Paeds · growth-development-and-behaviour
Specific learning disorders
Also known as Specific learning disorder · Learning disability · Dyslexia · Dyscalculia · Dysgraphia · Reading disability · Written expression disorder · Mathematics learning disorder
Fellowship guide to specific learning disorders: DSM-5 domain thinking for reading, writing and maths; medical evaluation of academic underachievement; differentials from IDD, ADHD and sensory impairment; psychoeducational pathway; evidence-based remediation; school supports; and exam defence across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A Year 3 teacher writes: “bright child, cannot read.” The parents ask whether the eyes need exercises. Your job is not to hand out a brand of therapy. Your job is to decide whether this is a specific learning disorder (SLD), what domain is affected, what medical mimics must be excluded, and how the child will be taught and supported while you wait for formal testing. [1] [3]
SLD means persistent difficulty learning and using academic skills. The difficulty starts during the years of formal schooling. It is not better explained by intellectual disability, uncorrected sensory impairment, neurological disease alone, lack of instruction, or psychosocial adversity alone. The child’s general reasoning is usually within the broad average range or higher. The underachievement is unexpected relative to age, opportunity and overall ability. [3] [4]
Older labels such as “learning disability,” “dyslexia,” “dysgraphia” and “dyscalculia” still appear in school reports and family language. DSM-5 folds them into one clinical category — specific learning disorder — with domain specifiers. In clinic you still use the familiar words, because families recognise them, but you diagnose with domain precision. [3] [4]
This page owns the medical and developmental approach to SLD. Global cognitive impairment belongs with intellectual developmental disorder. Attention-first pathways belong with ADHD. Pure oral language delay has its own leaf. Do not hide those chapters here. Cross-link them. [5] [15]
Classification
Classify three things early: the academic domain, the severity, and the system label (clinical diagnosis versus school eligibility). They are related, not identical. [3] [4]
Domain specifiers
| Domain | Everyday names | What fails | What often stays stronger |
|---|---|---|---|
| Reading | Dyslexia, reading disability | Word reading accuracy, fluency, reading comprehension | Oral conversation in many children |
| Written expression | Dysgraphia, written language disorder | Spelling, grammar, organisation, handwriting/transcription | Spoken ideas that outrun the page |
| Mathematics | Dyscalculia, math learning disability | Number sense, fact retrieval, calculation, math reasoning | Reading may be intact |
A child can have one domain or several. Comorbidity across reading, maths and ADHD is common and not random. [4] [13]
Severity
Severity is clinical: how much support the child needs to learn academic skills. Mild may manage with targeted classroom support. Moderate needs intensive specialised teaching. Severe needs ongoing individualised instruction across settings. Exact cut-offs on proprietary tests live in manuals — do not invent them in a viva. [4]
Clinical diagnosis versus school category
A clinical SLD formulation and a school “learning disability” or “additional learning needs” category serve different legal systems. The paediatrician’s job is medical clarity plus advocacy so the education plan matches the child’s real skill profile. Names differ by country; the principle does not. [11]
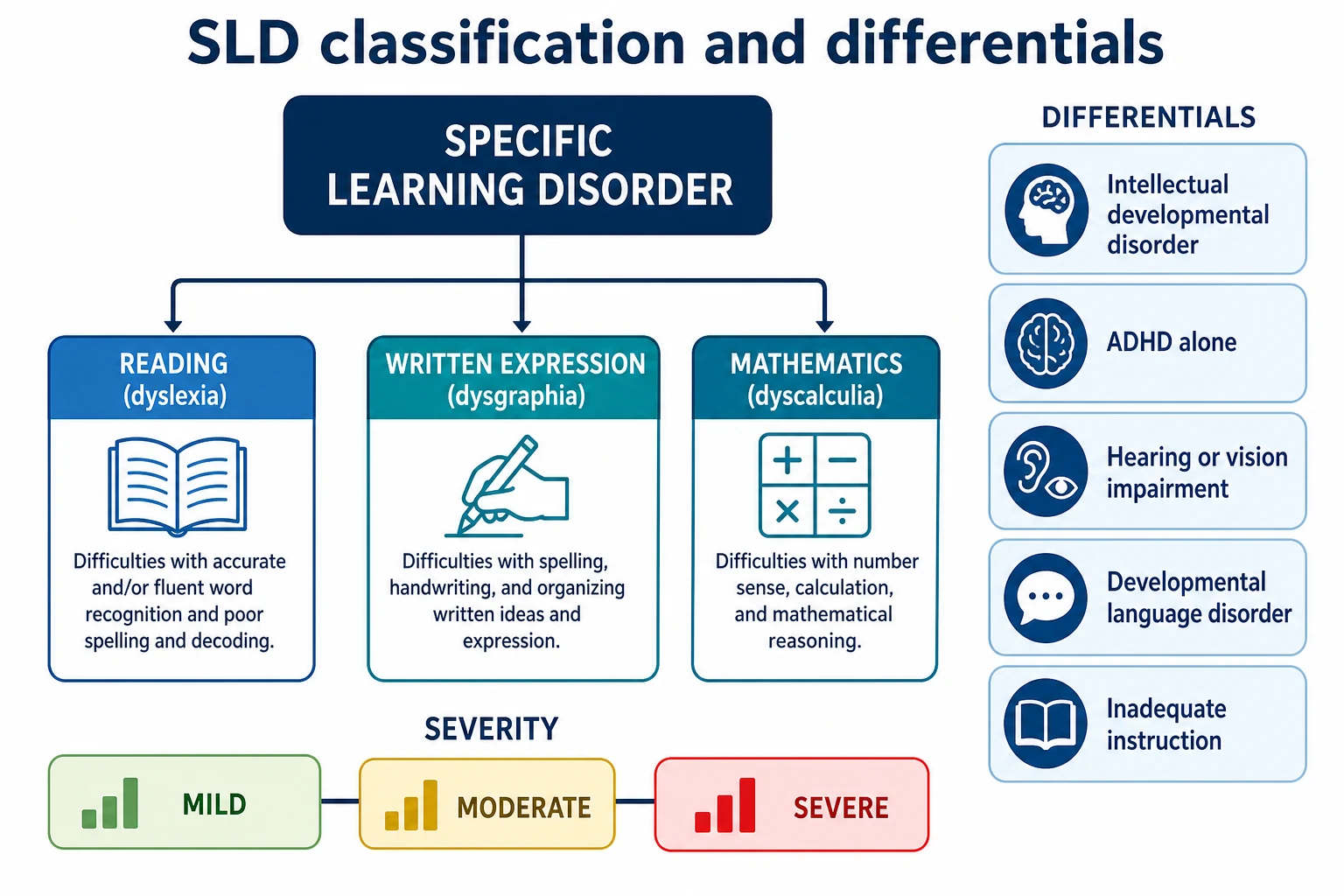
Read the figure like this: if you jump from “poor school marks” to a single label, you will miss either a sensory mimic or a second domain that needs its own intervention. [1] [4]
Models of identification
The old IQ–achievement discrepancy model waited until a gap was large enough to “prove” disability. That delayed help for young children. Modern practice uses response to high-quality instruction (RTI / multi-tiered systems of support) plus a pattern of strengths and weaknesses on comprehensive assessment. Non-response to good teaching strengthens the case for SLD. It does not replace clinical judgement or sensory checks. [3] [7]
Epidemiology & Risk Factors
SLD is common enough that every general paediatric clinic will see it. Reported prevalence depends on criteria, language and school systems. Moll’s school-age work shows domain-specific rates that commonly sit in a roughly 5–15% discussion range depending on thresholds and whether single or multiple domains are counted. Do not quote a single universal percentage as if it were a laboratory constant. [4]
Reading SLD is identified more often in boys in many samples. Part of that difference is true liability; part is referral bias and behaviour that brings boys to attention. Girls with compensated reading difficulty may present later with anxiety or secondary-school volume overload. [4] [18]
Risk factors do not equal destiny. They change prior probability: [3]
- Family history of reading or maths difficulty (strong genetic contribution for dyslexia). [3]
- Early oral language delay and developmental language disorder. [9] [15]
- Prematurity, very low birth weight, lead exposure, chronic otitis media with hearing impact, iron deficiency — medical and environmental contributors that still require domain assessment. [1]
- Limited print exposure and socioeconomic disadvantage — confounders and amplifiers, not proof of “laziness.” [12]
- ADHD comorbidity — shared pathways and additive academic risk. [5] [13]
Under-identification is patterned: culturally and linguistically diverse learners, children in out-of-home care with fragmented schooling, and quiet high-achieving families who tutor around the problem until Year 9. [16] [17]
Pathophysiology
Start with the skill the child is trying to learn, then the cognitive route that failed. [3]
Reading (dyslexia)
Most children with dyslexia have a phonological bottleneck. They struggle to hear and manipulate the sound structure of language, map sounds to letters, and build automatic word recognition. Fluency never becomes effortless, so comprehension collapses under time pressure even when listening comprehension is better. Peterson and Pennington synthesise the cognitive and neural literature: left-hemisphere reading networks, including temporoparietal and occipitotemporal systems, are repeatedly implicated. [3]
Not every reading problem is pure phonology. Orthographic knowledge, rapid naming and language comprehension each can contribute. Children with co-occurring developmental language disorder show different literacy profiles from pure dyslexia — Snowling’s profile work matters when you plan speech-language input. [15]
Mathematics (dyscalculia)
Butterworth frames dyscalculia as a core number-sense difficulty — representing and manipulating numerical magnitude — with educational consequences for fact learning and calculation. Population surveys such as Reigosa-Crespo’s Havana work link basic numerical capacities to prevalence estimates of developmental dyscalculia. [10] [19]
Written expression
Writing is not “spelling only.” Berninger’s model separates transcription (handwriting, keyboarding, spelling) from text generation (words, sentences, discourse) and shows how attention and executive functions load the writing system. A child can talk fluently and still produce almost nothing on the page. [6] [20]
Shared and secondary pathways
Working memory and processing speed support all three academic domains without making every slow worker “ADHD.” When ADHD is also present, academic skill acquisition and classroom output both suffer — DuPaul’s comorbidity framing is the exam-safe way to say this. [5] [20]
Instructional casualties matter mechanistically. Weak teaching or chronic absenteeism can produce skill gaps that look like SLD until quality instruction is delivered. SLD diagnosis assumes the child has had a fair chance to learn. [3] [7]
Secondary harm is real: repeated failure breeds anxiety, avoidance of reading aloud, school refusal and a self-story of being “stupid.” That emotional cascade is treatable and preventable with earlier accurate framing. [3] [12]
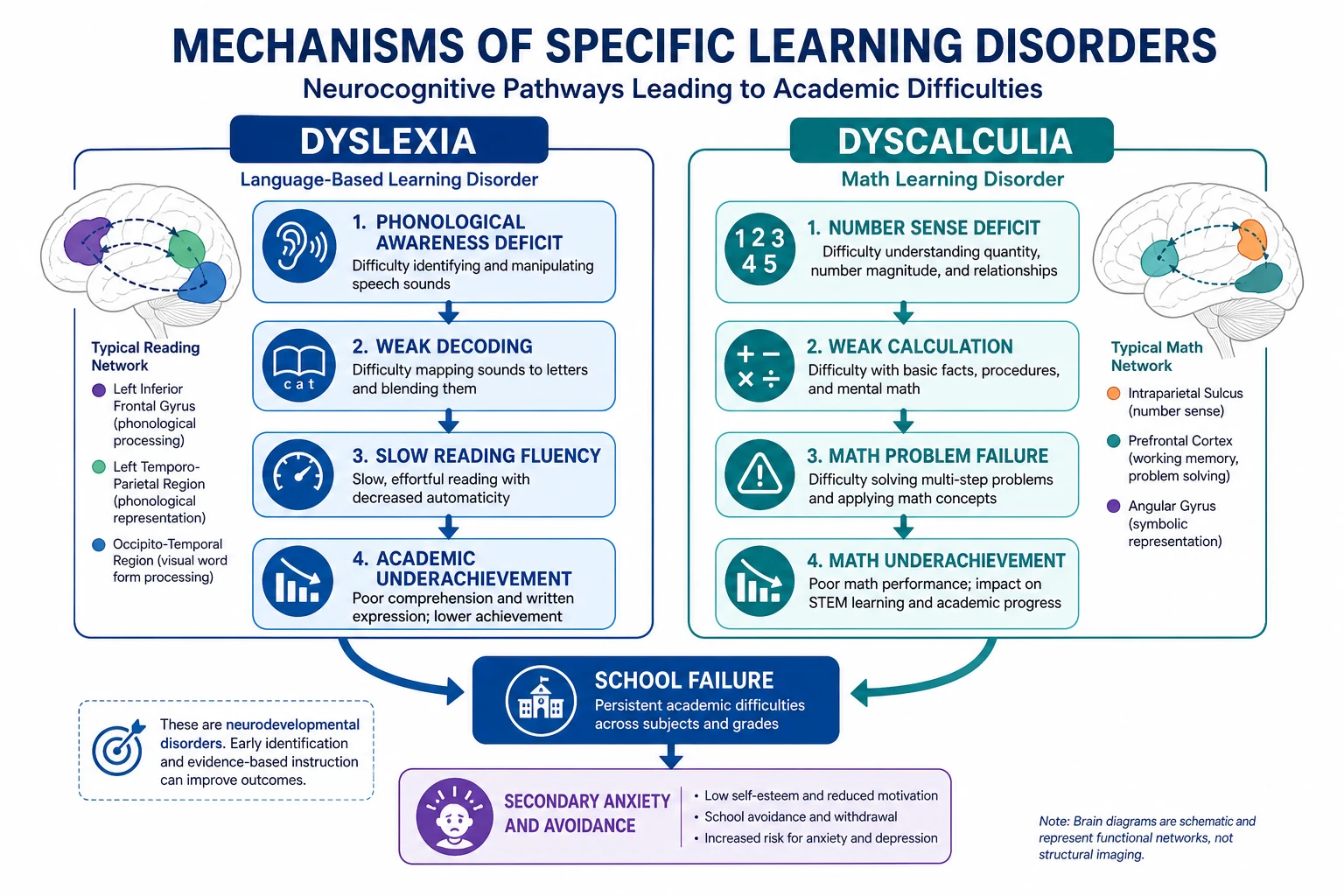
Read the figure like this: remediation must hit the failed route (phonics/structured literacy; number sense), not only “try harder” or eye exercises. [1] [3] [10]
Clinical Presentation
SLD presents as school work, not as a rash. You hear it in report cards and you see it in how the child approaches print and numbers. [3]
Early school years
- Slow letter-sound learning; guessing from pictures.
- Painful oral reading; loss of place; refusal to read aloud.
- Spelling that does not match the sounds the child can say.
- Finger counting for simple sums long after peers stop.
- Extremely short written answers despite rich spoken stories.
Later presentation
Bright children may compensate with memory and context until secondary school multiplies reading volume. Then marks fall, homework wars begin, and anxiety appears. Girls may present with perfectionism and internalising symptoms rather than classroom disruption. [3] [18]
Behaviour as the ticket of entry
“Naughty in literacy hour” can be SLD plus shame. “Doesn’t listen” can be ADHD, language disorder, hearing loss — or all three. Always ask what the child does when the task is oral versus written. [5] [15]
Atypical and high-risk presentations
- Multilingual households where instruction language is new — still possible true SLD, but language opportunity must be assessed. [16]
- Foster care with school moves and missing records. [17]
- Chronic illness with missed schooling versus primary SLD. [11]
- Twice-exceptional: high reasoning with a deep domain weakness. [3]
Differential Diagnosis
Examiners want the features that separate each alternative, not a laundry list. [1] [5]
Other important mimics and co-travellers: [15] [6]
- Developmental language disorder — oral language weak first; literacy often follows. Profile analysis distinguishes pure dyslexia from dyslexia-plus-language disorder. [15]
- Anxiety, depression, sleep debt — reduce output; look for skill gaps that pre-dated the mood change. [5]
- Autism — uneven academics can occur; social communication phenotype is the discriminator (cross-link autism leaves). [3]
- Developmental coordination disorder — graphomotor limits handwriting; spelling and idea generation may still show language-based SLD. [6]
- Acquired or progressive neurology — new decline after normal attainment is not lifelong SLD; think neurology. [1]
Clinical & Bedside Assessment
History that earns marks
Ask in learning order: what skill fails, since when, in which settings, after what teaching, and what has already been tried. [3]
- Onset and domains — reading, spelling, writing volume, maths facts, word problems.
- Instruction quality — school changes, absenteeism, phonics exposure, language of instruction.
- Early development — speech-language milestones, ear infections, perinatal risk.
- Family academic history — parents’ own school struggles.
- Attention, sleep, mood, bullying, school refusal.
- Languages spoken at home and interpreter need. [16]
Examination
- Growth and general examination.
- Dysmorphology and neurocutaneous signs if phenotype suggests.
- Full neurological screen with focus on tone, coordination, and focal signs.
- Vision and hearing — do not skip; document plan for formal testing if any doubt. [1] [2]
- Brief informal sampling: letter sounds, graded oral reading, dictated spelling, simple calculation — as screens, not diagnoses.
Formulation at the bedside
Write a one-line problem representation: “School-age child with persistent word-reading and spelling weakness despite mainstream instruction, average conversational language, possible family history of dyslexia; hearing/vision pending; ADHD traits to clarify.” That sentence drives tests and referrals. [3] [5]
Investigations
Always consider first
- Audiology when communication, attention or literacy is in question.
- Optometry/ophthalmology for acuity and ocular health — not as a freestanding “dyslexia cure” pathway. [1] [2]
Core educational investigation
Comprehensive psychoeducational assessment is the diagnostic backbone when difficulties persist. Typical elements include general cognitive ability, academic achievement across reading/writing/maths, and processing measures relevant to the complaint (for example phonological processing in reading SLD). Interpret patterns, not a single subtest. Manual cut-offs are proprietary — describe principles in exams, not invented numbers. [3] [6]
Often useful adjuncts
- Speech-language pathology assessment when oral language is weak or history suggests DLD. [15]
- Occupational therapy when graphomotor output is a major limiter. [6]
- Structured ADHD evaluation when attention symptoms impair learning or testing validity. [5]
Usually low value in isolated SLD
Routine brain MRI, broad metabolic panels, or shotgun genetics without neurological red flags, dysmorphic syndromes, or progressive features. Order targeted tests when history or examination changes the prior probability. [1]
Using school RTI data
Curriculum-based measures and tiered intervention logs show whether the child received sufficient high-quality instruction. Non-response supports SLD formulation. Missing intervention data weakens certainty and should trigger teaching intensity first when safe. [7]
Management — Resuscitation
“Resuscitation” in SLD is the conversion out of a quiet learning clinic when safety is threatened. [17]
- Suicidality, severe school refusal, or acute mental-health crisis — urgent mental-health pathway; do not leave the family with only a psychology waitlist letter.
- Regression, encephalopathy, new focal neurology — emergency/urgent neurology, not SLD paperwork.
- New sensory loss — same-day or urgent specialty review.
- Safeguarding — follow local child-protection process.
- Medically unwell child — treat illness; defer educational testing.
Management — Definitive & Stepwise
Paediatric SLD pathway
Clarify the domain and history
Reading, writing, maths; onset; languages; family history.
Exclude sensory and medical red flags
Hearing, vision, neurology, regression pathway.
Start or intensify high-quality instruction
Do not wait years for a perfect report before teaching.
Formal psychoeducational assessment if persistent
Pattern-based diagnosis; speech/OT/ADHD adjuncts as needed.
Domain-specific remediation + accommodations
Skills teaching plus access supports; treat comorbidity.
School–health plan and review
Closed-loop coordination; escalate if non-response.
Reading intervention
Effective reading intervention for word-level disability is structured, explicit, and phonics-rich (structured literacy). Torgesen showed that intensive remedial instruction can produce meaningful immediate and longer-term gains in children with severe reading disabilities. Early oral language programmes (Fricke; lasting NELI-related literacy benefits in Hulme’s later work) matter for prevention and for children whose language underpins literacy. [7] [9] [14]
Brand names are not magic. Stevens’ review of Orton-Gillingham-based interventions found limited high-quality evidence for that brand family as a universal solution. Teach the active ingredients (explicit phonology, decoding, fluency practice) rather than selling a logo. [8]
Writing and maths
- Writing: target transcription (spelling, handwriting/keyboarding) and composition separately; reduce copy load while skills grow. [6]
- Maths: rebuild number sense, fact fluency and problem language; calculator policies are accommodations, not cures. [10] [19]
Classroom accommodations
Extra time, text-to-speech, speech-to-text, reduced copying, note scaffolds, quiet testing spaces, and accessible worksheets protect learning while remediation runs. Accommodations without teaching leave the skill gap untouched. [6] [11]
Comorbidity care
If ADHD is present, treat it — but do not claim the SLD is cured when attention improves. Re-check academic skills. Anxiety treatment may be essential for school attendance and practice volume. [5]
Paediatrician roles that boards test
- Medical exclusion and red-flag triage.
- Clear explanation that SLD is not laziness and not primarily a vision-therapy problem. [1] [2]
- Contribution to educationally related service planning and care coordination. [11] [17]
- Primary-care literacy promotion as prevention and early support (Klass policy statement). [12]
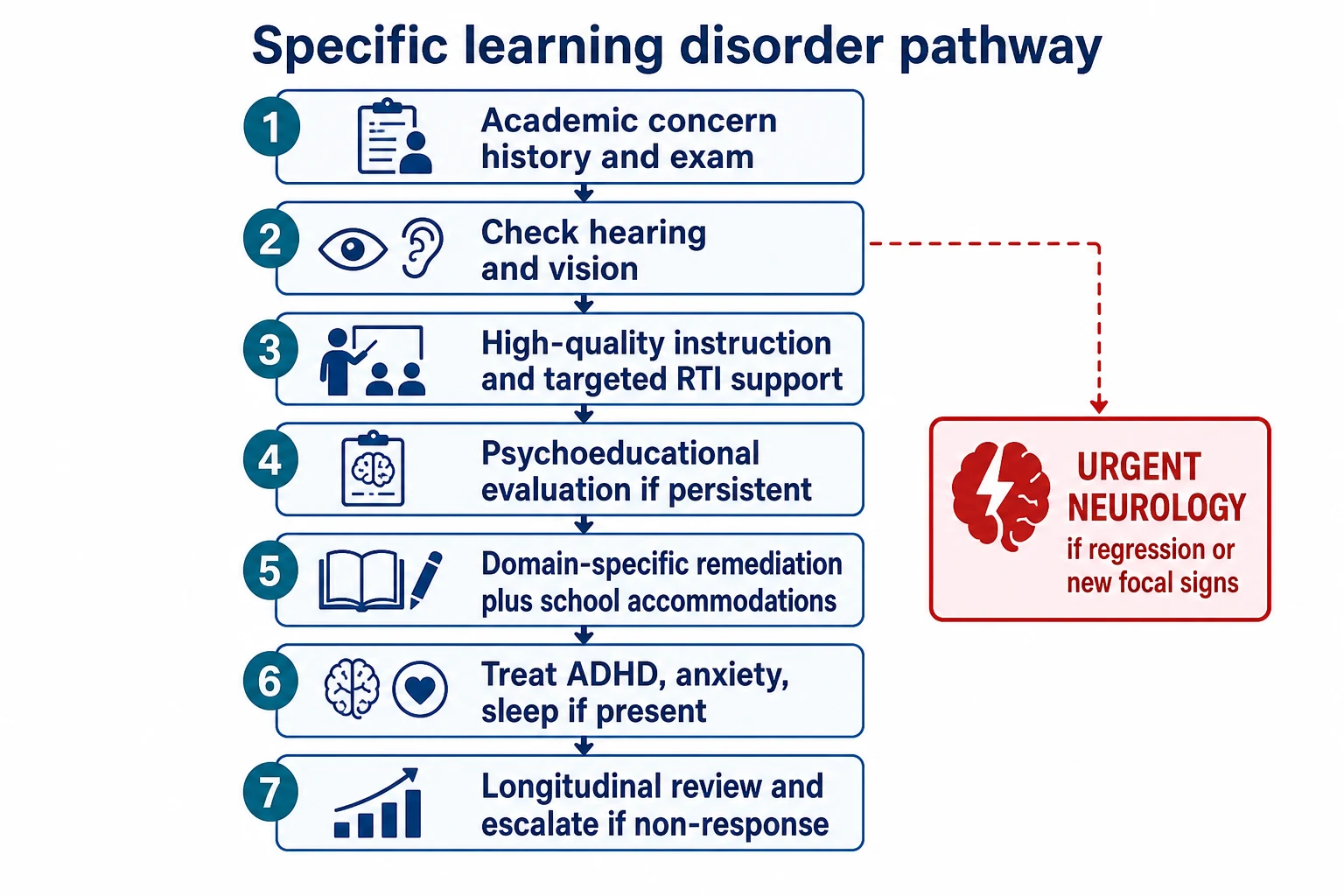
Read the figure like this: waiting passively for a 12-month psychology waitlist without interim teaching is a system failure, not evidence-based patience. [7] [17]
Specific Subtypes & Scenarios
Classic dyslexia in early primary school
Phonological weakness, slow decoding, better listening comprehension. Start structured literacy immediately; arrange hearing/vision; plan formal assessment if response is incomplete. [3] [7]
Dyscalculia with preserved reading
Number-line and fact-retrieval collapse with intact word reading. Target number sense; avoid “more worksheets” alone. [10] [19]
Written-expression SLD
Oral stories rich; written output minimal; spelling and handwriting drain working memory. Separate OT graphomotor support from language-based spelling intervention. [6] [20]
SLD + ADHD
Assess both. Sequence: safety and classroom function, ADHD treatment when indicated, concurrent skill remediation, re-evaluate achievement. [5] [13]
Late-identified adolescent
Compensated reader facing exam volume. Offer access arrangements, intensive catch-up where still plastic, anxiety care, and honest career/exam counselling. [3]
Multilingual learner
Use professional interpreters for history. Distinguish limited instruction-language exposure from true cross-linguistic academic disability. Avoid English-only conclusions. [16]
Family seeking vision therapy
Acknowledge visual comfort needs. State the evidence: learning disabilities and dyslexia are not treated by eye exercises as primary therapy; comprehensive educational evaluation and teaching are required. [1] [2]
Dyslexia with developmental language disorder
Profile differs from pure dyslexia; speech-language therapy and literacy intervention both belong in the plan. [15]
Complications & Pitfalls
- Missing hearing or vision impairment. [1]
- Calling everything ADHD. [5]
- Diagnosing SLD after no real teaching opportunity. [3]
- Selling vision therapy as dyslexia treatment. [1] [2]
- Waiting for a large IQ–achievement gap before intervening. [7]
- Ignoring secondary anxiety and self-esteem injury.
- Culturally biased testing without interpreters. [16]
- Open-loop psychology referral with no school coordination. [17]
- Assuming a brand-name multi-sensory programme is automatically evidence-proof. [8]
- Diagnostic overshadowing in medical complexity.
Prognosis & Disposition
SLD is a lifelong cognitive tendency with highly modifiable skills. Early intensive instruction improves reading accuracy and fluency trajectories; delayed recognition costs self-concept and secondary mental health. [3] [7]
Disposition is usually mainstream school with targeted intervention and accommodations. Specialist developmental-behavioural or educational psychology follow-up is needed when diagnosis is complex, comorbidity is heavy, or progress stalls. Review after a defined intervention block using curriculum-based measures and, when needed, repeat standardised testing. [7] [17]
Adolescent transition needs exam access arrangements, self-advocacy skills, and vocational planning — not discharge with “try harder next year.” [11]
Special Populations
- Preschool / school entry: promote literacy and language; be cautious labelling full SLD before sustained formal instruction, but do not withhold early help for clear risk. [9] [12] [14]
- Indigenous and migrant families: culturally safe assessment, interpreters, and distrust of systems that previously dismissed concerns. [16]
- Out-of-home care: assume incomplete records; rebuild school history. [17]
- Rural/remote: telehealth history is fine; testing access may need outreach advocacy.
- Twice-exceptional and chronic illness: protect enrichment and medical needs while remediating the weak domain. [11]
Evidence, Guidelines & Regional Differences
Vision and dyslexia. The AAP joint statement and Handler clinical report are the exam anchors: dyslexia is a language-based learning disability; vision problems can interfere with learning but do not cause dyslexia in the way vision-therapy marketing claims; eye exercises are not treatment for SLD. [1] [2]
Mechanisms and treatment principles. Peterson & Pennington’s Lancet review remains a high-yield synthesis for dyslexia cognition and management framing. [3]
Prevalence and sex differences. Moll and Arnett provide criteria-aware epidemiology rather than a single magic number. [4] [18]
Comorbidity science. DuPaul (LD–ADHD under DSM-5) and van Bergen (ADHD–dyslexia–dyscalculia co-occurrence/causality) stop the false choice between “only ADHD” and “only SLD.” [5] [13]
Intervention evidence. Torgesen supports intensive remediation; Fricke/Hulme support early language pathways into literacy; Stevens cautions against over-claiming for some branded OG packages. [7] [8] [9] [14]
Paediatric system roles. Educationally related services (AAP), care coordination (Turchi framework), and literacy promotion in primary care (Klass) define what the doctor does beyond writing “refer psychology.” [11] [12] [17]
Regional practice (principles)
Australia and Aotearoa New Zealand use school learning-support and disability-resourcing frameworks (including NCCD-style adjustments in Australia and learning support systems in Aotearoa). Paediatricians contribute medical reports and advocacy; education authorities own classroom resourcing rules. Name local pathways rather than importing US IEP paperwork wholesale. [17] [11]
Canada uses provincial special-education frameworks; principles of medical exclusion, comprehensive assessment and classroom accommodations still apply. [17] [11]
Exam Pearls
- SLD = unexpected academic underachievement, not low IQ. [3]
- Name the domain: reading, writing, maths. [4]
- Hearing and vision before labels. [1]
- Vision therapy is not dyslexia treatment. [1] [2]
- ADHD and SLD often co-occur — assess both. [5] [13]
- Start teaching early; do not wait for a perfect discrepancy. [7]
- Structured literacy beats vague “reading practice.” [3] [7]
- Brand names ≠ automatic evidence. [8]
- Girls may present late with anxiety. [18]
- Close the school–health loop. [17]
References
- [1]Handler SM Learning disabilities, dyslexia, and vision. Pediatrics, 2011.PMID 21357342
- [2]American Academy of Pediatrics, Section on Ophthalmology, Council on Children with Disabilities Joint statement--Learning disabilities, dyslexia, and vision. Pediatrics, 2009.PMID 19651597
- [3]Peterson RL Developmental dyslexia. Lancet, 2012.PMID 22513218
- [4]Moll K Specific learning disorder: prevalence and gender differences. PLoS One, 2014.PMID 25072465
- [5]DuPaul GJ Comorbidity of LD and ADHD: implications of DSM-5 for assessment and treatment. Journal of learning disabilities, 2013.PMID 23144063
- [6]Berninger VW Evidence-based diagnosis and treatment for specific learning disabilities involving impairments in written and/or oral language. Journal of learning disabilities, 2011.PMID 21383108
- [7]Torgesen JK Intensive remedial instruction for children with severe reading disabilities: immediate and long-term outcomes from two instructional approaches. Journal of learning disabilities, 2001.PMID 15497271
- [8]Stevens EA Current State of the Evidence: Examining the Effects of Orton-Gillingham Reading Interventions for Students With or at Risk for Word-Level Reading Disabilities. Exceptional children, 2021.PMID 34629488
- [9]Fricke S The efficacy of early language intervention in mainstream school settings: a randomized controlled trial. Journal of child psychology and psychiatry, 2017.PMID 28524257
- [10]Butterworth B Dyscalculia: from brain to education. Science, 2011.PMID 21617068
- [11]American Academy of Pediatrics Council on Children With Disabilities Provision of educationally related services for children and adolescents with chronic diseases and disabling conditions. Pediatrics, 2007.PMID 17545394
- [12]Klass P Literacy Promotion: An Essential Component of Primary Care Pediatric Practice: Policy Statement. Pediatrics, 2024.PMID 39342414
- [13]van Bergen E Co-Occurrence and Causality Among ADHD, Dyslexia, and Dyscalculia. Psychological science, 2025.PMID 40098496
- [14]Hulme C The Nuffield Early Language Intervention (NELI) programme is associated with lasting improvements in language and reading. Journal of child psychology and psychiatry, 2025.PMID 40074549
- [15]Snowling MJ Dyslexia with and without developmental language disorder: Profile analysis. Annals of dyslexia, 2026.PMID 41774411
- [16]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [17]Council on Children with Disabilities and Medical Home Implementation Project Advisory Committee Patient- and family-centered care coordination: a framework for integrating care for children and youth across multiple systems. Pediatrics, 2014.PMID 24777209
- [18]Arnett AB Explaining the sex difference in dyslexia. Journal of child psychology and psychiatry, 2017.PMID 28176347
- [19]Reigosa-Crespo V Basic numerical capacities and prevalence of developmental dyscalculia: the Havana Survey. Developmental psychology, 2012.PMID 21910533
- [20]Berninger V Relationships of Attention and Executive Functions to Oral Language, Reading, and Writing Skills and Systems in Middle Childhood and Early Adolescence. Journal of learning disabilities, 2017.PMID 26746315