is the modern consensus language from the Bax proposal and the Rosenbaum report. [2] [3]
Say the definition aloud in a viva without fluff: permanent motor disorder; early brain disturbance; lesion itself not progressive; associated impairments common. Then add the practical point: the clinical picture can still evolve in the first years as the nervous system matures, even though the original injury is not an ongoing degenerative disease. [3] [19]
Smithers-Sheedy and colleagues asked what still “counts” as CP in the twenty-first century. Registers and clinicians must keep clear inclusion rules. Progressive disorders, pure neuromuscular disease without early central injury, and transient motor signs that resolve do not belong under the CP label. When the story is wrong for a static early brain injury, stop and rethink. [19]
Classification
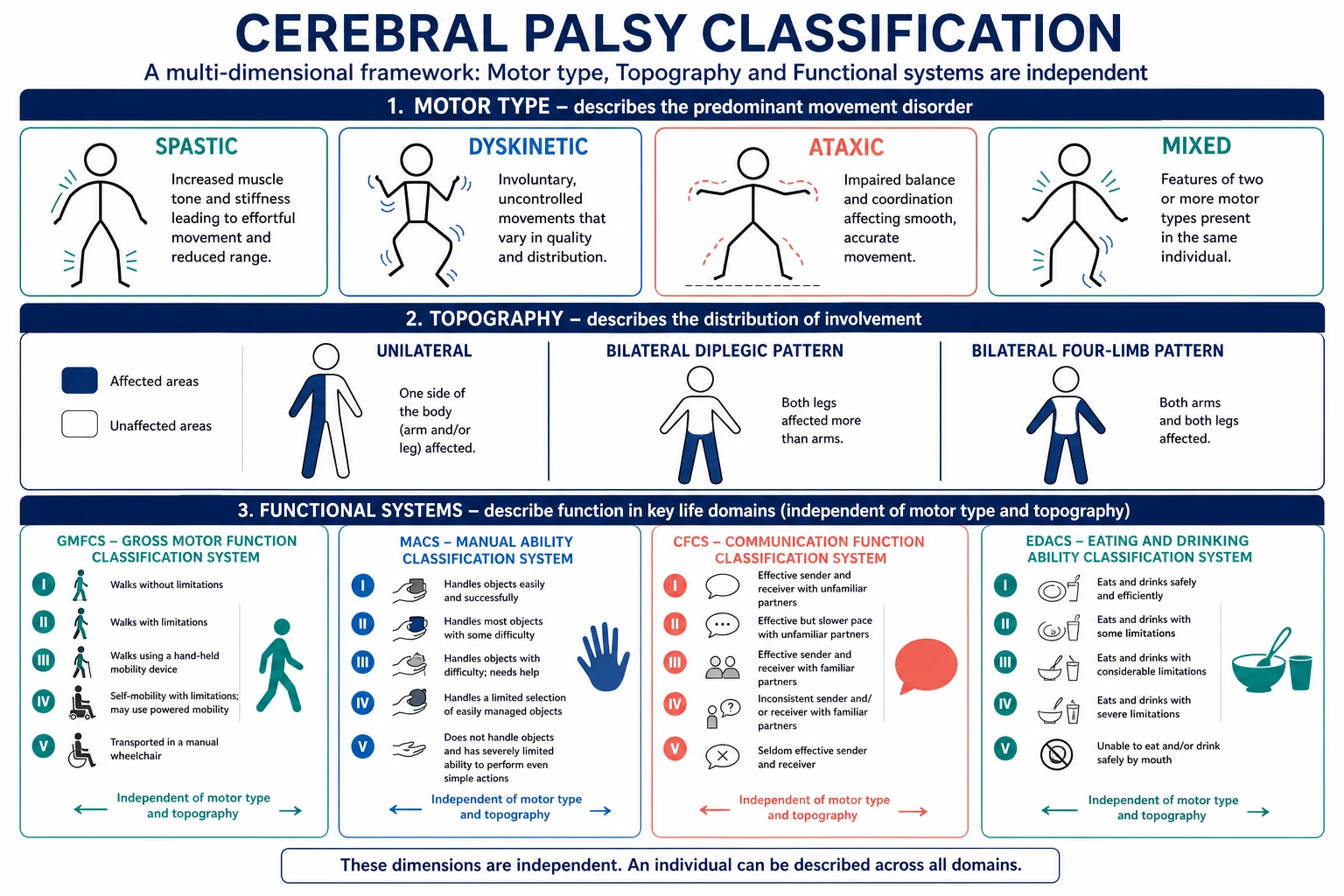
You need three parallel labels, not one. Motor type describes the movement disorder. Topography describes which body regions are affected. Function describes what the child can do in daily life. Mixing these three is a classic exam fail. [3] [17]
Motor type
Spastic CP is the most common pattern in many series. You see velocity-dependent increased tone, pathologically brisk reflexes and often a clasp-knife quality. Dyskinetic CP includes dystonia and choreoathetosis — involuntary postures and movements that often worsen with intention. Ataxic CP shows disordered balance and coordination with cerebellar features. Mixed patterns are common; name the predominant features rather than forcing a pure box. [3] [9]
Topography
Unilateral involvement (often called hemiplegia in clinic language) affects one side. Bilateral patterns may predominantly involve the legs (diplegic pattern) or all four limbs (quadriplegic/tetraplegic pattern). SCPE-style surveillance categories help epidemiology and communication across services. Use the words your local register and team understand, but always be clear whether one side or both sides are involved. [9] [3]
Functional classification
Functional systems answer different questions. They are not interchangeable severity scores. [17]
-
GMFCS (Gross Motor Function Classification System) describes usual gross motor performance from I (walks without limitations) through V (transported in a manual wheelchair). Palisano’s original work and the expanded and revised system (GMFCS-E&R) support reliable classification across ages with content validity for older children and youth. Assign GMFCS from observed and reported real-world mobility. Do not ask a parent, “What is your child’s GMFCS?” as if it were a blood group they should already know. [4] [5]
-
MACS (Manual Ability Classification System) describes how children handle objects in daily activities with their hands. [6]
-
CFCS (Communication Function Classification System) describes everyday communication effectiveness. [7]
-
EDACS (Eating and Drinking Ability Classification System) describes eating and drinking safety and efficiency. [8]
A child can walk well (favourable GMFCS) and still have major hand or communication needs. State domains separately. That is modern function-first disability classification. [17]
Epidemiology & Risk Factors
Cerebral palsy is one of the commoner physical disabilities of childhood. Prevalence is higher after extreme prematurity and very low birth weight than after uncomplicated term birth. Risk clusters into antenatal, perinatal and postneonatal windows. Prematurity and white-matter injury, hypoxic–ischaemic encephalopathy, perinatal stroke, congenital infection, multiple birth, growth restriction and neonatal seizures all raise probability. A minority of cases are postneonatal after meningitis, trauma or other acquired early brain injury. [9] [16] [19]
High-risk infant follow-up clinics see a different denominator from community clinics. In follow-up, you start with elevated prior probability. In community practice, caregiver concern and asymmetric motor signs may be the first alert. Equity matters: rural distance, language barriers, fragmented records and poverty delay recognition and service entry. [12] [15] [16]
Pathophysiology
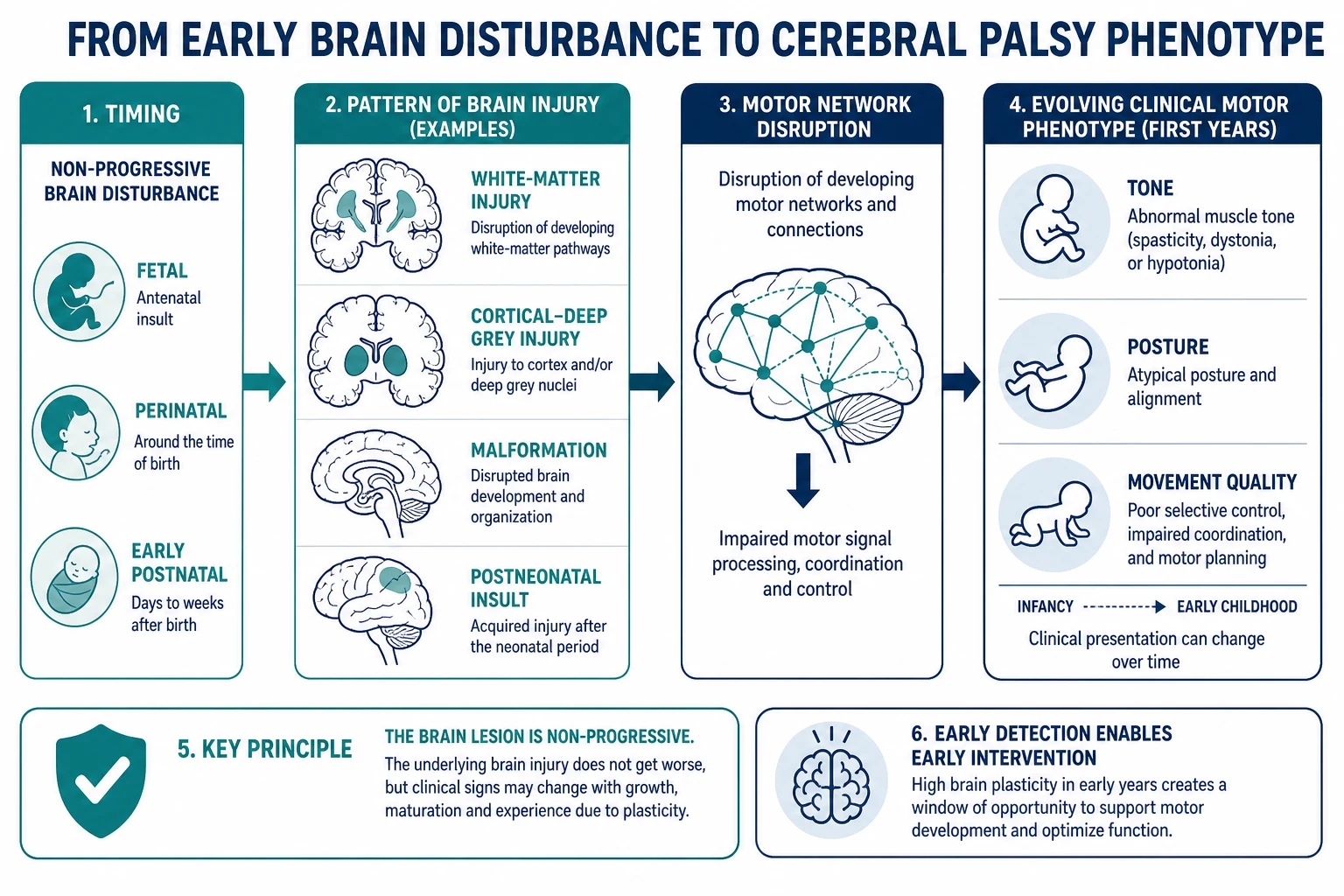
The key teaching point is timing. A disturbance in the developing brain — before birth, around birth, or in early infancy — disrupts motor networks. The original lesion does not keep expanding like a tumour or a degenerative storage disease. Growth, myelination and experience then shape how the motor phenotype looks at six months, two years and school entry. That is why early hypotonia can later show clear spasticity, and why classification is refined over time. [3] [18]
Broad MRI pattern groups help counselling and research. White-matter injury is common in preterm pathways. Cortical and deep grey injury appears after some term hypoxic or metabolic insults. Malformations reflect earlier developmental disruption. Postneonatal insults leave their own signatures. The MRICS framework organises MRI patterns for children with CP and supports more consistent communication about imaging. Imaging supports, but does not replace, the clinical diagnosis. [18]
Early detection matters because infancy is a period of high plasticity. Systematic reviews of motor interventions and enriched environments support the principle that active, goal-directed early therapy can improve motor outcomes compared with passive waiting. That is the biological and service rationale behind Novak’s early-detection push. [1] [13] [14]
General movements and neurological optimality scores sit on this pathway. Abnormal fidgety movements and low HINE scores raise the probability of later CP when interpreted by trained clinicians in context. They are not party tricks. They are structured observations of movement quality and neurological status. [10] [11] [20]
Clinical Presentation
Caregivers often notice first. Common phrases include “always fists,” “hates tummy time,” “only rolls one way,” “left hand is lazy,” “legs scissor when I pick him up,” or “she was floppy and now she is stiff.” Some children present from NICU follow-up with known risk and serial abnormal examinations. Others present late as a toe-walking preschooler who never crawled symmetrically. [1] [16]
Age colours the picture. In early infancy look for paucity of movement, persistent asymmetric tonic neck posture, tight popliteal angles, or a hand that never opens. Around the fidgety period (commonly discussed around three to five months corrected age), movement quality becomes especially informative for trained observers. Later in the first year, failure to sit with emerging arm support, early hand preference before it is developmentally expected, and delayed protective reactions raise concern. [1] [20]
Unilateral CP may show early hand neglect, asymmetric reach, or preferential fisting on one side. Bilateral spastic patterns often show lower-limb stiffness, toe pointing and delayed independent sitting or walking. Dyskinetic patterns may show fluctuating tone, grimacing and writhing postures that intensify with effort. Ataxic patterns show wide-based, poorly graded movements as skills emerge. [3] [9]
Differential Diagnosis
Hold two lists: common CP patterns and dangerous mimics. True progressive disease is the trap. New skill loss after a period of clear progress, continuously worsening weakness, rising creatine kinase, a strong neuromuscular family history, or multi-system disease should push you away from simple CP. Metabolic and genetic disorders can present with motor impairment; some need different urgent pathways. [19]
Separate global developmental delay without a clear early motor pattern of CP. Separate spinal lesions, peripheral neuropathies and myopathies when tone, reflexes and distribution do not fit a central pattern. Transient dystonia of prematurity and positional preference can worry families; serial examination and movement quality distinguish evolving CP from temporary patterns. Later in childhood, developmental coordination disorder is a different construct from early CP diagnosis. Autism may coexist with CP but does not explain spastic hemiparesis. [1] [19]
Clinical & Bedside Assessment
1. Start with risk and the story. Pregnancy, birth, gestation, NICU course, cooling for encephalopathy, imaging already done, seizures, meningitis, head injury, and the exact timeline of caregiver concern. Ask what the child can do at home: roll, sit, crawl, pull to stand, use both hands for toys, feed, communicate. [1] [12]
2. Watch spontaneous movement before you poke. Put the infant on a mat. Look for fluency, variability, symmetry, fidgety-quality movements in the right age window, and whether one limb is left out of the action. Formal General Movements Assessment requires training and standardised video methods. Even without formal certification, every paediatrician should recognise that stiff, cramped, monotone or highly asymmetric movement is not normal and needs expert review. [1] [20]
3. Examine tone, posture and reflexes with age in mind. Compare sides. Check axial versus limb tone. Look for persistent primitive reflexes and missing protective reactions. Test functional hand use with an age-right toy. Observe how the child is carried and dressed — real function hides in those minutes. [1] [10]
4. Use HINE when trained and available. The Hammersmith Infant Neurological Examination is a structured neurological exam used in early detection pathways. Low optimality scores, especially with risk history and abnormal movements, support a high-probability CP formulation. Scoring aids exist to support consistent early detection practice. Do not invent numeric cut-offs in a viva if you cannot defend the exact threshold from a source you know; describe the principle and local pathway. [10] [11]
5. Build a problem representation. Example: “Ex-28-week infant at four months corrected age with cramped general movements, asymmetric lower-limb tone, HINE suboptimal in a trained clinic, and MRI white-matter injury — high probability of bilateral spastic cerebral palsy; function still evolving.” [1] [18]
Investigations
Neuroimaging is central when it is not already done or when the clinical pattern is incomplete. MRI is preferred for pattern recognition in most modern pathways. MRICS-style pattern groups help teams speak a common imaging language. Timing depends on stability, sedation risk and whether results will change genetic testing, counselling or service access. A normal MRI does not completely exclude CP; a classic clinical syndrome can still stand. An unexpected progressive imaging pattern should reopen the differential. [1] [18]
Directed tests, not shotgun panels, follow atypical features: regression, dysmorphism, organomegaly, markedly elevated CK, or family history of neuromuscular disease. EEG follows seizure concern. Hearing and vision checks matter because sensory impairment changes developmental support. Genetic testing yield is rising in selected MRI and clinical patterns; use local neurology/genetics pathways rather than inventing a universal panel here. [18] [19]
Investigations that only delay therapy without changing near-term decisions are harmful delays. If probability is already high, start intervention while imaging and specialty review are arranged. [1] [12]
Management — Resuscitation
Most early-recognition visits are outpatient. Still, keep an emergency lens. A child with known or suspected CP can present with status epilepticus, aspiration, respiratory failure, acute severe dystonia, dehydration from feeding failure, or unexplained injury. Use ABCDE first. Treat seizures and hypoxia before classification debates. Consider non-accidental injury when the history and injuries do not fit. Safeguarding and disability care are not mutually exclusive. [1]
Management — Definitive & Stepwise
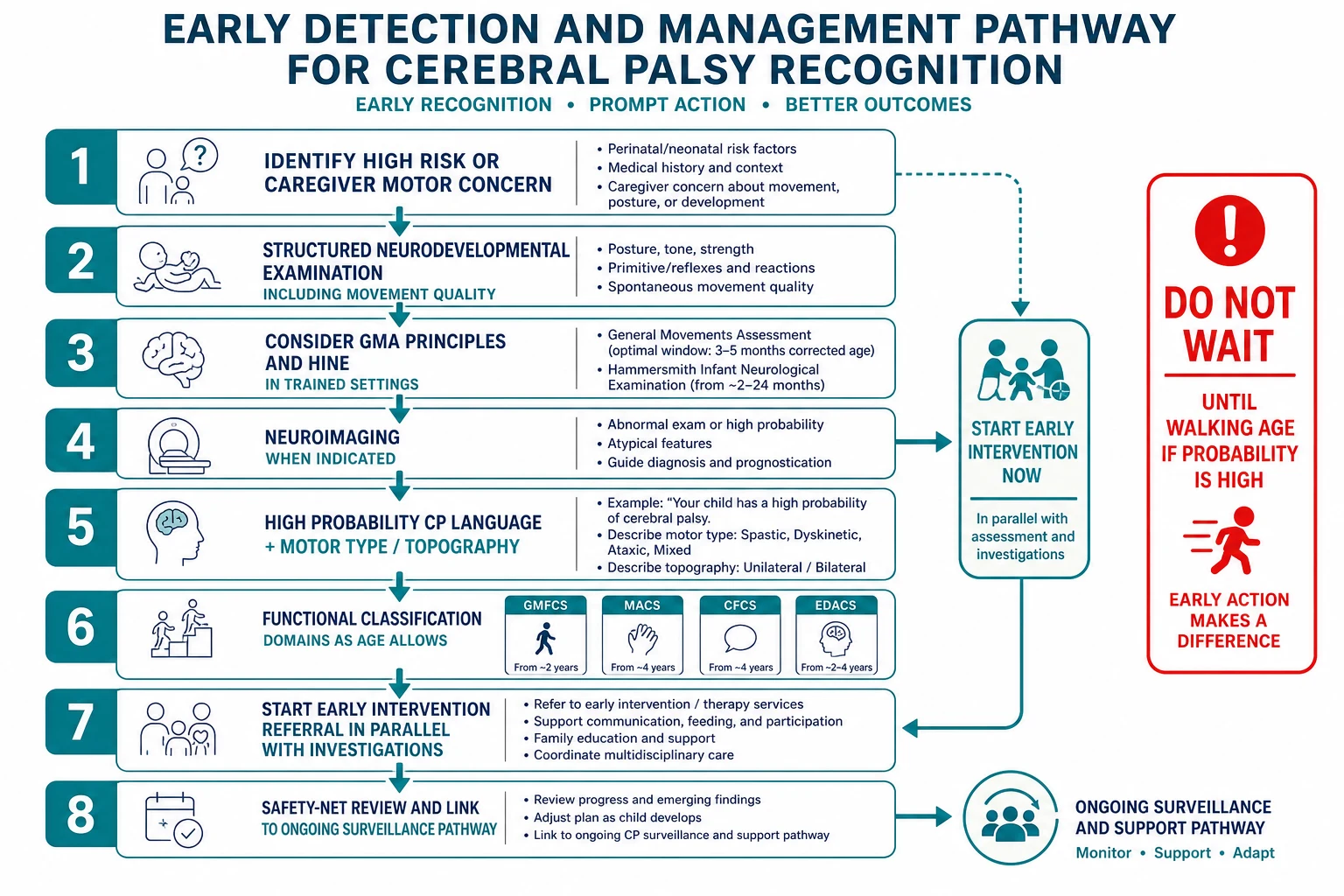
Novak and colleagues summarised the modern rule: earlier, more accurate diagnosis is possible when risk history, standardised neurological examination, neuroimaging and GMA are combined. Waiting until two years for “definite” CP wastes intervention time when probability is already high. Implementation work from early diagnosis clinics shows earlier median ages at diagnosis are achievable with acceptable family experience when pathways are organised. [1] [15] [16]
Step 1 — Name the probability. Use careful language: “high probability of cerebral palsy” when tools and history converge, and explain that labels refine with time. Do not over-promise cure. Do not under-call clear patterns. [1] [15]
Step 2 — Classify what you can today. Motor type and topography as far as the exam allows. Provisional functional descriptors with age caveats. GMFCS is more stable later; still, early functional language helps teams plan equipment and therapy goals without pretending false precision in a three-month-old. [4] [5] [17]
Step 3 — Open early intervention now. Physiotherapy and family-centred motor intervention should not wait for every test result. Evidence supports early motor intervention and enriched, active learning environments. Refer to local early childhood intervention, therapy services and, where relevant, neonatal follow-up or CP early-detection clinics. [1] [13] [14]
Step 4 — Write the plan. Imaging if needed, neurology/rehabilitation review, hearing and vision, social supports, interpreter if required, review interval, and clear safety-net advice. Hand over to the surveillance and multidisciplinary management pathway for hip surveillance, tone algorithms and long-term MDT care. [1] [12]
Specific Subtypes & Scenarios
Preterm graduate with abnormal fidgety movements. Corrected age, trained GMA, HINE, prior cranial imaging, and early therapy referral. Discuss bilateral spastic patterns as a common pathway without assuming final GMFCS yet. [1] [20]
Term HIE after cooling. Serial neurology, MRI pattern, evolving tone, seizure management, and honest prognostic uncertainty early with clear follow-up. [1] [18]
Early hand preference. Treat early strong hand preference as a warning, not a cute quirk. Look for unilateral upper-limb neglect, asymmetric reach and perinatal stroke patterns. [1]
Dyskinetic picture after deep grey injury. Fluctuating tone, involuntary postures, feeding and communication planning early; EDACS and CFCS thinking enter sooner than families expect. [7] [8] [18]
Late community “toe-walker”. Re-examine for upper motor neuron signs, perinatal history and alternative diagnoses. Mild bilateral CP is still CP and still needs accurate classification and support. [16]
Postneonatal CP. Date the insult. Rehabilitation still uses the same functional classification language. [19]
Rural family with interpreter needs. Use professional interpreting. Write plain-language plans. Do not let distance become “wait and see.” Telehealth can support follow-up but should not replace hands-on therapy access planning. [12] [15]
Complications & Pitfalls
- Waiting for independent walking before naming high-probability CP. [1] [16]
- Treating GMFCS as a single global severity number for hands, speech and eating. [6] [7] [8] [17]
- Assuming all unilateral CP is “mild.” Function must be observed. [4] [5]
- Missing progressive disease red flags. [19]
- Withholding intervention until imaging or genetics are perfect. [1] [13]
- Counselling without an interpreter when language discordance is present.
- Diagnostic overshadowing: attributing every new symptom to “just CP” without fresh thought. [17]
- Using classification labels as identity insults rather than planning tools. Speak about function with respect. [17]
Prognosis & Disposition
Early findings inform, but do not dictate, a single future. Many children with GMFCS I–II walk in the community with variable aids or speed. Higher GMFCS levels need more mobility support. Stability of GMFCS is better after early childhood than in young infants, so avoid false precision at three months. Associated epilepsy, vision impairment, intellectual disability and social supports shape quality of life as much as motor level alone. [4] [5] [3]
Disposition after first recognition: arrange early intervention, specialty review, imaging if needed, and a timed clinical review. Transfer ongoing surveillance tasks — hips, tone, growth, pain, equipment — to the multidisciplinary management pathway. Safety-net for seizures, breathing difficulty with feeds, unexplained deterioration and caregiver overwhelm. [1] [12]
Special Populations
NICU graduates need structured follow-up with corrected age, trained movement assessment and family support. Indigenous families need culturally safe conversations that name disability supports without racialised assumptions about parenting. Migrant and refugee families may lack birth records; work with what is known and still act on present findings. Children with medical complexity can have CP plus technology dependence; classification still helps teams plan. Co-existing autism or intellectual disability requires dual diagnostic honesty so neither motor nor behavioural needs are ignored. [12] [15] [17]
Evidence, Guidelines & Regional Differences
Novak 2017 is the landmark clinical synthesis that shifted practice toward early, tool-supported diagnosis and concurrent early intervention. Te Velde’s historical and implementation papers explain why diagnosis was late and how clinics can change that. Morgan’s reviews support early active motor intervention and environmental enrichment principles. Palisano, Eliasson, Hidecker and Sellers provide the core functional classification tools. SCPE and MRICS support surveillance and imaging communication. [1] [4] [5] [6] [7] [8] [9] [13] [14] [15] [16] [18]
Australian early-detection clinics and CP registers have operationalised earlier diagnosis pathways. Culturally safe care for Aboriginal and Torres Strait Islander families, and Te Tiriti-informed care in Aotearoa New Zealand, are service requirements. [15] [16]
UK practice routes high-risk infants through neonatal follow-up and neurodevelopmental services. Functional classification language is shared internationally even when service names differ. [1] [4]
US high-risk infant follow-up and developmental surveillance frameworks interact with early intervention systems; access varies by state and insurance. [1] [12]
Canadian pathways commonly combine paediatric neurology and rehabilitation services with GMFCS-centred planning. Family-facing GMFCS resources support counselling. [4] [5]
Controversies remain: exact age at which “definite” is required for every service; telehealth limits for formal GMA; and how aggressively to pursue genetics for every MRI-normal phenotype. State uncertainty honestly and still act on high probability. [1] [16] [19]
Exam Pearls
- CP = permanent motor disorder from non-progressive early brain disturbance; phenotype can still evolve. [2] [3]
- Early detection uses risk + exam/tools + imaging — not waiting for walking. [1]
- Motor type ≠ GMFCS. Hands = MACS. Talk = CFCS. Eating = EDACS. [4] [6] [7] [8]
- Assign functional levels from real-world performance; do not quiz parents for a letter grade. [5] [17]
- Abnormal fidgety movements and low HINE scores raise probability in trained hands. [10] [11] [20]
- Regression means rethink progressive disease. [19]
- Start early intervention when probability is high. [1] [13]
- Cross-link the management leaf for hip surveillance and advanced tone care.
References
- [1]Novak I Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA pediatrics, 2017.PMID 28715518
- [2]Bax M Proposed definition and classification of cerebral palsy, April 2005. Developmental medicine and child neurology, 2005.PMID 16108461
- [3]Rosenbaum P A report: the definition and classification of cerebral palsy April 2006. Developmental medicine and child neurology. Supplement, 2007.PMID 17370477
- [4]Palisano R Development and reliability of a system to classify gross motor function in children with cerebral palsy. Developmental medicine and child neurology, 1997.PMID 9183258
- [5]Palisano RJ Content validity of the expanded and revised Gross Motor Function Classification System. Developmental medicine and child neurology, 2008.PMID 18834387
- [6]Eliasson AC The Manual Ability Classification System (MACS) for children with cerebral palsy: scale development and evidence of validity and reliability. Developmental medicine and child neurology, 2006.PMID 16780622
- [7]Hidecker MJ Developing and validating the Communication Function Classification System for individuals with cerebral palsy. Developmental medicine and child neurology, 2011.PMID 21707596
- [8]Sellers D Development and reliability of a system to classify the eating and drinking ability of people with cerebral palsy. Developmental medicine and child neurology, 2014.PMID 24344767
- [9]Surveillance of Cerebral Palsy in Europe Surveillance of cerebral palsy in Europe: a collaboration of cerebral palsy surveys and registers. Developmental medicine and child neurology, 2000.PMID 11132255
- [10]Romeo DM Hammersmith Infant Neurological Examination in infants born at term: Predicting outcomes other than cerebral palsy. Developmental medicine and child neurology, 2022.PMID 35201619
- [11]Fehlings D The Hammersmith Infant Neurological Exam Scoring Aid supports early detection for infants with high probability of cerebral palsy. Developmental medicine and child neurology, 2024.PMID 38818710
- [12]Sutter EN Evidence-Based Infant Assessment for Cerebral Palsy: Diagnosis Timelines and Intervention Access in a Newborn Follow-up Setting. Journal of child neurology, 2024.PMID 39262331
- [13]Morgan C Effectiveness of motor interventions in infants with cerebral palsy: a systematic review. Developmental medicine and child neurology, 2016.PMID 27027732
- [14]Morgan C Enriched environments and motor outcomes in cerebral palsy: systematic review and meta-analysis. Pediatrics, 2013.PMID 23958771
- [15]Te Velde A Age of Diagnosis, Fidelity and Acceptability of an Early Diagnosis Clinic for Cerebral Palsy: A Single Site Implementation Study. Brain sciences, 2021.PMID 34439692
- [16]te Velde A Early Diagnosis and Classification of Cerebral Palsy: An Historical Perspective and Barriers to an Early Diagnosis. Journal of clinical medicine, 2019.PMID 31623303
- [17]Rosenbaum P Classification in childhood disability: focusing on function in the 21st century. Journal of child neurology, 2014.PMID 24810083
- [18]Himmelmann K MRI classification system (MRICS) for children with cerebral palsy: development, reliability, and recommendations. Developmental medicine and child neurology, 2017.PMID 27325153
- [19]Smithers-Sheedy H What constitutes cerebral palsy in the twenty-first century? Developmental medicine and child neurology, 2014.PMID 24111874
- [20]Einspieler C Are abnormal fidgety movements an early marker for complex minor neurological dysfunction at puberty? Early human development, 2007.PMID 17129688