Paeds · growth-development-and-behaviour
Family-centred developmental care and goal setting
Also known as Patient and family-centered care · Family-centered developmental care · Goal attainment scaling paediatrics · COPM paediatric goals · F-words child development · Shared decision making disability · ICF-CY goal setting
Fellowship-level approach to family-centred developmental care and goal setting: PFCC principles, ICF-CY and F-words framing, SMART/GAS/COPM goals, shared decisions, structural barriers, and regional service models.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Developmental care fails when professionals set goals that families cannot own. The child may need therapy, equipment, school support and medical surveillance — but the family lives the timetable. Family-centred practice treats caregivers as experts on their child, shares honest information, and makes decisions together. That is clinical skill, not soft optional extras. [1] [7]
Patient- and family-centred care (PFCC) in AAP framing rests on dignity and respect, information sharing, participation and collaboration. In developmental services the same principles apply across clinic, home visiting, school and hospital. A family sitting in the room while you dictate six unprioritised targets is not family-centred care. [1]
Goal setting turns values into a plan you can review. Good goals are few, meaningful, observable and owned. Tools such as the Canadian Occupational Performance Measure (COPM) and Goal Attainment Scaling (GAS) help individualise and track change without pretending every child fits a standard score. [5] [6]
Classification
Organise developmental planning on three layers: what the child can do (function), what roles they join (participation), and what the environment enables or blocks. The WHO ICF-CY supplies that language: body functions and structures, activities, participation, plus environmental and personal factors. Use it so goals are not only “increase range of motion” when the family wants “join playground play.” [8] [10]
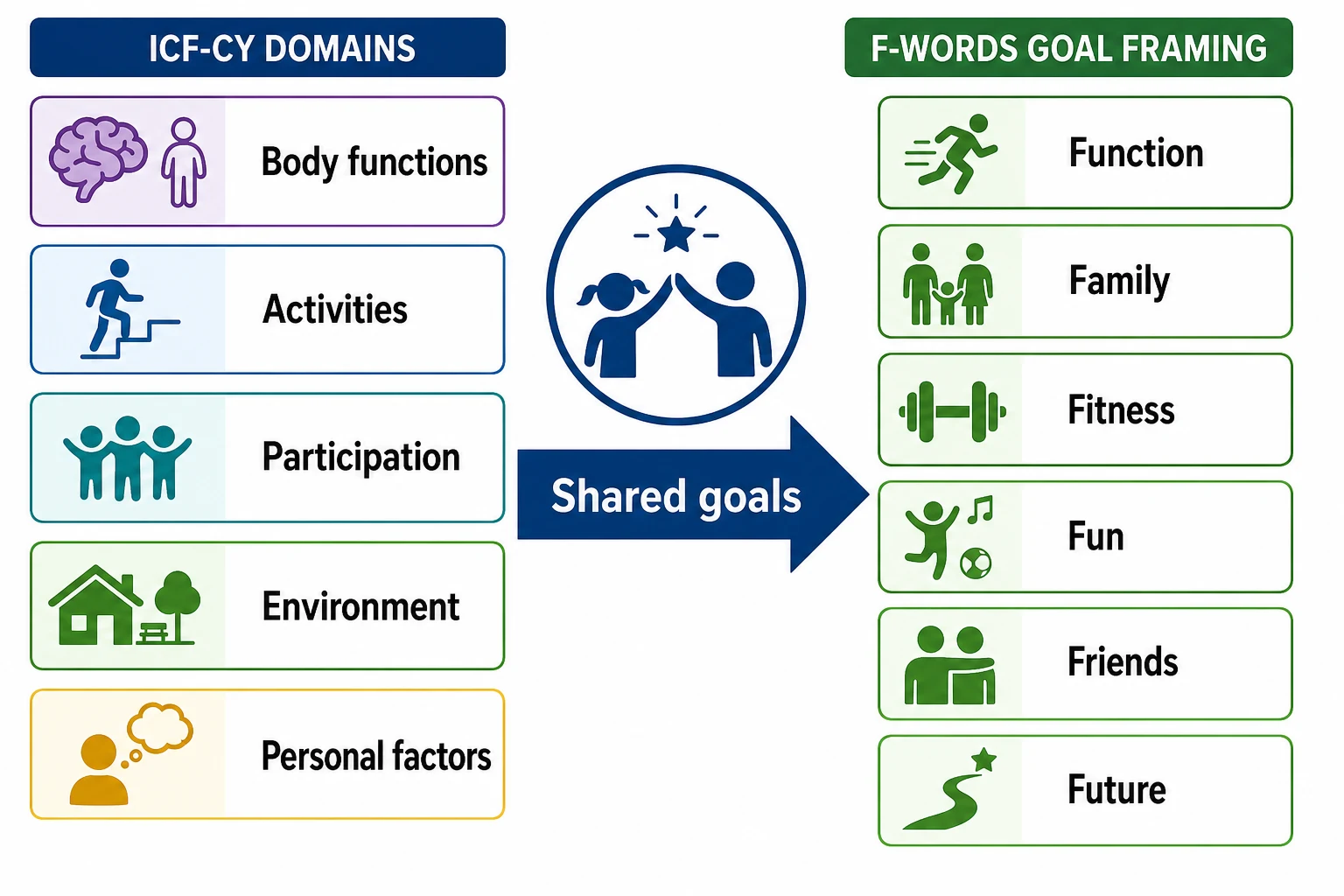
F-words for child development (CanChild tradition) translate ICF ideas into clinic English: Function, Family, Fitness, Fun, Friends, Future. Families and educators use this language to keep plans human. Recent work describes family and provider experiences of F-words tools and training. [11] [12]
| Frame | Use in clinic | Goal example |
|---|---|---|
| Impairment | Necessary medical/therapy targets | Reduce painful tone limiting seating |
| Activity | Everyday tasks | Transfer with one assist |
| Participation | Life roles | Attend two school sports sessions weekly |
| Environment | What must change around the child | Ramp, transport, interpreter, equipment |
| F-words check | Balance the plan | Fun and friends not deleted by therapy load |
Epidemiology & Risk Factors
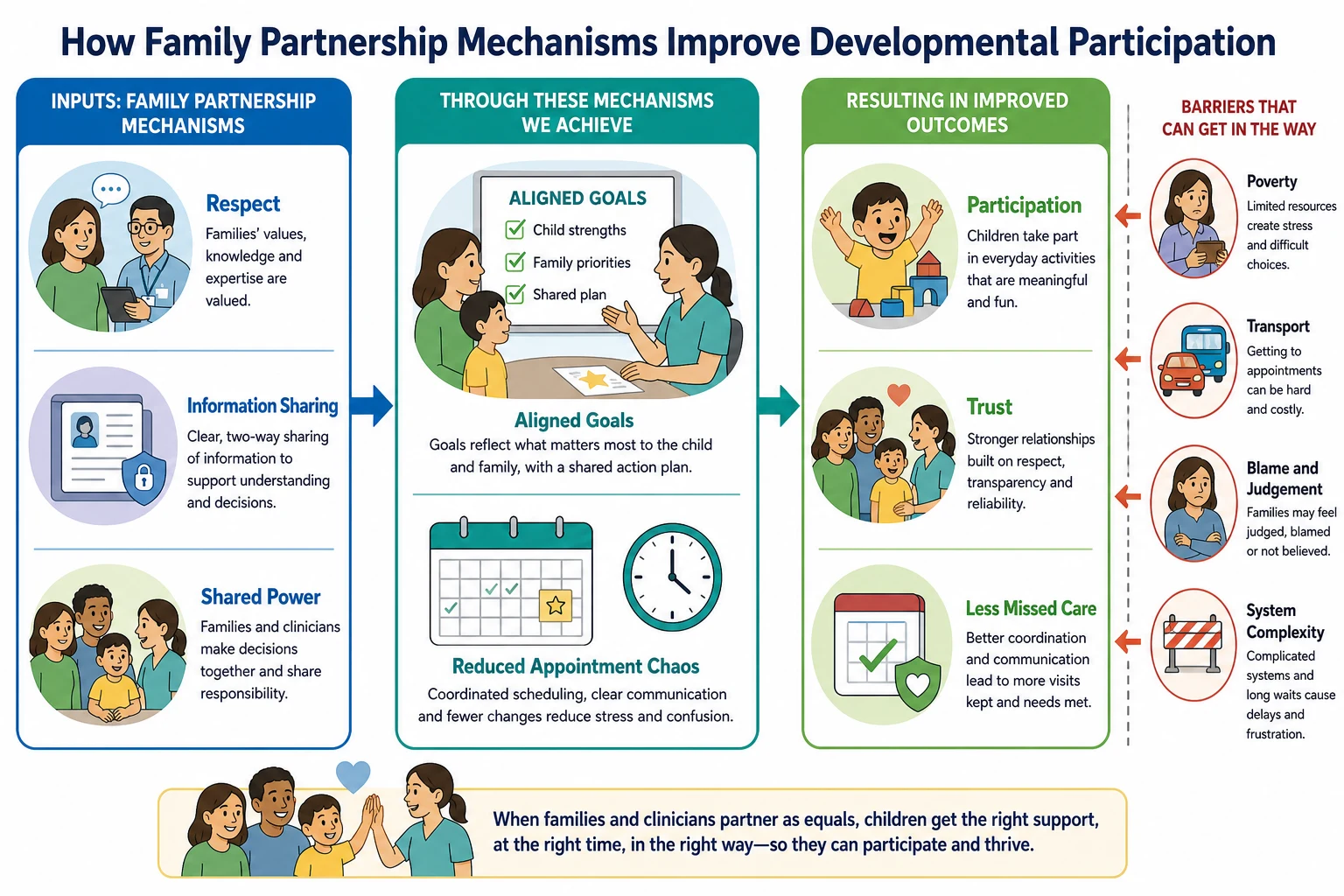
Every family deserves partnership; not every system delivers it. Risk of poor partnership rises with poverty, language barriers, racism, rural distance, caregiver mental health load, and multi-service complexity. Public health and paediatric roles intersect here: the medical home cannot outsource dignity. [3] [4]
Home visiting is a structured way to bring services into family space and support early development. It is one evidence-informed model for engaging families under stress, not a universal replacement for clinic care. [2]
Service providers describe family-centred approaches as relational and adaptive — yet structural delivery problems still shape parent experience. King and colleagues link system design to whether parents feel care is truly family-centred. [7] [13]
Pathophysiology
There is no enzyme pathway for partnership, but there is a mechanism of engagement. Trust grows when information is honest and timely. Shared power reduces hidden non-adherence. Aligned goals free cognitive load for the family. Mismatched goals raise stress, missed visits and conflict between school and clinic. [1] [13]
Participation restriction is the clinically meaningful “end organ” for many developmental plans. ICF-CY tools help quantify function and participation beyond a single diagnosis label, including for children with communication and cognitive challenges. [8] [10]
Clinical Presentation
You will hear partnership failure before you see it on a growth chart. Families cancel, arrive late, or seem “unmotivated.” Caregivers may say every professional wants something different. Adolescents may disengage when goals are parental only. Sibling needs surface as “we cannot do another appointment.” [7] [13]
A high-yield presentation is the post-intervention goal gap: after surgery or a new therapy block, professionals track technical outcomes while the young person wanted a participation goal such as dressing or sport. Patient-defined goals in cerebral palsy upper-limb care illustrate that mismatch risk. [9] [5]
Differential Diagnosis
| Surface story | Partnership-centred reading | Alternative that must not be missed |
|---|---|---|
| Missed appointments | Unrealistic timetable; no key worker | Avoidance of an unsafe home visitor or concealed safeguarding issue |
| “Won’t do exercises” | Goals not meaningful; pain; equipment missing | Depression, misunderstanding, or true capacity limit |
| School vs clinic conflict | Different participation priorities | Learning need or bullying unrecognised |
| Parent disagrees with diagnosis | Need time, second opinion, cultural framing | Factitious disorder or harmful denial of clear risk |
| Adolescent refuses plan | Autonomy and identity | Capacity concerns, mental health crisis |
Safeguarding is not cancelled by family-centred language. If a child is unsafe, act. Partnership continues around the safety plan, not instead of it. [1]
Clinical & Bedside Assessment
Open with: “What would make the next three months a success for you and your child?” Then map the current service load. Count appointments. Ask who else sets goals (school, NDIS/early intervention, therapists). Check language needs and decision preferences. [1] [7]
Minimum partnership assessment: [1] [11]
- Child and family priorities (F-words prompt if helpful). [11]
- Current function and participation (ICF-CY thinking). [8]
- Barriers: money, transport, housing, work, sibling care, digital access. [4]
- Who must be in the room for real decisions?
- How will we know a goal is met?
When occupational performance priorities matter, COPM-style interviewing surfaces the tasks the family values most. In intensive care rehabilitation, COPM has been used to individualise goals beyond generic pathways. [6]
Investigations
You do not order a “family-centred blood test.” Investigation here means structured tools and documentation: [1] [8]
- ICF-CY-based checklists to describe impairment, activity and participation. [8] [10]
- Written goal sheets with baseline, target and review date. [5]
- Developmental and medical assessments as inputs to goals, not substitutes for them. [1]
- Social needs screening when poverty or housing will sink the plan. [4] [14]
Management — Resuscitation
In crisis, stabilise the child first. Then stabilise the plan. A family in housing crisis or acute hospitalisation cannot absorb ten new therapy targets. Prioritise safety, feeding, sleep, pain and one or two participation anchors. Name a single contact person. Stop contradictory advice between teams the same day. [1] [14]
Management — Definitive & Stepwise
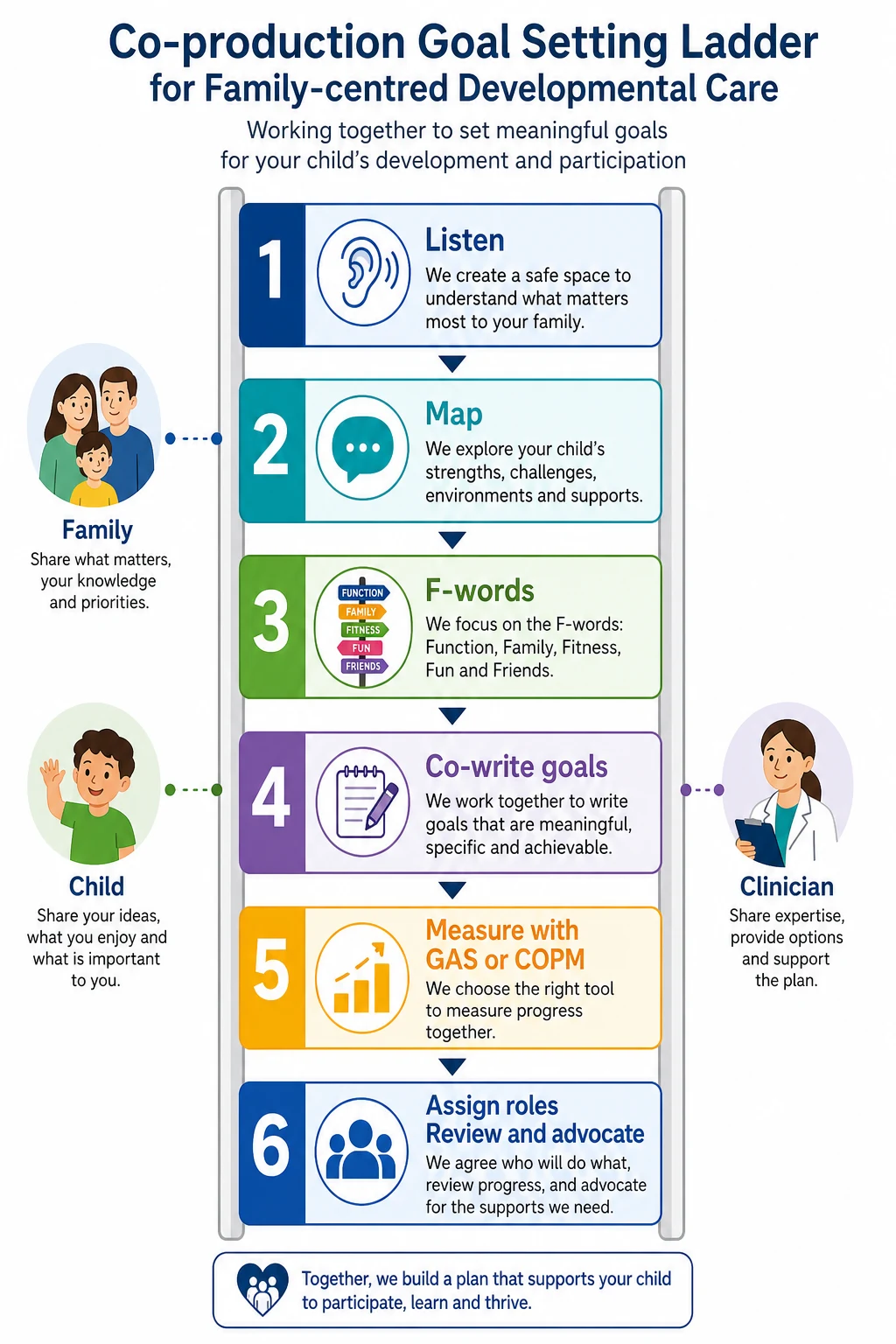
Use a ladder you can recite in viva: [1] [5]
- Listen to child and family priorities without interrupting to “correct” them. [1]
- Translate into F-words / ICF-CY so the team shares a map. [11] [8]
- Co-write 2–4 goals that are specific, measurable, achievable, relevant, time-bound. [5]
- Choose a measurement style when useful: COPM for occupational performance priorities; GAS for graded attainment levels. [5] [6]
- Assign roles (who books, who practices, who funds equipment, who speaks to school). [7]
- Review on a named date; retire goals that no longer matter. [1]
- Advocate when systems block progress. [3] [13]
Shared decision-making in practice. Offer options with benefits, burdens and uncertainty. Check understanding with teach-back. Document the chosen plan in plain language. For home-based support, consider early childhood home visiting pathways where available and appropriate. [1] [2]
Co-production in one clinic visit
Ask what matters this season
Map F-words and barriers
Write two shared goals
Name owners and review date
Send a plain-language summary
Specific Subtypes & Scenarios
New developmental diagnosis. Families need time. Early goals should include family understanding and support, not only therapy hours. [1] [2]
Orthopaedic or tone intervention in cerebral palsy. Capture goals with GAS/COPM so success is not only radiographic or range-of-motion change. [5] [9]
PICU and step-down rehabilitation. COPM can individualise rehab targets when generic pathways miss family priorities. [6]
School conflict. Align health goals with classroom participation; invite education partners with family consent. [11] [12]
Adolescent ownership. Shift the conversation toward the young person’s Future and Friends goals; support supported decision-making. [1] [9]
Material hardship. A participation goal fails if there is no transport or food security. Fix barriers as part of the developmental plan. [4] [14]
Complications & Pitfalls
- Tokenism: family present, power unchanged. [1] [13]
- Impairment-only plans that erase fun and friends. [11]
- Goal inflation — twelve targets, zero progress. [5]
- Professional territorial fights played out through the child. [7]
- Ignoring structural barriers then diagnosing non-compliance. [13] [4]
- Excluding the child’s voice when it is available. [1]
Prognosis & Disposition
Plans owned by families are more likely to be lived. Disposition is not only “review in clinic.” It is a written goal plan, a named key contact, a review date, and clear routes to escalate equipment, funding or safeguarding. Public health partnerships and medical-home continuity improve the odds that goals survive real life. [1] [3]
Disposition rules of thumb: [1] [13]
- Home with a co-written plan and early check-in if goals are new. [1]
- Multidisciplinary case conference when services conflict or overload. [7]
- Advocacy/legal pathways when entitlement barriers block essential supports. [13]
- Safety pathway first if the child is at risk. [1]
Special Populations
Infants need caregiver coaching and home-based options. School-age children live goals across classroom and sport. Adolescents need autonomy-respecting processes. Indigenous and migrant families need culturally safe partnership and interpreters, not faster talking. Out-of-home care requires clarity on who holds decision authority. Technology-dependent children need goals that include equipment reliability and carer capacity. [1] [2] [4]
Evidence, Guidelines & Regional Differences
Anchor policy: AAP Patient- and family-centered care and the pediatrician’s role (2012). Complementary AAP work on home visiting, poverty, and paediatric public health roles frames the system context. Measurement literature supports GAS and COPM for individualised goals, including after orthopaedic intervention and in ICU-based rehab. ICF-CY tools structure function and participation assessment. F-words research describes family and provider uptake. King and colleagues show structural service design shapes whether parents experience true family-centred service. [1] [2] [3] [4] [5] [6] [8] [11] [13]
Regional practice differences
In Australia, early childhood approaches and NDIS planning conversations are core places to practise co-owned goals; in Aotearoa New Zealand, whānau-centred models and Ministry of Education learning support interfaces matter. Use local key-worker models and culturally safe partners. The clinical ladder stays the same. [1] [7]
Exam Pearls
- PFCC four ideas: respect, information, participation, collaboration. [1]
- F-words: Function, Family, Fitness, Fun, Friends, Future. [11]
- ICF-CY stops impairment-only thinking. [8]
- GAS and COPM make individual goals measurable. [5] [6]
- Fewer goals beat more goals. [5]
- Structural barriers can look like non-compliance. [13]
- Safeguarding still applies inside partnership. [1]
- Long-case gold: one participation goal, one barrier fixed, one review date.
Red Flags (quick list)
- Blame without barrier analysis. [13]
- Unsafe child despite “family choice” language. [1]
- Contradictory multi-service goals with no coordinator. [7]
- Adolescent excluded from decisions they can join. [1]
- Housing or food crisis ignored while therapy intensifies. [4] [14]
One-page recovery
Ask what matters, frame with F-words and ICF-CY, write a few co-owned goals, measure if needed with GAS/COPM, fix barriers, review. That is family-centred developmental care under exam pressure. [1] [5] [11]
References
- [1]COMMITTEE ON HOSPITAL CARE and INSTITUTE FOR PATIENT- AND FAMILY-CENTERED CARE Patient- and family-centered care and the pediatrician's role. Pediatrics, 2012.PMID 22291118
- [2]Duffee JH Early Childhood Home Visiting. Pediatrics, 2017.PMID 28847981
- [3]Kuo AA Pediatricians and Public Health: Optimizing the Health and Well-Being of the Nation's Children. Pediatrics, 2018.PMID 29358481
- [4]COUNCIL ON COMMUNITY PEDIATRICS Poverty and Child Health in the United States. Pediatrics, 2016.PMID 26962238
- [5]Carman S Lower limb orthopedic surgery in children and adolescents with cerebral palsy is well captured using individualized Goal Attainment Scale (GAS) and Canadian Occupational Performance Measure (COPM) goals. Disability and rehabilitation, 2025.PMID 40257191
- [6]Hwang Y Individualized Goal Setting for Pediatric Intensive Care Unit-Based Rehabilitation Using the Canadian Occupational Performance Measure. Children, 2023.PMID 37371217
- [7]Britt K Family-centred service in childhood disability: a qualitative study of service providers perspectives on their approaches to practice. Disability and rehabilitation, 2026.PMID 41964287
- [8]Abbas R An international classification of functioning, disability and health-children and youth (ICF-CY) based assessment tool for evaluating impairments, function and participation of children and adolescents with cerebral palsy in special education schools. Pakistan journal of medical sciences, 2026.PMID 42369915
- [9]van Ossenbruggen RM Classification of patient-defined hand-arm treatment goals in young people with cerebral palsy and upper extremity spasticity undergoing upper extremity surgery. Disability and rehabilitation, 2026.PMID 42226630
- [10]Iype M Quantifying Disability in Children Challenged by Communicative and Cognitive Disorders Using the ICF-CY-Checklist: Results of a Cross-Sectional Study of a Retrospectively Assembled Cohort. Pediatric neurology, 2026.PMID 41780223
- [11]Canlas K Families' perspectives and experiences in using the F-words for Child Development in daily life and services. Disability and rehabilitation, 2026.PMID 42400954
- [12]Canlas K Exploring Health Care Providers, Families and Educators' Perceptions of an Online Self-Paced F-Words for Child Development Foundations Course. Child: care, health and development, 2026.PMID 41994940
- [13]King G Does the healthcare system support family-centred service?: linking structural issues in healthcare service delivery to parents' relational experiences of care. Disability and rehabilitation, 2026.PMID 41879330
- [14]Council on Community Pediatrics Providing care for children and adolescents facing homelessness and housing insecurity. Pediatrics, 2013.PMID 23713108