Paeds · growth-development-and-behaviour
Developmental regression: urgent diagnostic approach
Also known as Developmental regression · Neuroregression · Loss of developmental milestones · Skill loss in children · Developmental skill regression
Fellowship urgent diagnostic approach to developmental regression: confirm true skill loss, triage threat, phenotype-guided investigation, parallel supports, and exam-ready communication across ages.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A parent says, “She used to say six words. Now she is silent.” That sentence should change your day. Developmental delay means skills never arrived on time. Developmental regression means skills that were clearly present have gone. Consensus work is tightening how childhood regression is defined so clinics and research stop talking past each other, but the bedside rule is already simple: prove what was gained, prove what was lost, then act on tempo and red flags. [1] [19]
This page owns the urgent diagnostic approach. Cross-link global delay evaluation, autism recognition, intellectual disability, epilepsy and specialty leukodystrophy care rather than hiding those full chapters here. [3] [4] [8]
L.O.S.S. first
Overview & Definition
Picture two toddlers. Both are “not talking.” The first never used words. The second used several words for months, then stopped and stopped pointing. Only the second is regression. That distinction drives urgency because progressive neurological, epileptic, metabolic and some genetic diseases can present as skill loss after a period of typical or near-typical development. [1] [3] [4]
Surveillance systems already treat regression as a red flag that converts the visit out of routine preventive mode. Evidence-informed milestone lists help you decide whether a skill was ever expected and whether it was truly acquired. A skill the child never had is delay or difference. A skill the child had and lost is regression until proven otherwise. [1] [2]
Early language or social loss can occur in autism pathways and is not automatically a storage disease. Pickles and colleagues documented language loss in early autism and specific language impairment. Your job is not to panic every lost word into a rare-disease protocol. Your job is also not to wave every lost word away as “probably autism” without a neurological scan of the whole child. [7] [9] [11]
Classification
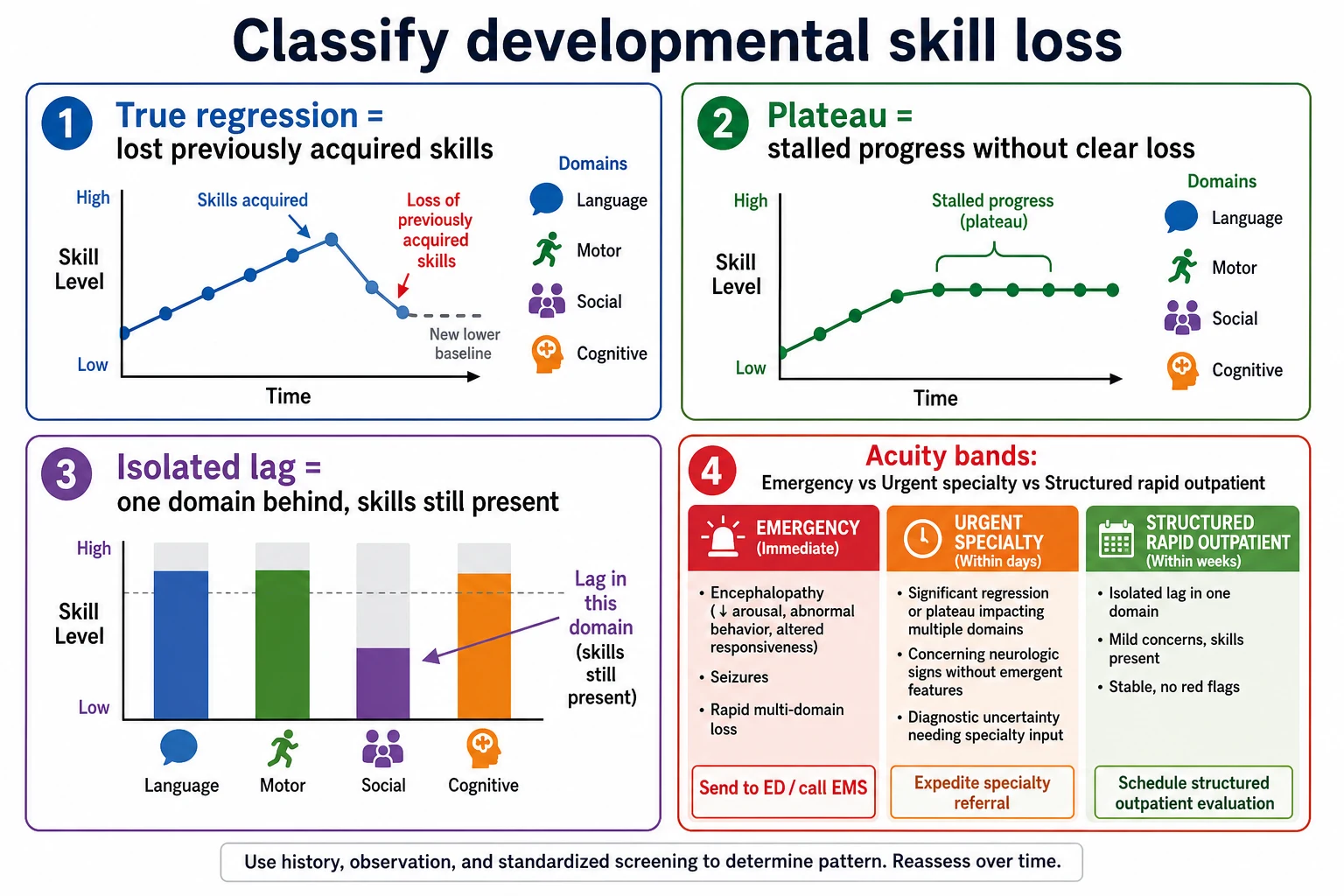
Classify three things at the same time: pattern, tempo and acuity. [1] [4]
Pattern asks which domains fell. Language and social skills alone point one way. Motor loss with tone change points another. Multi-domain loss with adaptive collapse is higher risk. Epilepsy-linked loss may track seizure burden. [4] [7]
Tempo asks how fast. Hours to days with encephalopathy is emergency medicine. Weeks of progressive change is urgent specialty work. Months of stepwise loss still needs a progressive differential, not a birthday-screen wait. [1] [4]
Acuity asks whether the child is unsafe today. Encephalopathy, status epilepticus risk, severe infection, metabolic decompensation and active safeguarding are emergency pathways. Stable children with clear skill loss still need rapid structured evaluation, not a six-month developmental queue alone. [1] [18]
Age bands reshape the shortlist. Infants and toddlers: autism-pathway loss, Rett-window phenotypes, hearing loss, epileptic encephalopathies, early metabolic disease. School-age: leukodystrophies and other progressive white-matter diseases, autoimmune and inflammatory encephalopathies, and overshadowed progressive disease in children already labelled with autism or intellectual disability. [4] [5] [6] [9] [20]
Epidemiology & Risk Factors
Parent-reported skill loss is not rare in early developmental clinics. Most of those stories will not end as a classic leukodystrophy. A smaller group will have progressive disease that you only get one good chance to catch early. Population data show inherited leukodystrophies are uncommon at population scale but carry high morbidity when missed. [5] [7]
Risk clues that raise your pre-test concern include consanguinity, unexplained sibling death or disability, X-linked family patterns, progressive school failure with new neurology, and any child whose “behaviour” is actually a step-down in adaptive skill. Medical complexity raises overshadowing risk: teams may attribute every change to baseline disability. [4] [9] [12]
Language discordance, fragmented records and out-of-home care all increase the chance that “what the child could do last year” is unknown. Professional interpreters improve communication quality for families with limited English proficiency and should be used rather than child interpreters when taking a regression history. Trauma-exposed children can lose skills through environmental and relational pathways without a primary neurodegeneration; that still needs recognition and protection. [13] [16]
Caregiver concern that the child is deteriorating is a clinical signal. In hospital-presenting children, caregiver concern associates with critical illness. In regression work, the same respect applies: do not talk a parent out of a real change you have not verified. [18]
Pathophysiology
Skills are networks that were built and then used. Regression means something disrupted a network that had already formed. The surface finding — fewer words, less hand use, less play — can come from different engines. [4] [6]
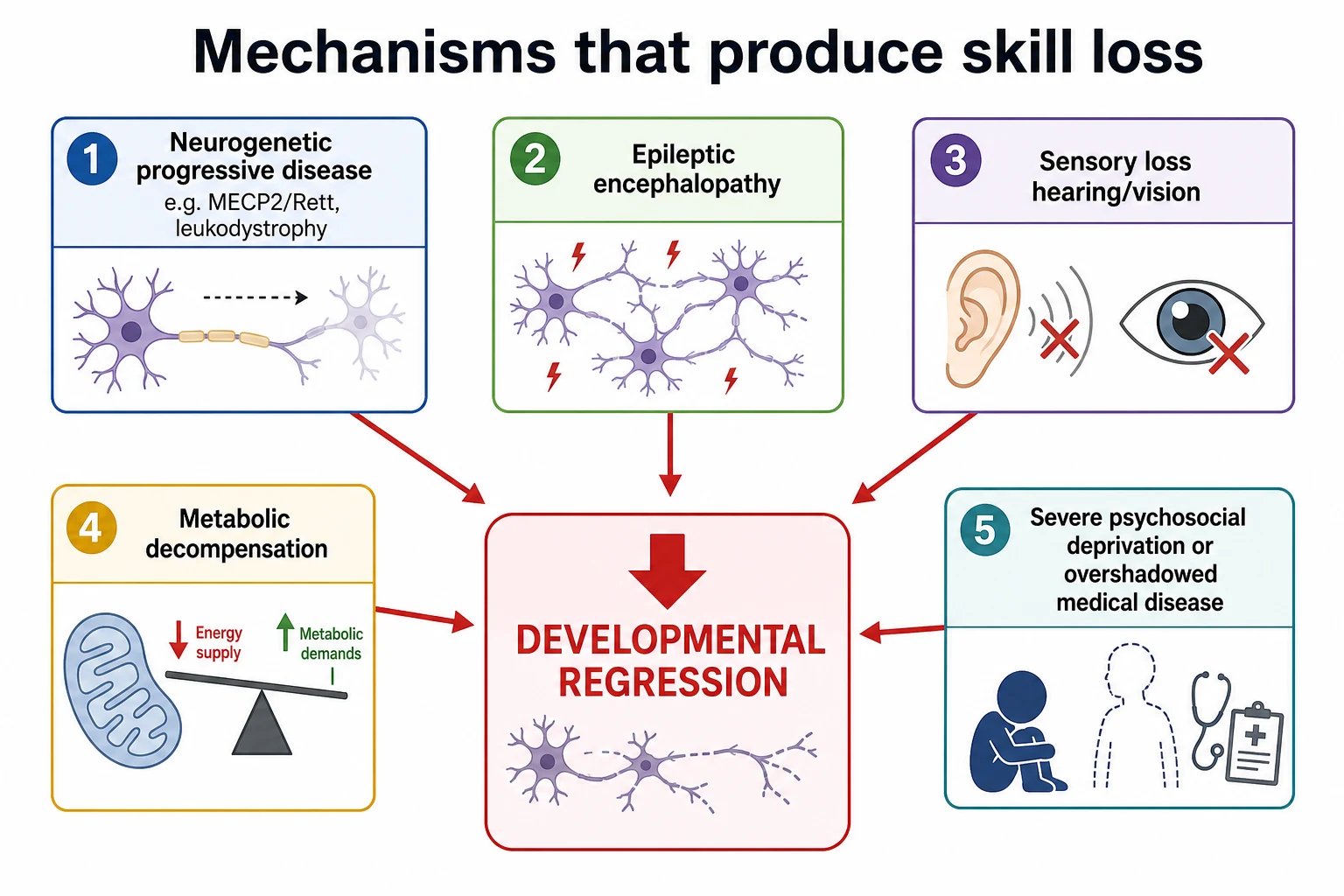
In classic Rett syndrome, early development often looks typical or near-typical, then purposeful hand use and communication fall while hand stereotypies and other features emerge. Revised diagnostic criteria organise that clinical pattern and related variant forms. Symptom-onset analyses continue to refine when families first notice change. The mechanism lesson for the generalist is simple: a quiet early infancy does not exclude later devastating skill loss. [6] [20]
Leukodystrophies injure white-matter pathways that carry motor, cognitive and behavioural signals. Children may present with school failure, behaviour change, spasticity, ataxia or progressive disability. Specialty guidance stresses coordinated diagnosis, care and disease-specific treatment pathways rather than isolated reassurance after one normal clinic visit. [4] [5]
Epileptic encephalopathies can stall or reverse development around uncontrolled seizures or continuous epileptic activity. Sensory loss can look like language regression when the child can no longer hear or see the world that taught those skills. Metabolic decompensation may produce stepwise loss with each illness. Severe psychosocial deprivation and trauma can erode skills without a gene name. Diagnostic overshadowing lets any of these hide under an old autism or intellectual disability label. [7] [9] [10] [16]
Clinical Presentation
The classic story is a toddler who used words and gestures, then stopped. You may also see reduced joint attention, loss of play complexity, or social withdrawal. Some children keep walking and smiling while language collapses. Others lose motor skills first. Ask for videos from birthdays and holidays. Old phone clips often settle arguments about whether a skill was real. [1] [7] [11]
A young girl who loses purposeful hand use, develops hand stereotypies, and shows deceleration of head growth sits in the Rett-window phenotype until proven otherwise. Do not wait for a perfect textbook appearance before referring. [6] [20]
School-age presentations are easy to misread as behaviour or mental health alone. New aggression, school collapse, incontinence after dryness, progressive gait change or cognitive slip with neurological signs needs a progressive white-matter and encephalopathy differential. [4] [5]
Subtle and high-risk variants include: fluctuating skills with illness; post-ictal “loss” that never fully recovers; a child with known disability who stops using a communication device; pain or catatonia misread as “behaviour”; and a polite clinic visit where the child looks calm while the parent describes a freefall at home. [9] [10] [12]
Differential Diagnosis
Hold common and dangerous causes together. [1] [3] [4]
Autism-associated early language or social loss is real and needs autism-pathway evaluation and support. It is not a free pass to skip hearing tests or progressive red-flag review. [7] [11]
Hearing or vision loss can mimic communication regression. Treat sensory access as urgent, not optional. [1] [8]
Epileptic encephalopathy and non-convulsive status can destroy developmental momentum. New seizures, staring runs, regression around sleep or cognitive freefall need neurology and EEG pathways. [4]
Rett spectrum / MECP2-related phenotypes in the classic early childhood window. [6] [20]
Leukodystrophies and other progressive white-matter diseases, including childhood cerebral adrenoleukodystrophy patterns in school-age boys with behavioural and neurological decline. [4] [5]
Storage and metabolic disorders, including neuronal ceroid lipofuscinosis phenotypes and illness-triggered metabolic steps. Use phenotype-guided testing rather than inventing a universal panel. [3] [4] [8]
Infection, autoimmune encephalitis and demyelinating disease when tempo is subacute with encephalopathy or focal neurology. [4]
Psychosocial deprivation, maltreatment and trauma-related skill loss — and mixed pictures where both biology and environment matter. [16]
Overshadowed progressive disease or catatonia in a child already labelled with autism or intellectual disability. [9] [10]
Age shifts the shortlist. Infants: metabolic, epileptic, early genetic progressive disease, severe sensory loss. Toddlers: autism-pathway loss, Rett-window, hearing loss. School-age: leukodystrophy patterns, inflammatory disease, overshadowing. Adolescents: late progressive presentations, mental-health overlap, and transition-system gaps. [3] [4] [8]
Clinical & Bedside Assessment
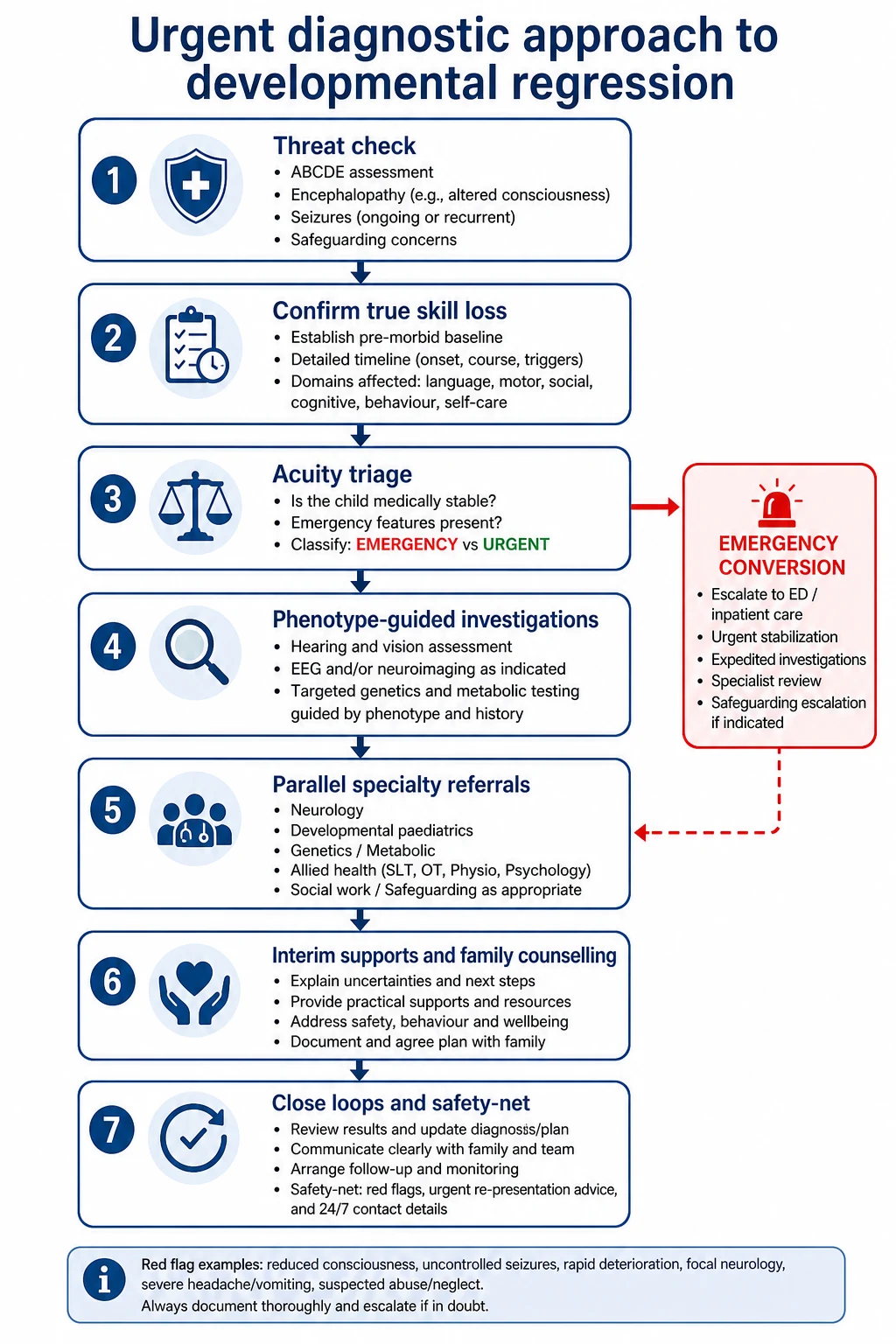
1. Threat first. Before you debate milestones, look at airway, breathing, circulation, disability and exposure. Reduced consciousness, meningism, status epilepticus risk, severe dehydration or a child who “is not themselves” outrank the developmental form. Caregiver concern for deterioration raises your threat threshold. [18]
2. Build a skill ledger. For each domain — gross motor, fine motor, language, social, play, adaptive — ask: what could the child do, at what age, with what example, and what can they do now? Separate “never did” from “did, then lost.” Use prior clinic notes, child health books and videos. Evidence-informed milestone frameworks help you judge whether a claimed early skill was plausible. [1] [2]
3. Map tempo and triggers. Sudden after fever? Stepwise with each illness? Slow over months? Around new seizures? After a house move or placement change? Tempo rewrites the differential. [4] [16]
4. Examine the nervous system like you mean it. Tone, power, reflexes, gait, cerebellar signs, cranial nerves, fundi if skilled and indicated, head circumference trajectory, neurocutaneous findings, dysmorphism, hepatosplenomegaly and growth. A “behavioural” label without a neurological exam is an incomplete assessment. [4] [8]
5. Check sensory access and seizures. Any communication fall needs hearing and vision pathways. Ask about staring, myoclonus, night events and developmental freefall around epilepsy. [1] [8]
6. Assess environment and safety in parallel. Food security, supervision, trauma exposure, caregiver mental health, and whether the history is developmentally plausible. Trauma-informed care is not optional window dressing when skill loss and family stress co-exist. [16]
7. Write a problem representation that forces honesty. Example: “22-month-old with three-month loss of words and pointing after previously using six words, reduced social engagement, normal gait, no seizures reported — urgent regression work-up with autism-pathway and progressive red-flag review.” That sentence stops vague reassurance. [1] [7] [9]
Investigations
Investigations follow phenotype. They do not replace history and exam. [3] [8]
Same-day or emergency tests when encephalopathy, meningitis features, status risk, metabolic crisis or acute progressive neurology is present: local emergency panels, glucose and electrolytes, blood gas as indicated, neuroimaging per neurology/ED pathway, and EEG when non-convulsive status or epileptic encephalopathy is plausible. Do not invent a one-size CT-versus-MRI rule here; state acuity and use local imaging pathways with specialty input. [4] [18]
Urgent but planned bundle for clear regression without immediate ICU threat: formal hearing and vision assessment; consider EEG; MRI brain with attention to white matter when progressive neurology or leukodystrophy is plausible; and early genetics/metabolic discussion. AAP comprehensive evaluation guidance for intellectual disability and global delay structures genetic testing approaches; regression and progressive features escalate urgency inside that framework rather than licensing endless unfocused tests. Canadian guidance offers a practical regional map for GDD/ID evaluation that generalists can adapt. [3] [8]
Targeted tests by phenotype, not by superstition: very-long-chain fatty acids and related pathways when childhood cerebral adrenoleukodystrophy is in play; disease-specific metabolic tests when exam and history point there; MECP2 and related testing when Rett-window criteria are met. Specialty leukodystrophy guidance emphasises coordinated diagnosis and treatment referral. Omit uncited enzyme cut-offs and gene-panel shopping lists. [4] [6]
Low-value moves to avoid: repeating the same normal basic labs every fortnight while no one owns the MRI or genetics referral; calling a single normal investigation “reassurance” in a progressive phenotype; and delaying hearing tests because “it looks like autism.” [1] [9]
Document who will chase each result. Open loops are a common way correct plans fail. [14]
Management — Resuscitation
Regression becomes resuscitation when physiology or safety is failing now. [18]
Manage airway, breathing and circulation. Treat seizures that threaten airway or brain. Correct glucose and critical electrolyte problems. Consider raised intracranial pressure and severe infection early. Do not discharge an encephalopathic child with “developmental clinic in three months.” [4] [18]
Active safeguarding threats — severe neglect, injury patterns, coercive control — convert the visit into a protection pathway while you still investigate medical causes. Trauma-informed practice means you stabilise the child and the system around them, not only the MRI slot. [16]
Rural and telehealth settings change logistics, not standards. If you cannot examine neurology adequately or the child is deteriorating, retrieve. Send a clean handoff: skills lost, tempo, seizures, exam findings, tests pending, and what would make you re-escalate tonight. Structured handoff reduces critical omissions. [14] [18]
Management — Definitive & Stepwise
Once threat is controlled or excluded, run a deliberate plan. [1] [3] [4]
Step 1 — Confirm regression. Skill ledger, videos, records, domains, tempo. [1] [2]
Step 2 — Assign acuity. Emergency, urgent specialty bundle, or rapid structured outpatient pathway with hard dates. [1] [18]
Step 3 — Start phenotype-guided tests. Hearing and vision early. Imaging, EEG, genetics and metabolic tests by pattern. [3] [4] [8]
Step 4 — Refer in parallel, not in a multi-year queue. Neurology, developmental-behavioural paediatrics, genetics/metabolic, audiology, ophthalmology, allied health and early intervention as indicated. Autism-pathway tools such as M-CHAT-R/F risk-stratify toddlers; they do not diagnose, and they do not exclude progressive disease. [3] [11]
Step 5 — Start supports before the final gene name. Communication strategies, physiotherapy or occupational therapy as needed, safety planning, school or early-childhood adjustments, and caregiver support. Waiting for perfect diagnostic closure wastes developmental time. [1] [4]
Step 6 — Counsel with honesty and consent. Explain what you know, what you fear, what you are testing, and what will happen while you wait. Informed consent for genetic testing includes uncertain results and family implications. [15]
Step 7 — Close loops. Named owner, date, and chase plan for every referral and result. Safety-net seizures, further skill loss, reduced alertness and caregiver concern for deterioration. Safety-netting approaches matter in acute childhood care and transfer cleanly to this pathway. [14] [17]
Same-day registrar script
Specific Subtypes & Scenarios
Toddler language-social loss without hard neurology. Treat as urgent developmental evaluation. Check hearing. Use autism-pathway assessment appropriately. Still scan for seizures, head growth change and progressive clues. [1] [7] [11]
Rett-window girl. Lost hand use, hand stereotypies, communication fall, possible head-growth deceleration. Apply clinical criteria concepts and refer for genetics/neurology without waiting for every optional feature. [6] [20]
School-age boy with behaviour change and school collapse. Ask about vision, gait, incontinence, family adrenal or neurological disease, and progressive signs. Leukodystrophy pathways belong early when the story fits. [4] [5]
Epileptic encephalopathy. Developmental freefall around seizures needs seizure control and epilepsy specialty care as part of the developmental rescue, not afterthought. [4]
Apparent regression from hearing loss. Fix access while you complete the rest of the differential. [1] [8]
Neuroregression mislabelled as autism. Progressive signs, new neurology or relentless skill loss after an autism label need reopening of the diagnosis. [9]
Child with medical complexity. New loss is not automatically “baseline.” Diagnostic overshadowing is a known harm pattern. [9] [10] [12]
Out-of-home care or language-discordant family. Rebuild the skill history with interpreters and collateral records. Do not accept an empty past as reassurance. [13] [16]
Rural family on a long waitlist. Create an interim medical-home plan: what is already booked, what is escalated, what returns the child to ED, and who phones when the appointment slips. [14] [17]
Complications & Pitfalls
The classic pitfall is reassurance. “Boys talk late” is not a plan for lost words. Other high-yield traps: treating a screen or autism checklist as a full neurological clearance; missing hearing loss; missing non-convulsive seizures; accepting a prior disability label as the whole story; ordering endless tests with no owner; and failing to safety-net. [1] [9] [11]
Catatonia can be misread as behaviour in neurodevelopmental populations. Reduced movement, mutism or autonomic signs need specific recognition. [10]
Handoff failures drop the progressive differential between ED, ward and clinic. Use structured transfer of the residual risk list. [14]
Prognosis & Disposition
Prognosis follows cause, residual skills, seizure control, therapy access and how early a treatable pathway was opened. Some autism-pathway losses stabilise or improve with support. Some progressive diseases need disease-specific therapy windows that specialty teams own — generalists must not invent those thresholds, but must not delay the referral that reaches them. [4] [5] [7]
Disposition rules of thumb: emergency stabilisation and admission when threat is present; same-week urgent specialty bundling for clear regression with neurological concern; rapid outpatient pathway with hard dates for stable clear skill loss; never “see you at the next birthday check.” [1] [18]
Tell families what improvement or further loss would look like, how to seek help after hours, and which tests are pending. Safety-netting is part of disposition, not an afterthought. [17]
Sibling and cascade genetic testing may follow a confirmed diagnosis. Handle that with genetics counselling and consent standards, not casual corridor advice. [15]
Special Populations
Infants and toddlers need especially careful separation of never-acquired skills from true loss, and early hearing access. [1] [2]
Children with existing autism or intellectual disability are high risk for overshadowing when new regression appears. [9] [10]
Technology-dependent children may lose device-mediated communication that teams misread as non-compliance. [12]
Indigenous families need culturally safe communication, local support pathways and zero tolerance for dismissive care. [13] [16]
Migrant and refugee families need interpreters, rebuilt histories and attention to incomplete screening records. [13]
Out-of-home care needs collateral history and explicit ownership of follow-up across placements. [16]
Socioeconomic disadvantage turns open loops into lost children. Build transport, cost and literacy supports into the plan. [12] [14]
Maltreatment-exposed children may show skill loss from trauma and neglect; medical progressive disease can still coexist. Hold both. [16]
Evidence, Guidelines & Regional Differences
AAP surveillance and screening guidance treats regression as a prompt for evaluation, not observation alone. Milestone modernisation work helps clinicians judge acquisition versus loss more cleanly. [1] [2]
AAP genetic evaluation guidance for intellectual disability and global developmental delay, and Canadian Paediatric Society evaluation guidance, frame comprehensive work-ups that generalists escalate when regression or progressive features appear. [3] [8]
AAP leukodystrophy clinical reporting and earlier burden data support early recognition and coordinated specialty care. Neul’s revised Rett criteria remain a core clinical framework for that phenotype. [4] [5] [6]
Language-loss research in autism warns against equating every regression with neurodegeneration, while overshadowing case teaching warns against the opposite error. [7] [9]
Regional practice maps differ in service names, not in the core duty. ANZ pathways often run through paediatricians, child development services and tertiary neurology/genetics. UK practice sits among NICE autism recognition pathways and regional neurodisability networks. US practice uses Bright Futures/medical-home screening plus AAP evaluation frameworks. Canada uses CPS evaluation guidance and provincial service maps. Name the local door, keep the same red flags. [1] [3] [8]
Exam Pearls
- Lost skill ≠ late skill. Say the difference out loud. [1] [19]
- Ask for videos before you argue with memory. [1]
- Hearing and vision are urgent when communication falls. [1] [8]
- Prior autism label does not exclude progressive disease. [9]
- Rett-window: regression after early typical development with loss of purposeful hand use and hand stereotypies. [6] [20]
- School-age behavioural collapse plus neurology: think white-matter disease early. [4] [5]
- Refer in parallel; close the loop. [3] [14]
- Safety-net seizures, encephalopathy and further loss in plain language. [17]
- Caregiver concern for deterioration is data. [18]
- In long cases, structure: threat → confirm regression → differential by age/tempo → investigations → interim supports → communication. [1] [3] [4]
High-yield anchors
References
- [1]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [2]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439
- [3]Moeschler JB Comprehensive evaluation of the child with intellectual disability or global developmental delays. Pediatrics, 2014.PMID 25157020
- [4]Bonkowsky JL Leukodystrophies in Children: Diagnosis, Care, and Treatment. Pediatrics, 2021.PMID 34426533
- [5]Bonkowsky JL The burden of inherited leukodystrophies in children. Neurology, 2010.PMID 20660364
- [6]Neul JL Rett syndrome: revised diagnostic criteria and nomenclature. Annals of neurology, 2010.PMID 21154482
- [7]Pickles A Loss of language in early development of autism and specific language impairment. Journal of child psychology and psychiatry, and allied disciplines, 2009.PMID 19527315
- [8]Bélanger SA Evaluation of the child with global developmental delay and intellectual disability. Paediatrics & child health, 2018.PMID 30919832
- [9]Loo KK Diagnostic Overshadowing: Insidious Neuroregression Mimicking Presentation of Autism Spectrum Disorder. Journal of developmental and behavioral pediatrics : JDBP, 2022.PMID 35943376
- [10]Reinfeld S Diagnostic overshadowing clouding the efficient recognition of pediatric catatonia: a case series. CNS spectrums, 2023.PMID 36440510
- [11]Robins DL Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics, 2014.PMID 24366990
- [12]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [13]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [14]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [15]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [16]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [17]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428
- [18]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [19]Gawade G Consensus definition for developmental regression during childhood. Developmental medicine and child neurology, 2026.PMID 42406921
- [20]Percy AK Symptom Onset in Classic Rett Syndrome: Analysis of Initial Clinical Severity Scale Entries. Annals of the Child Neurology Society, 2025.PMID 40880843