Paeds · growth-development-and-behaviour
Cerebral palsy: surveillance and multidisciplinary management
Also known as CP surveillance · Cerebral palsy multidisciplinary care · GMFCS hip surveillance · Neurodisability medical home CP · Cerebral palsy comorbidity screening
Fellowship guide to lifelong cerebral palsy surveillance and multidisciplinary management: functional classification, hip and comorbidity surveillance, tone and motor interventions, medical-home coordination, transition and exam defence — cross-linked to early recognition without cloning it.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A seven-year-old with bilateral spastic cerebral palsy rolls into clinic in a wheelchair. The parent asks whether the hips are “still OK,” whether botulinum toxin is due, and why school says fine-motor work is falling behind. Your job today is not to re-diagnose CP from scratch. Your job is surveillance and multidisciplinary management: functional classification, prevention of secondary harm, coordinated therapy, and a plan the family can use. [1] [18]
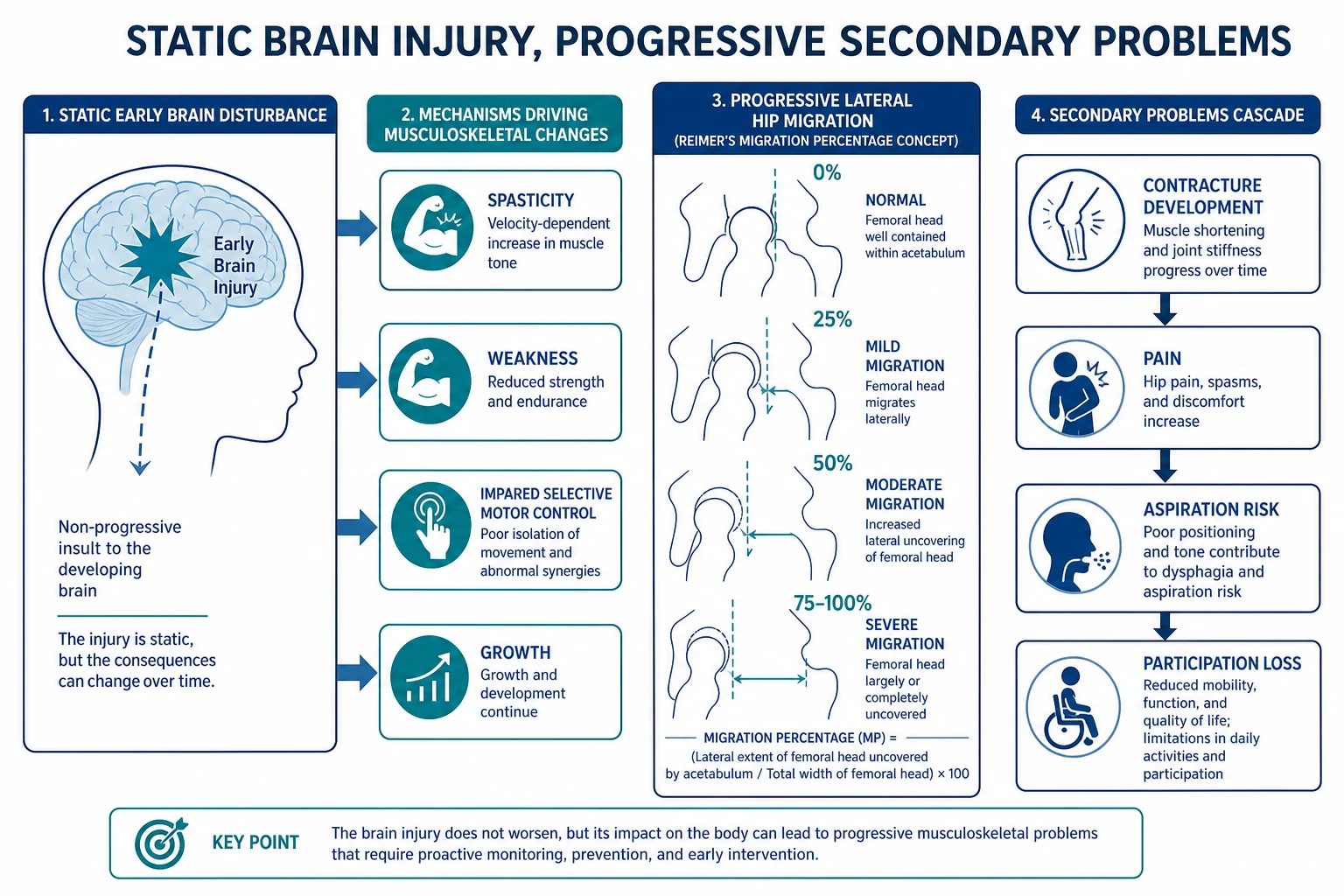
The consensus definition still anchors the viva. Cerebral palsy describes permanent disorders of the development of movement and posture, causing activity limitation, that are attributed to non-progressive disturbances in the developing fetal or infant brain. The motor disorder is often accompanied by disturbances of sensation, perception, cognition, communication and behaviour, by epilepsy, and by secondary musculoskeletal problems. [1]
That last clause is the surveillance engine. The brain injury does not “progress like a tumour,” but the hips, spine, nutrition, airways and participation can deteriorate if nobody is watching. First diagnosis, neuroimaging patterns and early detection tools live on the sibling early-recognition page. This leaf owns what happens after the label is on the chart. [1] [15]
Classification
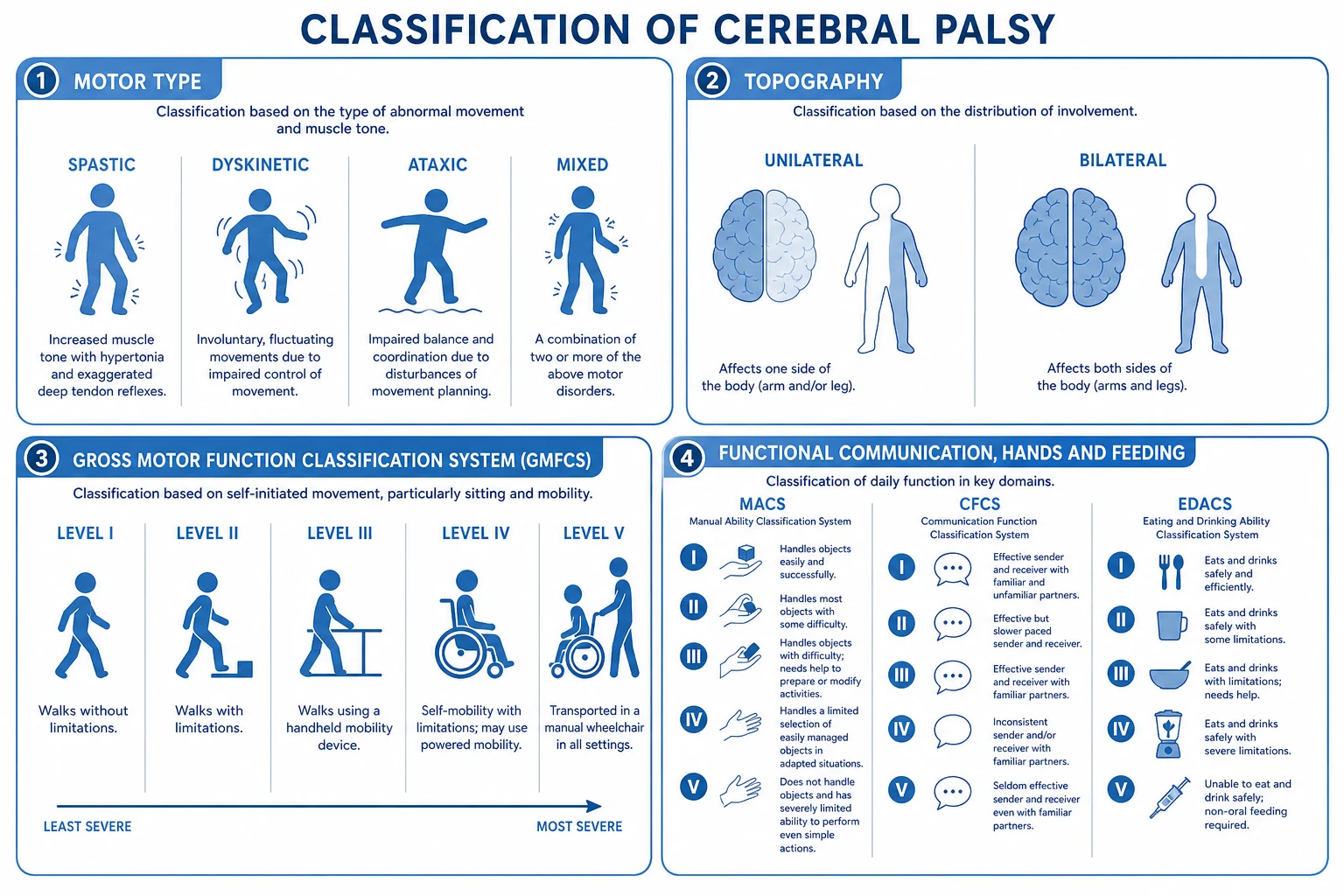
Start every case with three layers: motor type, topography, and function. Motor type is spastic, dyskinetic (dystonia/choreoathetosis), ataxic or mixed. Topography is unilateral or bilateral. Function is how the child moves, uses hands, communicates and eats in daily life. Examiners punish candidates who only say “spastic diplegia” and stop. [1] [3]
GMFCS (Gross Motor Function Classification System) levels I–V describe self-initiated movement with emphasis on sitting, walking and wheeled mobility. Expanded and revised descriptors improve content validity across ages. Rough clinical language for the viva: I walks without limitation; II walks with limitations; III walks using a hand-held mobility device; IV self-mobility with limitations, often powered mobility; V transported in a manual wheelchair. Recheck as the child grows; the level is usually relatively stable after early childhood but the equipment and goals change. [3] [4]
MACS classifies how children with CP handle objects in daily activities (I handles objects easily and successfully through V does not handle objects). CFCS classifies everyday communication effectiveness with familiar and unfamiliar partners (I effective with all partners through V seldom effective even with familiar partners). EDACS classifies eating and drinking ability by safety and efficiency (I eats and drinks safely and efficiently through V unable to eat or drink safely — tube feeding may be considered). Use the scale that matches the problem in front of you. [5] [6] [7]
Functional scales — what each answers
- Gross motor mobility I–V
- Drives hip surveillance intensity
- Frames equipment and therapy goals
- Hand use in daily activities
- Guides OT and school fine-motor plans
- Independent of walking level
- CFCS: everyday communication partners
- EDACS: safety and efficiency of eating/drinking
- Both flag AAC, speech and feeding pathways
Epidemiology & Risk Factors
Global analyses place cerebral palsy among the commonest physical disabilities of childhood. McIntyre and colleagues synthesised population data and reported a global birth prevalence on the order of about 1.6 per 1000 live births in recent high-quality estimates, with higher rates in some lower-resource settings and in high-risk neonatal populations. Use the paper’s figures in exam answers rather than memorised local folklore. [2]
Risk clusters include extreme prematurity, neonatal encephalopathy, perinatal stroke, congenital anomalies and post-neonatal brain injury. Service need is not uniform: children at GMFCS IV–V carry the highest rates of hip displacement, respiratory admission, tube feeding and medical complexity. Low weight on CP-specific growth interpretation associates with higher morbidity and mortality. Equity gaps — rural distance, racism, language discordance, poverty — turn good guidelines into missed radiographs and open-loop referrals. [2] [8] [20] [22]
Pathophysiology
The primary lesion interrupts descending motor pathways and central motor networks. What the child then experiences is a mix of spasticity, weakness, impaired selective motor control, dystonia, ataxia and sensory-motor learning limits. Growth multiplies the problem. Muscles that cannot lengthen with bone create contracture. Persistent adductor and iliopsoas tone with delayed weight-bearing lets the femoral head migrate laterally. Migration percentage on an AP pelvis film is the practical radiographic language of that process. Higher GMFCS means less stable hip biomechanics and higher displacement risk. [1] [8]
Dystonia is not “worse spasticity.” It is fluctuating, often triggerable involuntary muscle contraction that can cause severe posturing and pain. Treating pure dystonia with a pure spasticity script fails. Feeding pathophysiology runs through oromotor incoordination, delayed swallow, gastro-oesophageal reflux and weak cough — EDACS makes that risk visible. Respiratory morbidity follows aspiration, low lung volumes, scoliosis and poor secretion clearance. Pain and sleep debt raise tone; raised tone worsens pain. The ICF model keeps you honest: body structure problems only matter if they change activity and participation. [7] [17]
Clinical Presentation
Surveillance clinics see phenotypes, not textbooks. A GMFCS II school-age child may walk into the room, trip on uneven ground, and struggle with handwriting fatigue. A GMFCS III child may use a walker outdoors and show progressive crouch or equinus. A GMFCS IV–V child may be non-ambulant, dependent for transfers, and at high hip and respiratory risk even when smiling and interactive. [3] [4]
Hip disease can be silent until late. Reduced abduction, asymmetric thigh creases, pelvic obliquity or a rising migration percentage may precede pain. Dystonic storms present with sustained posturing, sweating and distress that parents distinguish from “usual stiffness.” Feeding problems present as long meal times, coughing with liquids, chestiness after feeds or falling off the growth curve. Pain may present only as night waking, tone spikes or school refusal. Families may present with burnout and a bag of uncoordinated appointments. Adolescents may present when paediatric services stop and adult services have not started. [8] [18] [21]
Differential Diagnosis
Not every change in a child with CP is “just CP.” [1] [20]
- True secondary musculoskeletal progression versus a progressive neurological disease with skill loss — regression is a red flag, not a shrug. [1]
- Hip displacement pain versus fracture, septic arthritis, appendicitis or severe constipation in a non-verbal child. [8]
- Spasticity-dominant versus dystonia-dominant versus mixed tone — wrong label, wrong intervention. [17]
- Epileptic events versus dystonic movements, reflux sandifer-type posturing or medication effects. [17]
- Aspiration versus viral LRTI versus cardiac failure in technology-dependent children. [20]
- Behaviour change from pain, sleep debt, bullying, anxiety or hearing/vision loss. [18]
- Faltering growth from oromotor dysfunction versus inadequate offered calories versus endocrine disease or neglect. [22]
- Equipment or seating failure masquerading as “worsening tone.” [18]
Clinical & Bedside Assessment
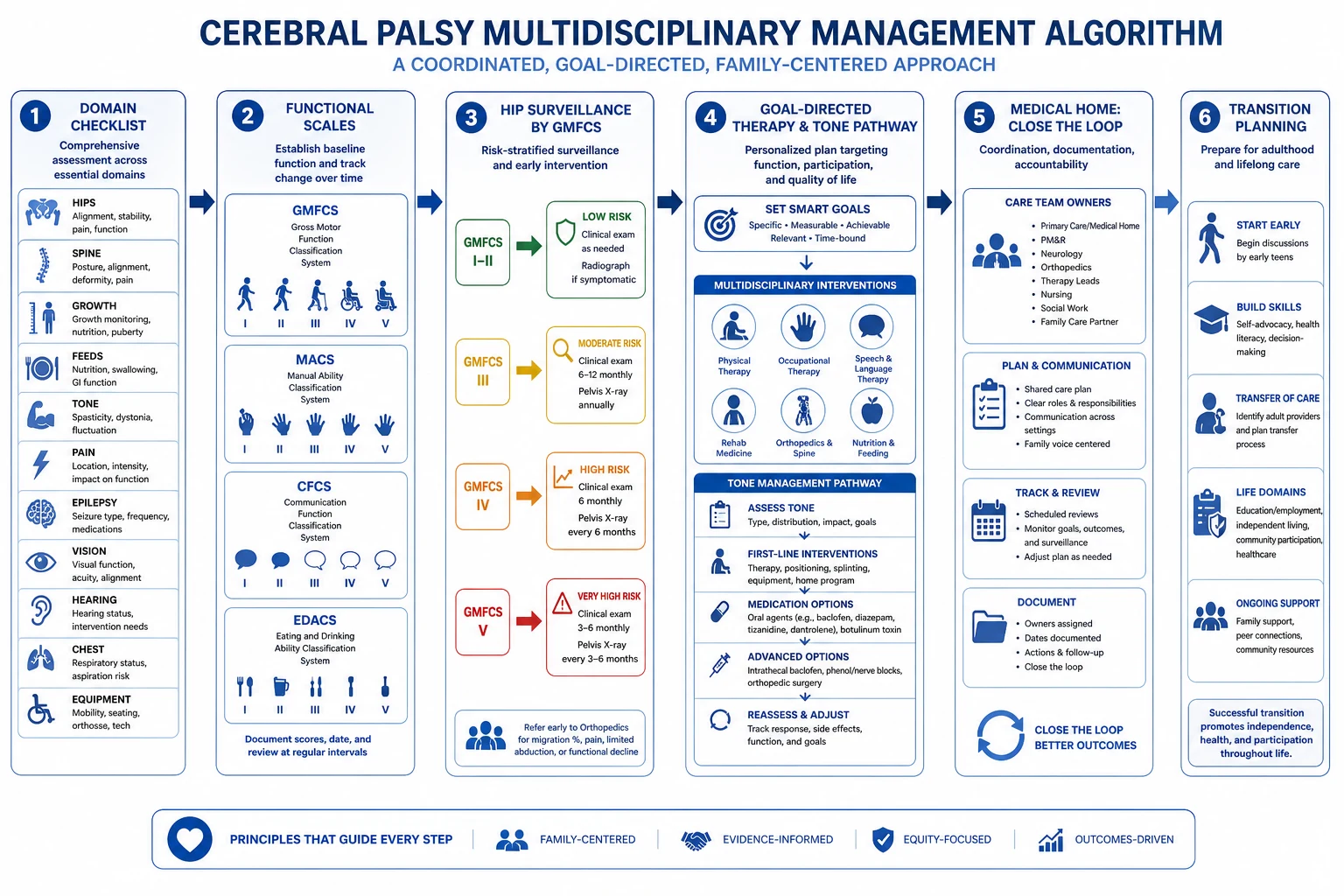
Run a domain checklist every visit. Ask about function at home and school, pain, sleep, seizures, feeding and chest symptoms, continence, skin, equipment and caregiver load. Assign or recheck GMFCS, and add MACS, CFCS and EDACS when hands, talk or meals are the issue. Examine posture, range, selective motor control, hip abduction, spinal curve in sitting, skin over pressure points, and respiratory effort. Watch a transfer or a few steps if safe. Observe communication with the parent and with you. [3] [5] [6] [7] [18]
Do not let the wheelchair become a diagnostic blindfold. Look for treatable medical disease. Document a usable problem list: “GMFCS IV bilateral spastic CP; hips under surveillance; epilepsy on two agents; EDACS III; goals — pain-free sitting and school attendance.” That sentence is more valuable than a paragraph of tone adjectives. [18] [20]
Investigations
Investigations serve decisions. Hip surveillance radiographs are the signature test for non-ambulant and high-risk children. Soo showed displacement risk rises with GMFCS level. Population programmes such as Hägglund’s Swedish model show that structured surveillance plus timely surgery can prevent dislocation at scale. Australian hip surveillance guidelines (Wynter five-year review; Gibson ten-year update) stratify frequency by GMFCS and age — use the current local protocol ages and migration-percentage action thresholds rather than inventing numbers in the viva. [8] [9] [10] [11]
Consider swallow assessment when EDACS or history suggests unsafe feeding. Review bone health when fractures, severe immobility or chronic anticonvulsants feature. Repeat vision and hearing when communication or learning changes. EEG belongs to seizure characterisation, not to “routine CP bloods.” Avoid low-value panels in stable ambulatory children without red flags. CP-specific growth charts (Brooks) help interpret low weight against peers with similar motor severity, but they do not replace clinical judgement about intake and illness. [7] [22]
Management — Resuscitation
Most CP care is longitudinal, but some presentations are time-critical. [17] [20]
- Airway and breathing first — severe dystonic crisis, status epilepticus, or aspiration with respiratory failure. Support oxygen, positioning, suction and senior help. [17] [20]
- Stop the driver — treat pain, fever, constipation or equipment failure that is fuelling dystonia or distress. [17]
- Suspect surgical emergencies in non-verbal children with unexplained pain — hips, abdomen, fracture. [8]
- Escalate early to PICU, neurology, orthopaedics or retrieval when the trajectory is wrong. [20]
- Transfer a map — GMFCS, airway risks, feed route, seizure plan, allergies, goals of care and parent contact. [19] [20]
Clinic is not the place to finish a form while a child is tiring. [20]
Management — Definitive & Stepwise
Build a surveillance calendar by age and GMFCS. Pair it with a goal list the family owns. Therapy should be goal-directed and activity-based. Novak’s systematic reviews and the 2019 traffic-light update support interventions that train real tasks and motor learning; many passive or non-specific modalities sit on yellow or red lights. Early intervention principles for infants at high risk are detailed in Morgan 2021 and on the early-recognition sibling — do not delay supports waiting for perfect labels. [12] [13] [15] [16]
Tone pathway. Optimise seating, orthoses, sleep and pain first. Use focal botulinum toxin for focal goals (for example equinus interfering with brace use or hygiene) within specialist protocols; historical RCTs such as Koman’s equinus work support neuromuscular blockade as a tool, not a lifestyle. Systemic antispasticity medicines and dystonia agents need specialist oversight because sedation and tone trade-offs are real. Intrathecal baclofen and selective dorsal rhizotomy are tertiary pathway decisions for selected children — refer with clear goals rather than inventing selection scores. Fehlings reviews dystonia options and highlights limited high-quality comparative evidence for many agents. [12] [13] [17]
Hip and spine pathway. Follow local hip surveillance schedules; act on rising migration and clinical change with orthopaedic referral before dislocation. Scoliosis needs seating review and orthopaedic input when curves progress or seating fails. [9] [10] [11]
Nutrition, airway, epilepsy, senses. Treat faltering growth as a medical problem. Discuss gastrostomy when oral feeding is unsafe or unacceptably burdensome — values-based, not purely radiographic. Plan chest physiotherapy, vaccination and early antibiotics pathways for high-risk children. Keep epilepsy plans current. Recheck vision and hearing. Dental care and constipation management prevent crises. [18] [22]
Coordination. The medical home holds the map: who owns hips, who owns tone, who owns school supports, when the next radiograph is due. Turchi and Liptak frame family-centred coordination; Kuo frames medical complexity. Start transition planning in early adolescence using White’s medical-home transition principles. [18] [19] [20] [21]
One surveillance visit — practical sequence
Confirm wellbeing and red flags; convert if unstable
Update function: GMFCS ± MACS/CFCS/EDACS and participation goals
Domain screen: hips/spine, growth/feeds, tone/pain, seizures, vision/hearing, chest, skin, equipment
Act: imaging or referral due; therapy goals; medication review
Close loops: owners, dates, safety-net, school communication
Specific Subtypes & Scenarios
GMFCS I–II unilateral CP. Prioritise bimanual hand function, constraint or intensive upper-limb programmes when goals are clear, orthoses for equinus, school access and sports participation. Hip risk is lower than non-ambulant peers but not zero if function changes. [5] [12]
GMFCS III. Watch gait efficiency, knee and ankle alignment, fatigue and equipment. Therapy and orthopaedics share crouch and lever-arm decisions. [3]
GMFCS IV–V. Hip surveillance is non-negotiable. Seating, pain, nutrition, secretion management and carer support dominate. Respiratory admission risk is high — plan early. [8] [9] [10]
Dyskinetic CP. Separate dystonia from spasticity. Avoid serial pure antispasticity escalation. Use Fehlings-informed specialist pathways and aggressive pain/sleep care. [17]
Unsafe swallow. EDACS guides urgency. Involve speech pathology early; discuss texture modification versus tube feeding with family values on the table. [7]
Rural or language-discordant care. Bring imaging and therapy to the child when possible; use professional interpreters; write one shared plan that travels. [19]
Adolescent transition. Inventory skills, legal decision-making, adult neurology/rehab/GP, equipment funding and sexual health. Start years before the birthday cliff. [21]
Complications & Pitfalls
- Missing silent hip migration until painful dislocation. [8] [9]
- Labelling dystonia as spasticity and escalating the wrong drugs. [17]
- Open-loop referrals — therapy or radiographs ordered with no review date. [19]
- Diagnostic overshadowing: sepsis, fracture or constipation called “behaviour.” [20]
- Unfocused botulinum toxin without a functional goal. [12]
- Ignoring nutrition until fracture or repeated infection. [22]
- Equating GMFCS with IQ.
- No transition plan. [21]
- Inventing hip cut-offs or toxin units not in the local protocol.
Prognosis & Disposition
GMFCS after early childhood is relatively informative for mobility counselling, though goals still change with growth and environment. Novak’s prognostic messages paper is examinable: many children walk, many have pain, many have comorbidities, and families need honest, specific counselling rather than vague reassurance. Structured hip programmes reduce dislocation. Mortality and high hospital use concentrate in non-ambulant children with respiratory, epilepsy and nutritional complexity. [9] [14] [22]
Disposition is usually outpatient medical-home plus therapy networks. Admit or refer urgently for respiratory failure, status dystonicus, uncontrolled seizures, suspected surgical emergencies or safeguarding. After every visit, safety-net what would make the family return sooner: new pain, chestiness, feed refusal, seizure cluster, equipment failure. [18] [20]
Special Populations
Infants after early diagnosis need early intervention intensity and first hip plans as they approach the ages in local protocols. Preschool years are rich for motor learning and communication systems. School age adds learning, peer inclusion and fatigue. Adolescents need transition, mental health and autonomy supports. Technology-dependent children need CMC-level coordination. Indigenous, rural and refugee families need culturally safe, interpreter-supported pathways that do not assume transport and leave are free. Out-of-home care needs aggressive record reconstruction so surveillance ages are not missed. [15] [16] [20] [21]
Evidence, Guidelines & Regional Differences
Rosenbaum’s definition remains the conceptual spine. Functional classification rests on Palisano (GMFCS), Eliasson (MACS), Hidecker (CFCS) and Sellers (EDACS). Hip prevention evidence is strongest from population surveillance plus timely surgery (Hägglund) and from risk stratification by GMFCS (Soo), operationalised in Australian hip surveillance guidance (Wynter, Gibson). Novak’s traffic-light reviews are the standard viva language for “what works.” Morgan 2021 guides early intervention for high-risk infants. Liptak, Turchi, Kuo and White cover medical home, complexity and transition. Brooks growth charts inform nutrition risk. [1] [3] [8] [9] [10] [13] [16] [18] [21] [22]
Australian hip surveillance guidelines are a core local standard — schedule by GMFCS and age, act on migration trends, and link to orthopaedics before dislocation. Disability supports often run through national funding schemes; the clinician still owns clinical surveillance even when therapy is externally funded. [10] [11]
Controversies that examiners enjoy: who is a good SDR or ITB candidate; how intensive early therapy must be; when gastrostomy is “too early” versus “too late”; how aggressively to treat radiographic hip migration in a pain-free child. Answer with goals, evidence colour and family values — not slogans. [12] [13] [17]
Exam Pearls
- Always state type + topography + GMFCS (add MACS/CFCS/EDACS when relevant). [1] [3]
- Brain lesion static; hips and contractures can progress. [8]
- Hip risk climbs with GMFCS; IV–V means structured radiographic surveillance. [8] [10]
- Migration percentage is the film language; local guideline ages and thresholds are the action language. [10] [11]
- Spasticity ≠ dystonia. [17]
- Green-light therapies train real activities; many passive therapies are weak. [12] [13]
- Pain, constipation, reflux and dental disease drive “behaviour.”
- GMFCS is not IQ.
- Medical home closes loops; transition starts early. [18] [21]
- Regression means rethink the diagnosis. [1]
References
- [1]Rosenbaum P A report: the definition and classification of cerebral palsy April 2006. Developmental medicine and child neurology. Supplement, 2007.PMID 17370477
- [2]McIntyre S Global prevalence of cerebral palsy: A systematic analysis. Developmental medicine and child neurology, 2022.PMID 35952356
- [3]Palisano R Development and reliability of a system to classify gross motor function in children with cerebral palsy. Developmental medicine and child neurology, 1997.PMID 9183258
- [4]Palisano RJ Content validity of the expanded and revised Gross Motor Function Classification System. Developmental medicine and child neurology, 2008.PMID 18834387
- [5]Eliasson AC The Manual Ability Classification System (MACS) for children with cerebral palsy: scale development and evidence of validity and reliability. Developmental medicine and child neurology, 2006.PMID 16780622
- [6]Hidecker MJ Developing and validating the Communication Function Classification System for individuals with cerebral palsy. Developmental medicine and child neurology, 2011.PMID 21707596
- [7]Sellers D Development and reliability of a system to classify the eating and drinking ability of people with cerebral palsy. Developmental medicine and child neurology, 2014.PMID 24344767
- [8]Soo B Hip displacement in cerebral palsy. The Journal of bone and joint surgery. American volume, 2006.PMID 16391257
- [9]Hägglund G Prevention of dislocation of the hip in children with cerebral palsy: 20-year results of a population-based prevention programme. The bone & joint journal, 2014.PMID 25371472
- [10]Wynter M Australian hip surveillance guidelines for children with cerebral palsy: 5-year review. Developmental medicine and child neurology, 2015.PMID 25846730
- [11]Gibson N Australian hip surveillance guidelines at 10 years: New evidence and implementation. Journal of pediatric rehabilitation medicine, 2022.PMID 35311729
- [12]Novak I A systematic review of interventions for children with cerebral palsy: state of the evidence. Developmental medicine and child neurology, 2013.PMID 23962350
- [13]Novak I State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Current neurology and neuroscience reports, 2020.PMID 32086598
- [14]Novak I Clinical prognostic messages from a systematic review on cerebral palsy. Pediatrics, 2012.PMID 23045562
- [15]Novak I Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA pediatrics, 2017.PMID 28715518
- [16]Morgan C Early Intervention for Children Aged 0 to 2 Years With or at High Risk of Cerebral Palsy: International Clinical Practice Guideline Based on Systematic Reviews. JAMA pediatrics, 2021.PMID 33999106
- [17]Fehlings D Pharmacological and neurosurgical interventions for managing dystonia in cerebral palsy: a systematic review. Developmental medicine and child neurology, 2018.PMID 29405267
- [18]Liptak GS Providing a primary care medical home for children and youth with cerebral palsy. Pediatrics, 2011.PMID 22042817
- [19]Turchi RM Patient- and family-centered care coordination: a framework for integrating care for children and youth across multiple systems. Pediatrics, 2014.PMID 24777209
- [20]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [21]White PH Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home. Pediatrics, 2018.PMID 30348754
- [22]Brooks J Low weight, morbidity, and mortality in children with cerebral palsy: new clinical growth charts. Pediatrics, 2011.PMID 21768315