Paeds · growth-development-and-behaviour
Normal cognitive, emotional and behavioural development
Also known as Cognitive development · Emotional development · Behavioural development · Self-regulation · Executive function development · Temperament
Fellowship approach to normal cognitive, emotional and behavioural development from infancy through adolescence: age bands, temperament, executive function, self-regulation, red flags, counselling, screening triggers and multi-board exam performance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
This page owns normal cognitive, emotional and behavioural development. Cross-link motor development, language and social communication, autism recognition, ADHD, global delay, tantrums and formal assessment tools rather than hiding full disorder chapters here. [1] [2]
C.O.P.E. at the bedside
Overview & Definition
Parents rarely say “executive function.” They say the child cannot wait, cannot calm, cannot plan or cannot get along. Cognitive development is how a child thinks, remembers, solves problems and understands others’ minds. Emotional development is how feelings are recognised, expressed and recovered from. Behavioural development is how those skills show up in daily life with caregivers, peers and school. [3] [4]
Temperament is the child’s early biological style of reactivity and regulation. It is not a disease label. A high-reactive infant may cry hard and need more help to settle. That child can still develop well with responsive caregiving. [9]
Self-regulation is the growing capacity to manage attention, emotion and behaviour toward a goal. Young children borrow regulation from adults. That borrowed support is co-regulation. Later, more control becomes internal. School readiness depends heavily on these skills. [4]
Executive functions are core control skills: holding information in mind (working memory), stopping an automatic response (inhibitory control), and shifting strategy (cognitive flexibility). They underpin learning, social behaviour and emotional control across childhood. [3]
Use evidence-informed milestones for surveillance. Lists should reflect skills most children of that age have achieved, not folklore averages that falsely reassure. [1]
Classification
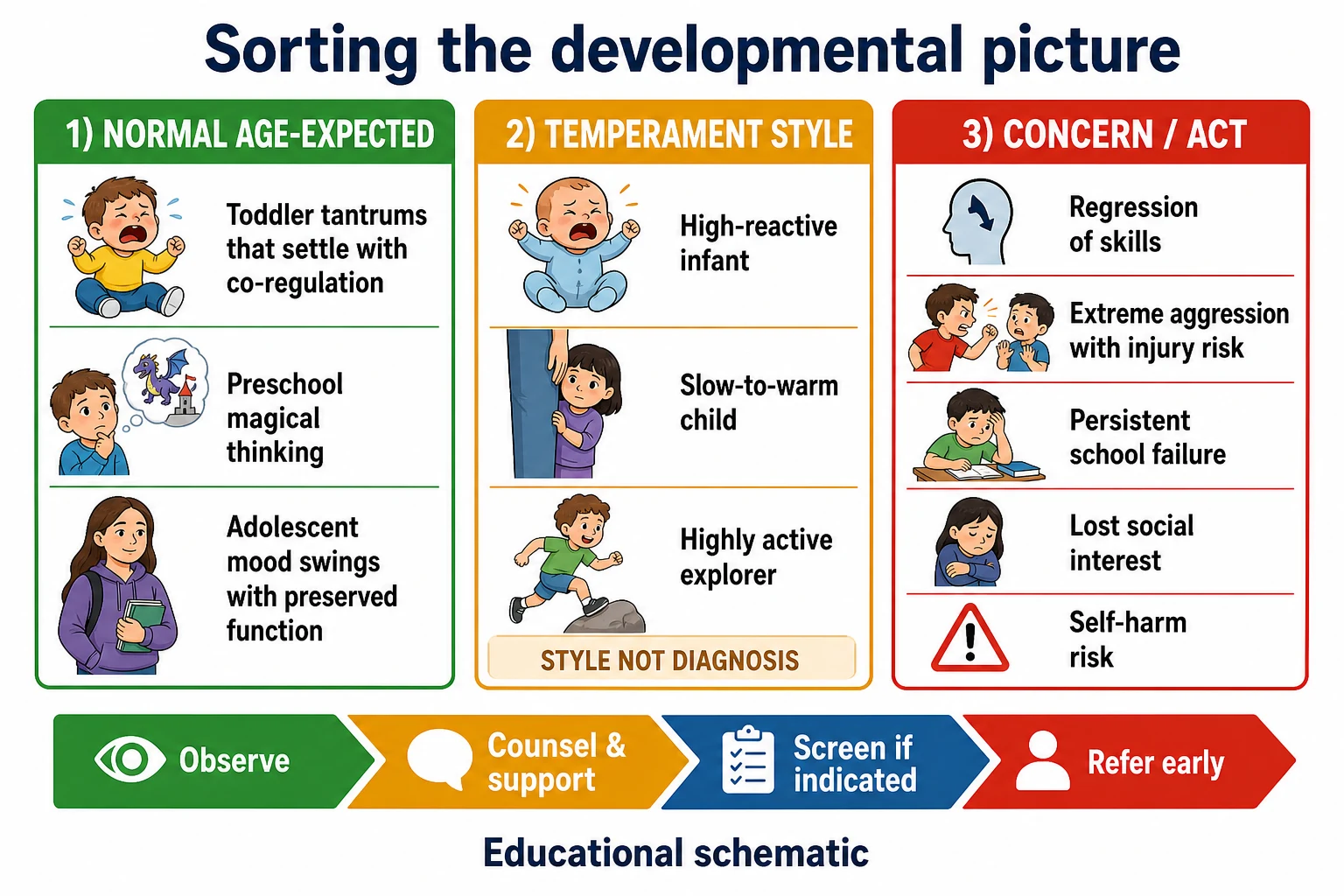
Sort every encounter into one clinical bucket before you counsel. [1] [2]
- Age-expected behaviour — common for the developmental stage and still compatible with safety and learning.
- Temperament variation — enduring style without clear disorder criteria; coaching and environment fit matter.
- Concerning pattern — delay, plateau, regression, severe impairment, safety risk or multi-setting failure that needs action. [1] [2] [9]
Classify by domain as well: cognition/problem-solving, emotion regulation, behaviour control, attention, social use of skills and adaptive function at home and school. One delayed domain is not the same as global delay. [2]
Behavioural-emotional screening tools help risk-stratify when concern persists. A screen does not diagnose ADHD, autism, anxiety or intellectual disability on its own. [7] [8]
Epidemiology & Risk Factors
Most children follow broad developmental pathways with wide normal variation. Late recognition is more common when visits are rushed, services are fragmented, or families face language, transport or trust barriers. [2]
Caregiver concern is a high-value signal. Do not dismiss “something is not right” because the child smiles in clinic. [2] [7]
Adversity and toxic stress shift risk. Prolonged activation of stress systems without a buffering adult can alter attention, emotion regulation and learning. This is biology meeting environment, not parental moral failure. [5] [6]
Media exposure is a modifiable environmental factor. Early childhood is especially sensitive to displacement of play, sleep and caregiver interaction by screens. [10]
Language discordance without professional interpreting degrades both history and counselling about behaviour plans. [11]
Pathophysiology
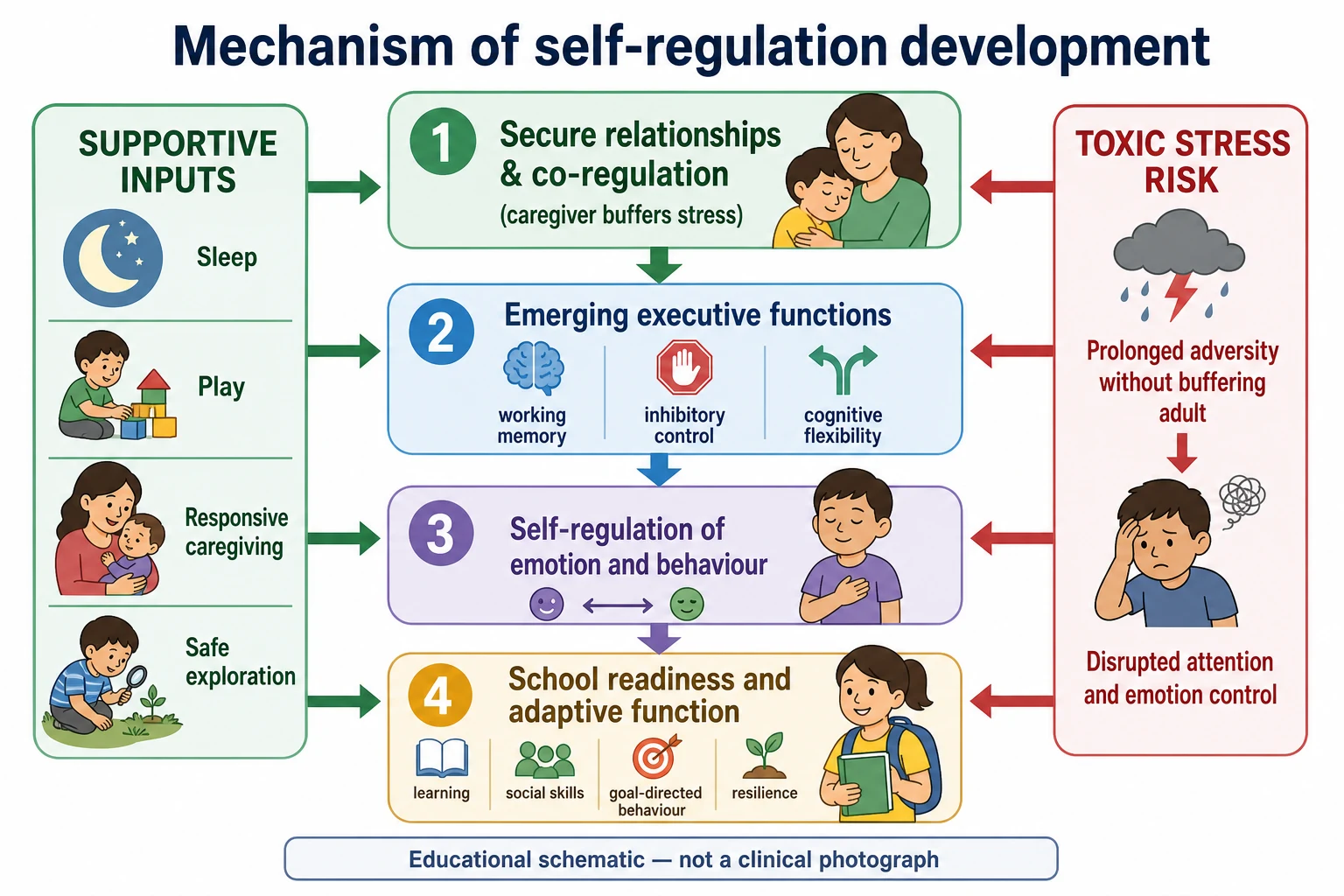
Early brain circuits for attention, emotion and control are experience-dependent. Responsive caregiving, sleep, play and safe exploration build regulation. Chronic threat without protection does the opposite. [4] [5]
Executive functions mature over years. Inhibitory control and working memory improve through preschool and school age, with continued refinement in adolescence. That is why a two-year-old cannot “just stop” a tantrum the way a ten-year-old might. [3]
Temperament reflects early differences in reactivity and regulation. Environment can amplify or buffer those differences. A slow-to-warm child in a harsh setting looks very different from the same child with patient scaffolding. [9]
Toxic stress is not ordinary daily hassle. It is strong, frequent or prolonged activation of the stress response without buffering relationships. The paediatric role includes recognising that pathway and supporting safe relationships, not only listing behaviour tips. [5] [6]
Clinical Presentation
Infant
You look for social engagement, emerging attention to faces and voices, and recovery after distress with caregiver help. Stranger wariness and separation protest can appear as attachment and memory mature. Persistent lack of social responsiveness is not “just a quiet baby.” [1] [9]
Toddler
Toddlers want autonomy with immature inhibition. Tantrums are common when language, frustration tolerance and impulse control lag behind desire. You still expect growing pretend play, simple problem-solving and recovery with co-regulation. Extreme aggression with injury, or total absence of social sharing, needs more than reassurance. [1] [3]
Preschool
Preschoolers expand emotion words, rule-based play and early perspective-taking. They can start waiting short turns and following simple multi-step routines with help. Persistent inability to play with others, extreme rigidity that blocks learning, or no progress in self-control needs structured review. [1] [3] [4]
School-age
School demands working memory, planning, peer negotiation and emotion recovery after setbacks. A child may look “fine” at home and fall apart with classroom load. Ask about homework battles, friendships and teacher comments, not only clinic behaviour. [3] [4]
Adolescent
Abstract reasoning, identity formation and peer belonging accelerate. Emotion intensity can still outrun control. Distinguish normal mood variability with preserved function from anhedonia, withdrawal, self-harm risk or dangerous impulsivity. [6] [7]
Differential Diagnosis
Start with the question: is this still within expected development for age and context? [1] [2]
- Normal variation / temperament — style present early, consistent, and not destroying function after reasonable supports. [9]
- Isolated skill lag — for example attention or emotional control lagging while other domains look solid. [3]
- Global developmental delay — multiple domains behind age expectations; needs full evaluation pathway. [2]
- Language or hearing barrier — can mimic cognitive or behavioural problems; never skip sensory checks when communication is off. [2]
- Trauma or adversity-related behaviour — hypervigilance, aggression, withdrawal or regression in context of threat; use trauma-informed framing without delaying needed evaluation. [5] [6]
- Emerging neurodevelopmental or mental health disorder — ADHD, autism, anxiety, mood disorder or intellectual disability pathways belong to dedicated leaves once concern is established. Screening is a bridge, not the diagnosis. [7] [8]
Clinical & Bedside Assessment
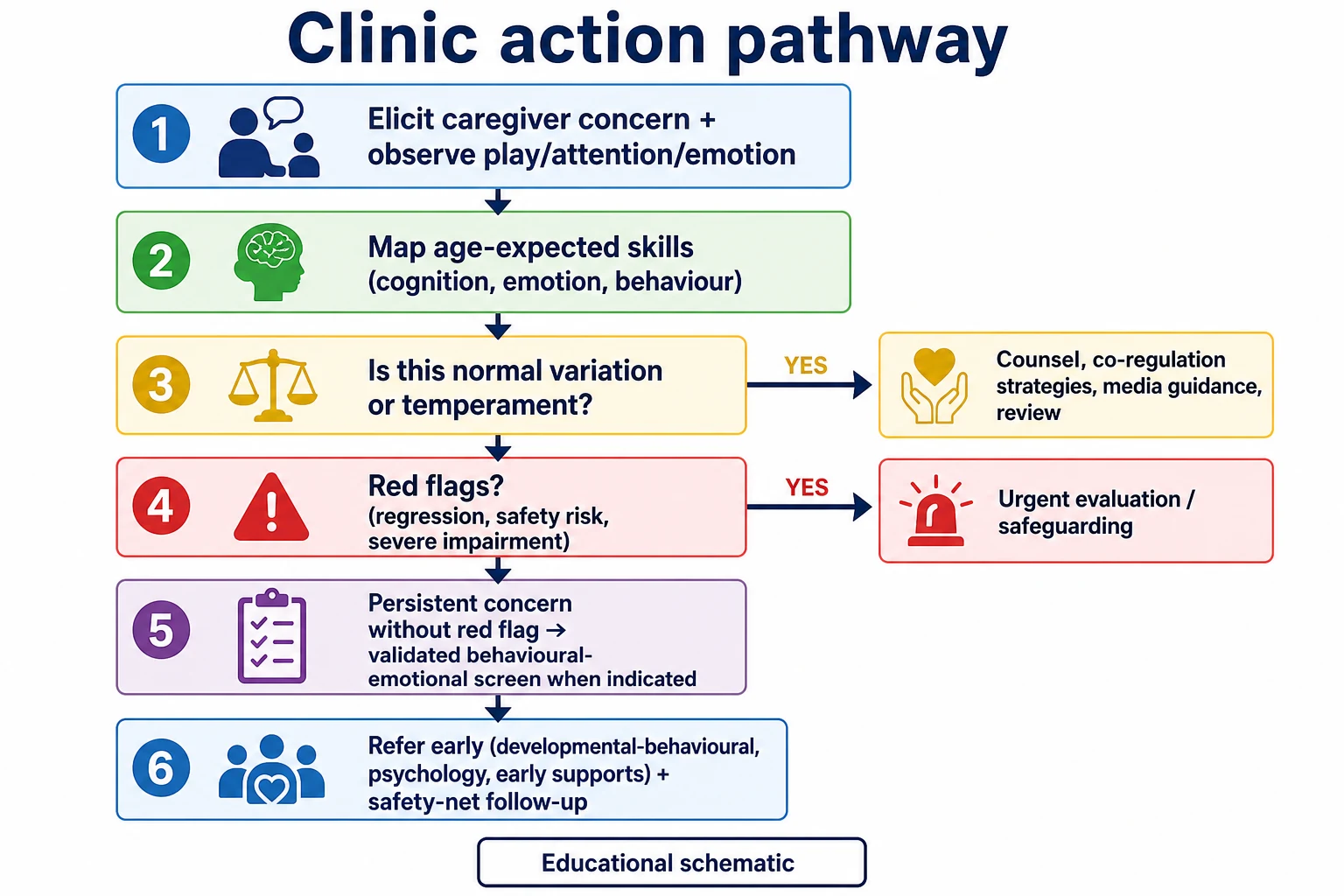
Open with concern: “Do you have any worries about how your child learns, plays, manages feelings or behaves with others?” Then watch the child. Note attention span for age, problem-solving with toys, emotion peaks and recovery, and how the caregiver soothes or sets limits. [1] [2]
Map domains out loud across cognition, emotion, behaviour and executive control. [3] [4]
- Cognition — curiosity, problem-solving, memory for routines, pretend or abstract thinking by age.
- Emotion — range of feelings, labelling, recovery time, need for co-regulation.
- Behaviour — impulse control, aggression, rule following, adaptability.
- Attention / executive control — holding instructions, waiting, shifting activity. [3] [4]
Use evidence-informed milestone content rather than personal folklore. Document what you saw, what caregivers report, and the setting. [1]
When behavioural or emotional concern is more than transient, use validated mental health, emotional and behavioural screening approaches recommended for primary care and explain limits of a positive screen. [7] [8]
In language-discordant families, use professional interpreters for history and counselling. Do not use the child as interpreter for behavioural concerns. [11]
Investigations
Most questions about normal development are answered by history, observation and context — not blood tests. [2]
- Hearing and vision when communication, learning or behaviour raises concern. [2]
- Targeted medical testing belongs with evaluation teams when red flags suggest neurological disease, regression or syndromic features. [2]
- Psychoeducational or developmental standardised testing is referral territory for assessment services, not a first reflex for every intense toddler. [2] [7]
- Safeguarding assessment if neglect, violence or severe deprivation is suspected. [5] [6]
Avoid shotgun labs for temperament alone. Investigations should change management, not decorate the chart. [2]
Management — Resuscitation
True developmental counselling is usually outpatient. Switch tracks immediately when safety is threatened. [2] [6]
- Acute behavioural crisis with injury risk: protect the child and others, assess for medical delirium or intoxication if indicated, and use local acute mental health or emergency pathways. [6] [7]
- Developmental regression: treat as urgent evaluation, not “review in six months.” [2]
- Suspected severe maltreatment or unsafe caregiving: open safeguarding routes now. [5] [6]
- Adolescent self-harm or suicidal ideation: safety assessment first; developmental teaching second. [7]
Management — Definitive & Stepwise
- Name the age-expected pattern in plain language the caregiver can repeat.
- Separate temperament from danger. High intensity needs coaching; regression needs work-up. [9]
- Strengthen co-regulation: calm presence, predictable routines, sleep, feed, and one-step limits for young children. [4]
- Protect developmental time: play, conversation and sleep over excessive early media. Follow paediatric media guidance rather than inventing personal cut-offs. [10]
- Screen for behavioural and emotional problems when concern persists or function is impaired. [7] [8]
- Refer early to developmental-behavioural, psychology, school supports or early intervention pathways as indicated. Do not wait for a perfect label before offering help. [2] [7]
- Safety-net: what to watch for, when to return, and how to chase referrals while waiting. [12]
Specific Subtypes & Scenarios
High-reactive infant. Expect bigger cry peaks and longer settling. Coach responsive soothing, protect parental sleep supports, and avoid early disease labels for temperament alone. Review if social engagement is missing. [9]
Toddler tantrums. Common when desire outruns language and inhibition. Counsel prevention (hunger, fatigue, transitions), brief safe limits and recovery connection. Escalate if aggression is extreme, daily and injurious, or paired with language loss. [1] [3]
Preschool school-readiness worry. Focus on self-regulation, play skills and following simple group routines, not only letter knowledge. Self-regulation predicts school readiness more than isolated academic drills. [4]
School-age homework wars. Ask about working memory load, sleep, anxiety and classroom fit. A child who can play football but cannot organise a bag may still need executive-function supports rather than blame. [3]
Adolescent intensity. Validate strong feelings while assessing function, safety, sleep, substances and supports. Normal development does not include sustained hopelessness or self-harm plans. [6] [7]
Adversity-exposed child. Behaviour may be adaptation to threat. Use trauma-informed care: safety, trust, collaboration and no shaming, while still completing developmental assessment. [5] [6]
Complications & Pitfalls
- Labelling temperament as ADHD or “bad parenting” without a proper assessment. [9]
- Reassuring on outdated milestone folklore. [1]
- Waiting years after clear caregiver concern. [2]
- Treating a behavioural screen as a final diagnosis. [7] [8]
- Ignoring sleep, hearing, vision, trauma or language access. [2] [6] [11]
- Using screens as a behaviour strategy that displaces co-regulation. [10]
- Missing regression because the child “was always a bit delayed.” [2]
Prognosis & Disposition
Self-regulation and executive skills strongly influence school readiness and later adaptive success. Supportive caregiving and early help improve trajectories for many children. [3] [4]
Disposition options follow function and risk. [2] [4]
- Routine surveillance when skills track age expectations. [1] [2]
- Active coaching and timed review for temperament strain or mild situational behaviour issues. [4] [9]
- Screen and refer when impairment persists or multi-setting concern accumulates. [2] [7]
- Urgent pathway for regression, safety risk or safeguarding concerns. [5] [6]
Always leave a chase plan for referrals. Waitlists are not a clinical plan by themselves. [12]
Special Populations
Ex-preterm and medically complex children. Use corrected age early when local developmental protocols advise, and still watch emerging self-regulation and attention under medical load. [2]
Out-of-home care and trauma-exposed families. Expect attachment and regulation challenges; pair developmental support with trauma-informed practice and stable caregiving advocacy. [5] [6]
Indigenous, migrant and refugee families. Interpret behaviour in cultural and language context. Use interpreters and culturally safe services. Avoid pathologising difference. [11]
Neurodiverse children. Baseline may differ; measure change from the child’s own trajectory and function, not only from a neurotypical checklist. [2]
Socioeconomic disadvantage. Poverty-related stress can tax self-regulation. Address material supports alongside behaviour advice. [4] [5]
Evidence, Guidelines & Regional Differences
Evidence-informed milestone content supports surveillance tools so clinicians are not falsely reassured by outdated “average age” lists. [1] AAP guidance on identifying developmental disorders frames continuous surveillance plus screening and early action. [2] Executive function and school-readiness science explain why co-regulation and attention control are clinical, not optional soft skills. [3] [4]
Toxic stress and trauma-informed care reports translate adversity biology into paediatric action. [5] [6] AAP behavioural-emotional screening reports guide when and how to look for mental health and behaviour problems beyond classic milestone lists. [7] [8] Temperament research clarifies early individual differences without forcing disease labels. [9] Media guidance highlights early childhood vulnerability to screen displacement of interaction. [10]
Use local child health books, jurisdictional developmental surveillance schedules and early childhood support pathways. Cultural safety, interpreter access and family-led goals are part of valid assessment. Map to local paediatric, psychology and education supports rather than importing US tool ages as law. [2] [11]
Healthy child programme contacts and NICE-aligned education wellbeing guidance shape population approaches. Community paediatric and CAMHS pathways vary by area — state the local route when you counsel. [2] [7]
Bright Futures and AAP schedules drive surveillance and behavioural-emotional screening expectations. Canadian provincial programmes differ; name the local tool and service pathway instead of inventing universal cut-offs. [2] [7] [8]
Exam Pearls
- Temperament is style; diagnosis needs impairment, pattern and proper assessment. [9]
- Executive functions = working memory + inhibitory control + cognitive flexibility. [3]
- Young children co-regulate before they self-regulate. [4]
- Use evidence-informed milestones, not memory folklore. [1]
- Caregiver concern is data. [2]
- Screens risk-stratify; they do not replace clinical judgement or diagnosis. [7] [8]
- Regression and safety risk leave the “normal development” pathway immediately. [2] [6]
- Protect play, sleep and relationships from excessive early media. [10]
- Interpreter access is part of valid behavioural history. [11]
- Safety-net the wait for services. [12]
Keep four bedside anchors ready for viva: executive-function triad (working memory, inhibit, flexibility); toddler desire outrunning brakes; self-regulation as school-readiness core; and toxic stress as prolonged threat without an adult buffer. [3] [4] [5]
References
- [1]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439
- [2]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [3]Diamond A Executive functions. Annual review of psychology, 2013.PMID 23020641
- [4]Blair C School readiness and self-regulation: a developmental psychobiological approach. Annual review of psychology, 2015.PMID 25148852
- [5]Garner AS Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics, 2012.PMID 22201148
- [6]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [7]Weitzman C Promoting Optimal Development: Screening for Mental Health, Emotional, and Behavioral Problems: Clinical Report. Pediatrics, 2025.PMID 40850690
- [8]Weitzman C Promoting optimal development: screening for behavioral and emotional problems. Pediatrics, 2015.PMID 25624375
- [9]Gartstein MA Temperament development in infancy: What we have learned about the origins of individual differences in the past 25 years. Infant behavior & development, 2025.PMID 40554909
- [10]COUNCIL ON COMMUNICATIONS AND MEDIA Media and Young Minds. Pediatrics, 2016.PMID 27940793
- [11]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [12]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428