Paeds · growth-development-and-behaviour
Early intervention and developmental care planning
Also known as Early childhood intervention · Developmental care plan · IFSP paediatric · Part C early intervention referral · Family-centred early intervention
Fellowship guide to early intervention and developmental care planning: from parental concern and failed screens to urgent gates, parallel referral, family-centred goals, key-worker coordination, parent-mediated supports, equity, waitlist safety-nets and ANZ/UK/US/Canada system principles without cloning tool-level assessment or condition-specific therapy leaves.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A mother says her 20-month-old is “not talking like the cousin.” The screen is delayed. The waiting list for formal psychology is months long. The wrong move is to send them home with “boys talk later” and no plan. The right move is early intervention thinking: protect the child from preventable secondary harm while you work out the full diagnosis. [1] [3]
Early intervention (EI) means organised supports—therapy, parent coaching, education, equipment and social help—started as soon as developmental risk or delay is recognised, rather than after school failure. It is not the same as a single clinic appointment, and it is not the same as a laboratory diagnosis. [4] [9]
A developmental care plan is the written, shared agreement: who the child is in functional terms, what matters to the family, which goals come first, who does what, when you review, and how you escalate. In US Part C language this often appears as an Individualised Family Service Plan (IFSP) style document; other jurisdictions use different names with the same job. [4] [11]
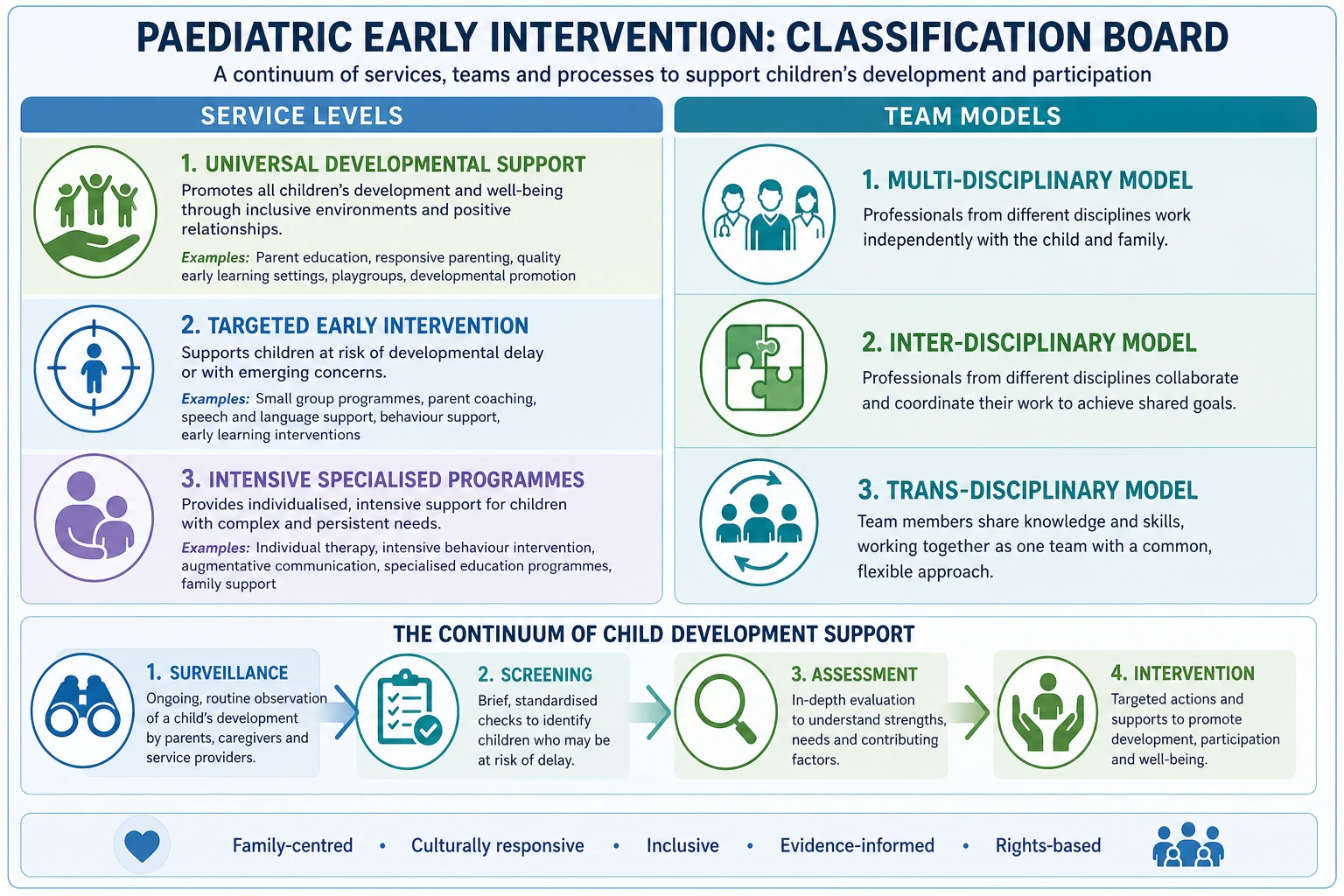
Developmental surveillance is the continuous process of asking, observing and listening at every visit. Screening uses a standardised tool at selected ages. Assessment defines strengths and needs in more depth. Intervention changes daily experience. Examiners punish candidates who collapse those four words into one. [1] [2] [3]
Five questions before you plan early intervention
What is the functional problem?
Communication, motor, social, learning, behaviour, daily living—name it in plain language.
Is anything urgent?
Regression, seizures, safeguarding, severe neglect, unsafe caregiver mental health.
What must run in parallel?
Hearing, vision, medical work-up and EI referral can move together.
What does the family want first?
Goals owned by caregivers beat therapist-only checklists.
Who owns follow-up?
Key worker, medical home and review date—or the plan dies on a waitlist.
Classification
Classification here is about service intensity and team design, not a new disease taxonomy. [4] [18]
Service levels
Universal developmental support is what every child should receive in the medical home and community: surveillance, responsive caregiving advice, safe sleep, reading, play and social supports. [1] [21] [24]
Targeted early intervention adds structured therapy and parent coaching when delay or high risk is identified—speech pathology, physiotherapy, occupational therapy, developmental education, social work. [4] [9]
Intensive specialised programmes concentrate hours and expertise for selected conditions (for example some autism early intervention models, or high-intensity motor programmes after early CP diagnosis). Intensity must still be family-feasible. [5] [7] [8]
Team models
Multidisciplinary: separate professionals, separate plans, shared reports.
Interdisciplinary: shared goals, regular joint planning.
Transdisciplinary: a primary interventionist delivers across domains with team coaching—often more practical for families. [18]
| Term | Bedside meaning | Exam trap |
|---|---|---|
| Surveillance | Continuous asking and observing | Same as a one-off screen |
| Screening | Standardised tool at set ages | A diagnosis |
| Assessment | Deeper profile of strengths/needs | Automatically starts therapy |
| Early intervention | Supports that change daily practice | Waiting for a perfect label |
| Key worker | Named navigator for the family | “Someone will call you” |
| Care plan | Shared goals, owners, review date | A clinic letter alone |
Watch and wait
Hope without a plan
- No review date
- No hearing/vision check
- Family left alone
- High exam fail risk
Parallel pathway
Support + diagnosis
- EI starts now
- Investigations continue
- Family goals written
- Waitlist safety-net
Label first only
Delay for certainty
- Misses plasticity window
- Secondary disability grows
- Family loses trust
- Sometimes still needed for specific Rx
Epidemiology & Risk Factors
Not every delayed milestone needs the same package, but some groups carry higher risk of lasting impairment: extremely or very preterm infants, neonatal encephalopathy, congenital anomalies, genetic syndromes, hearing or vision impairment, prenatal substance exposure, and children living with poverty, housing instability, out-of-home care or severe caregiver mental illness. [5] [6] [10] [13] [16]
Equity shapes who gets help. Low-income families, mobile families and non-English-speaking caregivers are more likely to miss appointments and fall off waitlists unless services redesign access. Same referral letter is not the same opportunity. [15] [16] [17]
Population surveillance programmes only help if positive findings convert into completed pathways. Incomplete follow-up after a failed screen is a system failure, not a family failure. [1] [3]
Pathophysiology
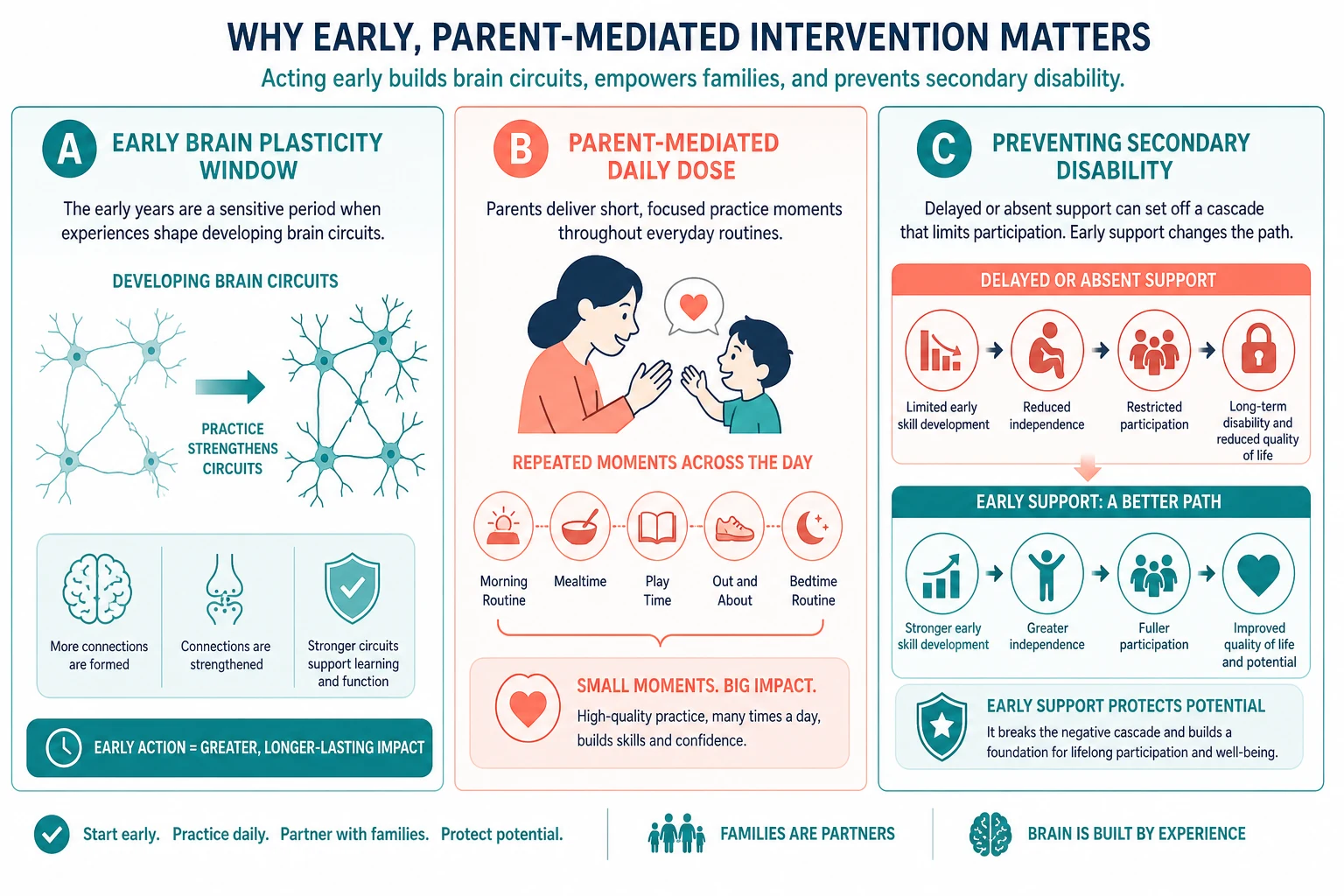
Early intervention works through three linked mechanisms you should be able to explain in a viva. [6] [9] [13]
Experience-dependent plasticity
In the first years of life, circuits for language, motor control and social attention are highly experience-sensitive. Repeated, meaningful practice strengthens useful pathways. Waiting wastes practice opportunities even when the primary diagnosis cannot be “cured.” [6] [9]
Parent-mediated dose
Therapists see a child for hours per week. Caregivers live the other hours. Parent coaching multiplies practice across meals, play, nappy changes and walks. That is why family-centred models outperform “drop-off therapy only” for many goals. [7] [8] [9]
Preventing secondary disability
A motor impairment can become contractures, pain and exclusion. A language delay can become behaviour escalation and social isolation. Untreated hearing loss can look like global delay. Early supports reduce these secondary cascades. [5] [9]
Toxic stress biology explains why unbuffered adversity threatens developmental trajectories and why supporting caregivers is part of EI, not a soft extra. [13] [14] [20]
Clinical Presentation
EI work presents as concerns and pathways, not as a single rash. Common entries: parental worry, childcare or preschool report, failed developmental screen, high-risk NICU follow-up, sibling comparison, or regression. [1] [2] [10]
Families may present exhausted, angry at prior dismissal, or hopeful for a quick medical “fix.” Some want only a label; others want only therapy and fear medicalisation. Your first job is to hear the functional story: what the child can and cannot do at home and in care. [11] [23]
Caregiver perinatal depression or social crisis may present as missed sessions or “non-compliance.” Treat that as clinical data needing support, not blame. [15] [20]
Differential Diagnosis
EI planning is not a substitute for differential diagnosis—and diagnosis is not a substitute for EI. Think in parallel tracks. [1] [5]
Working frames that change the package: isolated speech-language delay; global developmental delay; autism spectrum concern; motor delay/CP risk; hearing or vision impairment; intellectual developmental disorder risk; environmental deprivation or adversity; neurodegenerative or neurometabolic regression. Sibling pages own full disease algorithms; here you must know that the package and urgency change with the frame. [5] [9]
Separate need for urgent biomedical work-up from need for immediate supports. Many children need both on day one. Avoid low-value overtesting that delays the first helpful session. [5] [22]
Clinical & Bedside Assessment
Start with the child’s function and the family’s day. Ask what a morning looks like, what play looks like, how the child communicates wants, and what the caregiver most wants to change this month. [11] [23]
Take a focused developmental history: pregnancy and neonatal course, hearing newborn screen and later concerns, vision, seizures, regression, family history, languages spoken at home, childcare hours, and prior therapy. Observe interaction in the room. [1] [2] [3]
Assess access barriers: transport, work rosters, literacy, digital access, trust, cultural safety and housing. A perfect plan that cannot be attended is not a plan. [15] [16] [17]
Document consent, goals in the family’s words, the referral owner, and the review date. [4] [11]
Investigations
Investigations support safety and diagnosis; they should not become the only activity. [1] [5]
Non-negotiable early checks: hearing and vision pathways appropriate to age and concern. Undiagnosed sensory loss wrecks developmental interpretation. [1] [3]
Parallel medical work-up (genetics, neuroimaging, metabolic tests) follows the condition-specific leaf and local pathways. Do not hold all therapy until every test returns unless the test truly changes immediate safety. [5] [9]
Referral package quality is an investigation of the system: clear concerns, functional examples, languages spoken, caregiver contacts, prior results, and what has already been tried. Poor packages create bounce-backs and delay. [4] [11]
Management — Resuscitation
Most EI is not resuscitation—but some presentations are. Manage ABCDE threats first. Treat suspected infantile spasms, encephalopathy, severe dehydration, or traumatic injury on emergency pathways. Protect the child if safeguarding concerns dominate. Stabilise caregiver crisis with urgent mental-health and social supports when infant safety is at risk. [5] [13] [20]
Do not use a developmental waitlist as a holding pattern for an unsafe home. [13] [16]
Management — Definitive & Stepwise
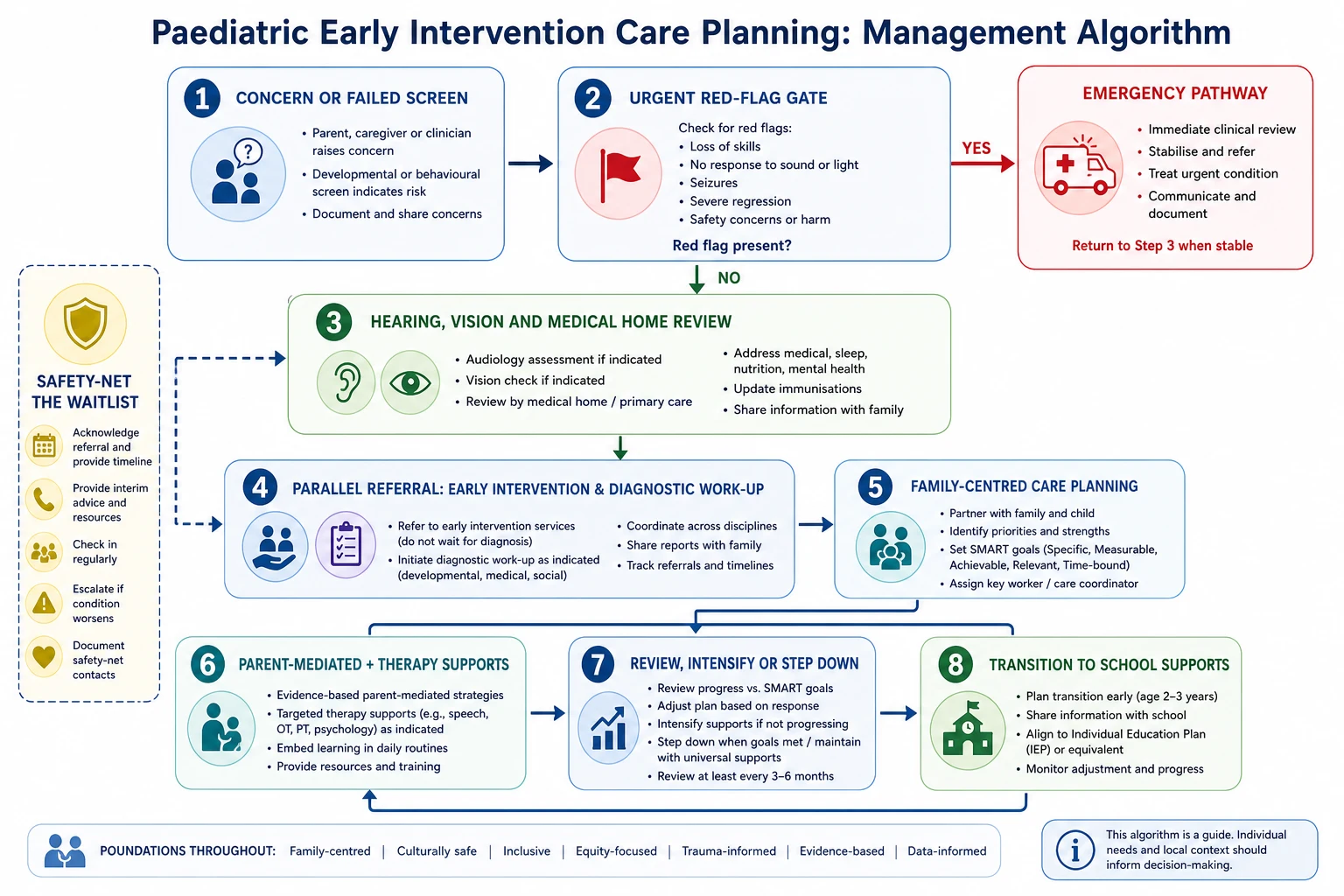
Work this sequence out loud in exams. Confirm the concern and functional impact. Gate for urgent red flags. Check hearing and vision pathways. Refer to early intervention / allied health and arrange indicated diagnostic assessment in parallel. Build a family-centred plan with a few SMART goals written in caregiver language. Assign a key worker or clear navigator. Deliver parent-mediated strategies plus discipline-specific therapy. Coordinate the medical home. Review progress, barriers and new concerns on a named date. Intensify, change model or step down. Plan transition toward school-age supports when appropriate. [1] [3] [4] [5] [9] [11] [12]
Counselling scripts examiners want
Starting before the label: “We do not need every test back to begin helpful practice. Support and diagnosis can run together.” [4] [5]
No false cure: “Early help improves skills and participation. It is not a promise to erase every difference. We will measure progress against goals you choose.” [7] [9] [23]
Waitlist safety-net: “While you wait, here is what to practise, who to call if things worsen, and the date I will check the referral has been received.” [1] [4]
Medical-home role
The medical home keeps the whole child in view: immunisation, growth, sleep, feeding, behaviour, caregiver mental health, care coordination and advocacy when systems stall. [4] [11] [12] [21]
Specific Subtypes & Scenarios
Preterm graduates. Structured developmental follow-up pathways (NICE-style principles) identify risk early; post-discharge developmental programmes show benefit signals for cognitive outcomes in Cochrane synthesis—use local follow-up clinics and do not rely on opportunistic care alone. [6] [10]
Cerebral palsy risk. Earlier accurate diagnosis enables earlier targeted motor intervention and family support; do not wait for a late walking milestone if early signs are clear. Full CP algorithms sit on CP leaves. [5]
Autism concern. Early parent-mediated and comprehensive models such as ESDM have randomised evidence for improving developmental scores in toddlers; later multi-site work is more mixed versus treatment-as-usual—teach evidence humility, start supports, and avoid commercial miracle claims. ASD leaves own diagnosis and full management. [7] [8]
Intellectual disability risk. Comprehensive EI emphasises family patterns of interaction, comprehensive educational supports and reducing secondary behavioural disability. [9]
Speech-language predominant delay. Rapid hearing check, language-rich coaching, and speech pathology referral without waiting for school age. [1] [3]
Social complexity. Redesign visits, outreach and flexible appointments; screen poverty-related needs and link real resources. [15] [16] [17]
Rural and telehealth. Hybrid coaching can preserve parent-mediated dose when travel is hard; still name who owns in-person urgent review. [4] [11]
Transition out of EI. School entry is a planned handoff, not a cliff; adolescent transition principles apply later for ongoing disability. [19]
Complications & Pitfalls
Common pitfalls: watch-and-wait without safety-net; dismissing parental concern; delaying all support for a genetic result; ignoring hearing/vision; therapist-only goals the family cannot live; fragmented agencies with no key worker; equity-blind waitlists; overpromising cure language; and overtesting as a substitute for help. [1] [3] [4] [5] [11] [15] [22] [23]
Prognosis & Disposition
Prognosis depends on the underlying condition, severity, comorbidities, timing of supports, family resources and service quality. EI success is measured in functional participation, family confidence and reduced secondary disability—not only in a single standardised score. [6] [9] [23]
Intensify when goals stall, new red flags appear, or access barriers block the plan. Step down when skills generalise and natural environments can maintain progress. Disposition always includes a review date and a named contact. [4] [11]
Special Populations
NICU graduates. Corrected age, structured follow-up and earlier motor surveillance matter. [6] [10]
Medical complexity. Coordinate devices, feeding, pain and therapy so appointments do not destroy family life. [11] [12]
Indigenous and culturally diverse families. Cultural safety, local language and community-controlled supports improve engagement; specialist cultural leaves own depth. [11] [15]
Migrant and refugee families. Interpreter use is mandatory for goal-setting; do not equate limited English with limited parenting. [15] [17]
Out-of-home care. Clarify consent, ensure a durable medical home and chase incomplete referrals aggressively. [12] [16]
Socioeconomic disadvantage. Transport support, flexible hours and co-located services reduce dropout. [15] [16]
Adolescents with late-recognised needs. EI principles still apply as “timely support,” then link transition planning. [19]
Evidence, Guidelines & Regional Differences
Global intellectual spine. AAP surveillance/screening algorithms (2006, Lipkin 2020) and milestone modernisation (Zubler) anchor identification. Adams links medical home to Part C early intervention collaboration in the US. Novak summarises earlier CP diagnosis and intervention. Cochrane reviews (Orton/Spittle lineage) synthesise post-discharge developmental programmes for preterm infants. Dawson’s ESDM RCT and later Rogers multi-site work inform autism early intervention evidence with evolving effect sizes. Guralnick updates EI for intellectual disability. NICE preterm follow-up principles are summarised for clinicians by McKinnon. AAP care-coordination and medical-home statements define system roles. Family quality-of-life reviews remind you that EI is also a family intervention. [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [23]
Australia / Aotearoa New Zealand. Community child health, allied health and disability support systems vary by jurisdiction and funding stream. Teach principles: early referral, family goals, care coordination; check current local pathways rather than freezing another country’s entitlement list. [4] [11]
United Kingdom. NICE-linked developmental follow-up for preterm children and multi-agency early help frameworks are high-yield; use local integrated care pathways. [10]
United States. IDEA Part C early intervention for eligible infants and toddlers collaborates with the medical home; IFSP language is exam-familiar. State implementation varies. [4] [12]
Canada. Provincial delivery varies; family-centred care coordination principles still apply. [11]
Controversies. How intensive is intensive enough; waitlist rationing; commercial unregulated programmes; balancing neurodiversity-affirming language with evidence-based early support; and avoiding overtesting while not missing treatable disease. [7] [8] [22]
Use jurisdictional community child health and disability support pathways. Refer early, write family goals, and verify current local access rules rather than memorising another country’s hours. [4] [11]
NICE-informed preterm developmental follow-up and multi-agency early help language are exam-safe frames; always name the local integrated pathway. [10]
US Part C / IFSP collaboration with the medical home is a classic teaching model; Canadian services are provincial with shared family-centred coordination principles. [4] [11] [12]
Exam Pearls
- Refer early—do not wait for a perfect label. [1] [4]
- Parental concern is data. [1] [3]
- Hearing and vision early. [1] [3]
- EI and diagnostic work-up run in parallel. [4] [5]
- Family goals beat therapist-only goals. [11] [23]
- Key worker reduces fragmentation. [11] [18]
- Safety-net the waitlist. [1] [4]
- Regression is urgent until proven otherwise. [5]
- Same referral ≠ same access. [15] [16]
- Name the jurisdiction before quoting entitlement hours. [4]
REFER early
References
- [1]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening Pediatrics, 2020.PMID 31843861
- [2]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools Pediatrics, 2022.PMID 35132439
- [3]Council on Children With Disabilities Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening Pediatrics, 2006.PMID 16818591
- [4]Adams RC Early intervention, IDEA Part C services, and the medical home: collaboration for best practice and best outcomes Pediatrics, 2013.PMID 24082001
- [5]Novak I Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment JAMA pediatrics, 2017.PMID 28715518
- [6]Orton J Early developmental intervention programmes provided post hospital discharge to prevent motor and cognitive impairment in preterm infants The Cochrane database of systematic reviews, 2024.PMID 38348930
- [7]Dawson G Randomized, controlled trial of an intervention for toddlers with autism: the Early Start Denver Model Pediatrics, 2010.PMID 19948568
- [8]Rogers SJ A Multisite Randomized Controlled Two-Phase Trial of the Early Start Denver Model Compared to Treatment as Usual Journal of the American Academy of Child and Adolescent Psychiatry, 2019.PMID 30768394
- [9]Guralnick MJ Early Intervention for Children with Intellectual Disabilities: An Update Journal of applied research in intellectual disabilities : JARID, 2017.PMID 26764896
- [10]Mckinnon K Developmental follow-up of children and young people born preterm, NICE guideline 2017 Archives of disease in childhood. Education and practice edition, 2019.PMID 29802095
- [11]Council on Children with Disabilities and Medical Home Implementation Project Advisory Committee Patient- and family-centered care coordination: a framework for integrating care for children and youth across multiple systems Pediatrics, 2014.PMID 24777209
- [12]Medical Home Initiatives for Children With Special Needs Project Advisory Committee The medical home Pediatrics, 2002.PMID 12093969
- [13]Garner AS Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health Pediatrics, 2012.PMID 22201148
- [14]Shonkoff JP The lifelong effects of early childhood adversity and toxic stress Pediatrics, 2012.PMID 22201156
- [15]Coker TR Well-child care clinical practice redesign for serving low-income children Pediatrics, 2014.PMID 24936004
- [16]Council on Community Pediatrics Poverty and Child Health in the United States Pediatrics, 2016.PMID 26962238
- [17]Berman RS Screening for Poverty and Poverty-Related Social Determinants of Health Pediatrics in review, 2018.PMID 29716966
- [18]Bell A Collaborative transdisciplinary intervention in early years - putting theory into practice Child: care, health and development, 2010.PMID 19961502
- [19]White PH Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home Pediatrics, 2018.PMID 30348754
- [20]Earls MF Incorporating Recognition and Management of Perinatal Depression Into Pediatric Practice Pediatrics, 2019.PMID 30559120
- [21]Committee on Practice and Ambulatory Medicine 2023 Recommendations for Preventive Pediatric Health Care Pediatrics, 2023.PMID 36938620
- [22]Størdal K Overtesting and overtreatment-statement from the European Academy of Paediatrics (EAP) European journal of pediatrics, 2019.PMID 31506723
- [23]Pérez-Granado S Family quality of life in early intervention: systematic review and meta-analysis Frontiers in pediatrics, 2026.PMID 42422446
- [24]Committee on Practice and Ambulatory Medicine, Bright Futures Periodicity Schedule Workgroup 2021 Recommendations for Preventive Pediatric Health Care Pediatrics, 2021.PMID 33593848