Paeds · growth-development-and-behaviour
School refusal and school attendance problems
Also known as School avoidance · School phobia (historical term) · Anxious school refusal · School non-attendance · School reluctance · Kearney functional model · Return-to-school plan
Fellowship guide to school refusal and attendance problems: behaviour not diagnosis, Kearney four-function analysis, Egger anxious-refusal versus truancy profiles, multi-informant assessment, exposure-based CBT and caregiver training, graded return-to-school, SSRI evidence for underlying anxiety (CAMS) with Melvin fluoxetine caution, and stepped multi-agency care.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
F.E.S.S. stack
Overview & Definition
A parent asks for a long medical certificate because their child “cannot cope with school.” The child is distressed on weekday mornings, stays home with a carer, and improves once school is off the table. That pattern is school refusal — a behavioural presentation, not a DSM or ICD diagnosis you can code as a freestanding disease. [1] [2] [3]
School refusal means difficulty attending school with emotional distress (anxiety, fear, somatic symptoms, or mood symptoms) in a young person who usually remains at home with caregiver knowledge. The old label “school phobia” is too narrow for exams: functions and drivers are heterogeneous. School anxiety or school reluctance is earlier fear or avoidance that still allows partial attendance — the best window for prevention before chronic absence consolidates. [1] [3]
Your job as a general paediatrician is to formulate the function of the non-attendance, exclude medical and safeguarding danger, treat the psychiatric or developmental driver, and write a graded return plan with school — not to convert every stomach-ache into open-ended home leave. [3] [4] [10]
Classification
Sort attendance problems by who knows, who initiated the absence, and what maintains it. [1] [3]
| Construct | Core feature | Intervention emphasis |
|---|---|---|
| Anxious school refusal | Distress-driven non-attendance; parents usually know | Exposure CBT, return plan, treat anxiety/mood |
| Truancy | Absence without permission; often externalising profile | Behavioural/systemic and school pathways |
| School withdrawal | Parent-condoned absence (illness beliefs, crisis, culture) | Family work, medical liaison, education law |
| School exclusion | System-initiated removal | Education advocacy plus treat any mental-health drivers |
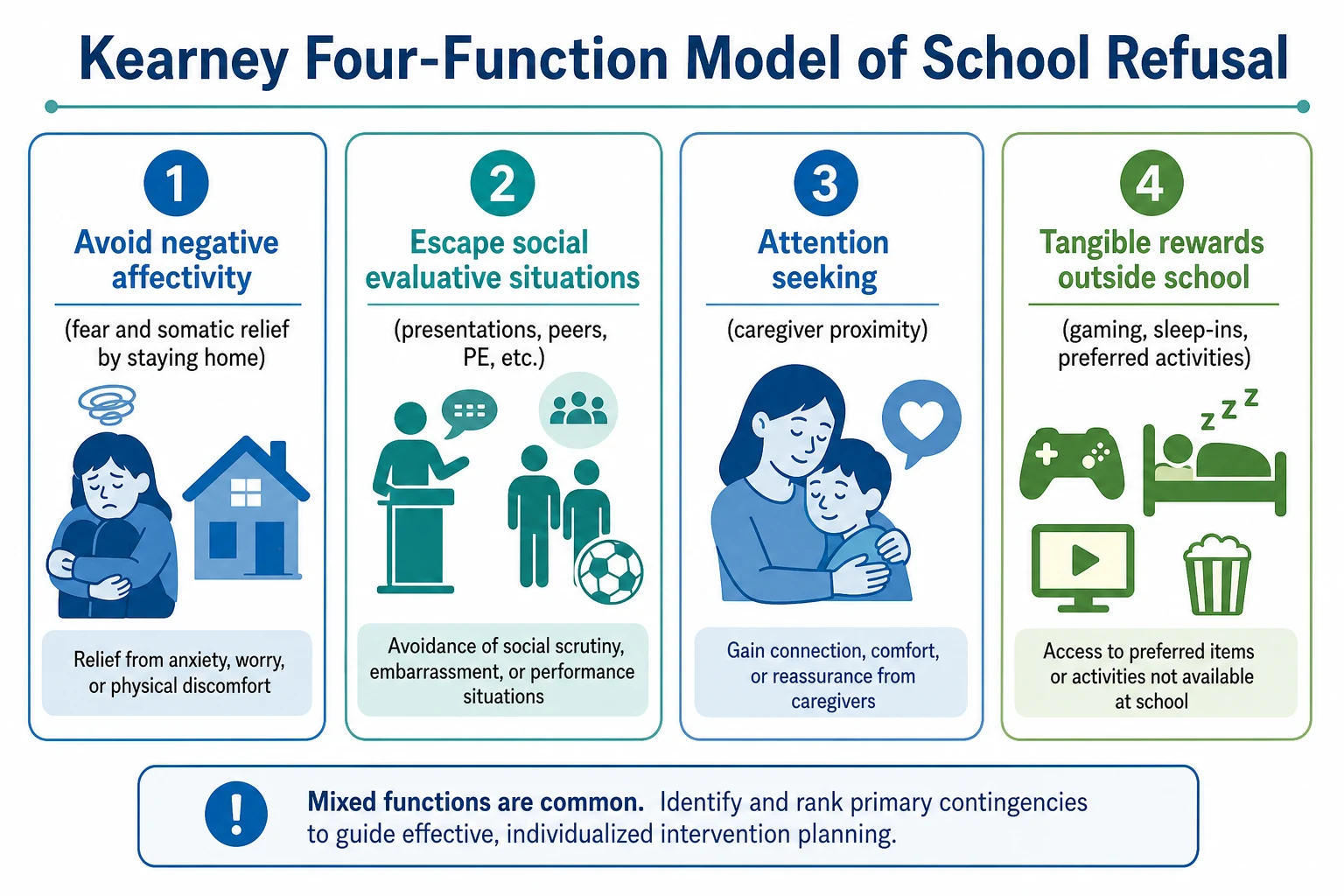
Kearney’s four functions are the viva framework. Youth often show mixed functions; rank the primary maintaining contingencies from interview, diary, and school collateral. [1] [2]
- Avoidance of negative affectivity — school, separation, or anticipatory anxiety/somatic distress falls when the child stays home (negative reinforcement). [1]
- Escape from aversive social/evaluative situations — presentations, PE, canteen, peer scrutiny, bullying contexts. [1]
- Attention-seeking — caregiver proximity, special attention for symptoms, reduced demands when distressed. [1]
- Tangible reinforcement outside school — gaming, sleep-ins, shopping, unstructured leisure that competes with school. [1] [2]
Common DSM/ICD drivers include separation anxiety, social anxiety, GAD, specific phobia, panic, major depression, and mixed anxiety–depression. Autism, ADHD, learning disorders, and trauma-related conditions frequently co-shape school distress. Code the psychiatric diagnosis that fits; treat school non-attendance as the functional problem. [3] [10]
Four clinical patterns examiners expect
Separation-driven
- Fear of harm to attachment figures
- Drop-off clinginess
- Weekday morning somatic symptoms
- Improves if parent stays nearby
Social-evaluative
- Fear of scrutiny and negative evaluation
- Avoids presentations, peers, PE
- Blushing, voice freeze, post-event rumination
- May attend with special arrangements
Mood-driven
- Anhedonia, low energy, hopelessness
- Global withdrawal not only school
- Sleep and appetite change
- Higher suicide-risk priority
Truancy/externalising
- Covert absence or peer-linked skipping
- Little anxiety about school itself
- Enjoyment of out-of-school activities
- Different pathway from pure exposure CBT
Epidemiology & Risk Factors
Community work by Egger and colleagues linked anxious school refusal with internalising disorders and a different psychiatric profile from truancy, which associates more with disruptive behaviour. Do not treat all non-attendance as one entity. [3]
Risk and maintaining factors include behavioural inhibition and anxiety diathesis; parental anxiety and modelling of avoidance; family accommodation; bullying (including online); undiagnosed learning or language difficulties; ASD sensory/social load; ADHD executive barriers; chronic medical illness and prolonged sick leave; transitions (school entry, primary-to-secondary, post-holiday); socioeconomic and transport barriers; and parental mental illness. [3] [10]
Consequences of untreated chronic non-attendance include academic lag, peer isolation, family conflict, secondary depression, reduced help-seeking, and longer-term educational risk mediated by persistent internalising disorders. [3] [10]
Exam-order framing
Pathophysiology
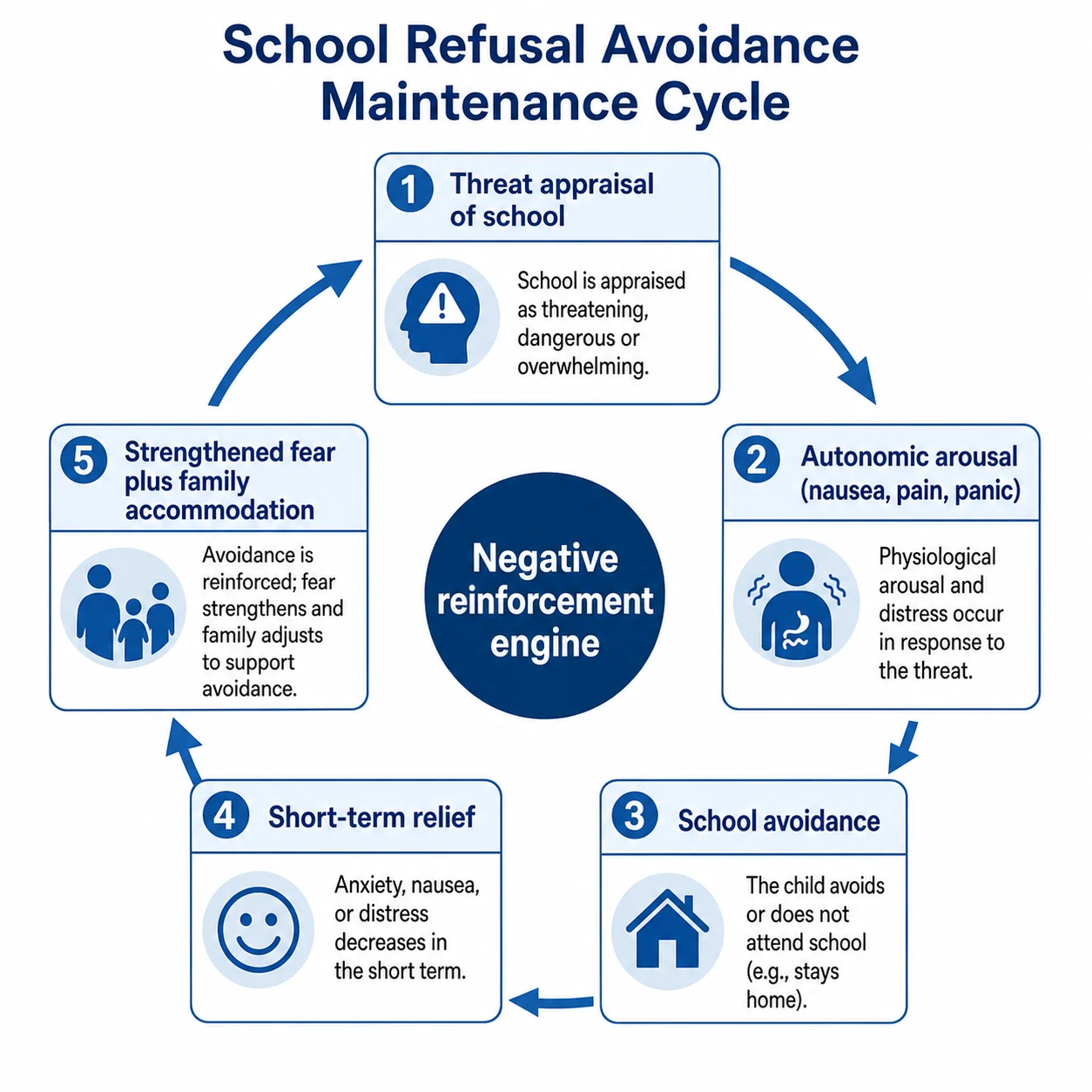
The engine of chronicity is short-term relief. When the child avoids school, fear and somatic arousal drop quickly. That is negative reinforcement. Home may also deliver attention and tangible rewards — positive reinforcement. Over weeks, anticipatory anxiety rises and self-efficacy collapses (“I cannot cope at school”). [1] [2]
Cognitive themes map to drivers: catastrophic separation beliefs; fear of negative evaluation; intolerance of uncertainty about performance; depressive hopelessness about peer belonging. [10]
Family systems matter. Accommodation (answering for the child, last-minute cancellations, unlimited reassurance, medical shopping) is usually well-intended and highly maintaining. Parental anxiety can synchronise with the child’s alarm system. [4] [5] [10]
Somatic pathway. Autonomic symptoms are read as illness. GP visits and certificates without a behavioural plan medicalise avoidance. Always exclude true medical red flags first, then avoid endless investigation as therapy by default. [3] [10]
Clinical Presentation
Primary-school separation pattern. Sunday-night dread; weekday morning abdominal pain, nausea, or headache that remits if the child stays home; tearful clinginess at the gate; preserved weekend function with cousins or screens. [3]
Adolescent social-evaluative pattern. Partial attendance; sick bay; missing oral assessments, PE, or specific teachers; online schoolwork may be intact while in-person school is avoided; post-event rumination and peer comparison. [1] [10]
MSE and multi-informant clues. Affect may look calm once school is “off the table”; distress rises when return is discussed. Thought content centres on anticipated catastrophe at school or home. Insight is often partial. Parent–youth discrepancy is common — prioritise attendance data and teacher reports over clinic minimisation. [3] [10]
Differential Diagnosis
| Differential | Discriminators | Why it matters |
|---|---|---|
| Truancy / ODD | Covert absence; little school-related anxiety; peer-linked skipping | Wrong if you only offer exposure hierarchy |
| Depression | Pervasive anhedonia, sleep/appetite change, hopelessness | Risk stratification and mood treatment intensity |
| ASD overload | Lifelong social-communication profile, sensory load | Adapt exposure; do not force “just try harder” |
| Learning/language disorder | Subject-specific failure, literacy history | Education assessment changes the hierarchy |
| Bullying / safety threat | Specific peers, locations, online harassment | Safety plan may precede full return |
| Medical disease | Red-flag exam/labs; nocturnal symptoms; progressive course | Do not miss organic illness |
| OCD / PTSD / psychosis prodrome | Obsessions, trauma re-experiencing, odd beliefs | Different specialist pathways |
Clinical & Bedside Assessment
Interview the young person alone and with carers. Structure: onset and course; fear map; somatic pattern by day of week; attendance calendar; antecedents (Sunday night, particular lessons, peers); consequences (parent attention, gaming, reduced demands); bullying; sleep; substances; self-harm and suicide; developmental and neurodiversity history; family psychiatric history; prior certificates and school responses. [1] [3] [10]
Functional analysis (Kearney). Rank each of the four functions from history and diary. Mixed functions need multi-pronged contingencies. [1] [2]
Collateral. School attendance officer, year coordinator, wellbeing staff, GP. Ask about partial attendance, library refuge, toilet avoidance, and peer conflicts. [10]
Scales (adjuncts). SCARED, SCAS, RCADS for anxiety; mood and self-harm screens as indicated. Track attendance percentage as a primary outcome alongside symptoms. [10]
Risk and legal. Anxiety does not protect against suicide. Explain confidentiality limits. Capacity principles are decision-specific. Compulsory education and mental-health legal tools are jurisdiction-specific — name local frameworks; do not invent foreign section numbers. [10] [11]
Investigations
Targeted medical review when red flags exist (weight loss, nocturnal pain waking the child, focal neurology, fever, progressive systemic features). Plot height and weight. Take relevant observations before medication. ECG when history, dose, combination risk, or local protocol indicates cardiac screening. No routine brain imaging for uncomplicated school anxiety. Avoid serial tests that delay graded return without improving safety. [10]
Management — Resuscitation
Stabilise risk first. For acute panic-like presentations, exclude medical emergency when indicated, then plan rapid outpatient exposure-based care rather than long-term benzodiazepines for chronic school anxiety in youth. [10]
Certificates. If a short medical certificate is truly needed for acute unfitness, pair it with a written reintegration date and plan. Indefinite certificates are a common iatrogenic pitfall. [1] [4]
Management — Definitive & Stepwise
Core principles
- Psychoeducation: school refusal is treatable behaviour maintained by avoidance and contingencies; families did not “cause” anxiety by caring, but accommodation can maintain it. [4] [5]
- Function-matched intervention: exposure for negative-affectivity and social-evaluative functions; contingency management for attention and tangible-reward functions. [1] [2]
- Graded return-to-school as active treatment, not optional aftercare. [4] [5]
- Treat the psychiatric driver with evidence-based youth anxiety/depression care. [8] [9] [10]
Psychological therapy
Exposure-based CBT is first-line psychological care for anxiety-driven school refusal. Controlled evaluation supports CBT for school-refusing children. Trials of child therapy plus caregiver training emphasise the parental role in supporting attendance and reducing accommodation. [4] [5]
Active ingredients examiners want named: psychoeducation; emotion identification; cognitive restructuring of catastrophic school/separation beliefs; fear hierarchy and graded in vivo exposure to school steps; contingency management (remove high-value home rewards during school hours; reward approach behaviours); parent sessions; school liaison; relapse prevention. [4] [5] [9]
Broader youth anxiety CBT evidence (Cochrane review; comparative effectiveness meta-analysis) supports exposure-based CBT when an anxiety disorder drives the presentation. [9] [13]
Graded return-to-school plan
Same-week return architecture
School meeting this week (sooner if complete absence)
Write hierarchy: drive past → gate → short wellbeing room → partial preferred subjects → full day with check-ins → normal timetable
Escort/safe-person early, then fade supports
No competing high-value home leisure during school hours
Address bullying, learning supports, and ASD/sensory adaptations in parallel
Measure attendance weekly; expect short-term anxiety rise as attendance improves
Pharmacotherapy
Medication is not first-line for “school refusal” as a behaviour. It is indicated for moderate–severe underlying anxiety or depression, CBT non-response/unavailability, or combination strategies when impairment is high. [8] [10]
| Evidence | Population / design | Exam takeaway |
|---|---|---|
| CAMS Walkup 2008 | Ages 7–17; separation, GAD, social anxiety; CBT vs sertraline vs combo vs placebo | Combo highest acute CGI response; CBT and sertraline each beat placebo |
| Birmaher fluoxetine 2003 | Childhood anxiety RCT | Fluoxetine efficacious vs placebo |
| Melvin 2017 | Anxious school-refusing adolescents; CBT ± fluoxetine | Fluoxetine augmentation did not clearly outperform CBT alone for key outcomes — avoid overclaiming SSRI superiority for SR attendance specifically |
| Bernstein 2000 | School refusal; imipramine + CBT vs placebo + CBT | Historical TCA + CBT signal; modern practice prefers SSRIs with monitoring, not routine first-line TCAs |
Use CAMS for the underlying separation/social/GAD package, Melvin for SR-specific fluoxetine caution, and Bernstein as historical TCA context only. [6] [7] [8] [14]
Practical SSRI starts (when indicated for underlying anxiety/depression). Prefer low start and slow titration with structured monitoring. [8] [10]
- Sertraline: commonly 25 mg oral daily in children (some adolescents 25–50 mg depending on size/sensitivity), titrate gradually; CAMS allowed flexible titration up to 200 mg oral daily. Monitor activation, GI effects, sleep change, headache, and suicidality/self-harm thoughts especially early and after dose increases. [8] [11]
- Fluoxetine: typical start 10 mg oral daily, often toward 20 mg as needed with monitoring; Melvin trial context is school-refusing adolescents — use for anxiety/mood indication, not as a magic attendance pill. [6] [14]
Black-box / suicidality counselling. Meta-analysis of paediatric antidepressant RCTs shows a small absolute increase in suicidal ideation/behaviour signals versus placebo alongside clinical response benefits — discuss risk–benefit, involve carers, schedule early review. [11]
Benzodiazepines are poor fellowship answers for chronic youth school anxiety maintenance (dependence, cognitive effects, weak long-term evidence). [10]
Family and multi-agency work
Train carers to limit excessive reassurance, support planned exposures, and hold consistent morning routines. Coordinate GP, school, and specialist mental health so messages do not conflict. Parent-led and school-based supports expand access in stepped care for milder presentations. [5] [10]
Specific Subtypes & Scenarios
Preschool/early primary separation. Heavier parent coaching; brief classroom settling plans; medication threshold high and specialist. [10]
Adolescent social anxiety with exam avoidance. Exposure to evaluative situations; school adjustments that do not permanently remove all evaluation; consider SSRI if severe impairment. [8] [10]
Mixed anxiety–depression chronic non-attendance. Prioritise risk; combine behavioural activation with school hierarchy; lower threshold for SSRI plus intensive CBT. [6] [11]
ASD + school distress. Visual schedules, sensory plan, predictable transitions; exposure still needed for phobic avoidance, but social-communication load must be adapted. [10]
Post-illness reintegration. Time-limited medical leave with explicit return dates; avoid “wait until 100% well.” [1]
Cultural and ANZ context. Explore idioms of distress, family hierarchy, Indigenous cultural safety, interpreter needs, and rural telehealth CBT access without abandoning attendance goals. [10]
Complications & Pitfalls
Failing viva answers: calling school refusal a diagnosis; pure medicalisation of morning pain; open-ended home schooling; punitive discipline alone for anxious refusal; benzodiazepines as default; starting SSRI without exposure plan or monitoring; missing bullying, learning disorder, depression, or safeguarding; waiting for anxiety to fully remit before any school contact. [1] [3] [6] [11]
Prognosis & Disposition
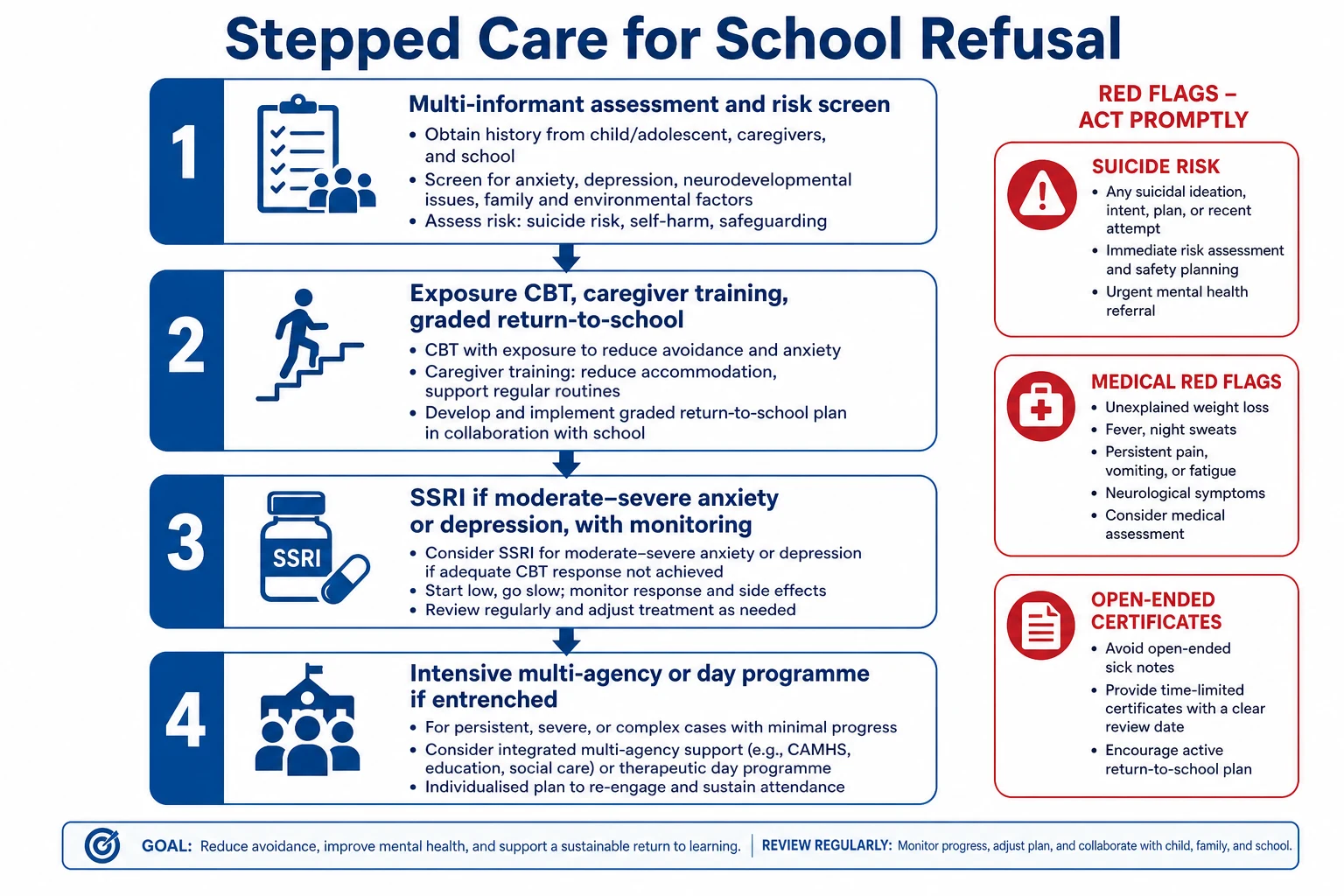
Earlier consistent intervention improves trajectory. Chronic multi-year non-attendance is harder and often needs intensive multi-agency care. Attendance may improve before anxiety fully remits — that is expected in exposure work. Stepped care: school–GP liaison and parent-supported CBT for mild → specialist CBT for moderate → SSRI or combination for moderate–severe/non-response → intensive community or day programmes for entrenched avoidance. [4] [5] [8] [10]
Special Populations
Neurodevelopmental disorders, intellectual disability (simplified hierarchies), LGBTQ+ minority stress and school climate, refugee/trauma backgrounds, out-of-home care, and medically complex youth need adapted formulation without abandoning graded return principles. [10]
Evidence, Guidelines & Regional Differences
ANZ. General paediatric and CAMHS practice uses Kearney-informed formulation, exposure CBT, school liaison, and SSRI evidence (CAMS/fluoxetine) within public services, private specialists, and education systems. Cite international trial evidence plus local consent, mandatory reporting, and education-law frameworks. Do not invent foreign Mental Health Act section numbers. [4] [8] [10]
Named evidence stack for viva: Kearney functional model; Egger community study; King 1998 CBT; Heyne 2002 child + caregiver training; Melvin 2017 CBT ± fluoxetine; Bernstein 2000 imipramine + CBT (historical); CAMS Walkup 2008; James Cochrane CBT 2020; AACAP Walter 2020. [1] [3] [4] [5] [6] [7] [8] [9] [10]
Exam Pearls
- School refusal = behaviour, not diagnosis. [1]
- Anxious refusal ≠ truancy (Egger profiles). [3]
- Weekday somatic symptoms remitting at home scream anxiety pathway — still exclude medical red flags. [3]
- Melvin: do not claim fluoxetine clearly beats CBT alone for adolescent school-refusal attendance. [6]
- CAMS still anchors treatment of the underlying separation/social/GAD package. [8]
- Always counsel activation and suicidality monitoring with youth antidepressants. [11]
References
- [1]Kearney CA, Albano AM. The functional profiles of school refusal behavior. Diagnostic aspects. Behav Modif, 2004.PMID 14710711
- [2]Kearney CA. Forms and functions of school refusal behavior in youth: an empirical analysis of absenteeism severity. J Child Psychol Psychiatry, 2007.PMID 17244270
- [3]Egger HL, Costello EJ, Angold A. School refusal and psychiatric disorders: a community study. J Am Acad Child Adolesc Psychiatry, 2003.PMID 12819439
- [4]King NJ, Tonge BJ, Heyne D, Pritchard M, et al. Cognitive-behavioral treatment of school-refusing children: a controlled evaluation. J Am Acad Child Adolesc Psychiatry, 1998.PMID 9549960
- [5]Heyne D, King NJ, Tonge BJ, Rollings S, et al. Evaluation of child therapy and caregiver training in the treatment of school refusal. J Am Acad Child Adolesc Psychiatry, 2002.PMID 12049443
- [6]Melvin GA, Dudley AL, Gordon MS, Klimkeit E, et al. Augmenting Cognitive Behavior Therapy for School Refusal with Fluoxetine: A Randomized Controlled Trial. Child Psychiatry Hum Dev, 2017.PMID 27485100
- [7]Bernstein GA, Borchardt CM, Perwien AR, Crosby RD, et al. Imipramine plus cognitive-behavioral therapy in the treatment of school refusal. J Am Acad Child Adolesc Psychiatry, 2000.PMID 10714046
- [8]Walkup JT, Albano AM, Piacentini J, Birmaher B, et al. Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. N Engl J Med, 2008.PMID 18974308
- [9]James AC, Reardon T, Soler A, James G, Creswell C. Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database Syst Rev, 2020.PMID 33196111
- [10]Walter HJ, Bukstein OG, Abright AR, Keable H, Ramtekkar U, et al. Clinical Practice Guideline for the Assessment and Treatment of Children and Adolescents With Anxiety Disorders. J Am Acad Child Adolesc Psychiatry, 2020.PMID 32439401
- [11]Bridge JA, Iyengar S, Salary CB, Barbe RP, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA, 2007.PMID 17440145
- [12]Connolly SD, Bernstein GA, Work Group on Quality Issues. Practice parameter for the assessment and treatment of children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry, 2007.PMID 17242630
- [13]Wang Z, Whiteside SPH, Sim L, Farah W, et al. Comparative Effectiveness and Safety of Cognitive Behavioral Therapy and Pharmacotherapy for Childhood Anxiety Disorders: A Systematic Review and Meta-analysis. JAMA Pediatr, 2017.PMID 28859190
- [14]Birmaher B, Axelson DA, Monk K, Kalas C, et al. Fluoxetine for the treatment of childhood anxiety disorders. J Am Acad Child Adolesc Psychiatry, 2003.PMID 12649628