Paeds · growth-development-and-behaviour
Developmental coordination disorder
Also known as DCD · Developmental dyspraxia · Specific developmental disorder of motor function · Clumsy child syndrome · Motor coordination disorder
Fellowship guide to developmental coordination disorder: DSM/EACD criteria, red-flag exclusions, DCDQ and standardised motor testing, task-oriented intervention, comorbidity, school and activity supports, and regional practice — without inventing uncited cut-offs or drugs for core DCD.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A Year 2 teacher says the child is “messy and lazy in PE.” The parent says buttons take forever. The child can walk and talk. Your job is not to shrug. Your job is to decide whether this is developmental coordination disorder (DCD) — a neurodevelopmental problem of learning and performing coordinated movement — and then to act. [1] [4]
DCD means the child acquires and executes coordinated motor skills substantially below what age, opportunity and practice would predict. The difficulty must interfere with activities of daily living, school work or play. Onset is in the developmental period. The picture must not be better explained by intellectual disability alone, uncorrected visual impairment, or a neurological condition such as cerebral palsy or a progressive neuromuscular disease. That is the clinical spine of modern diagnostic systems and of the EACD international recommendations. [1] [2]
Older labels still appear in notes: “clumsy child,” “dyspraxia,” “motor dyspraxia.” In many services, dyspraxia is used loosely for motor planning difficulty. For exams and for families, prefer DCD and explain it in plain words: the brain finds it hard to plan, time and refine movement, so everyday tasks cost more effort and look less accurate. [1] [4]
This leaf owns DCD recognition, criteria, tools, intervention principles and comorbidity care. Acute floppy-infant work-up, cerebral palsy classification, full ADHD prescribing and pure learning-disorder diagnosis live on linked pages. Cross-link them. Do not hide a second neurology textbook here. [1]
Clinic spine for suspected DCD
Hear the story
Self-care, handwriting, PE, play, family impact — in the child’s words too.
Hunt red flags
Regression, weakness, spasticity, Gowers, seizures — leave the DCD pathway if present.
Document impact
ADL and school participation are diagnostic criteria, not optional colour.
Screen then quantify
Parent questionnaire (DCDQ) plus standardised motor testing when needed.
Plan task practice
Functional goals, OT/PT, school adaptations, successful activity — not blame.
Classification
Classify three things early: is this DCD criteria?, are there red-flag exclusions?, and what is the functional phenotype (fine motor, gross motor, or mixed). [1]
Diagnostic criteria in practice
| Element | What you need | Common fail |
|---|---|---|
| Motor skill | Performance substantially below age and opportunity | Calling normal late handwriting “DCD” |
| Impact | Interference with ADL, school, play or vocation | Ignoring PE avoidance and self-care |
| Onset | Developmental period, not late acquired injury | Labelling post-traumatic clumsiness as DCD |
| Exclusion | Not better explained by ID alone, vision, or neurological disease | Missing mild CP or DMD |
The EACD 2012 long and pocket recommendations set a shared European standard. The 2019 international clinical practice recommendations update definition, diagnosis, assessment, intervention and psychosocial aspects, including adolescents and adults. Defend 2019 as the modern international anchor, and know that 2012 still appears in older exam stems. [1] [2] [3]
Severity and phenotype
There is no single universal staging system you must invent. In clinic, describe impact: mild (compensates with effort), moderate (needs adaptations and therapy goals), severe (major daily restriction). Phenotype may be fine-motor dominant (handwriting, cutlery, fasteners), gross-motor dominant (balance, ball skills, PE), or mixed. Dual diagnosis with ADHD, learning disorder, autism or speech-language disorder is allowed and common. [1] [4]
Tool classes
Parent screens such as the revised Developmental Coordination Disorder Questionnaire (DCDQ'07) flag risk. They do not diagnose. Standardised motor tests such as the Movement Assessment Battery for Children (MABC-2) or Bruininks–Oseretsky (BOT) quantify skill relative to norms. Clinical synthesis still owns the diagnosis. [1] [7]
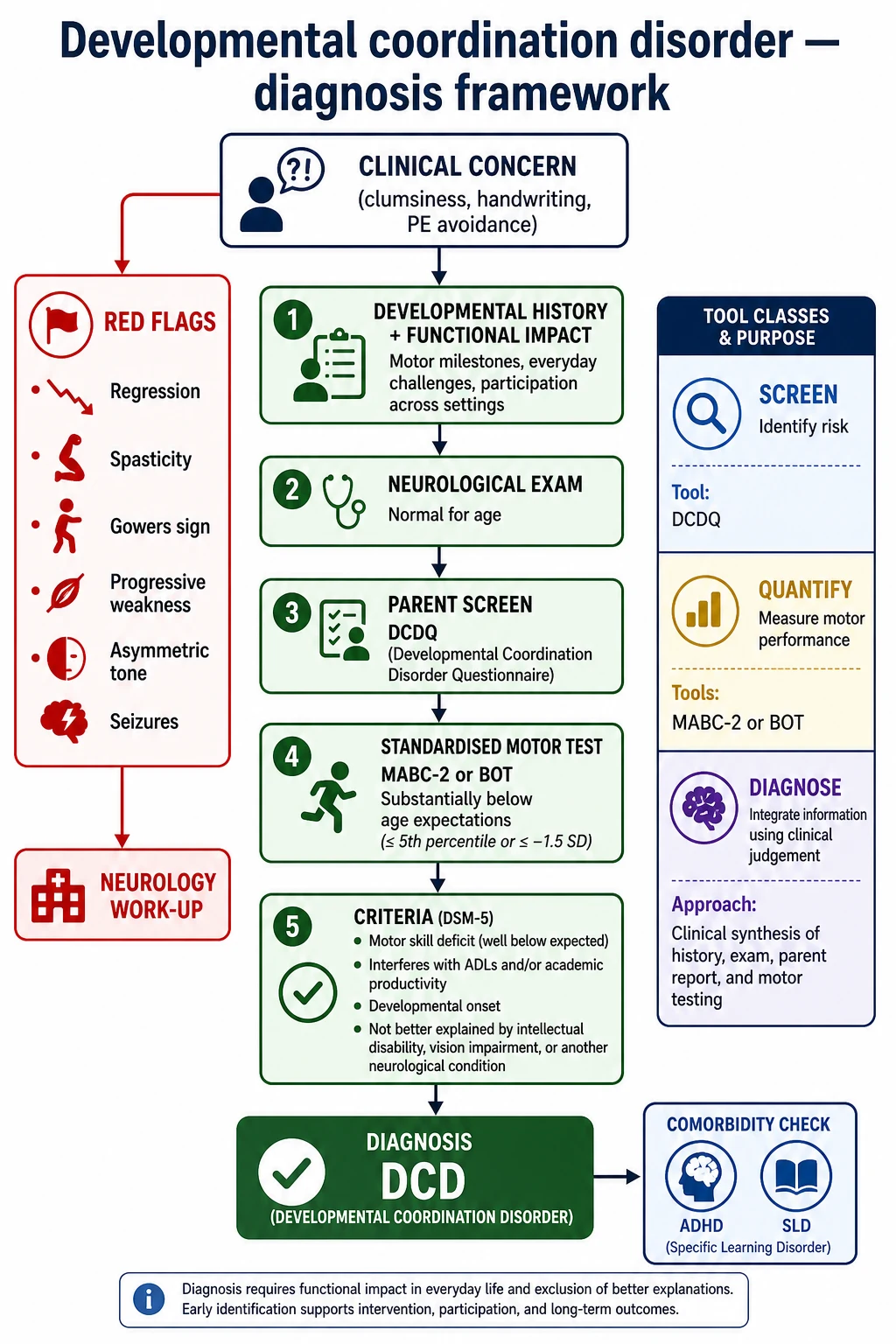
Read the figure like this: if you only score a form, you miss progressive disease. If you only watch PE, you miss handwriting impact. Criteria need both performance and life impact. [1]
Epidemiology & Risk Factors
DCD is common. Reviews and international guidance repeatedly place prevalence around 5–6% of school-age children. That means several children in a typical primary class may meet criteria if you look carefully. Under-recognition is the rule in mild phenotypes and in girls with quieter fine-motor stories. [4] [1]
Boys are referred more often. Part of that is true sex difference in some samples; part is referral bias when PE failure is loud. Preterm birth and very low birth weight raise risk. Community clinics see “always clumsy” schoolchildren; neonatal follow-up clinics see residual coordination difficulties after early motor delay was labelled “catch-up.” [4] [1]
Comorbidity drives complexity. ADHD co-occurs frequently — clinical series often report very high overlap (order of magnitude up to about half in some samples). Specific learning disorders, speech-language difficulties and autism spectrum conditions also co-travel. Treat each problem that is impairing; do not let one label erase the others. [4] [1]
Participation risk is not optional detail. Children with DCD often move less, are less fit, and carry higher overweight and obesity risk as school years progress — the activity-deficit pathway described by Cairney and colleagues. Early childhood risk may not yet show a full activity gap; the disparity often widens with age. [9] [10] [11] [12]
Equity matters. Families facing cost, transport, language discordance or sparse rural OT access complete fewer assessments and fewer therapy blocks. Incomplete foster-care histories delay recognition. Practice design — school-linked OT, telehealth coaching, interpreter-supported questionnaires — is clinical care, not soft extras. [1]
Pathophysiology
DCD is a disorder of motor skill acquisition and control, not a progressive muscle disease. Children take longer to build stable internal models of movement. Performance is often slow, inaccurate and more variable than peers. Dual-task demand — write while listening, run while watching a ball — unmasks the problem in class and PE. [4] [1]
Neuroimaging and motor-learning studies point to atypical function in networks that support planning, timing and online correction (cerebellar and parietal themes appear in reviews). Do not claim a single lesion on a viva. Claim a developmental motor learning difference that is real, measurable and remediable with practice design. [4]
Then comes the activity deficit cycle. Hard tasks feel costly. The child avoids PE, playground games and practice. Less practice widens the skill gap. Fitness falls. Weight may rise. Peers notice. Shame and anxiety grow. Avoidance deepens. That cycle is pathophysiology you can interrupt. [9] [10] [12]
Process-oriented therapies that try only to “fix underlying sensory processes” without enough real-task practice have weaker average effects in meta-analysis. Task-oriented and activity-oriented approaches — teaching the actual skill with structured practice, feedback and cognitive strategies — show stronger motor outcomes. That is why CO-OP (Goal–Plan–Do–Check) and neuromotor task training appear in the intervention evidence base. [5] [6]
Comorbid ADHD adds a second mechanism: inconsistent practice, weak persistence and classroom dual-task overload. Treating attention can help the child use motor practice; it does not replace motor teaching. [1] [4]
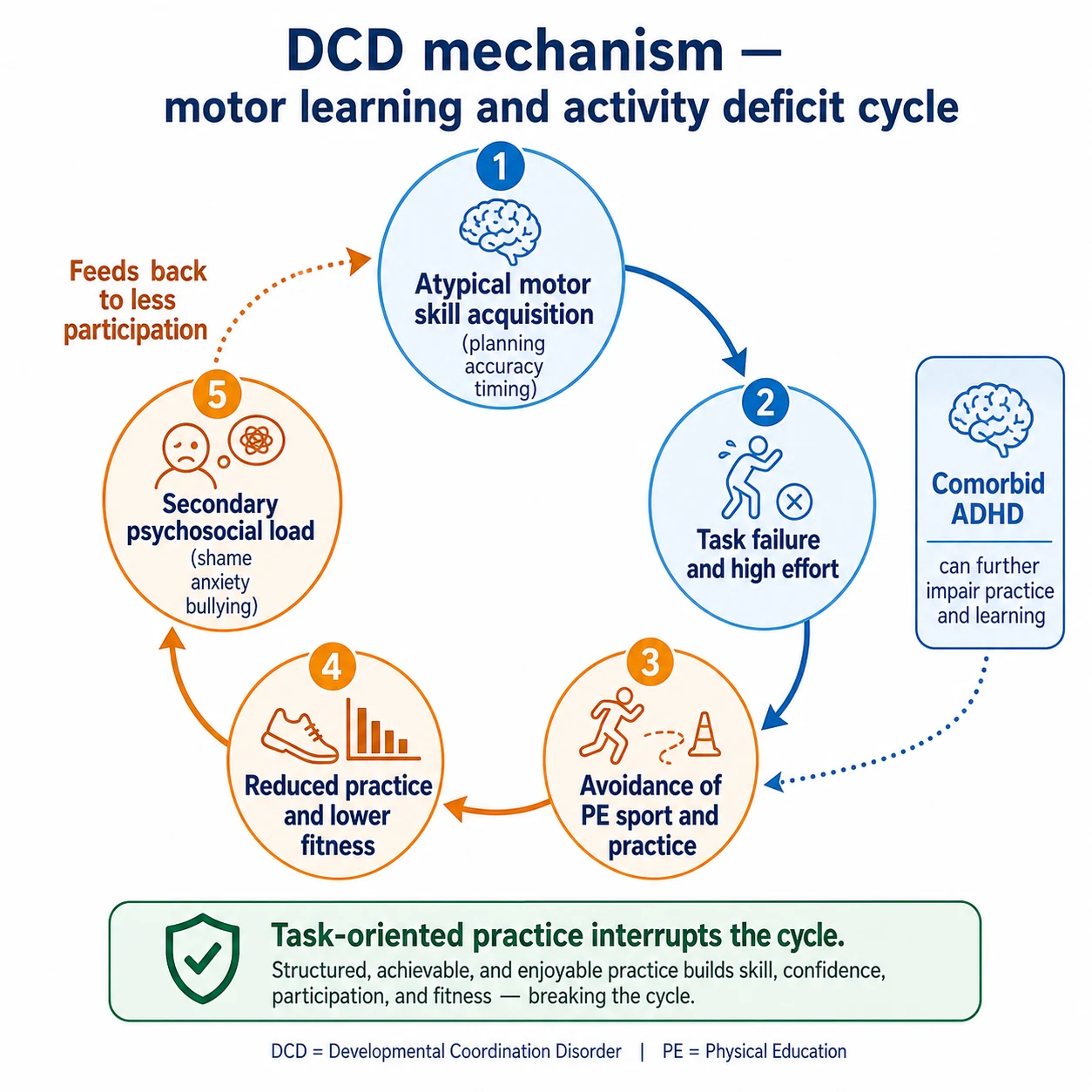
Read the figure like this: your management plan must change both skill practice and the environment that makes practice possible. [5] [9]
Clinical Presentation
Preschool
Parents report late or effortful dressing, cutlery struggle, frequent falls, awkward climbing, and messy mark-making. The child may avoid construction toys or outdoor play. Some still meet early gross-motor milestones “just late enough” that nobody worried until childcare noticed. [1] [4]
School age
Handwriting is slow or illegible. The child cannot keep up with written work. PE is the weekly crisis. Ball skills lag. Shoelaces remain a battle. Teachers may call the child careless. Parents may say “he doesn’t try.” Listen for effort that is high and output that is low — that pattern is DCD, not character failure. [1] [4]
Adolescence
Sports drop-out, low fitness, social exclusion, and anxiety about looking unskilled become the story. Vocational tasks (tools, kitchen, driving readiness) start to matter. Mental health presentations may dominate the referral letter. Ask about motor history even when the ticket says “anxiety” or “school refusal.” [1] [12]
Atypical and red-flag presentations
Stop and reframe if you hear regression, new asymmetric tone, spasticity, Gowers manoeuvre, progressive toe-walking with weakness, seizures, or encephalopathy. That is not routine DCD clinic. Girls may present later with handwriting and organisation load rather than PE drama. Preterm graduates may carry residual coordination difficulty after early “mild delay.” ADHD clinics are full of undiagnosed DCD if you only treat attention. [1] [4]
Differential Diagnosis
| Condition | Discriminators favouring it over pure DCD | First actions |
|---|---|---|
| Mild cerebral palsy | Early tone abnormality, asymmetric signs, abnormal neonatal history, upper-motor-neuron signs | Neurology exam; imaging if indicated |
| Duchenne muscular dystrophy (boys) | Progressive proximal weakness, Gowers, calf hypertrophy, rising falls | Urgent CK; neurology |
| Progressive neurology / ABI | Loss of skills, new focal signs, trauma history | Urgent work-up |
| Intellectual disability | Global cognitive limit explaining motor lag | Developmental assessment; still support motor needs |
| Visual impairment | Uncorrected acuity/field problems | Vision assessment |
| ADHD alone | Motor restlessness without true skill deficit on testing | ADHD pathway; recheck motor skill if impact persists |
| Autism motor difference | Broader social-communication profile | Autism evaluation; still treat impairing motor needs |
| Hypermobility / pain | Pain-limited performance, joint signs | MSK assessment |
| Neglect / deprivation | Extreme understimulation; safeguarding features | Safeguarding pathway |
Compare carefully: DCD can coexist with ADHD, autism and learning disorders. Coexistence is not a reason to discard the motor plan. [1]
Clinical & Bedside Assessment
Start with the child’s day. Dressing, toileting fasteners, cutlery, handwriting volume, PE, playground, bike, after-school sport, and family conflict about “hurry up.” Ask what the child avoids. Ask what the child wants to be able to do. Goals later will come from that list. [1]
Examine with a neurology brain, not only a school form. Tone, power, reflexes, gait, coordination, plantar responses, spine, and a Gowers check in boys who rise oddly from the floor. Observe a writing sample, buttoning, hopping, and a simple ball task if safe. Note effort and strategy, not only success. [1] [4]
Screen for ADHD features, learning concerns, speech-language history, autism red flags, vision and hearing. Collect school reports. Use a parent questionnaire such as DCDQ'07 as a structured screen when age-appropriate. Document impact explicitly — criteria require it. [7] [1]
Counsel while you assess. Say: “This is hard for your motor system, not because you are lazy.” Shame is already present in many rooms. [1]
Investigations
First-line in typical DCD pathway includes structured history and examination with functional documentation; parent motor screen (DCDQ'07) when suitable; standardised motor assessment by trained OT/PT (MABC-2 or BOT) when diagnosis or service access needs quantification; vision check and hearing if communication or classroom listening is an issue; and school academic screening if attainment is falling. [1] [7]
Guidelines discuss motor performance substantially below age expectations. Clinical services often use the lower end of the normative distribution (commonly discussed around the 16th centile and below on standardised batteries) as part of the motor criterion. Exact cut-offs and test editions live in the local manual. In a viva, state the principle and name the test version rather than inventing a full proprietary table. [1] [2]
When to add more: check CK in a boy with possible progressive proximal weakness or Gowers; refer neurology and consider MRI for focal signs, regression, atypical tone, or progressive course — not as routine for classic non-progressive DCD with normal exam; arrange cognitive/educational assessment when learning disorder is suspected; and evaluate ADHD when attention criteria are met. [1] [4]
Low value in pure DCD without red flags: shotgun metabolic panels, routine brain imaging “just in case,” and repeating motor tests monthly without a therapy plan. [1]
DCDQ'07 has demonstrated strong internal consistency and validity evidence as a screen for ages spanning mid-childhood; it is not a stand-alone diagnosis. Original DCDQ work established parent-report motor questionnaires as usable tools. [7] [8]
Management — Resuscitation
Most DCD care is elective. Convert immediately when the story is not DCD: regression, encephalopathy or new seizures; progressive weakness or Gowers (neuromuscular disease); upper-motor-neuron signs (cerebral palsy or other neurology); safeguarding concern hidden under “always bruised because clumsy”; acute mental health crisis, suicidal ideation, or severe bullying; or a child too unwell or too distressed for elective testing today. Stabilise the acute pathway first. Return to DCD planning only when the dangerous differential is gone. [1] [4]
Management — Definitive & Stepwise
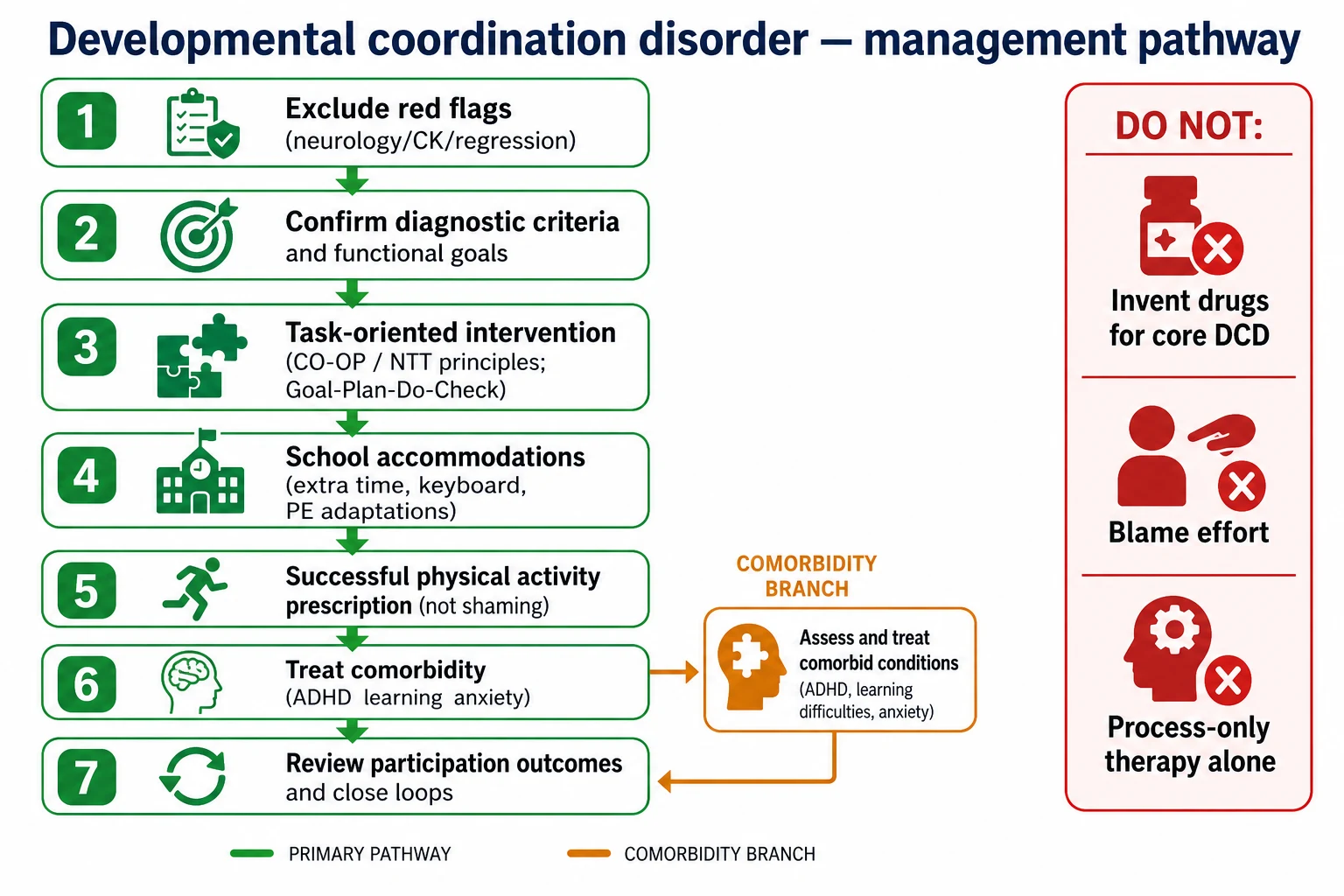
Step 1 — Name it and set goals
Explain DCD in plain language. Co-create two or three functional goals with the child and family: “tie shoes for sport,” “write a paragraph in 15 minutes,” “join a non-competitive swimming group.” Abstract “improve coordination” is not a goal. [1]
Step 2 — Task-oriented intervention
First-line philosophy is activity- and task-oriented practice: train the real skill with graded difficulty, feedback and enough repetition. CO-OP uses a cognitive strategy loop — Goal, Plan, Do, Check — so the child learns to problem-solve the task. Neuromotor task training is another structured task-focused model. Meta-analyses find task-oriented approaches more effective for motor performance than process-oriented approaches that mainly target underlying processes without enough functional practice. [5] [6] [1]
Refer to occupational therapy and/or physiotherapy with that brief. Ask therapists to report goal attainment, not only generic “sensory sessions completed.” [1] [5]
Step 3 — School and environment
Adapt the task while skill builds: extra time, reduced copying load, keyboard access, note outlines, seating, PE role adaptations, and safe alternatives that still include the child. Environment change is treatment. [1]
Step 4 — Successful physical activity
Prescribe movement the child can succeed at. Avoid public failure theatres. Build fitness and peer inclusion deliberately. This is secondary prevention against the activity-deficit and weight pathway. [9] [10] [12]
Step 5 — Comorbidity care
Treat ADHD, anxiety, learning disorders and speech-language needs on their own merits. Stimulant medication for ADHD does not replace motor teaching. There is no first-line disease-modifying drug for core DCD motor deficit — do not invent one in a viva. [1] [4]
Step 6 — Follow-up and closed loops
Review goals, participation, bullying, mood, weight/fitness trajectory and school plan. Close OT/PT and school loops with a named owner and date. Escalate to neurology if the course becomes progressive or atypical. [1]
Specific Subtypes & Scenarios
Fine-motor dominant — handwriting crisis at school entry. Prioritise OT task practice, keyboard options, and teacher load reduction while skill builds. [1]
Gross-motor dominant — PE avoidance and playground exclusion. Prioritise PT/task practice, inclusive PE roles, and a success-based sport. [1] [10]
DCD + ADHD — treat both. Motor goals fail if attention cannot sustain practice; ADHD care fails if every school note is still unreadable. [4]
DCD + specific learning disorder — dual educational plan; do not attribute all underachievement to messiness. [1] [4]
Preterm graduate — residual coordination difficulty after early delay; still use functional criteria and task practice. [4]
Adolescent — fitness, mental health, vocation and self-advocacy become central. [1] [12]
Rural / low access — school-based strategies, telehealth coaching, and fewer but highly goal-focused therapy bursts. [1]
Language-discordant families — interpreter-supported history and questionnaires; do not treat an invalid form as reassurance. [1]
Complications & Pitfalls
Other classic pitfalls include missing mild cerebral palsy; years of process-only therapy without functional goals; blaming effort and character; ignoring fitness and weight trajectory; open-loop referral with no school plan; overlooking bullying and anxiety; assuming puberty will “fix clumsiness”; and diagnosing from messy handwriting alone. [1] [5] [9]
Prognosis & Disposition
Without support, many children do not simply outgrow DCD. Skills can improve with practice and adaptations, but the relative difficulty often persists into adolescence and adulthood. Good outcomes look like participation: the child can do valued tasks with acceptable effort, stays active, and keeps self-worth. [1] [4]
Disposition is usually community and school-based: medical home coordination, OT/PT blocks, education supports, and periodic review. Specialty discharge is reasonable when goals are met, school plans are stable, and red flags are absent — with a clear re-entry route if function falls. [1]
Comorbidity load, late recognition, poverty of access, and chronic shame worsen prognosis. Early naming plus task practice plus environment change improve the trajectory you can influence. [5] [9]
Special Populations
Preterm / NICU graduates — higher DCD risk; separate residual coordination issues from evolving cerebral palsy. [4]
Intellectual disability — motor support still matters; dual-coding rules depend on whether motor skills are below what cognitive level predicts. Follow guideline principles rather than inventing local coding law. [1]
Autistic children — motor differences are common; impairing coordination still deserves a DCD-informed plan when criteria are met. [1]
Indigenous and culturally diverse families — choose culturally valued activities, use interpreters, and avoid tools administered without language access. [1]
Out-of-home care — incomplete histories; catch-up developmental and motor assessment is part of medical-home work. Rural/remote — sparse allied health; prioritise school partnerships and telehealth. Adolescents / transition — self-management, fitness, mental health, driving and work tasks. [1]
Evidence, Guidelines & Regional Differences
Guidelines. EACD 2012 long and pocket recommendations established a shared diagnostic and intervention framework. The 2019 international clinical practice recommendations (Blank and colleagues) are the modern multi-domain update, including psychosocial care and lifespan framing. Use them as your viva anchor. [1] [2] [3]
Intervention evidence. Smits-Engelsman meta-analyses show task-/activity-oriented interventions outperform process-oriented approaches for motor outcomes. That does not ban all sensory-informed strategies; it bans making process-only work the whole plan. [5] [6]
Health behaviour evidence. Cairney and related work link DCD with lower activity/fitness and higher overweight risk across school years; early childhood gaps may still be emerging. [9] [10] [11] [12]
Regional practice (principles, not invented codes). Pathways differ by jurisdiction, but diagnostic criteria and task-oriented care remain shared. [1] [2]
Medical home plus allied health (often NDIS or education-linked pathways depending on impact); school adjustments under local education frameworks; use EACD principles and local service manuals. [1]
OT/PT and education support plans; “dyspraxia” language still common in families — translate to DCD criteria. [1] [2]
School-based OT under education law frameworks when educational impact is documented; medical diagnosis still needs clinical criteria. [1]
CanChild resources are widely used; provincial education and rehab pathways vary — apply criteria and task-oriented care. [1] [2]
Controversies. Cut-off choice on motor tests; adult DCD recognition; sensory integration as sole therapy; overdiagnosis versus chronic under-recognition. Where evidence is weak — drugs for core DCD — omit rather than invent. [1] [5]
Exam Pearls
- Prevalence ~5–6% school-age — common, under-recognised. [4]
- Criteria = motor skill + impact + developmental onset + exclusions. [1]
- DCDQ screens; MABC-2/BOT quantifies; clinic diagnoses. [7]
- Task-oriented > process-only for motor outcomes. [5] [6]
- Check CK/neurology red flags before labelling DCD. [4]
- ADHD comorbidity is common — treat both. [4]
- Activity deficit → fitness/obesity risk — prescribe successful movement. [9]
- EACD 2019 is the modern international recommendation set. [1]
- Never diagnose from messy handwriting alone. [1]
- Convert for regression, progressive weakness or safeguarding. [1]
DCD clinic checklist
Document motor skill and daily impact
Check red flags (CP, DMD, regression)
DCDQ / standardised motor testing as needed
Task-oriented goals and school adaptations
Activity and comorbidity plan; close the loop
Task-oriented (preferred core)
- Practice the real skill with graded difficulty and feedback
- Cognitive strategies such as CO-OP Goal–Plan–Do–Check
- Neuromotor task training and functional goals
- Stronger motor outcome evidence in meta-analyses
Process-only as the whole plan
- Focus mainly on underlying sensory/perceptual processes
- Insufficient functional task practice
- Weaker average motor effects in meta-analysis
- May accompany but should not replace task practice
References
- [1]Blank R International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder Developmental medicine and child neurology, 2019.PMID 30671947
- [2]Blank R European Academy for Childhood Disability (EACD): recommendations on the definition, diagnosis and intervention of developmental coordination disorder (long version) Developmental medicine and child neurology, 2012.PMID 22171930
- [3]Blank R European Academy of Childhood Disability (EACD): Recommendations on the definition, diagnosis and intervention of developmental coordination disorder (pocket version) Developmental medicine and child neurology, 2012.PMID 22320659
- [4]Zwicker JG Developmental coordination disorder: a review and update European journal of paediatric neurology, 2012.PMID 22705270
- [5]Smits-Engelsman BC Efficacy of interventions to improve motor performance in children with developmental coordination disorder: a combined systematic review and meta-analysis Developmental medicine and child neurology, 2013.PMID 23106530
- [6]Smits-Engelsman B Evaluating the evidence for motor-based interventions in developmental coordination disorder: A systematic review and meta-analysis Research in developmental disabilities, 2018.PMID 29413431
- [7]Wilson BN Psychometric properties of the revised Developmental Coordination Disorder Questionnaire Physical & occupational therapy in pediatrics, 2009.PMID 19401931
- [8]Wilson BN Reliability and validity of a parent questionnaire on childhood motor skills The American journal of occupational therapy, 2000.PMID 11006808
- [9]Cairney J Developmental coordination disorder and overweight and obesity in children aged 9-14 y International journal of obesity, 2005.PMID 15768042
- [10]Rivilis I Physical activity and fitness in children with developmental coordination disorder: a systematic review Research in developmental disabilities, 2011.PMID 21310588
- [11]King-Dowling S Physical activity in young children at risk for developmental coordination disorder Developmental medicine and child neurology, 2019.PMID 30963540
- [12]Cairney J Participation in Physical Activity, Fitness, and Risk for Obesity in Children with Developmental Coordination Disorder: A Cross-cultural Study Occupational therapy international, 2015.PMID 26123622