Paeds · growth-development-and-behaviour
Intellectual developmental disorder
Also known as Intellectual disability · Intellectual developmental disorder · IDD · Intellectual disability disorder · Mental retardation (historical term) · Global developmental delay evolving to ID
Fellowship approach to intellectual developmental disorder: dual intellectual and adaptive criteria, severity by adaptive function, GDD-to-ID framing, aetiological evaluation including CMA and genomics, treatable mimics, medical-home longitudinal care, comorbidity without overshadowing, education and transition.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A seven-year-old is referred because school says he is “behind.” He cannot manage classroom routines. He needs help with toileting and dressing. He struggles to learn letter sounds. His parents ask whether he is “just lazy.” Your job is to decide whether this is intellectual developmental disorder, a specific learning disorder, a sensory problem, autism, deprivation, or more than one of these — and then to open help without waiting for every test result. [6] [7]
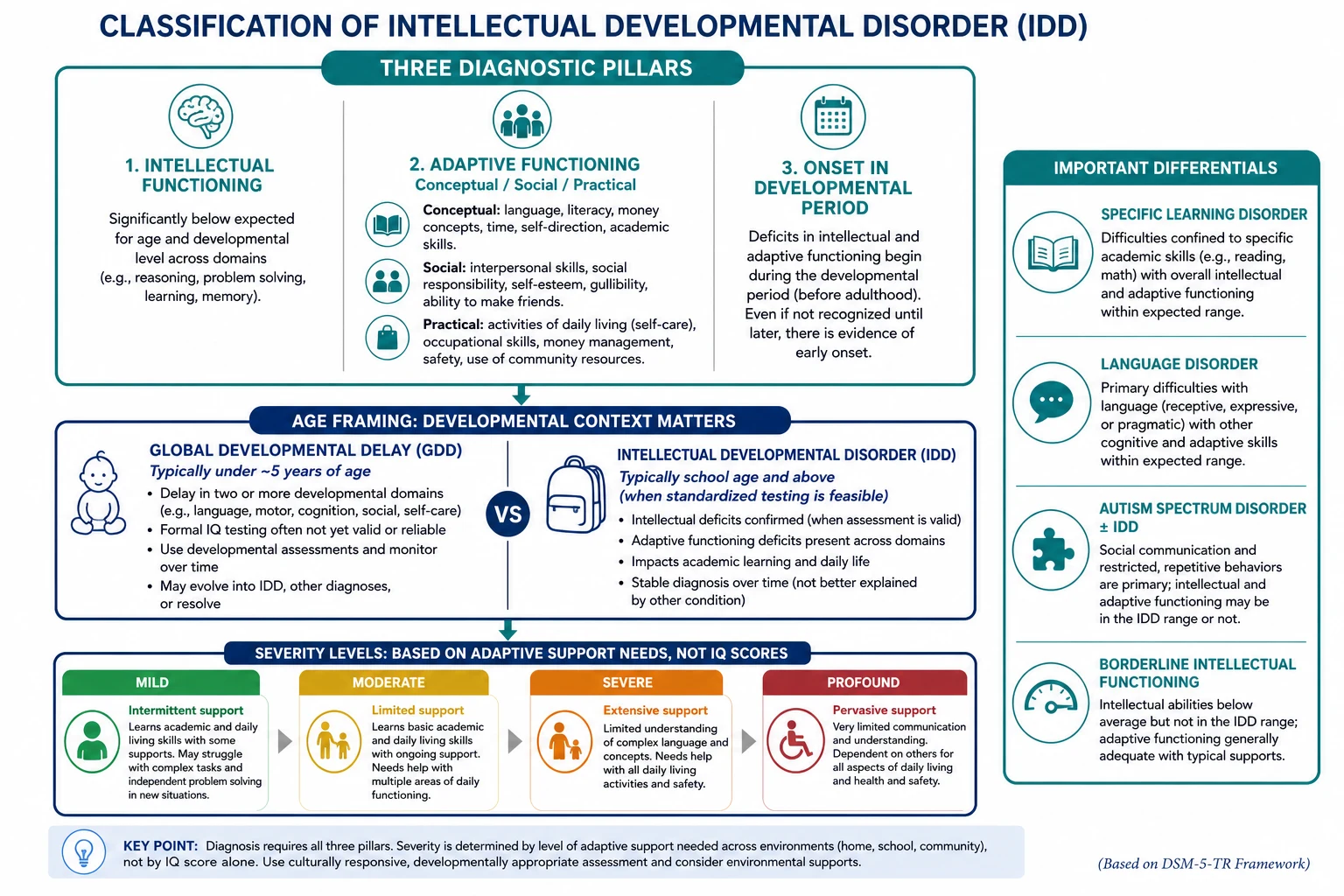
Intellectual developmental disorder (also called intellectual disability) requires three things together: deficits in intellectual functioning, deficits in adaptive functioning, and onset during the developmental period. Adaptive function is not optional decoration. Tassé’s work underlines that intellectual scores and adaptive behaviour are related but not interchangeable; diagnosis needs both. [5] [6]
Adaptive functioning is what the child can do in daily life across three domains. [5] [6]
- Conceptual — language, reading, writing, maths, memory, problem-solving, knowledge. [5]
- Social — communication, friendship, social judgement, gullibility, following social rules. [5]
- Practical — self-care, money and time concepts, transport, safety, school and work routines. [5] [6]
The historical term “mental retardation” is obsolete in clinical communication. Use person-first or identity-respecting language agreed with the family, and keep the diagnostic criteria precise. [6] [7]
This page owns the IDD diagnosis, aetiological evaluation and longitudinal medical-home plan. The broad GDD work-up spine is also covered on the linked global developmental delay page — cross-link it rather than cloning every differential table. Screening systems live on the preventive screening leaf; milestone observation craft lives on surveillance pages. [1] [15] [20]
What to do in the first clinic sequence
Picture the child
History, adaptive domains, exam, hearing and vision pathway.
Name the working problem
GDD if young; possible IDD if school-age criteria can be tested.
Start supports now
Early intervention, education adjustments, safety and family counselling.
Seek aetiology in parallel
CMA first-tier; fragile X when indicated; phenotype-driven next tests.
Plan the long game
Comorbidity surveillance, care coordination, transition.
Classification
Classify four things before you order a panel: the diagnostic construct, the age frame, the severity, and the aetiological class. [1] [6]
Diagnostic construct
| Construct | Core idea | Common exam trap |
|---|---|---|
| IDD / intellectual disability | Intellectual + adaptive deficits, developmental onset | Using IQ alone |
| Global developmental delay | Significant delay in ≥2 domains in a young child | Treating GDD as a final adult diagnosis |
| Specific learning disorder | Academic skill deficit with intellectual functioning not in the IDD range | Calling every school failure “ID” |
| Autism spectrum disorder | Social-communication differences + restricted/repetitive patterns; may co-occur with IDD | Assuming autism excludes IDD or replaces adaptive assessment |
| Borderline intellectual functioning | Cognitive scores near the lower average range without full IDD criteria | Over-labelling or under-supporting |
Age frame: GDD versus IDD
In toddlers and preschoolers, formal IQ testing is often unstable or invalid. Global developmental delay is the working clinical label when a young child has significant delays across multiple domains. Many of these children later meet criteria for IDD; some do not. Moeschler and Bélanger both frame evaluation of GDD and intellectual disability as one clinical continuum of comprehensive assessment. [1] [8]
When age and cooperation allow, use standardised cognitive and adaptive instruments administered by trained professionals. Do not invent proprietary cut-off tables in an exam answer — state the principle: significant intellectual limitation plus significant adaptive limitation. [5] [6]
Severity by adaptive support need
Modern severity bands are driven by adaptive functioning and support needs, not by memorised IQ brackets alone. [6] [7]
- Mild — may acquire basic academic skills; needs support for complex planning, money, social judgement and some daily living tasks. [6]
- Moderate — limited academic attainment; needs ongoing support for personal care, communication and community participation. [6]
- Severe — limited language and self-care; needs extensive support and supervision for safety. [6]
- Profound — very limited symbolic communication and self-care; needs pervasive support, often with major motor or sensory comorbidity. [6] [7]
Aetiological classes
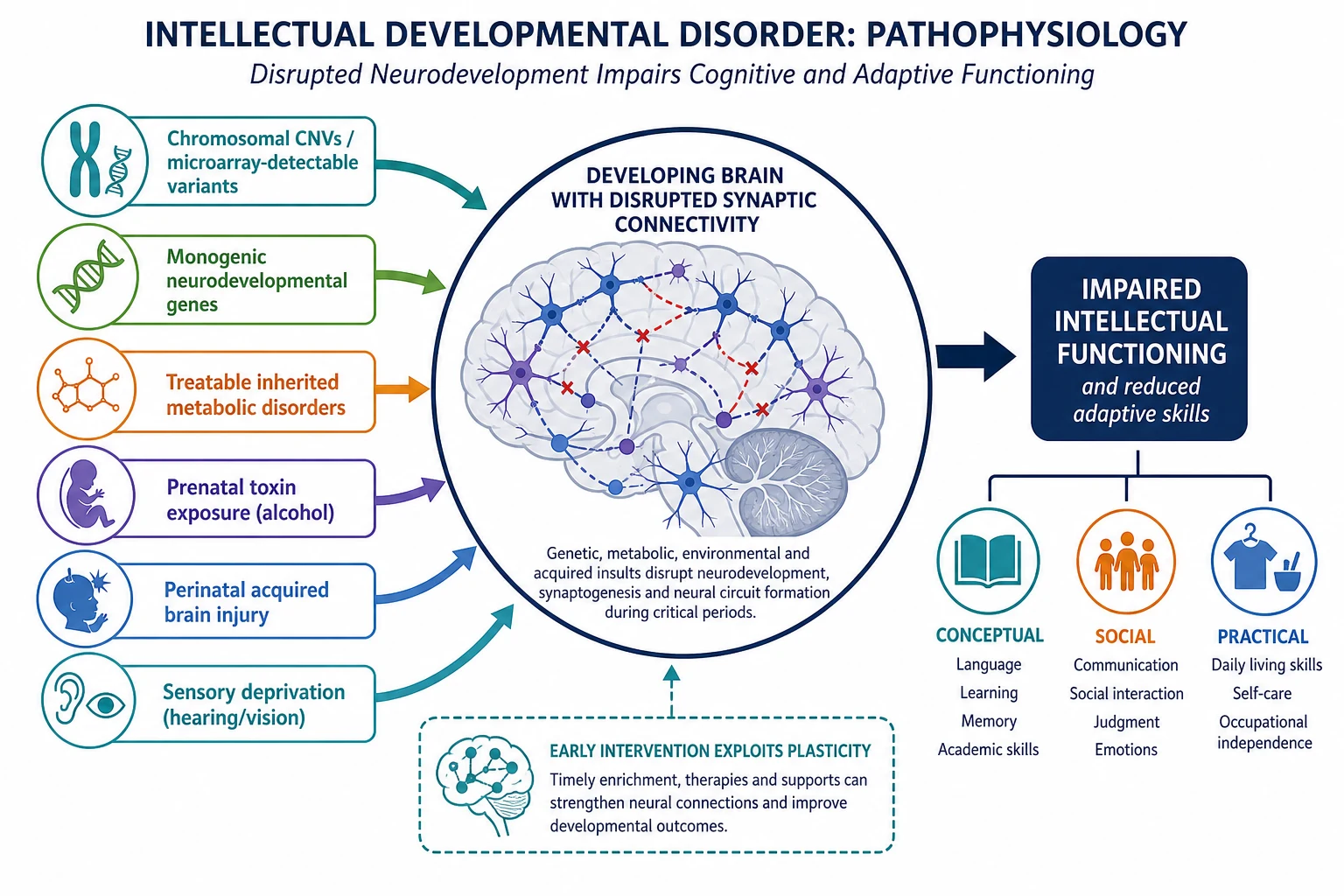
Think in pathways you can act on: chromosomal copy-number variants, monogenic syndromes, treatable inherited metabolic disorders, prenatal toxin exposure (including alcohol), perinatal acquired brain injury, postnatal infection or trauma, severe sensory impairment, and extreme psychosocial deprivation — often combined. [1] [10] [13]
Epidemiology & Risk Factors
Population prevalence of intellectual disability is on the order of about 1%. Maulik’s meta-analysis of population-based studies estimated an overall prevalence of approximately 10.37 per 1000. Mild forms are more common than severe forms. Estimates vary by case definition, age and region. Quote the meta-analysis as an order-of-magnitude anchor, not as your local clinic’s exact rate. [4] [6]
Risk factors and clues include prenatal, perinatal, postnatal and social pathways. [1] [6]
- Prenatal: genetic syndromes, teratogens including alcohol, congenital infection, severe maternal illness. [1] [13]
- Perinatal: extreme prematurity, hypoxic–ischaemic injury, neonatal meningitis or stroke. [1] [8]
- Postnatal: traumatic brain injury, meningitis/encephalitis, severe malnutrition, lead and other neurotoxins, extreme neglect. [1] [6]
- Family and social: consanguinity, affected relatives, poverty, limited service access, language discordance that delays recognition. [1] [19]
Boys appear more often in some clinic cohorts, partly because of X-linked conditions such as fragile X and partly because of referral patterns. Girls with fragile X are still missed when the classic male gestalt is expected. [12]
Common co-travellers include epilepsy, autism spectrum disorder, ADHD, cerebral palsy, sensory impairment, sleep problems, mental health disorders and medical complexity. Dual diagnosis is expected, not exotic. [6] [14] [18]
Pathophysiology
Intellectual developmental disorder is the functional result of disrupted brain development or injury. The shared final pathway is impaired network connectivity for learning, reasoning and adaptive control — not one single lesion. [6] [7]
Genetic and chromosomal pathways. Copy-number variants detectable by chromosomal microarray, aneuploidies such as Down syndrome, and monogenic neurodevelopmental disorders alter neuronal migration, synaptic signalling and circuit maturation. That is why first-tier genomic testing changed yield so dramatically compared with older karyotype-only pathways. [1] [2] [3]
Metabolic pathways. Some inherited metabolic disorders injure the developing brain progressively. A child who “looked delayed” may in fact be losing ground. Treatable-IMD frameworks exist precisely so you do not miss a reversible or stabilisable cause. [10] [9]
Toxic and acquired pathways. Fetal alcohol spectrum disorders damage structure and function across executive, adaptive and learning networks. Perinatal hypoxia, infection and later brain injury produce static or stepwise impairment depending on the insult. [13] [1]
Sensory and environmental pathways. Uncorrected hearing or vision loss, chaotic caregiving, and severe psychosocial deprivation can suppress language and adaptive skill acquisition. Environment can be the main driver or an amplifier of a biological vulnerability. Fix what is fixable while you still look for biology. [1] [15]
Why adaptive function matters biologically. Real-world disability is the mismatch between brain-supported skills and life demands. Two children with similar cognitive scores can function very differently if supports, sensory load, epilepsy control and family capacity differ. [5] [6]
Clinical Presentation
What families and schools actually say
- “He is always behind his cousins.”
- “She still needs help with every button and zip.”
- “He is friendly but gets exploited by other children.”
- “Homework ends in tears every night.”
- “They said he has a learning difficulty — but he cannot manage lunch money or the bus.”
- “She was slow from the start and never caught up.” [6] [7]
Age-patterned presentations
Infants and toddlers. Delayed motor and language milestones, poor problem-solving with toys, limited gesture, feeding difficulty, and caregiver concern that “something is not building.” Surveillance and standardised screens should already have flagged risk. [15] [20]
Preschool. Multi-domain delay, limited pretend play, difficulty with toilet training and following simple routines, possible dysmorphic or growth clues. This is classic GDD territory. [1] [8]
School-age mild IDD. Often mislabelled as laziness or pure specific learning disorder. Look for broad academic struggle plus adaptive gaps in self-care, social judgement and practical independence. [6] [7]
Moderate to profound IDD. Earlier recognition is common. Limited language, high support needs, frequent medical comorbidity, and major family care load. [6] [18]
Adolescence. Undiagnosed mild IDD may surface as mental health crisis, school refusal, exploitation, justice contact, or failure of independent living skills. Transition planning is already overdue. [17] [6]
Clues that push aetiology
Dysmorphic features, micro- or macrocephaly, growth failure, neurocutaneous signs, congenital anomalies, epilepsy, movement disorder, known prenatal alcohol exposure, or a pedigree with intellectual disability or premature ovarian failure (fragile X family clue) change the genetic and metabolic urgency. [1] [12] [13]
Differential Diagnosis
Ask: is this IDD, something that mimics IDD, or IDD plus something else? [6] [8]
| Pattern | Prefer | Also consider | Do not assume |
|---|---|---|---|
| Broad delay + adaptive gaps | IDD / GDD pathway | Sensory loss, medical illness | “Just immature” |
| Academic failure with preserved adaptive skills and non-ID cognition | Specific learning disorder | ADHD, attendance problems | Automatic IDD label |
| Social-communication differences ± restricted patterns | Autism evaluation | Autism + IDD dual diagnosis | That autism excludes ID testing |
| Isolated language lag | Hearing loss, language disorder | Bilingual tempo with true delay still needing action | Cognitive impairment without testing |
| Progressive loss of skills | Neurodegenerative / metabolic disease | Epileptic encephalopathy | Static IDD without rethink |
| Marked deprivation history | Psychosocial deprivation ± biological IDD | Maltreatment, PTSD | That social history cancels genetic testing |
| New behaviour change in known IDD | Pain, seizure, abuse, mental illness, constipation, dental disease | “Baseline behaviour” | Diagnostic overshadowing |
Clinical & Bedside Assessment
History that earns marks
Take a developmental biography: pregnancy, alcohol and medication exposures, birth and neonatal course, milestones, plateaus or regression, seizures, sleep, hearing and vision, school trajectory, and a three-generation pedigree. Map adaptive skills with concrete examples — not “copes okay.” Ask what the child can do alone at home, in the community and at school. [1] [8] [13]
Use professional interpreters when language discordance exists. A developmental history taken through a child translator is unsafe. [19]
Examination
Measure growth and head circumference. Perform a careful dysmorphology and skin survey. Complete a neurological exam. Look for congenital anomalies. Observe communication, play, attention and how the child uses the caregiver. Document a clear baseline function so future clinicians can recognise change. [1] [8]
Adaptive domains at the bedside
Walk through conceptual, social and practical skills with age-matched expectations. Example for a school-age child: Can they tell time concepts? Manage simple money? Stay safe near roads? Maintain friendships without exploitation? Complete hygiene with prompts only? Those answers often decide severity more honestly than a single clinic IQ anecdote. [5] [6]
Formal testing
Request standardised cognitive and adaptive assessments through psychology or neurodevelopmental services when age-appropriate. Interpret results with the child’s language, culture, sensory status and cooperation in mind. Re-test if illness, trauma or sensory barriers contaminated the first attempt. [5] [6]
Screen for co-occurring conditions
Autism, ADHD, anxiety, depression, epilepsy, sleep apnoea, feeding difficulty and sensory impairment are common. Assess them on their own merits. Hyman’s autism clinical report is the cross-link for autism pathways; do not collapse every social difference into IDD or every IDD into autism. [14] [6]
Investigations
Investigations answer two questions: what caused this? and is anything treatable or surveillance-changing? Supports do not wait for the answer. [1] [8]
First-line principles
- Hearing and vision pathways are non-negotiable when communication or learning is impaired. [1] [15]
- Chromosomal microarray is a first-tier clinical diagnostic test for individuals with developmental disabilities or congenital anomalies (Miller consensus). ACMG array guidance supports array-based technology for detecting chromosomal imbalance in this setting. [2]
- Fragile X testing remains a core consideration, especially with suggestive phenotype, male sex with X-linked pedigree clues, or family history features such as fragile X–associated conditions. Follow local genetics pathways and Hersh health-supervision context once fragile X is confirmed. [12] [1]
- Metabolic testing is phenotype-driven. Prioritise when there is regression, episodic decompensation, consanguinity, specific exam clues, or other red flags for treatable inherited metabolic disease. Van Karnebeek’s treatable-IMD review exists to stop “static label, no rethink.” [10] [9]
- Exome or genome sequencing is supported by the 2021 ACMG evidence-based guideline as a first- or second-tier test for pediatric patients with congenital anomalies or intellectual disability, within the guideline’s scope and after appropriate counselling. Local access and funding differ — name the principle, then your service pathway. [3]
- MRI brain is not automatic for every mild static non-syndromic presentation. It is more useful with abnormal neurology, focal signs, micro/macrocephaly, seizures, stepwise course or other phenotype prompts. Follow local neurology advice rather than inventing a universal imaging rule. [1] [8]
Low-value moves
Shotgun panels without consent or phenotype. Repeating the same normal CMA under a new brand name. Delaying therapy until “the gene comes back.” Ordering invasive tests before hearing has been checked. [1] [3]
Historical parameters still tested in exams
Shevell’s older AAN/CNS practice parameter and Michelson’s evidence report shaped earlier GDD testing algorithms. They are partly superseded by microarray-first and broader genomic practice, but examiners still expect you to know the trajectory from those documents to Moeschler, Miller and Manickam. [9] [1] [2] [3]
Management — Resuscitation
Most IDD care is longitudinal. Still, convert fast when the child is unsafe or acutely ill. [18]
- ABCDE first for encephalopathy, status epilepticus, shock, severe respiratory compromise or trauma.
- Do not blame “baseline behaviour” for reduced responsiveness, new aggression with fever, or refusal to walk. Search for pain, sepsis, raised intracranial pressure, metabolic crisis, constipation, dental abscess and abuse. That is anti-overshadowing in practice. [18] [6]
- Regression with neurological red flags is an urgent diagnostic pathway, not a routine psychology waitlist. [10] [1]
- Safeguarding concern supersedes elective developmental paperwork. Protect the child, then continue the developmental plan. [16]
- Carry an emergency information summary for complex children: diagnoses, baseline communication, seizures, medications, airway risk and decision-makers. [18]
Management — Definitive & Stepwise
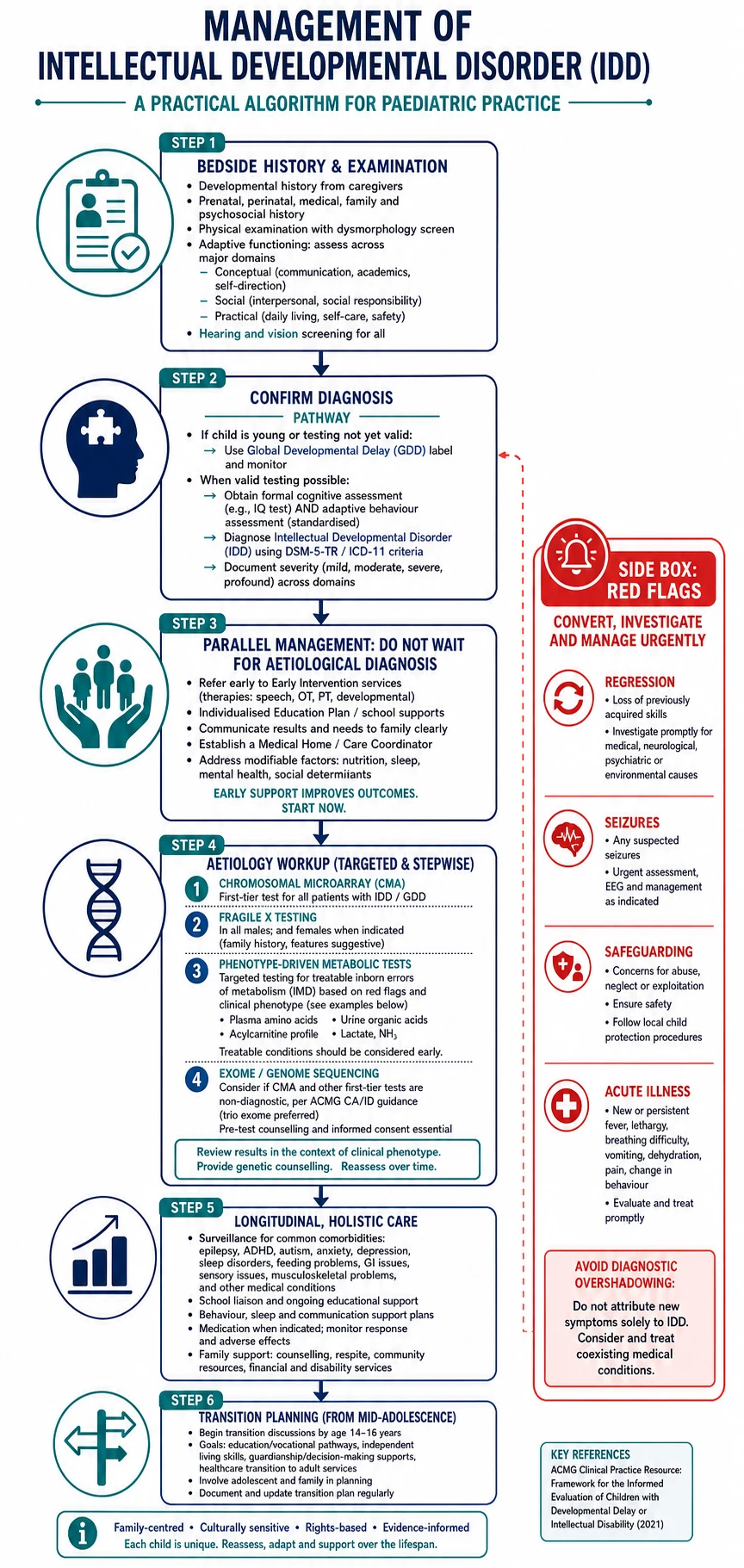
- Confirm the working diagnosis. GDD in the young child; formal cognitive and adaptive assessment when valid. State severity by adaptive support need. [5] [6] [8]
- Start intervention in parallel. Speech, occupational and physiotherapy, early childhood intervention, education adjustments, behaviour support and caregiver coaching do not wait for genetics. [1] [15] [16]
- Run aetiology testing as above: CMA first-tier; fragile X when indicated; metabolic tests for red flags; ES/GS per ACMG CA/ID guidance and local access; imaging when neurologically indicated. [2] [3] [10]
- Counsel with precision and humanity. Explain what IDD means, what it does not mean, uncertainty, recurrence risk pathways via genetics, and the service map. Use teach-back. Offer written plain-language summaries. [1] [6]
- Build the medical home plan. Immunisation, growth, dental, vision, hearing, sleep, feeding, continence, sexual health in adolescence, mental health and comorbidity surveillance. Care coordination is clinical work, not admin fluff. [16] [18]
- Treat comorbidities as real diseases. Epilepsy, autism, ADHD, anxiety, reflux, constipation and pain all deserve proper pathways. Medication for behaviour is never a first substitute for communication support, sleep care and functional analysis. [14] [6]
- Partner with education. Share functional strengths and support needs. Advocate for reasonable adjustments and safety. Review the plan when the child changes schools. [16]
- Plan transition early. White’s medical-home transition framework expects preparation from adolescence, not a surprise discharge at 18. Address decision-making supports, adult services, sexual health, mental health and emergency plans. [17]
- Close loops. Genetics results need a named interpreter of meaning. Therapy referrals need owners and dates. Safety-net regression, new seizures and safeguarding. [16] [3]
Specific Subtypes & Scenarios
Toddler with multi-domain delay. Call it GDD, open early intervention, check hearing/vision, start aetiology evaluation, and reassess over time for IDD criteria. [1] [8] [15]
School-age mild IDD. Distinguish from specific learning disorder by adaptive breadth. Support school and practical independence; still consider genetic evaluation if not previously done. [6] [7]
Down syndrome. Use Bull’s health-supervision framework for surveillance (cardiac, thyroid, hearing, vision, sleep-disordered breathing, atlantoaxial concerns as indicated, development and behaviour). IDD is expected but severity and comorbidities vary. [11]
Fragile X syndrome. Follow fragile X health-supervision principles for medical and developmental surveillance once molecularly confirmed; counsel the wider family because of X-linked inheritance and premutation risks. [12]
Fetal alcohol spectrum disorders. Hoyme’s diagnostic guidelines structure dysmorphology and neurodevelopmental assessment after confirmed or unknown prenatal alcohol exposure. IDD may be part of the neurodevelopmental profile; supports and safeguarding still run in parallel. [13]
Treatable metabolic ID. Regression, consanguinity, decompensation with illness, or specific biochemical clues should trigger urgent metabolic pathways rather than a static label. [10]
IDD plus autism. Dual diagnosis is common. Each condition needs explicit assessment and support planning. [14]
Severe IDD with medical complexity. Technology dependence, feeding tubes, epilepsy and high care load need CMC-style care coordination and anti-overshadowing discipline. [18] [16]
Rural waitlists. Start local therapy and education supports, use telehealth where safe, and escalate red flags without waiting for a capital-city genetics slot. [16]
Complications & Pitfalls
- Diagnosing from a single cognitive score. [5]
- Wait-and-see after clear multi-domain delay. [15]
- Missing treatable metabolic disease. [10]
- Diagnostic overshadowing of pain, seizure, abuse or mental illness. [18] [6]
- Ignoring hearing and vision. [1]
- Delaying early intervention for “results first.” [1] [16]
- Confusing specific learning disorder with IDD. [6]
- Ordering genomic tests without counselling about uncertainty and secondary findings pathways. [3]
- No transition plan. [17]
- No interpreter, then calling the family “poor historians.” [19]
Prognosis & Disposition
Functional prognosis depends on severity, aetiology, comorbidities, timing of supports, education quality and family/system resources. Mild IDD with strong supports can include substantial community participation and, for some adults, supported employment. Severe and profound IDD usually need lifelong pervasive supports. Aetiology-specific risks (for example cardiac disease in Down syndrome) change surveillance more than they erase the need for educational support. [6] [11] [4]
Disposition after diagnosis should name owners and review points. [16]
- Medical home with named care coordinator roles. [16]
- Education and therapy plan with review dates. [16]
- Genetics follow-up when a variant or syndrome is found. [3]
- Specialty clinics as phenotype demands (neurology, metabolics, developmental paediatrics). [1]
- Earlier review if regression, new seizures, safeguarding concern or major placement change. [1] [10]
Transition readiness — knowledge of conditions, emergency plans, adult providers, decision supports — is an outcome you can measure, not a birthday. [17]
Special Populations
High-risk neonates and infants. NICU graduates need intensified surveillance; GDD may declare later. Corrected age is used for early milestone interpretation per local neonatal follow-up practice, but persistent multi-domain delay still needs action. [15] [20]
Children with medical complexity. Baseline-aware assessment prevents both over-investigation of stable features and under-reaction to new decline. [18]
Indigenous families. Use culturally safe practice, local Aboriginal/Torres Strait Islander or Māori health pathways as relevant, and avoid deficit-only framing. Service access barriers are clinical problems. [16]
Migrant and refugee families. Interpreters, trauma-informed pacing, catch-up health care and careful explanation of disability systems. [19]
Out-of-home care and youth justice. Incomplete histories, missed diagnoses and high trauma load are common. Mild IDD is easy to miss and highly consequential for consent, interviewing and sentencing contexts. [6] [17]
Adolescents exploring identity and relationships. Capacity assessment must be individualised. Provide accessible sexual health education and safeguarding. [17]
Evidence, Guidelines & Regional Differences
Core evidence spine for this leaf includes the following anchors. [1]
- Moeschler 2014: comprehensive evaluation of ID/GDD in paediatrics. [1]
- Miller 2010: CMA as first-tier for developmental disabilities/congenital anomalies. [2]
- Manickam 2021 ACMG: ES/GS for pediatric congenital anomalies or intellectual disability. [3]
- Maulik 2011: prevalence meta-analysis (~10.37/1000 overall). [4]
- Tassé 2016: adaptive behaviour essential to diagnosis. [5]
- Patel 2020 and Purugganan 2018: clinical primers/reviews for bedside framing. [6] [7]
- Bélanger 2018 CPS guidance for GDD/ID evaluation. [8]
- Syndrome and exposure overlays: Bull (Down syndrome), Hersh (fragile X), Hoyme (FASD), Hyman (autism), White (transition), van Karnebeek (treatable IMD). [11] [12] [13] [14] [17] [10]
Regional practice differences (operational, not biological) change service maps, not the biology of IDD. [16]
- ANZ: medical home plus early childhood intervention and disability support systems (for example NDIS early childhood approach in Australia; local Aotearoa pathways). Genetic testing access varies by jurisdiction and public genetics services. [16]
- UK: NICE-linked learning disability and challenging behaviour pathways, EHCP education processes, regional genetics services. [6]
- US: developmental-behavioral and genetics pathways often framed by AAP statements (Moeschler, Lipkin, White) and IDEA educational entitlements; ES/GS uptake influenced by ACMG guidance and payer rules. [1] [3] [15] [17]
- Canada: CPS evaluation guidance (Bélanger) plus provincial therapy and education systems. [8]
Controversies. How early to offer genome-wide sequencing; how to talk about IQ without reifying a number; waitlist ethics when intervention capacity is scarce; balancing neurodiversity-affirming language with accurate adaptive-support planning. State uncertainty honestly. [3] [5]
Exam Pearls
IDD clinic spine — ADAPT
References
- [1]Moeschler JB Comprehensive evaluation of the child with intellectual disability or global developmental delays. Pediatrics, 2014.PMID 25157020
- [2]Miller DT Consensus statement: chromosomal microarray is a first-tier clinical diagnostic test for individuals with developmental disabilities or congenital anomalies. American journal of human genetics, 2010.PMID 20466091
- [3]Manickam K Exome and genome sequencing for pediatric patients with congenital anomalies or intellectual disability: an evidence-based clinical guideline of the American College of Medical Genetics and Genomics (ACMG). Genetics in medicine, 2021.PMID 34211152
- [4]Maulik PK Prevalence of intellectual disability: a meta-analysis of population-based studies. Research in developmental disabilities, 2011.PMID 21236634
- [5]Tassé MJ The Relation Between Intellectual Functioning and Adaptive Behavior in the Diagnosis of Intellectual Disability. Intellectual and developmental disabilities, 2016.PMID 27893317
- [6]Patel DR A clinical primer on intellectual disability. Translational pediatrics, 2020.PMID 32206581
- [7]Purugganan O Intellectual Disabilities. Pediatrics in review, 2018.PMID 29858292
- [8]Bélanger SA Evaluation of the child with global developmental delay and intellectual disability. Paediatrics & child health, 2018.PMID 30919832
- [9]Michelson DJ Evidence report: Genetic and metabolic testing on children with global developmental delay [RETIRED]: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology, 2011.PMID 21956720
- [10]Hoytema van Konijnenburg EMM Treatable inherited metabolic disorders causing intellectual disability: 2021 review and digital app. Orphanet journal of rare diseases, 2021.PMID 33845862
- [11]Bull MJ Health Supervision for Children and Adolescents With Down Syndrome. Pediatrics, 2022.PMID 35490285
- [12]Hersh JH Health supervision for children with fragile X syndrome. Pediatrics, 2011.PMID 21518720
- [13]Hoyme HE Updated Clinical Guidelines for Diagnosing Fetal Alcohol Spectrum Disorders. Pediatrics, 2016.PMID 27464676
- [14]Hyman SL Identification, Evaluation, and Management of Children With Autism Spectrum Disorder. Pediatrics, 2020.PMID 31843864
- [15]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [16]Council on Children with Disabilities and Medical Home Implementation Project Advisory Committee Patient- and family-centered care coordination: a framework for integrating care for children and youth across multiple systems. Pediatrics, 2014.PMID 24777209
- [17]White PH Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home. Pediatrics, 2018.PMID 30348754
- [18]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [19]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [20]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439