Paeds · growth-development-and-behaviour
Normal motor development and developmental variation
Also known as Gross motor milestones · Fine motor development · WHO motor windows · Bottom shuffling · Normal variation in walking
Fellowship guide to normal gross and fine motor development, WHO windows of achievement, healthy variation including non-crawling paths, bedside motor examination, and the first decision between reassure, recheck or escalate.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A parent says, “She is not crawling like her cousins.” Another says, “He walked at ten months — is early walking always good?” Your job is to separate normal motor development, healthy variation, and motor findings that need action. [1] [3]
Gross motor skills move the body through space: head control, rolling, sitting, locomotion, standing and walking. Fine motor skills use the hands for reach, grasp, transfer, pincer and tool use. Both rest on posture, tone and practice. Oral-motor feeding skill is adjacent but is not the whole motor story. [2]
A milestone is an observable skill. A trajectory is how skills build over months. Quality of movement is how the skill looks — stiff or floppy, symmetric or one-sided, variable or stereotyped. Examiners fail candidates who quote a single “should walk by twelve months” line and ignore quality. [1] [2]
This page owns normal sequences, WHO windows, common variation and the first clinic decision. Cross-link hypotonia work-up, cerebral palsy early recognition, developmental coordination disorder, specialised infant neuromotor tools, and surveillance or screening programmes rather than cloning those chapters. [3] [5] [6]
Classification
Classify four things before you reassure anyone. [1] [3]
Domains
| Domain | Examples | Clinic question |
|---|---|---|
| Gross motor | Sit, crawl or shuffle, stand, walk, run, climb | How does the body move in space? |
| Fine motor | Reach, transfer, pincer, stack, crayon | How do the hands explore and use tools? |
| Posture and balance | Head righting, trunk control, protective responses | Can the child hold and recover position? |
| Quality | Symmetry, fluidity, antigravity power | Does movement look efficient and variable? |
Result bands at the first look
- Normal — skills fit age, quality is good, tone and symmetry are reassuring.
- Healthy variation — alternative path (for example bottom-shuffling or no hands-and-knees crawl) still inside windows with a normal exam.
- Monitor — borderline age or limited observation; quality still acceptable; timed recheck planned.
- Escalate — red-flag age, abnormal tone, asymmetry, regression, or multi-domain concern. [1] [3] [5]
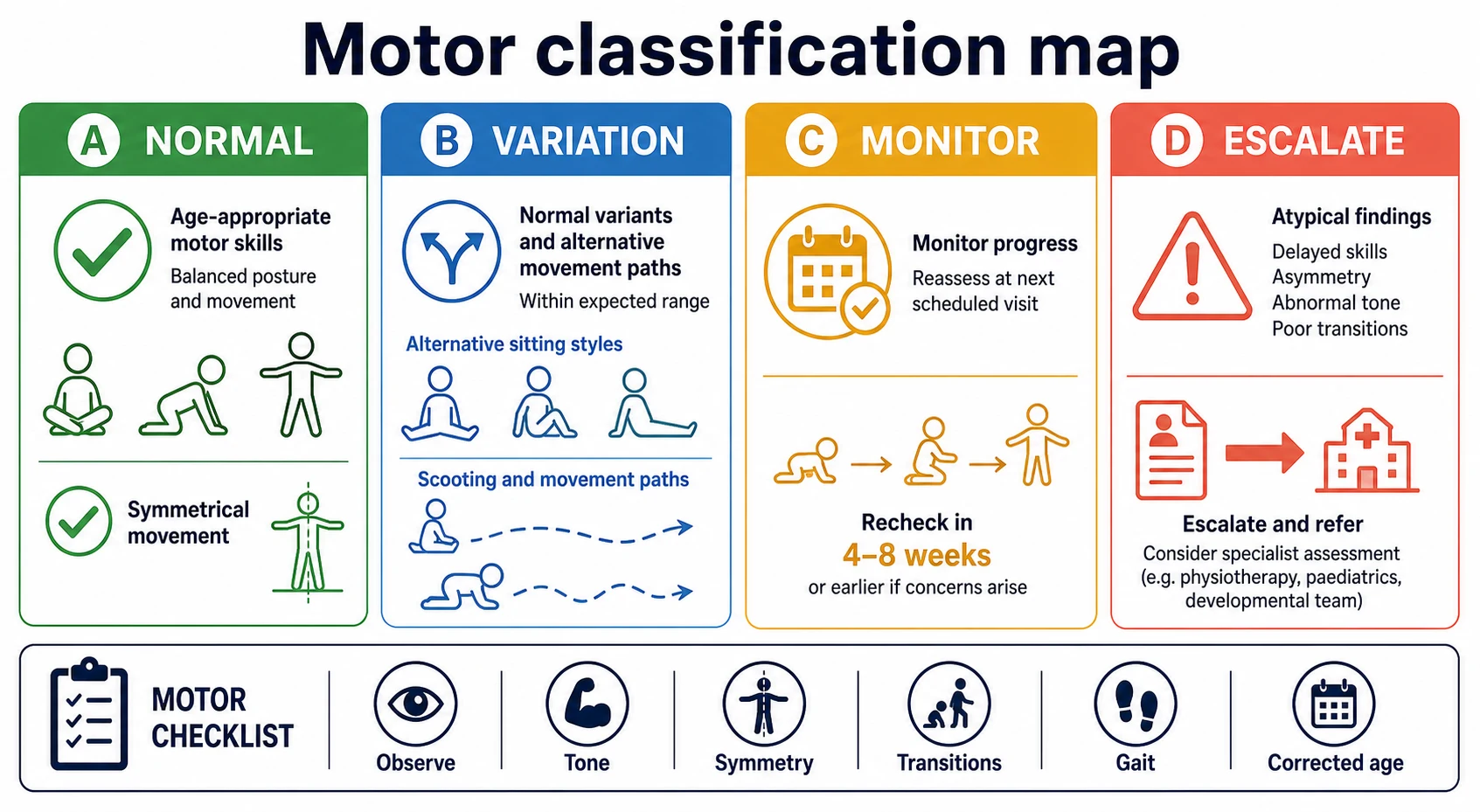
Read the figure like this: a late crawler with free floor movement and good sitting can still be variation. A “walker” who drags a stiff leg is not. [1] [5]
Variation patterns worth naming
- Bottom-shuffling — locomotion on the buttocks; may walk later within the window but can still be normal if tone and play are good.
- No hands-and-knees crawl — seen in about 4.3% of the WHO motor cohort; not automatically pathologic.
- Early rolling or early walking — not a prize if tone is high and movement is stiff.
- Toe-walking — brief intermittent toe gait can be common in new walkers; persistent toe-walking needs a fuller neurological and developmental look. [1] [5]
Epidemiology & Risk Factors
Healthy motor ages are wide. In the WHO Motor Development Study, the estimated 1st and 99th percentiles in months were: sitting without support 3.8–9.2; standing with assistance 4.8–11.4; hands-and-knees crawling 5.2–13.5; walking with assistance 5.9–13.7; standing alone 6.9–16.9; walking alone 8.2–17.6. About 90% of children achieved five milestones in a common sequence. Windows overlap. Widths differ; sitting is relatively narrow; standing alone and walking alone are wide. [1]
Population comparisons in the same WHO programme showed limited sex differences and described heterogeneity across sites while still supporting common windows for healthy children. Use windows for clinical thinking, not to shame cultural care practices. [4]
True motor pathology risk rises with extreme prematurity, neonatal encephalopathy, brain injury, neuromuscular disease, untreated severe illness, and some genetic syndromes. Opportunity also matters: little awake tummy time, long periods in restrictive devices, and limited floor play can slow ages without fixed neurology. Poverty, language barriers and fragmented care delay detection more than they invent biology. [3] [5] [8]
Children with medical complexity are at risk of diagnostic overshadowing — every new lag is blamed on the known label. Children in foster or kinship care often arrive with incomplete motor histories and need catch-up surveillance. [7] [13]
Pathophysiology
Motor control matures roughly cephalocaudal (head before trunk before legs) and proximodistal (shoulder before hand). Myelination, synaptic pruning and thousands of practice repetitions turn unstable postures into skilled action. Truncal stability frees the hands. Free hands feed exploration, which feeds more motor maps. [2]
Newborns show primary movement patterns often called primitive reflexes. As postural reactions and voluntary control mature, those patterns integrate into purposeful movement. Persistent obligatory patterns, obligatory asymmetry, or a stiff “all or none” motor style raise concern for upper-motor pathways — detail belongs with cerebral palsy early recognition. Flaccid power, reduced bulk and reduced reflexes point toward lower-motor or neuromuscular pathways — detail belongs with the floppy-infant leaf. [5]
Alternative locomotion can still lead to independent walking inside WHO windows. The mechanism is not magic. Children find another way to move while balance and antigravity strength catch up. That is why “never crawled” is not a diagnosis. [1]
Reduced opportunity changes the practice half of the equation. Trauma and severe adversity can also change exploration and regulation without turning every motor lag into a primary brain malformation story. Use trauma-informed habits while still examining neurology carefully. [9]
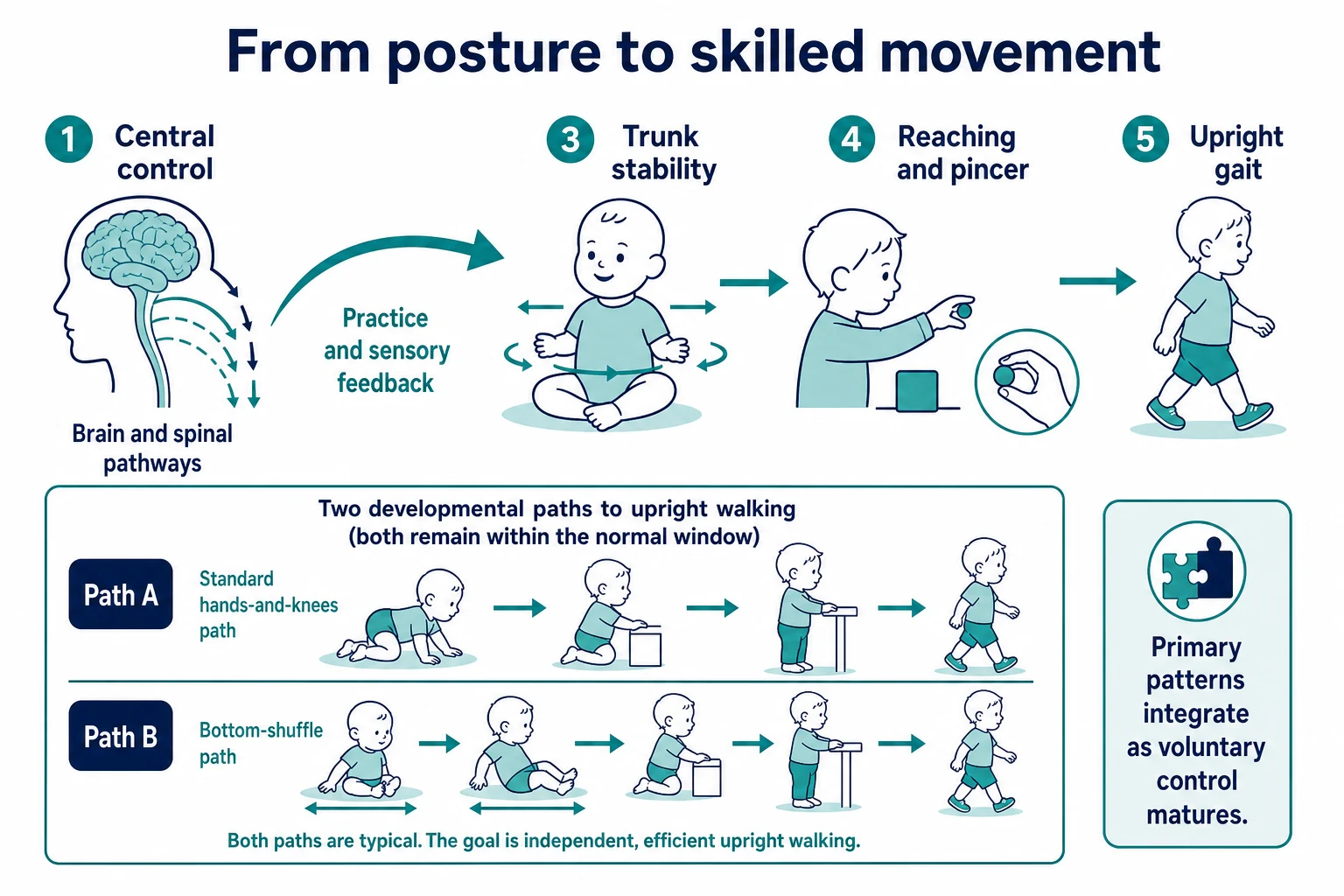
Read the figure like this: if practice is missing, ages slide. If central control is injured, quality breaks even when opportunity is perfect. Your exam tries to tell those stories apart. [1] [5]
Clinical Presentation
What families say
- “No crawling — only bum shuffling.”
- “Not sitting on the floor yet.”
- “Still not walking at fifteen months.”
- “Always uses the right hand and keeps the left closed.”
- “Walks on tiptoes all the time.”
- “He could pull to stand and then stopped trying.” [1] [3]
Age-banded clinic pictures
Newborn and early infant. Flexed posture, reciprocal limb movements, and emerging head control on pull-to-sit. Marked floppiness, frog-leg posture with weak antigravity effort, or extreme stiffness needs more than “newborn normal.” [2] [5]
Four to six months. Improving head control, hands to midline, beginning of rolling in many infants. Persistent head lag with poor trunk power is a clinical signal, not a chart decoration. [2]
Sitting window. Independent sitting without support appears across roughly 3.8–9.2 months in WHO data. A child near the upper edge needs a careful exam, not automatic panic and not automatic reassurance. [1]
Locomotion variants. Hands-and-knees crawling window is wide (5.2–13.5 months). Bottom-shuffling or no crawl can still be healthy. Watch for absence of any efficient locomotion plus poor sitting. [1]
Walking window. Walking alone spans roughly 8.2–17.6 months. A graceful 15-month non-walker with normal tone differs from a stiff 13-month “walker” with scissoring. [1] [5]
Preschool fine motor. Pincer, stacking, scribbling and later pencil grasp concerns often present as “messy eating” or “will not draw.” Link to opportunity and vision, and open a DCD-style pathway if coordination problems persist into school age with functional impact. [2] [6]
Regression
Loss of motor skills after clear acquisition is never healthy variation. Treat it as urgent structured evaluation. [3] [5]
Differential Diagnosis
| Pattern | Prefer first | Also consider | Do not assume |
|---|---|---|---|
| Late walker, normal exam, in WHO window | Healthy late-normal trajectory | Mild opportunity limit | “Lazy” child |
| Bottom-shuffle, good tone | Variation | Hypotonia if trunk is floppy | Automatic disorder label |
| Early hand preference + fisting | Evolving hemiplegic CP pathway | Painful limb, injury | Cute handedness |
| Multi-domain lag | Global developmental evaluation | Severe psychosocial deprivation | Isolated physio only |
| Progressive weakness | Neuromuscular pathway | Acute illness | Static late bloomer |
| School-age clumsiness with impact | DCD assessment pathway | ADHD overflow, vision, joint hypermobility | Pure laziness |
| Persistent toe-walking | Full neurodevelopmental look | Habitual idiopathic pattern after normal exam | Ignore associated language or social red flags |
Clinical & Bedside Assessment
History that earns marks
Ask open, then specific. “Show me what worries you on your phone video.” Record first ages for key skills, any loss of skill, perinatal history, family neuromuscular or CP history, and how much floor time the child gets. Use corrected age for preterm infants in early life according to local developmental follow-up practice. [2] [3] [5]
Use a professional interpreter when language discordance exists. Child interpreters are not acceptable for this history. [8]
Watch before you handle
Put the child on a mat if safe. Watch spontaneous movement, transitions, how they use each side, and whether they seek toys across the midline. A two-minute observation often beats a rushed reflex list. [2] [3]
Examination skeleton
- Growth parameters and general appearance.
- Head control, pull-to-sit, sitting balance, protective responses by age.
- Rolling, pivoting, crawling or shuffling, pull-to-stand, cruising, gait.
- Reach, grasp, transfer, pincer, release, handedness timing.
- Tone, power, deep tendon reflexes, clonus, plantar responses.
- Spine, hips, limb lengths and orthopaedic constraints.
- Cranial nerves and bulbar cues if weakness is possible. [2] [5]
Document domain by domain and who reported each skill. Clear handover reduces lost information when another clinician continues the work. [11]
M.O.T.O.R. bedside
Investigations
Many children with normal quality inside WHO windows need no test — they need explanation and continued surveillance. [1] [3]
Order tests because the exam or trajectory demands them, not because a single skill is a few weeks later than a cousin. Hearing and vision matter when exploration or fine-motor tool use is off. Creatine kinase and neuromuscular work-up belong when progressive weakness or true hypotonia patterns appear — follow the floppy-infant pathway. Neuroimaging and early CP work-ups belong with red-flag tone, asymmetry, perinatal high-risk features or specialist tools such as general movements assessment and Hammersmith Infant Neurological Examination on their dedicated leaf. [3] [5]
Standardised developmental screens at key ages still apply; motor is one domain inside that programme. Do not invent proprietary tool cut-offs in a viva. [3]
Management — Resuscitation
Most motor reviews are outpatient. Convert immediately when you meet: [5] [9]
- motor regression with encephalopathy or seizures;
- progressive weakness with feeding or breathing compromise;
- suspected limb injury or safeguarding concern presented as “not moving the arm”;
- an unwell child whose “milestone visit” is the wrong label. [5] [9]
Those children use acute paediatric and neurology pathways first. [5]
Management — Definitive & Stepwise
- Map current skills to WHO windows and evidence-informed surveillance milestones. [1] [2]
- Classify normal, healthy variation, monitor, or escalate.
- Reassure with specifics when the exam is clearly normal — name the window and the next expected skills.
- Promote opportunity supports: supervised awake tummy time for infants who tolerate it, floor play, and less prolonged time in restrictive devices. These supports are not treatment for fixed upper-motor injury. [2] [3]
- Plan a timed recheck for borderline findings instead of vague “wait and see.”
- Refer early to physiotherapy or occupational therapy and early childhood intervention when delay or quality is abnormal.
- Escalate to paediatric neurology and early cerebral palsy detection pathways when tone, asymmetry or high-risk history demands it. Early, accurate CP diagnosis principles favour action over false reassurance. [5]
- Counsel with teach-back and written next steps; consent applies when sharing information with services. [12]
- Safety-net return triggers and chase referrals so the loop closes. [10]
- Document owners, dates and interim home strategies. [11]
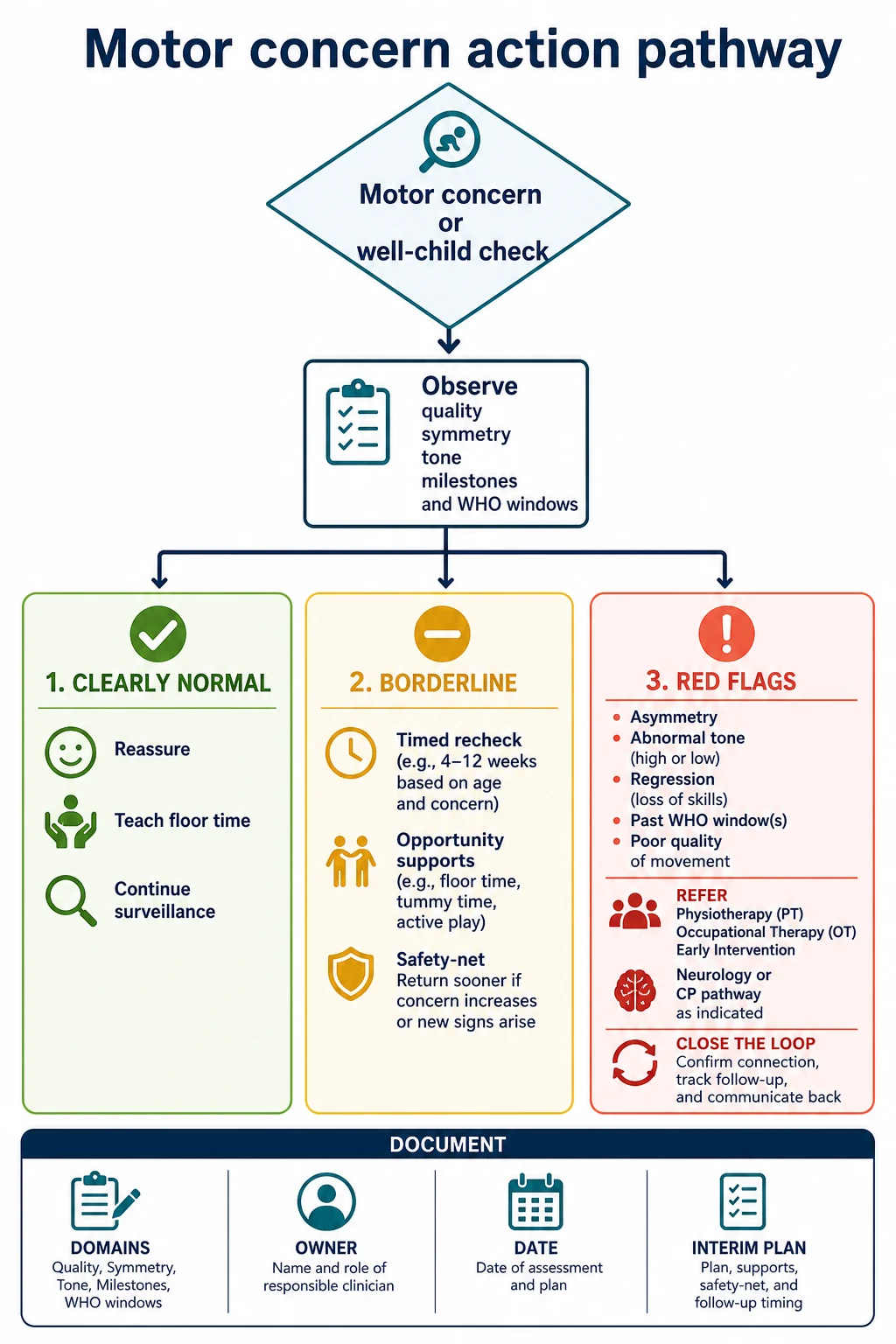
Read the figure like this: the product of the visit is a plan with a date, not a shrug. [3] [10]
Specific Subtypes & Scenarios
Term newborn. Establish baseline movement and feeding-related tone. Teach safe handling and supervised tummy time when awake. [2]
Ex-preterm infant. Use corrected age early, then transition toward chronological expectations as local follow-up protocols advise. Do not skip quality assessment because “prematurity explains everything.” [3] [5]
Bottom-shuffling eleven-month-old. If sitting, tone and fine motor are good, counsel variation and watch the walking window rather than forcing crawl practice as a moral project. [1]
Fifteen-month non-walker with normal exam. Still inside the WHO walking window. Re-examine carefully, promote opportunity, and set a clear review before the upper window is breached without progress. [1]
Eighteen-month non-walker. At or beyond the WHO 99th percentile for walking alone. This is not automatic cerebral palsy, but it is not casual reassurance either. Full exam and active referral planning are required. [1] [5]
Early hand preference at seven to ten months with fisting. Think hemiplegic pathway until proven otherwise. [5]
Clumsy school-age child. If motor coordination problems impair writing, sport or self-care, open a developmental coordination disorder assessment pathway using international recommendations rather than pejorative labels. [6]
Missing early history in out-of-home care. Rebuild the timeline from records and observation; catch-up surveillance is part of medical home work. [13]
Complications & Pitfalls
- Reassuring with outdated mean-age lists. [1] [2]
- Pathologising non-crawling when walking is on track. [1]
- Ignoring asymmetry because a few steps occurred. [5]
- Indefinite wait-and-see after caregiver concern. [3]
- Shotgun MRI for isolated late sitting with a normal neurological exam.
- Missing progressive weakness by calling the child a “late bloomer.”
- Using uncorrected age for early preterm motor calls.
- Open-loop referral with no interim therapy and no chase plan. [10] [11]
Prognosis & Disposition
Most children inside WHO windows with normal quality walk, run and play without motor disability. Disposition after a clearly normal visit is continued surveillance inside the medical home. Borderline visits need a dated review. Red-flag visits need referral plus interim support, not “refer and forget.” When true neuromotor pathology is present, earlier detection and intervention pathways improve the chance of better function. [1] [3] [5]
Safety-net concrete return triggers: loss of skills, new asymmetry, feeding collapse, or failure to gain the next planned skill by the agreed date. [10]
Special Populations
NICU graduates need structured motor surveillance and corrected-age thinking early. Known syndromes need a fresh look for change, not fatalism. Indigenous families need culturally safe counselling that does not blame carrying or kinship care practices for normal windows. Migrant and refugee families need interpreters and rebuilt timelines. Out-of-home care needs catch-up assessment. Socioeconomic disadvantage may limit floor space and therapy access — name the barrier and help navigate services. Technology-dependent children need protection from overshadowing. Neurodiverse children may have motor styles that coexist with sensory differences without one explaining away the other. [7] [8] [9] [13]
Evidence, Guidelines & Regional Differences
The WHO Motor Development Study supplies population windows for six gross motor milestones and documents that a minority of healthy children never show hands-and-knees crawling. [1] [4] Zubler and colleagues provide evidence-informed milestone content for surveillance tools so listed skills reflect ages when most children achieve them. [2] Lipkin’s AAP report frames motor findings inside every-visit surveillance and key-age standardised screening. [3] Novak and colleagues summarise advances supporting earlier cerebral palsy detection when the exam and risk profile demand it. [5] Blank and colleagues provide international DCD recommendations for school-age coordination disorders. [6]
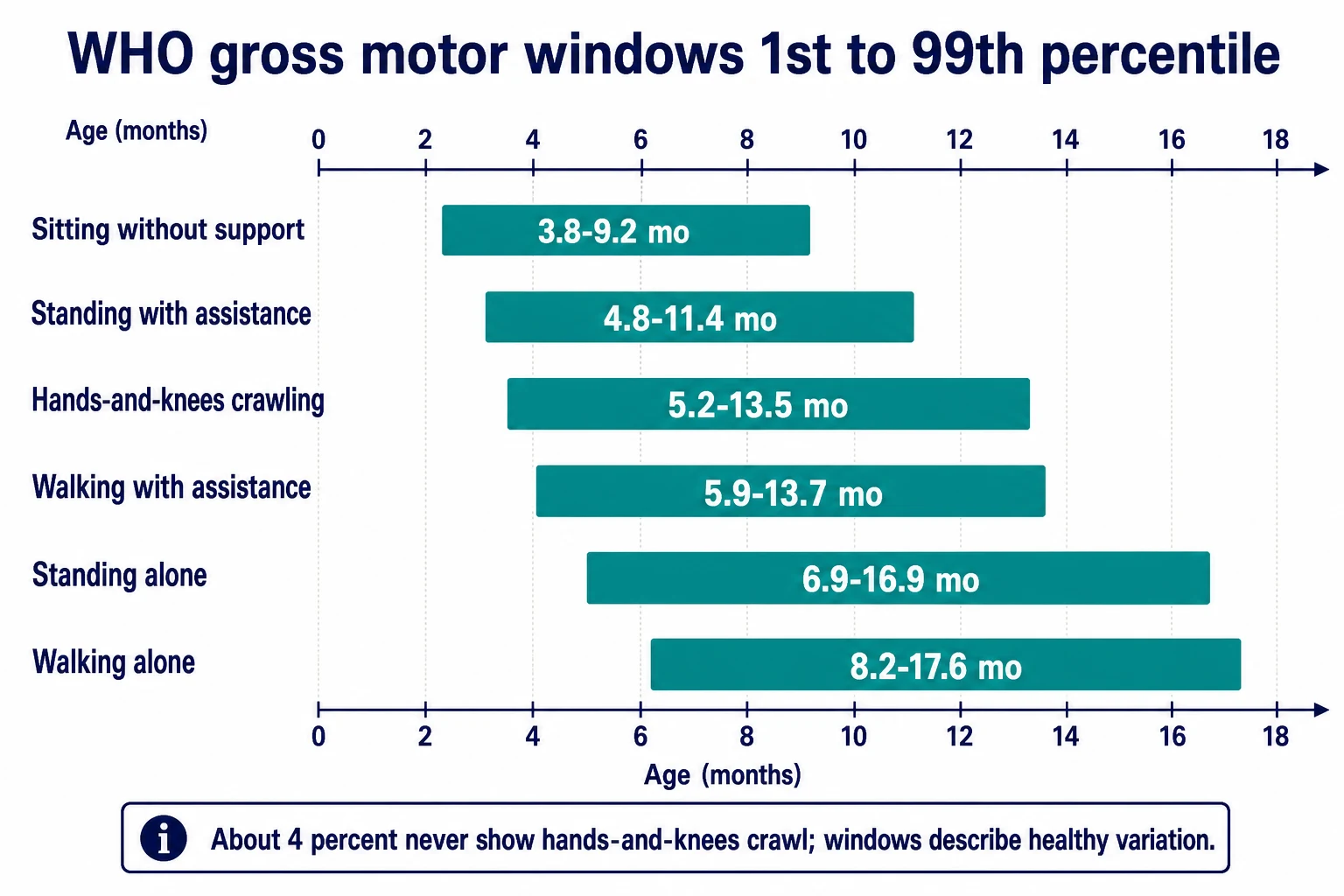
Read the figure like this: wide bars mean normal children disagree about timing. Your job is to know when disagreement becomes disease. [1]
Use local child health books, blue-book or Well Child Tamariki Ora contacts, and jurisdictional early intervention pathways. Cultural safety and interpreter access are part of valid motor history. Name local physiotherapy referral routes rather than inventing national cut-offs. [8]
Healthy Child Programme contacts and local community paediatric or child-development-team pathways shape escalation. Map NICE-aligned developmental concern routes used by your trust. [3]
Bright Futures and AAP surveillance-plus-screening schedules embed motor domain checks. Provincial Canadian tools vary — state the local programme rather than inventing universal ages beyond WHO and AAP anchors. [2] [3]
Exam Pearls
- Quote WHO windows, not playground averages. [1]
- About 4.3% of healthy WHO children never hands-and-knees crawl. [1]
- Walking alone 8.2–17.6 months; sitting 3.8–9.2 months. [1]
- Quality and symmetry beat a single birthday number. [5]
- Early hand preference with fisting is a red flag, not a talent show. [5]
- Correct age early for preterm infants. [3]
- Motor regression is never “variation.” [3]
- School-age functional clumsiness opens a DCD pathway, not insults. [6]
- Surveillance every visit; screening tools still matter at key ages. [3]
- Close the loop after every referral. [10] [11]
Sixty-second motor plan
Watch first
Spontaneous movement and transitions on the mat.
Place on windows
Compare key skills with WHO ranges and surveillance milestones.
Examine tone and symmetry
Power, reflexes, posture, handedness timing.
Choose the band
Normal, variation, monitor, or escalate.
Leave a dated plan
Reassure, recheck, or refer — with safety-net and owner.
References
- [1]WHO Multicentre Growth Reference Study Group WHO Motor Development Study: windows of achievement for six gross motor development milestones. Acta Paediatr Suppl, 2006.PMID 16817682
- [2]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439
- [3]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [4]WHO Multicentre Growth Reference Study Group Assessment of sex differences and heterogeneity in motor milestone attainment among populations in the WHO Multicentre Growth Reference Study. Acta Paediatr Suppl, 2006.PMID 16817680
- [5]Novak I Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA Pediatr, 2017.PMID 28715518
- [6]Blank R International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder. Dev Med Child Neurol, 2019.PMID 30671947
- [7]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [8]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI Evid Synth, 2020.PMID 32813387
- [9]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [10]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. Br J Gen Pract, 2025.PMID 39117428
- [11]Starmer AJ Changes in medical errors after implementation of a handoff program. N Engl J Med, 2014.PMID 25372088
- [12]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [13]Szilagyi MA Health Care Issues for Children and Adolescents in Foster Care and Kinship Care. Pediatrics, 2015.PMID 26416941