Paeds · growth-development-and-behaviour
Normal language, communication and social development
Also known as Language milestones · Speech and language development · Social communication development · Joint attention milestones · Prelinguistic communication
Fellowship guide to normal language, communication and social development from infancy through school age: age-banded milestones, bedside observation, red flags, bilingual assessment, anticipatory guidance and early escalation without cloning speech-delay or autism chapters.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
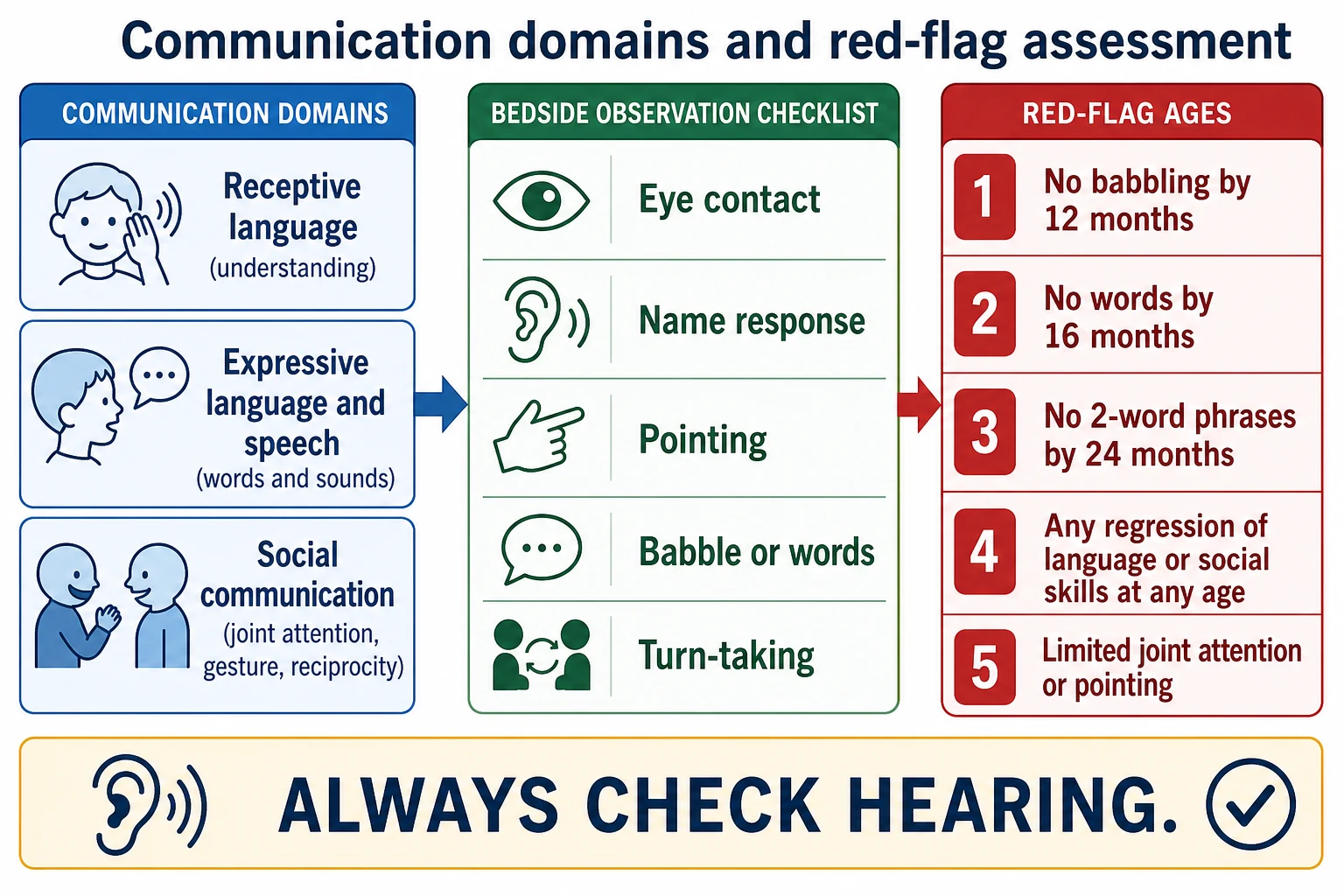
These domains travel together in clinic. A toddler with many words but no pointing needs a different pathway from a late talker who understands well and points to request. [1] [4]
T.A.L.K. at the bedside
Overview & Definition
Normal language development is the expected acquisition of understanding, words, grammar and speech sounds. Communication is broader. It includes prelinguistic skills such as eye gaze, cry patterns, babble and gesture. Social communication is how the child uses these skills with other people: sharing attention, requesting, commenting and later conversing. [4] [5]
Evidence-informed milestone lists now emphasise skills achieved by most children at a given age, not historical “average ages” that false-reassured families. That change matters for surveillance tools and for what you say in clinic. [1]
This page owns normal trajectories, bedside observation and anticipatory guidance. Cross-link surveillance technique, validated screening tools, speech-language delay work-up and autism recognition rather than hiding full specialty chapters here. [2]
Classification
Classify every concern by domain and by pattern. Domains: receptive language, expressive language, speech sound production, pragmatics and social communication. Patterns: age-expected, isolated lag, multi-domain delay, social-communication pattern concerning for autism, plateau, or true regression. [1] [2] [4]
Speech is how sounds are formed. Language is meaning, vocabulary and grammar. A child can have clear speech with empty social use, or rich language with unclear articulation. Do not collapse these into one vague “speech delay” label. [4] [5]
Epidemiology & Risk Factors
Late recognition is more common when visits are rushed, tools are not used, families face transport or language barriers, or clinicians wait for “school readiness.” Children with medical complexity may have diagnostic overshadowing. Caregiver concern remains a high-value signal. [2] [14]
Risk factors that raise later language or social-communication problems include permanent hearing loss, recurrent middle-ear disease with hearing impact, preterm birth, family history of language disorder, limited contingent language exposure and early adversity. Toxic stress can alter attention, regulation and engagement without replacing a careful developmental assessment. [6] [7] [10]
Language-discordant families need professional interpreters for history and counselling. Child interpreters are not acceptable for this work. [8]
Pathophysiology
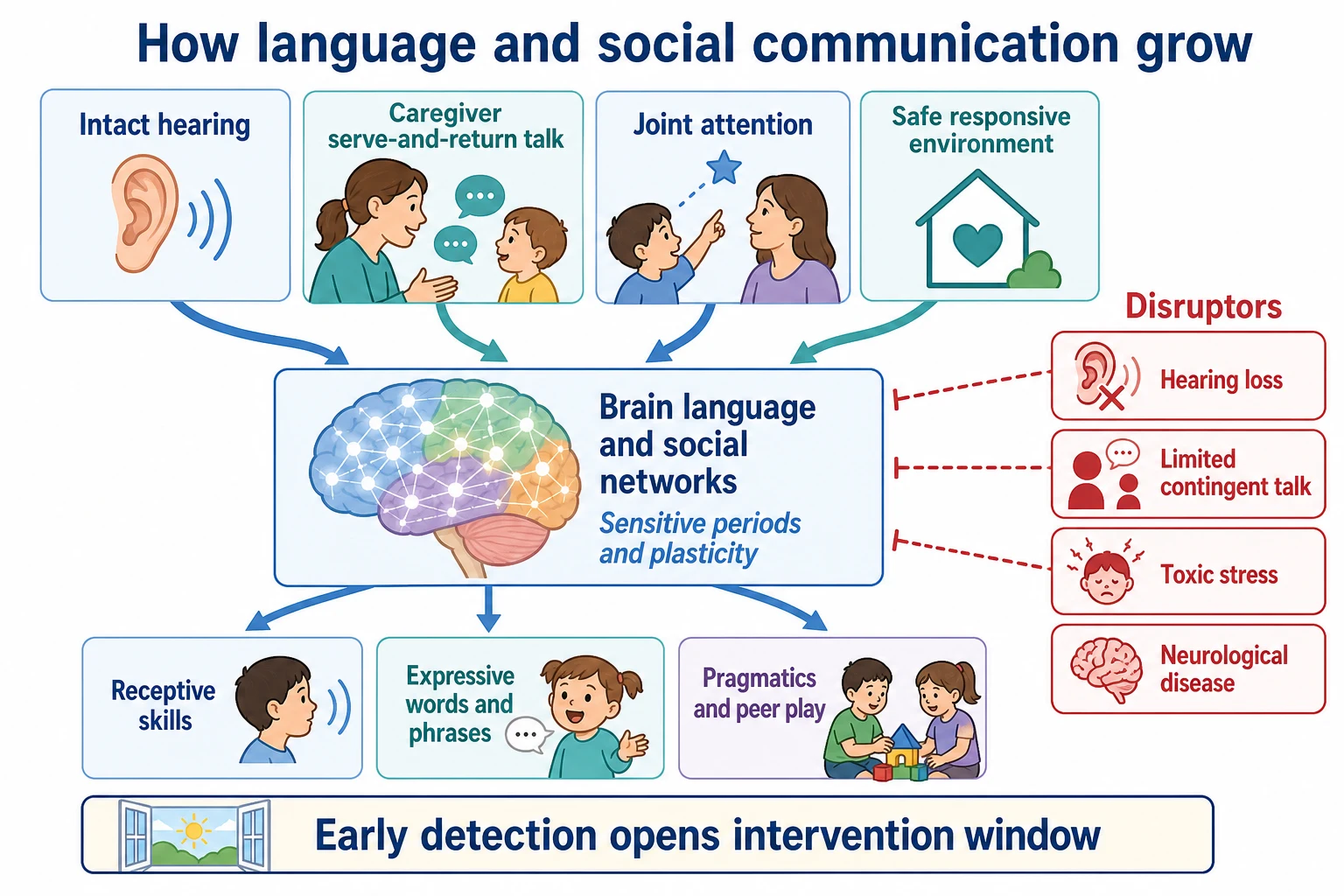
Language networks depend on audible input, social engagement and practice. Hearing delivers the signal. Caregivers provide serve-and-return talk that maps words onto shared attention. Joint attention links gaze, gesture and object so meaning can stick. Safe relationships support exploration and practice. [4] [6] [7]
Early childhood is a high-plasticity window. When hearing loss, severe social deprivation, untreated seizures or neurological disease interrupt input, the visible milestone pattern changes. Early detection opens intervention time. Delayed recognition narrows that window. [2] [6]
Clinical Presentation
0–6 months. Social smile, eye contact, cooing and differentiated cry. The infant calms to a familiar voice and begins reciprocal vocal play. [1] [4]
6–12 months. Canonical babble, response to name, gesture beginnings, and early joint attention. By the end of this window many infants use simple gestures such as reach-to-request and enjoy back-and-forth games. [1] [4]
12–18 months. First meaningful words appear for most children. Pointing to request or show interest is a major social-communication milestone. Comprehension of simple familiar phrases usually outruns expression. [1] [4]
18–24 months. Vocabulary expansion and emerging word combinations. Pretend play and showing objects to share interest grow. Persistent absence of words or gesture in this window is not a casual finding. [1] [4]
2–3 years. Short phrases, expanding vocabulary, and clearer speech to familiar listeners. Peer interest and simple turn-taking appear in play. [1] [5]
Preschool to school age. Connected sentences, storytelling, conversation repair, friendship skills and classroom listening demands. Pragmatic difficulty may surface as peer conflict even when vocabulary looks adequate. [4] [5]
Caregivers may say the child is “in their own world,” “not talking like cousins,” or “was saying words and stopped.” Write those phrases down. They are clinical data. [2]
Differential Diagnosis
Separate isolated speech-sound delay, language delay, social-communication pattern concerning for autism, hearing impairment, global developmental delay, bilingual sequential acquisition, selective mutism and environmental deprivation or neglect. Temperament can make a child quiet in clinic; it does not erase red-flag ages or absent joint attention. [2] [4] [5]
Hearing loss can mimic primary language delay. Autism-specific tools target social-communication risk and are not general language diagnoses. Full differential work-up for established delay or autism lives on linked pages; this page keeps the normal baseline clear so you notice when the pattern is off. [3] [6]
Clinical & Bedside Assessment
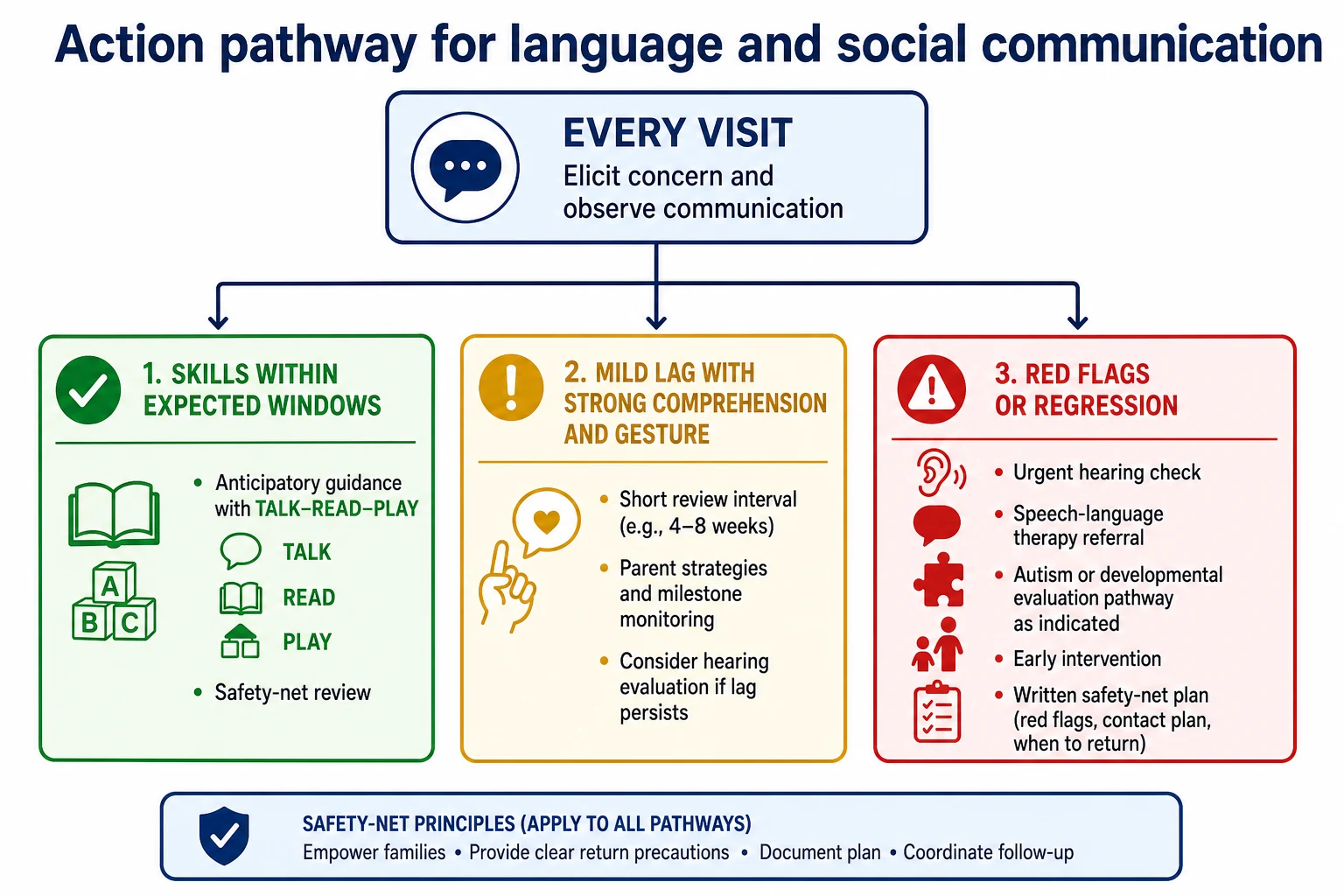
Start with an open question: “Do you have any concerns about how your child is talking, understanding, playing or connecting with others?” Then watch the child. Note eye contact, response to name, pointing, babble or words, turn-taking and how the child uses the caregiver for comfort and sharing. [1] [2]
Use an evidence-informed milestone list for the child’s age. Document receptive, expressive and social domains separately, with the source of each skill report. Do not invent personal cut-offs. If surveillance raises concern, or the child reaches a recommended screening age, use the validated general developmental screen your service supports. For toddler social-communication risk, autism-specific tools such as M-CHAT-R/F with follow-up interview risk-stratify; they do not alone diagnose. [1] [2] [3] [12]
In bilingual homes, assess total language exposure across languages. Counting only English words underestimates ability and can pathologise normal dual-language learning. Use professional interpreters for caregiver history and result counselling. [8]
Investigations
Arrange hearing assessment whenever language or communication is a concern. Newborn hearing screening is not a lifetime guarantee. Vision check matters when social engagement or dual sensory risk is present. Standardised speech-language assessment is indicated for persistent lag or red flags. Avoid shotgun laboratory or genetic testing from a single late first word without broader context; that work belongs with evaluation teams when multi-domain delay or other medical clues appear. [2] [4] [6]
Management — Resuscitation
Routine language surveillance is outpatient. Exceptions need acute pathways first: developmental regression with encephalopathy, new seizures, severe dehydration or collapse, or safeguarding emergencies when severe neglect is suspected. [2] [10]
Management — Definitive & Stepwise
- Complete communication and social surveillance every visit.
- Reassure only when skills sit within expected windows and no red flags are present.
- Give anticipatory guidance: talk during care routines, read daily, follow the child’s focus, pause for serve-and-return, and limit passive screen time in infancy and early toddler years.
- Check hearing and refer to speech-language therapy early on red flags or persistent lag.
- Open parallel autism or developmental evaluation pathways when social-communication concern is high.
- Explain findings with teach-back, share a written plan, and safety-net the wait for services. [1] [2] [4] [11] [13]
Consent principles still apply when you share information with early childhood services or schools. [9]
Specific Subtypes & Scenarios
Late talker with strong gesture and comprehension. Document domains, exclude hearing risk, give language-rich strategies, and set a short review rather than an open-ended wait. Escalate if social skills weaken or milestones still lag. [4] [5]
Limited joint attention and no pointing. Do not label this as simple late talking. Use social-communication screening pathways and refer early. [3]
Bilingual sequential learner. Assess both languages. Temporary English lag with rich home-language skills is not automatically a disorder. Still act on red-flag ages and caregiver concern. [8]
Ex-preterm infant. Use corrected age for early milestones as local developmental follow-up advises, and do not skip surveillance because the neonatal course “explains everything.” [2]
Deaf or hard-of-hearing infant. Early amplification or cochlear implant pathways and language access (spoken language, signed language or both as the family chooses with specialist support) change trajectory; early intervention is not optional. [6]
School-age pragmatic difficulty. Vocabulary may look fine while peer conversation fails. Reassess hearing, language, social communication, learning and mental health rather than blaming behaviour alone. [4] [5]
Complications & Pitfalls
“Wait and see” after clear red-flag ages. Ignoring hearing. Counting only words and missing gesture. Pathologising bilingualism. Using the child as interpreter. Treating a screen as a diagnosis. Losing families on long therapy waitlists without interim strategies. Attributing every lag to medical complexity without looking for treatable communication needs. [2] [3] [8] [14]
Prognosis & Disposition
Many children with isolated late talking and strong social and receptive skills catch up. Red flags and multi-domain patterns need action, not hope. Earlier access to hearing care, speech-language therapy and early intervention improves functional communication for many children. Disposition is a written plan, community supports and a chase plan for appointments — not “refer and forget.” [2] [6] [13]
Special Populations
NICU graduates, children with known syndromes, neurodiverse families seeking affirming care, Indigenous families needing culturally safe services, migrant and refugee families with interrupted care, children in out-of-home care, and children with medical complexity all need active communication surveillance rather than passive assumptions. Trauma-informed practice avoids blame while still completing a careful assessment. [7] [8] [10] [14]
Evidence, Guidelines & Regional Differences
Zubler and colleagues provide evidence-informed milestone content for surveillance tools. [1] Lipkin and colleagues set the AAP surveillance-plus-screening framework for early identification of developmental disorders. [2] Robins and colleagues validated M-CHAT-R/F for toddler autism risk screening with follow-up. [3] Preventive care periodicity schedules place developmental surveillance and screening inside the medical home. [11] Clinical reviews summarise speech-language monitoring and preschool evaluation principles used at the bedside. [4] [5]
Use local child health books, jurisdictional speech-language pathology pathways and early childhood early intervention services. Cultural safety and interpreter access are part of valid assessment. [8]
Healthy Child Programme schedules and local speech and language therapy pathways shape review timing. NICE autism recognition guidance applies when social-communication concern dominates. [2]
Bright Futures and AAP periodicity schedules drive surveillance and screening ages. Early intervention programmes vary by state or province — name the local pathway rather than inventing universal cut-offs. [1] [11]
Exam Pearls
- Joint attention and pointing matter as much as word count. [1]
- Receptive skills usually lead expression. [4]
- Use evidence-informed milestones, not folklore averages. [1]
- No babble by 12 months, no words by 16 months, no two-word phrases by 24 months, or any regression needs action. [1] [2]
- Always think hearing in language concern. [6]
- Bilingual assessment uses total language exposure. [8]
- A screen is not a diagnosis. [3]
- Safety-net the referral wait. [13]
References
- [1]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439
- [2]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [3]Robins DL Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics, 2014.PMID 24366990
- [4]McQuiston S Speech and language development: monitoring process and problems. Pediatrics in review, 2011.PMID 21632874
- [5]Feldman HM Evaluation and management of language and speech disorders in preschool children. Pediatrics in review, 2005.PMID 15805236
- [6]Moeller MP Early intervention and language development in children who are deaf and hard of hearing. Pediatrics, 2000.PMID 10969127
- [7]Garner AS Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics, 2012.PMID 22201148
- [8]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [9]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [10]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [11]Committee on Practice and Ambulatory Medicine 2023 Recommendations for Preventive Pediatric Health Care. Pediatrics, 2023.PMID 36938620
- [12]Schonhaut L Validity of the ages and stages questionnaires in term and preterm infants. Pediatrics, 2013.PMID 23629619
- [13]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428
- [14]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731