Paeds · growth-development-and-behaviour
Children with developmental disability in acute care
Also known as Disability-aware emergency care · Diagnostic overshadowing paediatrics · Hospital care autism intellectual disability · r-FLACC acute care · Reasonable adjustments paediatric ED
Fellowship approach to children with developmental disability in ED and hospital: avoid diagnostic overshadowing, use caregiver baseline and hospital passports, apply reasonable adjustments, assess pain with adapted tools, and manage medical complexity safely.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A non-verbal 7-year-old with intellectual disability arrives restless, hitting their head, heart rate 150. The triage note says “behavioural.” The parent says, “He only does this when his ear hurts.” That parent sentence is often more valuable than the first set of bloods. [4] [8]
Developmental disability here means enduring conditions that affect cognition, communication, motor control or adaptive function — autism, intellectual developmental disorder, cerebral palsy, and complex neurodisability, alone or combined. Acute care means ED, ward, retrieval and ICU moments when systems are noisy and time is short. [3] [6]
Diagnostic overshadowing means staff attribute symptoms to the disability itself and stop looking for a medical cause. It is a common, examinable failure mode and a real driver of inequality for people with learning disabilities in emergency settings. [6]
Reasonable adjustments are practical changes that make care accessible: quieter space, fewer staff, longer time, visual schedules, familiar carer present, and communication supports. They are clinical quality, not optional kindness. [3] [4]
Classification
Separate four acute-care problem clusters so you do not mix them up. [3] [6]
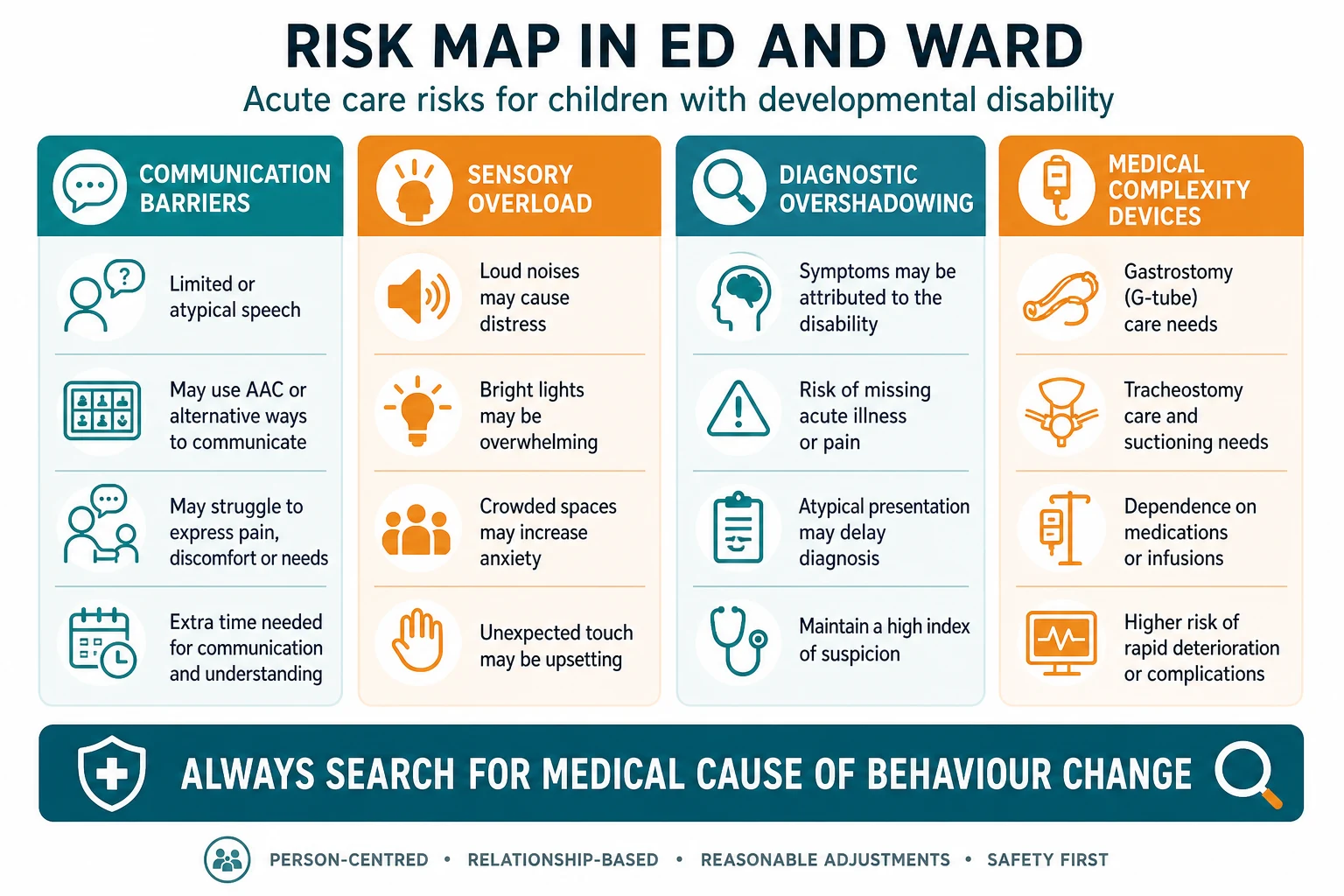
- Communication barriers — limited speech, AAC devices, delayed processing. [3]
- Sensory overload — lights, noise, touch, waiting. [3] [4]
- Diagnostic overshadowing — disability used as the whole explanation. [6]
- Medical complexity — devices, polypharmacy, multi-organ disease. [6]
Hospital passports and communication profiles classify how this child shows pain, fear and consent — not the diagnosis alone. Use them early. [3] [4]
Epidemiology & Risk Factors
Children with autism and other developmental disabilities use emergency services frequently. Australian parent surveys describe long waits, sensory distress, and difficulty having pain recognised. These are system problems, not family failures. [4]
People with learning disabilities experience well-documented health inequalities in emergency care, including delayed recognition of serious illness. Paediatric teams must assume risk is higher, not lower. [6]
Pain under-recognition is a specific hazard when children cannot self-report. Observational tools such as revised FLACC (r-FLACC) improve reliability in cognitive impairment compared with untrained guesswork. Systematic reviews continue to support structured behavioural tools for non-verbal and autistic children. [1] [2] [5] [8]
Risk is higher with incomplete carers (out-of-home care), remote retrieval, language barriers, and overnight staffing. Equity is part of the clinical plan. [4] [6]
Pathophysiology
Disability does not remove pain pathways. It changes expression. A child may rock, freeze, self-injure, become quiet, or become aggressive when in pain. Staff who expect adult verbal report will miss the signal. [8] [5]
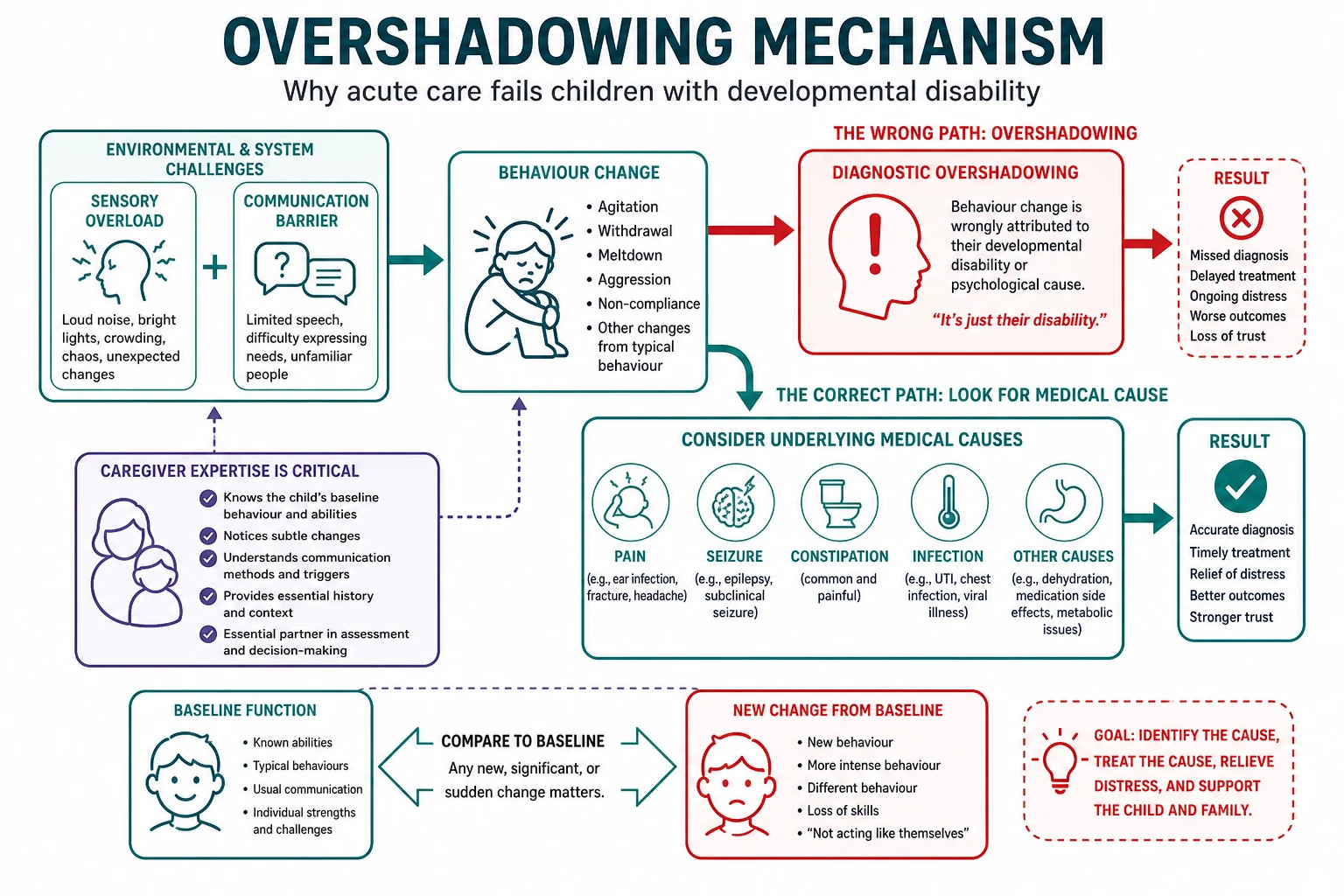
Acute environments push sensory systems hard. Noise and touch raise arousal. Raised arousal looks like “non-compliance,” which then triggers more restraint and more distress — a loop. Breaking the loop is clinical management. [3] [4]
Diagnostic overshadowing is a cognitive bias: once the disability label is activated, alternative hypotheses shrink. The physiological truth may be otitis, fracture, constipation, UTI, shunt failure or evolving sepsis. [6]
Clinical Presentation
- “Meltdown after three-hour wait.” [3] [4]
- “More irritable for 24 hours, not eating.” [6]
- “Self-injury started today.” [8]
- “Seizure-like episode, harder to assess because of baseline movements.” [6]
- “Parents brought the hospital passport and a favourite toy — use both.” [3] [4]
Subtle presentations: a usually active child who is still; a child with CP whose “tone is different today”; a technology-dependent child with subtle work of breathing. Caregiver concern is a red flag, not colour commentary. [6]
Differential Diagnosis
When behaviour changes, run a medical shortlist before you accept a primary behavioural label. [6] [8]
- Pain: ear, throat, teeth, abdomen, fracture, headache, pressure injury.
- Infection and sepsis.
- Constipation and urinary retention.
- Seizure, post-ictal state, encephalopathy.
- Shunt malfunction, gastrostomy dislodgement, tracheostomy problem.
- Medication effects, withdrawal, electrolyte disturbance.
- Safeguarding injury.
- Escalation from sensory overload alone — only after medical causes are reasonably excluded. [3] [6]
Clinical & Bedside Assessment
Start with PAT/ABCDE. Disability never cancels airway threat, hypoxia or shock. [6]
Then add the disability-aware layer: [3] [4]
- Who knows this child best today? [4]
- What is baseline communication, mobility, feeding, seizure pattern? [3]
- What does pain look like for them? [1] [8]
- What triggers and soothes them? [3]
- Devices, allergies, difficult airway, previous failed procedures? [6]
- Any safeguarding concerns? [6]
Examine with consent, prediction and one step at a time. Offer choices when safe (“arm first or ear first?”). Keep the familiar carer in view unless they prefer otherwise. [3]
Five-minute disability-aware assessment
Threat scan
ABC, glucose, seizure, anaphylaxis — same as any child.
Passport + caregiver
Baseline, pain signs, triggers, devices.
Environment
Quieter bay, fewer voices, dim lights if safe.
Pain score
r-FLACC or known tool; treat and reassess.
Medical hunt
Ear, abdomen, urine, chest, devices, neuro change.
Plan aloud
Predict next steps; avoid surprise procedures.
Investigations
Order tests for the medical differential, not because the child has a disability. New behaviour change plus systemic signs often needs glucose, infection evaluation and targeted imaging. Plan sensory load for bloods and imaging; batch procedures; use topical anaesthesia and distraction. [6] [8]
If restraint or procedural sedation is needed, document least-restrictive attempts first and use local paediatric sedation standards. Do not “just hold them down” as the plan. [3]
Management — Resuscitation
Life threats first: airway positioning (mind tone and secretions in neurodisability), oxygen, seizure control, fluid resuscitation, anaphylaxis pathway, haemorrhage control. Use an accurate weight — many families know dry weight from clinic. [6]
Give analgesia early once life threats are addressed. Pain itself drives escalation. Observational tools guide dosing and reassessment when self-report is impossible. [1] [2] [5]
De-escalate environment in parallel with medical care: fewer people, soft voices, one speaker, preferred sensory items. [3]
Management — Definitive & Stepwise
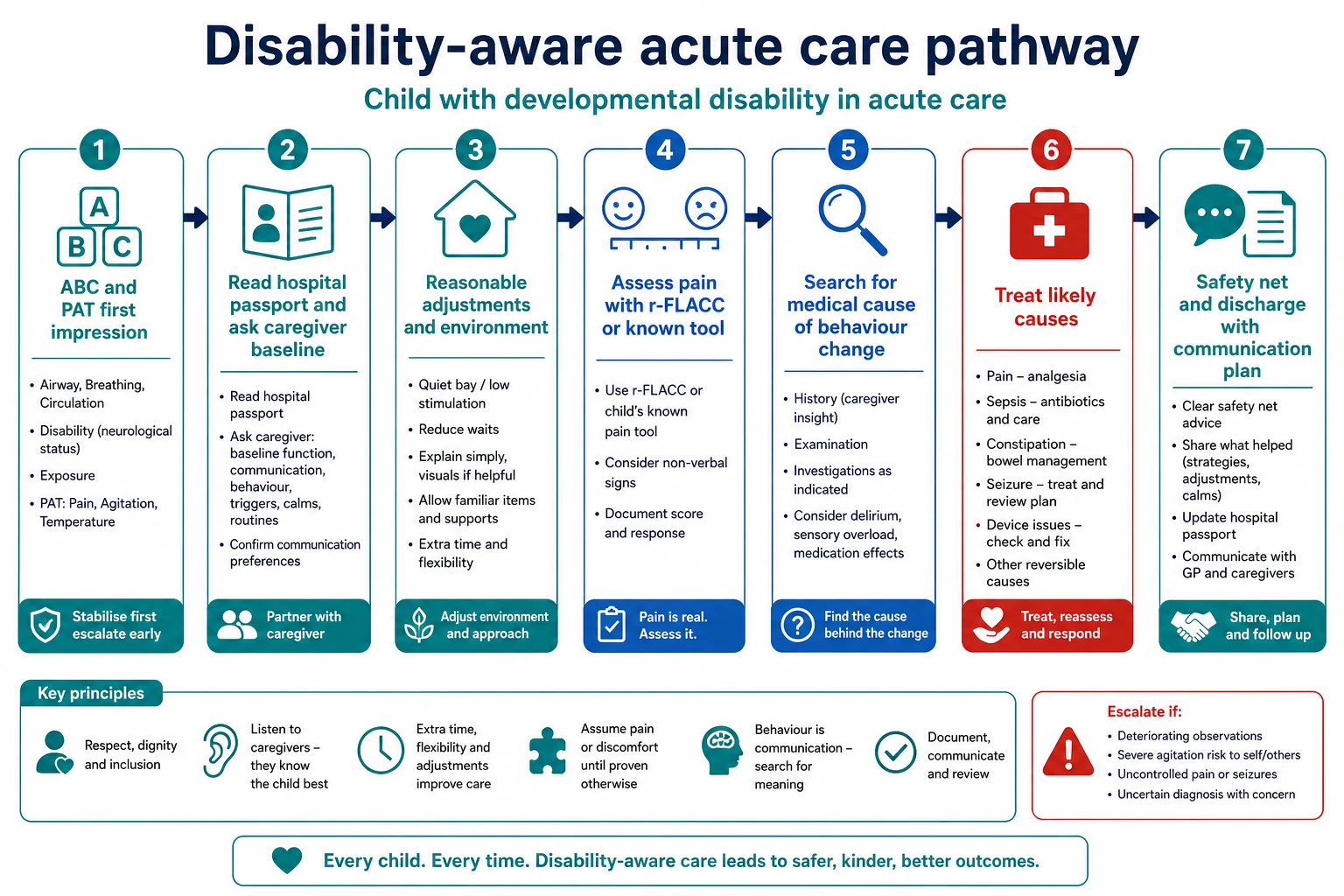
- Stabilise ABC and seizures. [6]
- Implement reasonable adjustments immediately. [3]
- Score and treat pain (r-FLACC or validated alternative). [1]
- Investigate and treat medical causes of behaviour change. [6] [8]
- Involve disability liaison, pain service, social work as needed. [6]
- Document what worked for the next team. [3]
- Discharge only with a written plan, medication clarity and community follow-up. [4]
Wrong versus right framing
- 'It's just autism'
- Skip pain score
- Force exam without prep
- 'What is new today?'
- r-FLACC + treat
- Predictable exam sequence
- Still do ABC
- Still consider sepsis
- Still safeguard
Specific Subtypes & Scenarios
Autism in PED: long waits are toxic; prioritise quieter space and short pathways. Parents report pain expression and environment as major stressors. [3] [4]
Severe intellectual disability: rely on observational pain tools and caregiver pain signatures. [1] [8]
Cerebral palsy / technology dependence: assess tone change, respiratory reserve, aspiration risk, device integrity. [6]
Out-of-home care: incomplete history — call the usual clinician and check records early. [6]
Adolescent: capacity and assent still matter; do not talk only to the parent. [6]
Complications & Pitfalls
- Diagnostic overshadowing. [6]
- Under-treated pain. [1] [5]
- Trauma from restraint without adjustments. [3]
- Missing safeguarding because “they fall a lot.” [6]
- Ignoring caregiver concern. [4]
- Discharge without supports after a frightening visit. [4]
Prognosis & Disposition
Disposition follows medical illness severity and the support package at home. Unexplained behaviour change may need observation even if early labs are normal. ICU criteria are physiological, modified by baseline respiratory and neurological reserve. Communicate the plan in plain language and write what worked. [4] [6]
Special Populations
Indigenous and culturally diverse families need culturally safe communication and interpreter access. Remote families may arrive after delayed presentation — do not punish late arrival. Technology-dependent children need device-competent staff. Out-of-home care needs multi-agency clarity. [4] [6]
Evidence, Guidelines & Regional Differences
Core evidence [1] [2] [3] [4] [5] [6] [7] [8]
- r-FLACC improves reliability/validity for pain assessment in cognitive impairment (Malviya 2006); clinical utility compared across tools (Voepel-Lewis 2008). [1] [2]
- Systematic reviews support structured pain assessment in cognitive impairment and ASD populations. [5] [8]
- Autism PED literature emphasises multi-strategy reasonable adjustments. [3]
- Australian parent ED survey highlights real-world experience gaps. [4]
- Emergency learning-disability inequality reviews stress TEACH-style framing and anti-overshadowing practice. [6]
Regional notes: UK systems often use hospital passports and statutory reasonable adjustments language; ANZ services use similar passport culture with variable local forms; US practice emphasises AAP disability-competent care and ED autism toolkits. Quote local documents in OSCEs. [3] [6]
Exam Pearls
- Behaviour change = medical symptom first. [6]
- Caregiver baseline is essential data. [4]
- r-FLACC for cognitive impairment pain. [1]
- Quiet bay and time are interventions. [3]
- Disability does not cancel ABC or safeguarding. [6]
- Document adjustments that worked. [3]
References
- [1]Malviya S The revised FLACC observational pain tool: improved reliability and validity for pain assessment in children with cognitive impairment Paediatric anaesthesia, 2006.PMID 16490089
- [2]Voepel-Lewis T A comparison of the clinical utility of pain assessment tools for children with cognitive impairment Anesthesia and analgesia, 2008.PMID 18165556
- [3]Richards B Caring for children with autism spectrum condition in paediatric emergency departments Emergency nurse, 2017.PMID 28703063
- [4]Garrick A An Australian Cross-Sectional Survey of Parents' Experiences of Emergency Department Visits Among Children with Autism Spectrum Disorder Journal of autism and developmental disorders, 2022.PMID 34061310
- [5]Pizzinato A Detection and assessment of postoperative pain in children with cognitive impairment: A systematic literature review and meta-analysis European journal of pain, 2022.PMID 35271756
- [6]Lee ACK Health inequalities for people with learning disabilities: why it matters and what emergency physicians need to know British journal of hospital medicine, 2024.PMID 38416523
- [7]Sierra-Núñez D Pain assessment in patients with cognitive dysfunction: Adaptation and validation of the r-FLACC scale Anales de pediatria, 2025.PMID 40639994
- [8]Shaban R Pain assessment in non-verbal children with neurocognitive impairment: a review on current tools, challenges, and clinical perspectives Frontiers in pain research, 2026.PMID 41987884