Paeds · growth-development-and-behaviour
Speech and language delay
Also known as Late talker · Late language emergence · Developmental language disorder · Speech delay · Language delay · Expressive language delay
Fellowship guide to speech and language delay: speech versus language versus social communication, late talkers versus DLD (CATALISE), mandatory hearing pathway, red flags, differentials, concurrent SLP and early intervention, equity and exam defence across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A parent says, “He is almost two and only says mama and ball.” Your job is not to guess whether he will “grow out of it” from the doorway. Your job is to define the problem, protect hearing and safety, and start a pathway that can still use early plasticity. [1] [2]
Speech is the motor and sound system: articulation, phonology, voice and fluency. Language is the code: understanding words and grammar (receptive) and producing words and sentences (expressive). Communication is broader and includes gesture, pointing and social use. A child can have clear speech with empty language, or rich language that is hard to understand because speech sounds are disordered. [1] [3]
Primary-care reviews treat speech-language delay as a common reason for concern in early childhood and emphasise structured evaluation rather than reassurance alone. [1] [2]
Classification
Start with what you can observe and what the parent can describe, then name the working class. Do not open with abstract taxonomy for its own sake — open with the child in front of you. [1] [3]
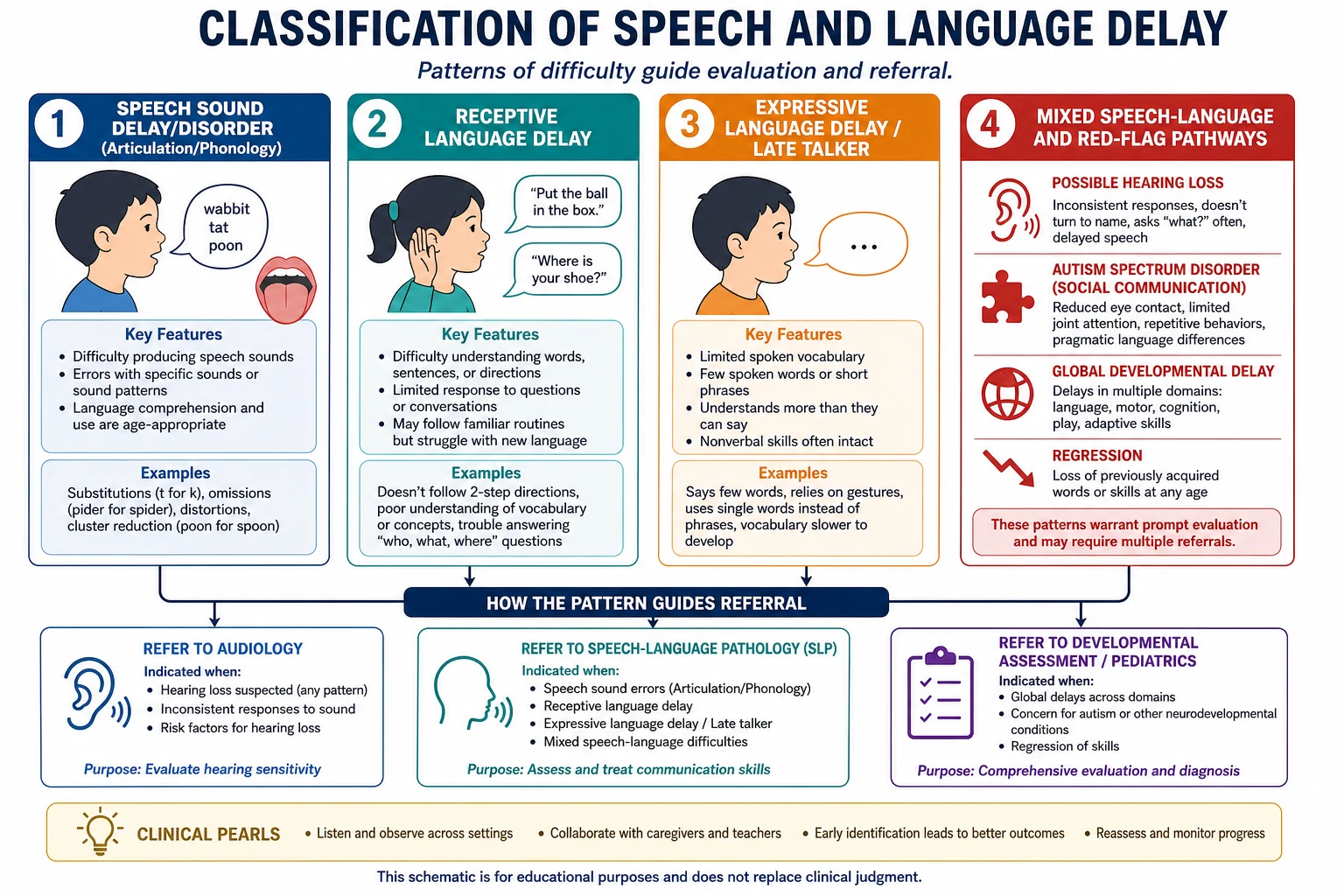
Late language emergence versus DLD
Late language emergence (often called late talking) is a toddler-stage description: spoken language is behind age expectations while other domains may look typical. Some children catch up; some do not. You cannot reliably pick winners in the room with a single visit, so you monitor and support rather than gamble. [1] [2] [3]
Developmental language disorder (DLD) is the CATALISE consensus term for persistent language difficulty that affects everyday function and is not better explained as a secondary feature of another condition in the way older labels implied. CATALISE moved the field away from inconsistent “specific language impairment” usage toward clearer identification language. [4] [5] [6]
Epidemiology & Risk Factors
Speech and language concerns are common enough that every general paediatrician must own the pathway. Exact prevalence varies by definition, age band and tool; do not invent a single global percentage. What matters clinically is who is missed: children in poverty, language-discordant families, incomplete medical homes, and out-of-home care. [1] [2] [14] [15]
Risk patterns repeatedly emphasised in primary-care frameworks include family history of language or learning problems, male sex, prematurity and ongoing middle-ear disease — each is a prompt for lower threshold action, not a diagnosis. [1] [2]
Toxic stress and limited contingent caregiving reshape developmental opportunity; language is one of the first skills to show the cost. Relational health and play are not soft extras — they are part of the developmental environment you influence. [15] [16] [17]
USPSTF statements (2015 and the 2024 update) conclude that evidence is insufficient to recommend for or against routine use of formal speech-language screening instruments in asymptomatic young children. That is not permission to ignore caregiver concern, failed surveillance items or functional delay. [9] [10]
Pathophysiology
Think of a cascade you can explain in one breath: hear → map meaning → plan words → move the mouth. Break any step and the child looks “quiet.” [1] [3]
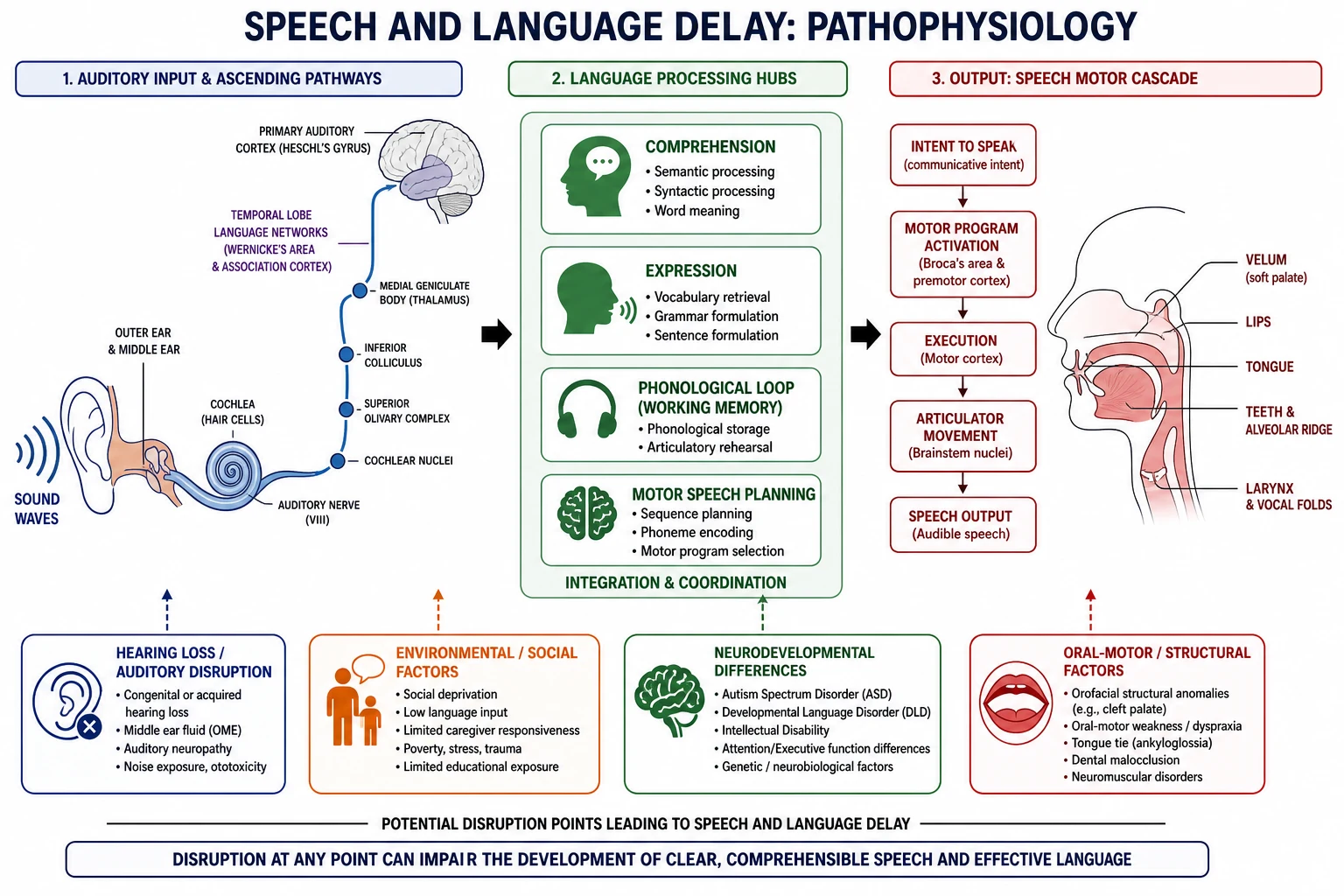
Hearing loss — permanent or fluctuating conductive loss from middle-ear disease — starves the language system of clear input. Parents may still say “he hears the TV” because loud environmental sound is not the same as clear speech-frequency hearing. [1] [2]
Language learning also depends on contingent, responsive talk and joint attention. Responsive linguistic input associates with later language performance in slow-to-talk toddlers, which is why parent-mediated strategies matter even while specialist services are pending. [18] [17]
Social-communication differences change how language is used for sharing attention and conversation, which is why autism pathways are not “just more speech therapy.” Structural or motor speech problems change sound production even when language networks are intact. [3] [11]
Clinical Presentation
The toddler who is “not talking yet”
Classic presentation: 18–30 months, limited vocabulary, parents comparing with peers or siblings. Ask what the child understands, what gestures exist, whether pointing and joint attention are present, and whether speech is absent or present but unclear. [1] [2]
The child who “does not listen”
This may be receptive language delay, hearing loss, attention difficulty, or oppositional behaviour secondary to not understanding. Do not diagnose behaviour first. [1] [3]
The preschooler others cannot understand
Speech sound disorder can devastate social confidence even when the child has ideas. Intelligibility to strangers matters more than perfect phonetic labels in the general clinic. [1] [3]
The school-age child with “behaviour” or literacy failure
Persistent language disorder often resurfaces as reading, writing, following classroom instructions and friendship strain. History of being a late talker is a clue, not a closed chapter. [3] [4]
Atypical and high-risk presentations
- Quiet “good” infant with little babble and limited social engagement. [8]
- Word loss after previously clear vocabulary — treat as regression until proven otherwise. [7]
- Medical-complexity child whose communication needs are overshadowed by devices and appointments. [13]
- Language-discordant family where the child’s skills in the home language were never elicited. [14]
Differential Diagnosis
Build the differential from discriminators, not a memorised list. [1] [3]
Other traps: over-attributing delay to bilingualism; blaming tongue-tie for true language delay; mistaking neglect-related understimulation for “laziness”; and missing safeguarding when language delay is one face of chronic adversity. [1] [14] [15]
Clinical & Bedside Assessment
History that changes decisions
Ask age of first concerns; babble onset; first words; current word approximations; two-word combinations; who understands the child; ability to follow one- and two-step instructions; gesture and pointing; play; regression; ear infections; newborn hearing result; languages spoken at home and hours of each; family history of language, literacy or autism; and school or childcare reports. [1] [2] [3]
Use professional interpreters for history and counselling when English is limited — family interpreters hide symptoms and distort developmental detail. [14]
Examination and observation
Watch how the child shares attention, requests, protests and plays. Look at ear examination, oral cavity, growth, neurology and dysmorphic clues without turning the visit into a genetics lecture. Evidence-informed milestone surveillance content (Zubler and the Lipkin identification framework) supports what you ask and observe at key ages; it does not replace clinical judgement. [7] [8]
HEAR-TALK
Red flags that end “wait and see”
Primary-care frameworks highlight concern-level markers such as limited babbling by late infancy, absence of meaningful words in the mid-second year, absence of two-word combinations by two years, and any loss of skills. Treat these as action thresholds, not as a licence to invent exact proprietary cut-offs beyond the cited teaching sources. [1] [2] [8]
Investigations
Always consider
Formal audiologic assessment for children with speech or language delay or concern — do not rely on informal office noise-making. Middle-ear assessment and ENT referral follow local findings. [1] [2] [3]
Often concurrent
Speech-language pathology evaluation; developmental screening or surveillance documentation at key ages; autism-specific screening when social-communication concerns exist (for example M-CHAT-R/F two-stage principles at toddler ages). [7] [11] [12]
Selective
Broader developmental assessment when more than language is affected; genetics or metabolic work-up only when history/exam or global pattern justifies them (owned in global delay leaves); neuroimaging is not routine for isolated speech-language delay without neurological red flags. [3] [7]
Low value
Repeating parent questionnaires without action; serial “reassurance visits” without audiology; MRI “just in case”; diagnosing from a single incomplete screen in a language the family does not use. [7] [9] [14]
Management — Resuscitation
This section is short on purpose. Most speech-language delay is outpatient work. The acute conversions are medical threats and safeguarding, not community SLP booking alone. [7] [15]
- Regression / encephalopathy / seizures — emergency assessment, not community SLP alone. [7]
- Safeguarding or severe neglect — protective pathway runs in parallel. [15]
- Acute ENT/airway disease — treat the medical threat first. [1]
- Caregiver crisis — stabilise safety and supports; still document the developmental plan. [16]
There is no resuscitation drug for speech delay. Do not invent stimulant, benzodiazepine or “tonics for talking.” [1] [2]
Management — Definitive & Stepwise
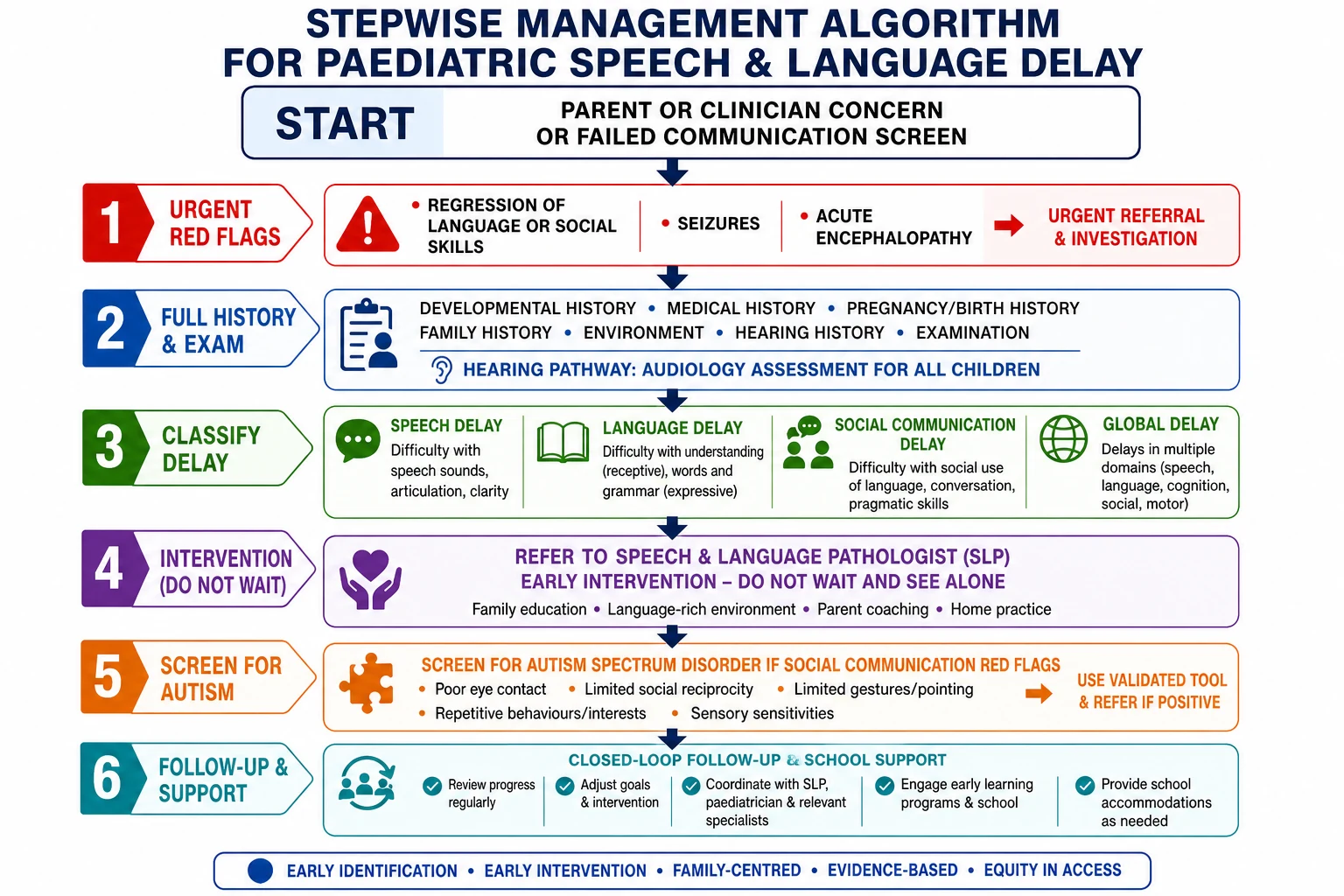
Step 1 — Name the concern and stop pure wait-and-see when action criteria are met
If caregiver concern is high, functional impact is clear, or age-based red flags are present, start evaluation and referral. Reassurance without a plan is not a plan. [1] [2] [7]
Step 2 — Hearing pathway
Book age-appropriate audiology. Treat middle-ear disease on its merits. Explain that hearing is checked because clear input builds language — not because you “think they are deaf” as a pejorative. [1] [2]
Step 3 — Concurrent SLP and early supports
Refer to speech-language pathology and to early childhood intervention services according to age and local systems. Parallel referral beats sequential waiting. [1] [3] [13]
Step 4 — Family language strategies while waiting
Coach contingent talk, follow-the-child’s-focus, reduce purely passive screen time in favour of interactive play, and celebrate gesture as communication. Responsive input is associated with better language performance in slow-to-talk toddlers. [17] [18]
Step 5 — Branching pathways
- Social-communication red flags → autism identification pathway (screens such as M-CHAT-R/F principles; specialist evaluation). [11] [12]
- Multi-domain delay → global developmental evaluation leaf. [7]
- Confirmed hearing loss → audiology/ENT/early hearing intervention systems (cross-link hearing leaf). [1]
Step 6 — Close the loop
Document tool/results, referrals, interim strategies and a review date. Care coordination is clinical work, not admin optional. [13]
Same-day clinic actions
Clarify speech vs language vs social pattern with examples from today
Screen for regression and other red flags
Order or book formal hearing assessment
Refer SLP ± early intervention concurrently
Add autism or global pathway if indicated
Teach 2–3 parent language strategies with teach-back
Book timed review and name the safety-net for worsening
Specific Subtypes & Scenarios
Late talker with good comprehension and social skills
Still confirm hearing, offer language-enrichment coaching, refer SLP when criteria or family preference/functional need support it, and review trajectory rather than discharging to hope. [1] [2] [18]
Receptive-expressive delay
Higher stakes. Prioritise hearing, SLP, and search for broader developmental issues. School readiness planning starts early. [3] [4]
Speech sound disorder with poor intelligibility
SLP is central. Hearing still matters. Avoid promising that frenotomy alone will fix language. [1] [3]
Language delay plus autism red flags
Do not wait for perfect speech therapy response before autism evaluation. Use validated autism screening pathways where age-appropriate and refer for comprehensive assessment. [11] [12] [7]
Bilingual households
Bilingualism is not a disease. Assess opportunity in each language, use interpreters, and avoid advising families to abandon the home language as a “treatment.” True disorder affects learning of language systems, not merely the second language. [1] [14]
Fluctuating hearing from middle-ear disease
Treat ears, track language, and do not assume tubes equal full language catch-up without support. [1] [2]
School-age residual language disorder
Partner with school learning supports; re-engage SLP; screen literacy and social participation; watch for secondary behaviour and mental health load. [3] [4]
Foster/kinship care and incomplete history
Assume missing newborn hearing and prior screens until proven; lower threshold for full evaluation; coordinate across carers. [13]
Complications & Pitfalls
Secondary complications include social withdrawal, behavioural escalation when the child cannot express needs, literacy failure, and family stress. Early relational support and clear plans reduce harm even before a definitive label exists. [15] [16]
Prognosis & Disposition
Prognosis depends on pattern (isolated expressive vs receptive/mixed), hearing status, co-occurring developmental conditions, language environment and access to intervention. Some late talkers improve substantially; persistent DLD needs long-view educational planning. Do not promise catch-up percentages that your cited sources do not defend in the room. [1] [3] [4]
Disposition tiers — choose intensity by pattern and risk, then name the review date. [1] [7]
- Community SLP + audiology + timed paediatric review for isolated concerns with supports in place. [1]
- Multidisciplinary developmental services when autism, global delay or complex needs emerge. [7] [13]
- Education supports as the child approaches school. [3]
Safety-net: any regression, new hearing concern, or major functional drop triggers earlier review. [7]
Special Populations
Preterm / NICU graduates — higher developmental surveillance intensity; language follow-up is part of the package. [7]
Indigenous children — culturally safe assessment, avoid deficit framing, partner with community-controlled services where available, and do not mistake language difference for disorder. [16]
Migrant and refugee families — professional interpreters; trauma-informed care; verify prior hearing screens. [14] [15]
Medical complexity — communication access is a safety issue (pain, fear, consent). Coordinate with existing teams; consider AAC pathways when speech is not enough (cross-link AAC leaf). [13]
Rural/remote — telehealth SLP, outreach audiology, and interim parent coaching reduce geography as destiny. [13]
Evidence, Guidelines & Regional Differences
Use local child health blue books / developmental surveillance contacts, state early childhood early intervention entry points, and audiology pathways. Name your hospital’s concurrent referral process in exams when asked for “what you would do Monday.” Operational ages and forms are jurisdiction-specific — do not invent them. [7]
Canada and other systems vary by province/territory. The clinical constants travel: hearing, pattern, concurrent therapy, closed loops, equity. [13]
Controversies you should defend calmly: universal tool screening versus surveillance-plus-concern; how long to watch a mild late talker; and how aggressively to investigate isolated delay. Lead with function, hearing and red flags rather than ideology. [9] [1] [7]
Exam Pearls
References
- [1]Rupert J Speech and Language Delay in Children. Am Fam Physician, 2023.PMID 37590860
- [2]McLaughlin MR Speech and language delay in children. Am Fam Physician, 2011.PMID 21568252
- [3]Feldman HM Evaluation and management of language and speech disorders in preschool children. Pediatr Rev, 2005.PMID 15805236
- [4]Bishop DVM Phase 2 of CATALISE: a multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology. J Child Psychol Psychiatry, 2017.PMID 28369935
- [5]Bishop DV CATALISE: A Multinational and Multidisciplinary Delphi Consensus Study. Identifying Language Impairments in Children. PLoS One, 2016.PMID 27392128
- [6]Bishop DVM Why is it so hard to reach agreement on terminology? The case of developmental language disorder (DLD). Int J Lang Commun Disord, 2017.PMID 28714100
- [7]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [8]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439
- [9]US Preventive Services Task Force Screening for Speech and Language Delay and Disorders in Children: US Preventive Services Task Force Recommendation Statement. JAMA, 2024.PMID 38261037
- [10]Siu AL Screening for Speech and Language Delay and Disorders in Children Aged 5 Years or Younger: US Preventive Services Task Force Recommendation Statement. Pediatrics, 2015.PMID 26152670
- [11]Robins DL Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics, 2014.PMID 24366990
- [12]Wieckowski AT Sensitivity and Specificity of the Modified Checklist for Autism in Toddlers (Original and Revised): A Systematic Review and Meta-analysis. JAMA Pediatr, 2023.PMID 36804771
- [13]Council on Children with Disabilities and Medical Home Implementation Project Advisory Committee Patient- and family-centered care coordination: a framework for integrating care for children and youth across multiple systems. Pediatrics, 2014.PMID 24777209
- [14]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI Evid Synth, 2020.PMID 32813387
- [15]Garner AS Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics, 2012.PMID 22201148
- [16]Garner A Preventing Childhood Toxic Stress: Partnering With Families and Communities to Promote Relational Health. Pediatrics, 2021.PMID 34312296
- [17]Yogman M The Power of Play: A Pediatric Role in Enhancing Development in Young Children. Pediatrics, 2018.PMID 30126932
- [18]Levickis P Associations between maternal responsive linguistic input and child language performance at age 4 in a community-based sample of slow-to-talk toddlers. Child Care Health Dev, 2018.PMID 30043426