Paeds · growth-development-and-behaviour
Children with disability in school and community settings
Also known as School inclusion disability · CYSHCN school supports · Disability education planning · Medical home school liaison · Community participation disability
Fellowship-level paediatric role for children with disability in school and community: ICF-style function, medical home partnership, school letters, emergency plans, participation supports, and regional education-interface principles.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A mother asks you to “write a letter for school.” The child has cerebral palsy, uses a walker some days, and has had two seizures this year. The school wants toileting help and an emergency plan. This is paediatric work. [2]
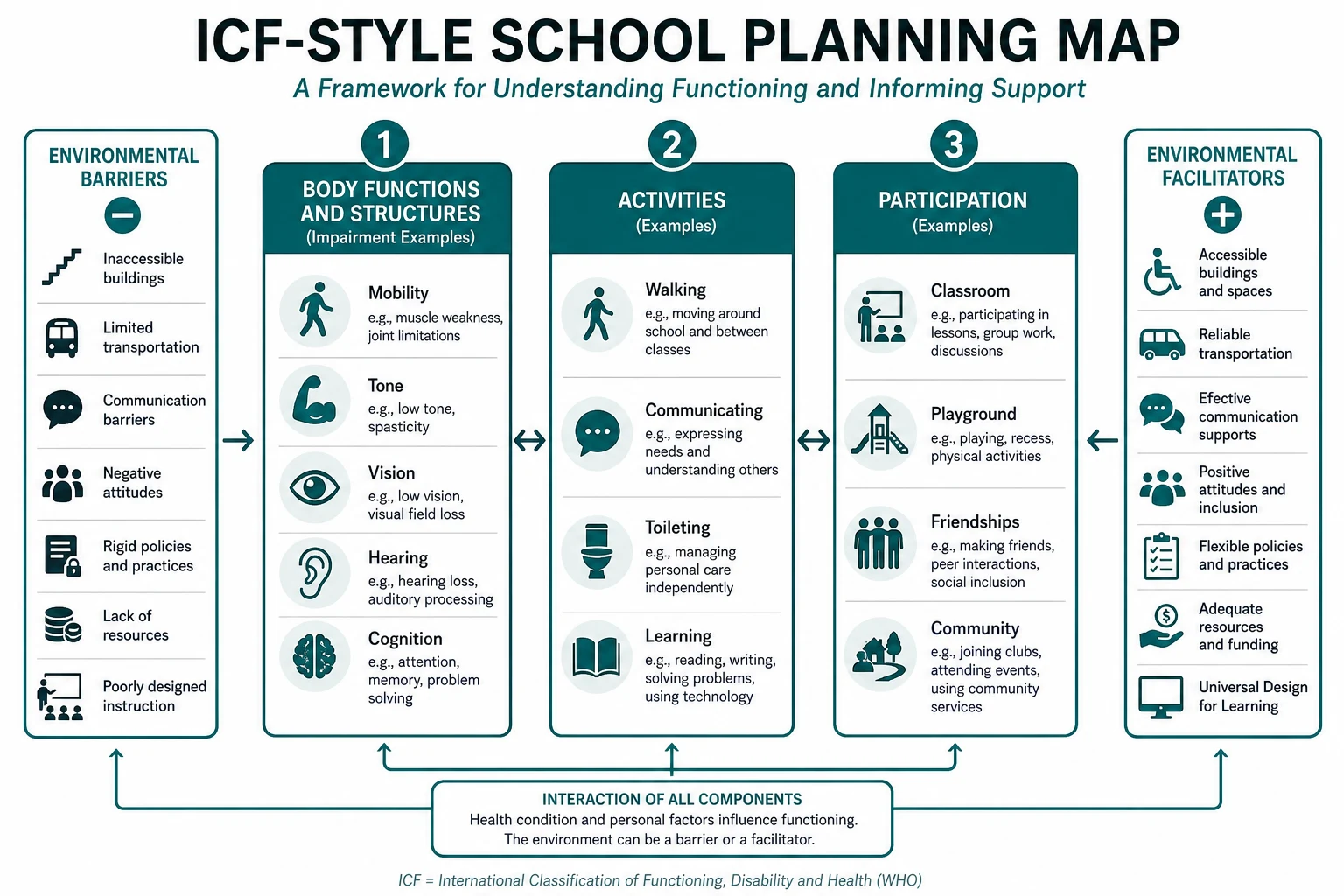
Disability in school and community settings means a health condition interacts with the environment so that learning, play, self-care or belonging is restricted. The WHO International Classification of Functioning (ICF) framing is useful: body functions/structures, activities, and participation, all shaped by environment and personal factors. A diagnosis is not a school plan. [2]
Children and youth with special health care needs (CYSHCN) is a broad service term. Children with medical complexity (CMC) are a smaller group with chronic conditions, functional limitations, high health-service use and often technology needs. Both groups need school and community supports; CMC usually need more intensive coordination. [1]
Your role is medical home leadership: clarify function, reduce avoidable risk, support participation, and communicate with education systems without pretending to be the education authority. [3] [4]
Classification
Sort three maps that examiners mix: medical diagnosis, functional profile, and education support category. They overlap but are not the same. [2]
Three labels that must stay distinct
- CP, autism, epilepsy, IDD, CMC cluster
- Guides health surveillance
- Does not specify classroom supports by itself
- Mobility, communication, self-care, learning, behaviour, fatigue
- What the child can do in a real day
- Core of a useful school letter
- Local plan names differ by jurisdiction
- Determines education resources
- Paediatrician informs; education decides placement process
Epidemiology & Risk Factors
Children needing school and community supports include those with developmental disability, physical disability, sensory impairment, chronic illness, mental health conditions and medical complexity. CMC are a high-need subset with frequent hospital use and care coordination demands that spill into school. [1]
Risks that change outcomes include inaccessible buildings and toilets, missing communication supports or untrained staff, fragmented hospital–school plans, bullying and exclusion, chronic absenteeism, and family burnout with socioeconomic disadvantage. [1] [2]
Protective factors include a continuous medical home, skilled school nursing, inclusive school culture, assistive technology that is actually used, and family-centred partnership. [2] [3] [7]
Pathophysiology
Do not teach disability as a fixed personal defect. Teach person–environment interaction. [2]
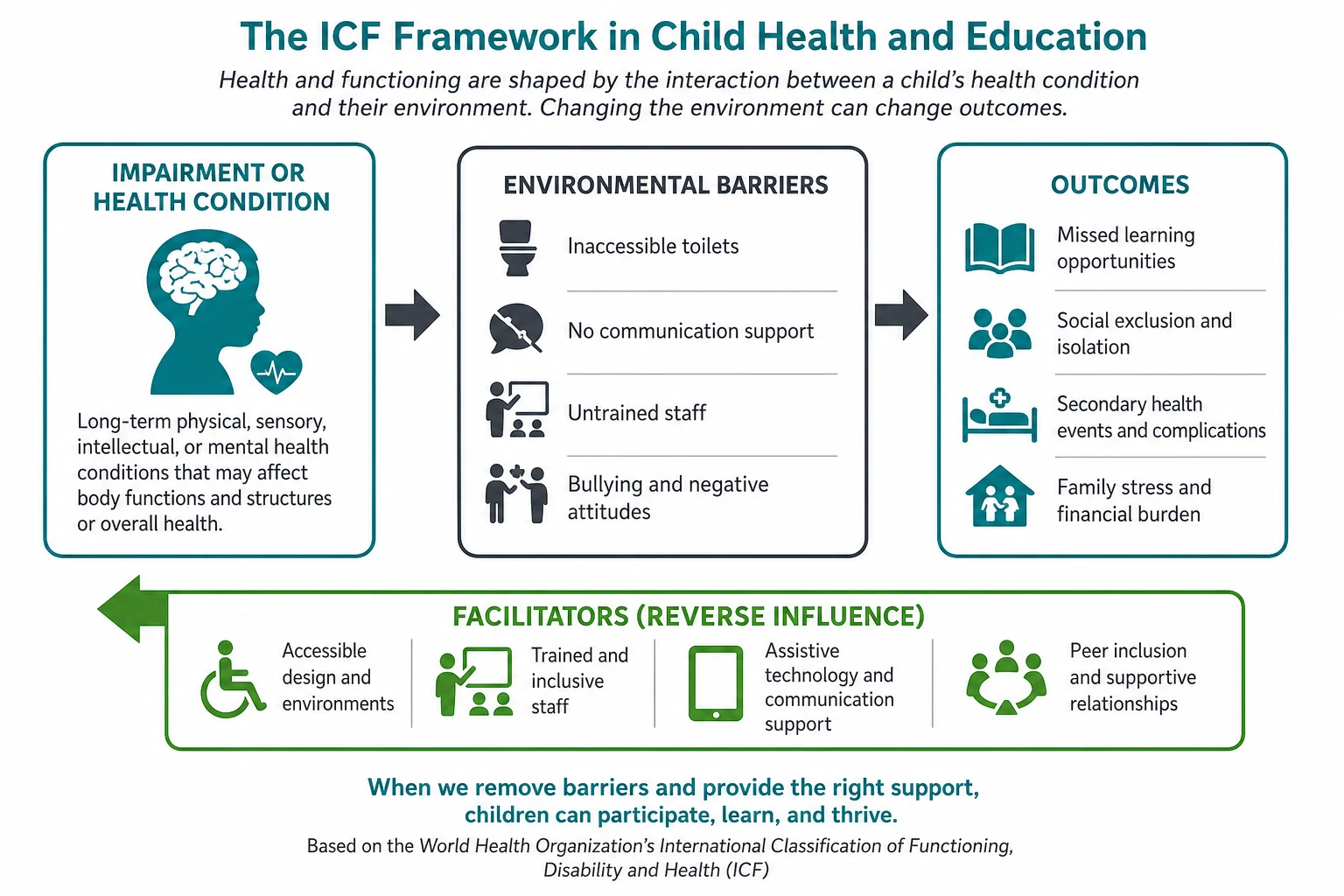
Mechanisms you will use clinically include fatigue and motor cost reducing endurance; communication barriers looking like “behaviour”; pain, seizure risk or toileting failure driving absences; sensory overload or inaccessible design blocking learning; and isolation or bullying worsening mental health. [2] [7]
Environment is modifiable. That is why school letters and equipment decisions matter clinically. [7]
Clinical Presentation
Common clinic prompts include requests for school letters or medication authorities; rising absences or playground exclusion; behavioural crisis after support cuts; family stress about toileting, transport or after-school care; and adolescent transition anxiety as secondary school ends. [1] [2] [3] [4] [5] [10]
Ask for a school-day map: bus or car, classroom seat, toilet access, medication times, playground, fatigue by afternoon, friends, and who helps. That map is more useful than another diagnosis list. [2]
Differential Diagnosis
| Presentation | Better framing | Trap |
|---|---|---|
| “Won’t try at school” | Fatigue, pain, inaccessible task, anxiety, undiagnosed sensory or hearing issue | Laziness narrative |
| Learning plateau | Unmet communication/access needs vs new neurological problem | Assuming placement is the only issue |
| Aggressive incident | Communication failure, sensory overload, pain, peer victimisation | Punishment without functional analysis |
| Frequent absences | Medical instability, toileting, bullying, transport, caregiver illness | Labelling family non-compliant |
| School wants home education only | Temporary medical need vs permanent over-restriction | Medicalising exclusion |
Safeguarding remains evidence-based. Disability does not exclude maltreatment; disability also does not equal neglect. [3]
Clinical & Bedside Assessment
Start with partnership. Introduce yourself. Invite the child to speak first when possible. Use family-centred care: respect, information sharing, participation and collaboration. [3] [4]
Functional history (must-hit domains): mobility and transfers; communication method; toileting, feeding and dressing; learning and attention across the day; behaviour as communication; friendships and bullying; sleep, pain, seizures and nutrition; equipment and who can use it. [2] [3]
School systems history: current education plan name, school nurse contact, emergency drills, medication storage, relief-teacher handover, and previous exclusions. [2]
Examination follows clinical need: growth, neurology, skin under equipment, respiratory status for technology-dependent children, and developmental observation. Document function you observed, not only diagnoses. [2]
Investigations
There is no “school panel.” Investigate for clinical indications only. [1]
Investigations when indicated include hearing and vision for learning or behaviour change; review of therapy reports rather than purposeless re-testing; specialist input for specific medical thresholds; and keeping emergency information form content current for high-risk CYSHCN. [1] [6]
Avoid both poles: under-investigating a new regression, and over-medicalising a pure educational placement dispute. [2]
Management — Resuscitation
School emergencies use standard paediatric algorithms. Anaphylaxis, seizure clusters, asthma, hypoglycaemia and trauma do not wait for a case conference. [6]
Prepare before the crisis with an individual emergency plan in plain language, trained people on site, emergency information form or care summary for complex children, and clear parent and medical-home contacts. [6] [2]
After a school emergency, update the plan, debrief staff and family, and check whether the child needs clinical review. [6] [2]
Management — Definitive & Stepwise
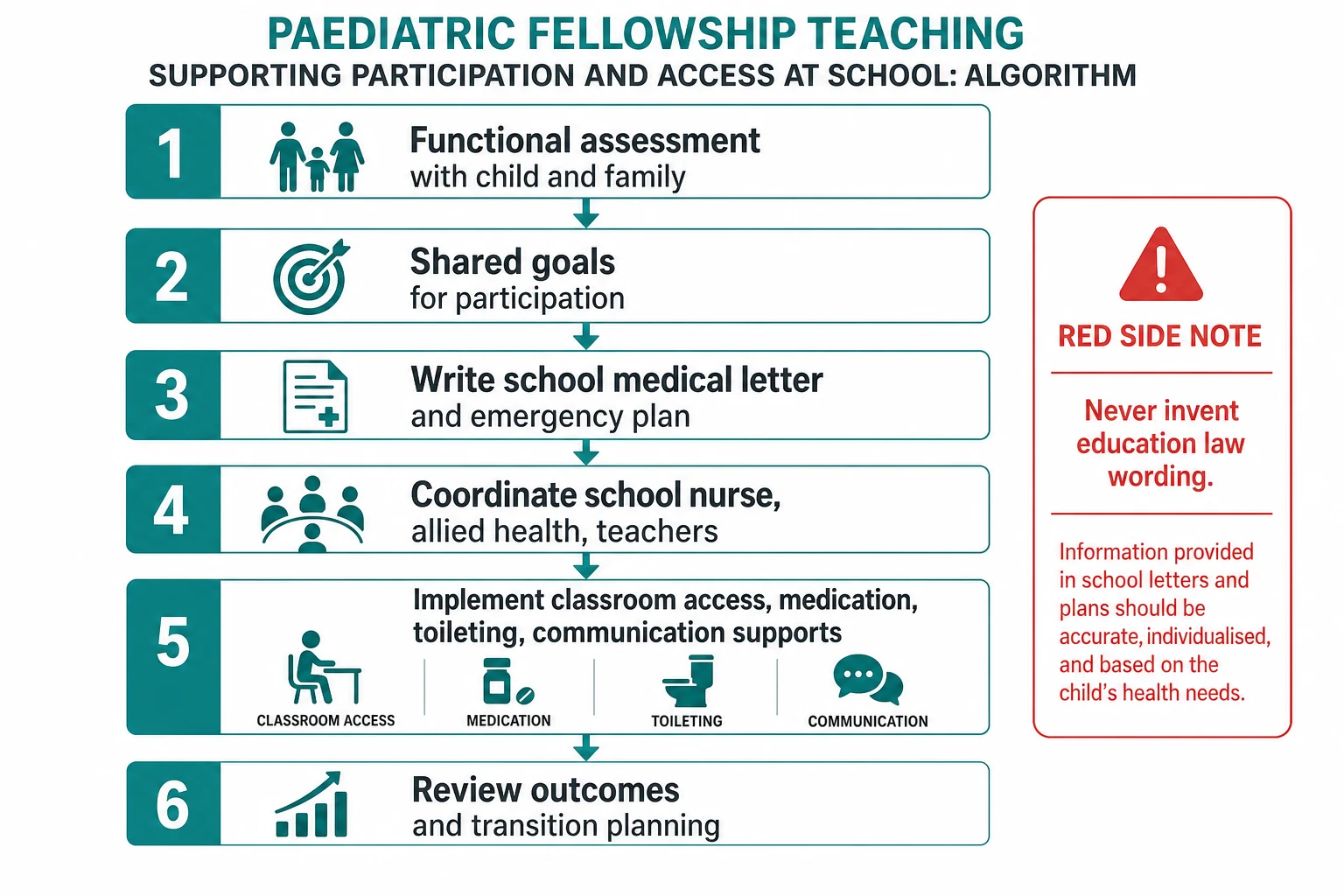
Clinic pathway you can defend
1
2
3
4
5
6
A useful school letter contains plain-language diagnosis only as context; current function and risks; specific supports requested; medication and emergency steps; who to call and when to send to ED; and a review date. [2]
Family-centred service is more than a friendly tone; families should influence goals and methods. [8] Community programmes beyond the medical home can build caregiver skill and peer connection. [9]
Specific Subtypes & Scenarios
Physical disability / CP in mainstream school. Medical home guidance for CP emphasises proactive coordination, equipment, pain, nutrition, and participation — exactly the issues schools face. [2]
CMC with technology. Ventilation, feeds, or complex medication schedules need trained staff and contingency plans; absences rise when coordination fails. [1]
Epilepsy, anaphylaxis, asthma, diabetes. Condition-specific emergency plans plus trained responders. Keep the plan short enough that a relief teacher can use it. [6]
Intellectual disability and curriculum access. Focus on communication, behaviour supports, and realistic goals; do not equate IQ label with inability to belong. [3]
Neurodiversity / autism interface. Sensory load, predictable routines and communication supports often matter more than another medical test. Use the autism-specific leaves for diagnosis detail. [3]
Assistive technology in class. Technology fails when training, family–school agreement and classroom routines are missing. Plan implementation, not only prescription. [7]
Adolescent transition. Start years before school exit. Health care transition needs structured medical-home processes; young adults with CP describe gaps when paediatric systems end abruptly. [5] [10]
Remote schooling. Telehealth helps specialist input, but local trained adults and transport remain rate-limiting. [1]
Complications & Pitfalls
Other pitfalls include assuming school can implement unsupported recommendations; medicalising a placement dispute without new clinical data; forgetting siblings and caregiver health; and letting hospital and school teams run parallel plans with no owner. [1] [3]
Prognosis & Disposition
Participation, friendships and sustainable family life are clinical outcomes, not soft extras. With coordinated supports, many children thrive in inclusive settings; others need specialist environments for part or all of the day. The test is function and wellbeing, not ideology alone. [2] [3]
After clinic, disposition includes named school contacts and document set, emergency plan update if needed, therapy or community referrals, a review date before the next school transition, and adolescent transition tasks when age-appropriate. [2] [5]
Special Populations
- Preschool: early intervention interface and school-entry readiness planning. [9]
- Adolescents: self-advocacy, sexual health privacy, mental health, transition. [5] [10]
- Technology-dependent CMC: nursing skill mix and emergency logistics dominate. [1]
- Indigenous families: culturally safe liaison; do not assume one service pathway. [3]
- Out-of-home care: school instability multiplies risk; over-communicate plans. [4]
- Migrant/refugee families: explain local education systems without jargon. [3]
Evidence, Guidelines & Regional Differences
[2] [5]Landmark anchors include Cohen on CMC as a high-coordination population; Noritz on the medical home for CP with school-relevant domains; AAP family- and patient-centered care statements; White/Cooley on health care transition; the emergency information form for CSHCN; classroom assistive technology implementation lessons; family-centred service and community academy models; and lived transition experience in young adults with CP. [1] [2] [3] [4] [5] [6] [7] [8] [9] [10]
Controversy: inclusion versus specialised settings is not a binary slogan. Match environment to function and wellbeing, review often, and avoid both under-support and over-restriction. [2] [3]
Exam Pearls
- Function and participation beat diagnosis lists. [2]
- Ask the child. [3]
- Emergency plan plus trained people. [6]
- CMC need proactive coordination. [1]
- Assistive technology needs classroom implementation, not only a device. [7]
- Transition planning starts early. [5] [10]
References
- [1]Cohen, E Children with medical complexity: an emerging population for clinical and research initiatives Pediatrics, 2011.PMID 21339266
- [2]Noritz, G Providing a Primary Care Medical Home for Children and Youth With Cerebral Palsy Pediatrics, 2022.PMID 36404756
- [3]Committee on Hospital Care and Institute for Patient- and Family-Centered Care Patient- and family-centered care and the pediatrician's role Pediatrics, 2012.PMID 22291118
- [4]Committee on Hospital Care, American Academy of Pediatrics Family-centered care and the pediatrician's role Pediatrics, 2003.PMID 12949306
- [5]White, PH Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home Pediatrics, 2018.PMID 30348754
- [6]American College of Emergency Physicians Emergency information form for children with special health care needs Annals of emergency medicine, 2010.PMID 20728781
- [7]Karlsson, P Stakeholders' views of the introduction of assistive technology in the classroom: How family-centred is Australian practice for students with cerebral palsy? Child: care, health and development, 2017.PMID 28419501
- [8]Schenker, R Is a family-centred initiative a family-centred service? A case of a Conductive Education setting Child: care, health and development, 2016.PMID 27283848
- [9]Thrall, RS Beyond the medical home: Special Care Family Academy for children and youth Pediatric nursing, 2012.PMID 23362633
- [10]Sarmiento, CA Experiences of young adults with cerebral palsy in pediatric care transitioning to adult care Developmental medicine and child neurology, 2025.PMID 38523396