Paeds · growth-development-and-behaviour
Temper tantrums, aggression and emotional dysregulation
Also known as Toddler tantrums · Childhood aggression · Emotional dysregulation in children · Irritability and temper loss · Disruptive behaviour preschool
Fellowship guide to temper tantrums, aggression and emotional dysregulation: developmental norms versus impairing behaviour, ABC assessment, medical and safeguarding differentials, first-line behavioural parenting, no corporal punishment, specialist escalation and exam defence.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A parent says, “He has tantrums all day. He hits. I am exhausted.” The child looks fine in the waiting room. Your first task is not a diagnosis code. Your first task is to decide whether this is expected temper loss, impairing emotional dysregulation, or aggression that needs a safety plan today. [1] [4]
A temper tantrum is a time-limited outburst of frustration or anger. You may see crying, screaming, thrashing, dropping to the floor, or a short loss of behavioural control. In toddlers, this often appears when desire and autonomy outrun language and self-regulation. [4]
Emotional dysregulation means the child struggles to modulate how strong feelings get, how long they last, and how quickly they recover, relative to age and context. Aggression is behaviour intended to harm or threaten harm to people, animals or property. Reactive (“hot”) aggression is different from proactive (“instrumental”) aggression. [11] [12]
More than 10% of young children experience clinically significant mental health problems. The medical home is often the first reliable contact, so general paediatricians lead early recognition and parenting support rather than waiting for a specialist letter. [1]
Deep technique for functional analysis lives on the linked behavioural assessment page. ODD-focused programme detail lives on the defiance management page. This leaf owns the clinical spine for tantrums, aggression and dysregulation. [15]
Classification
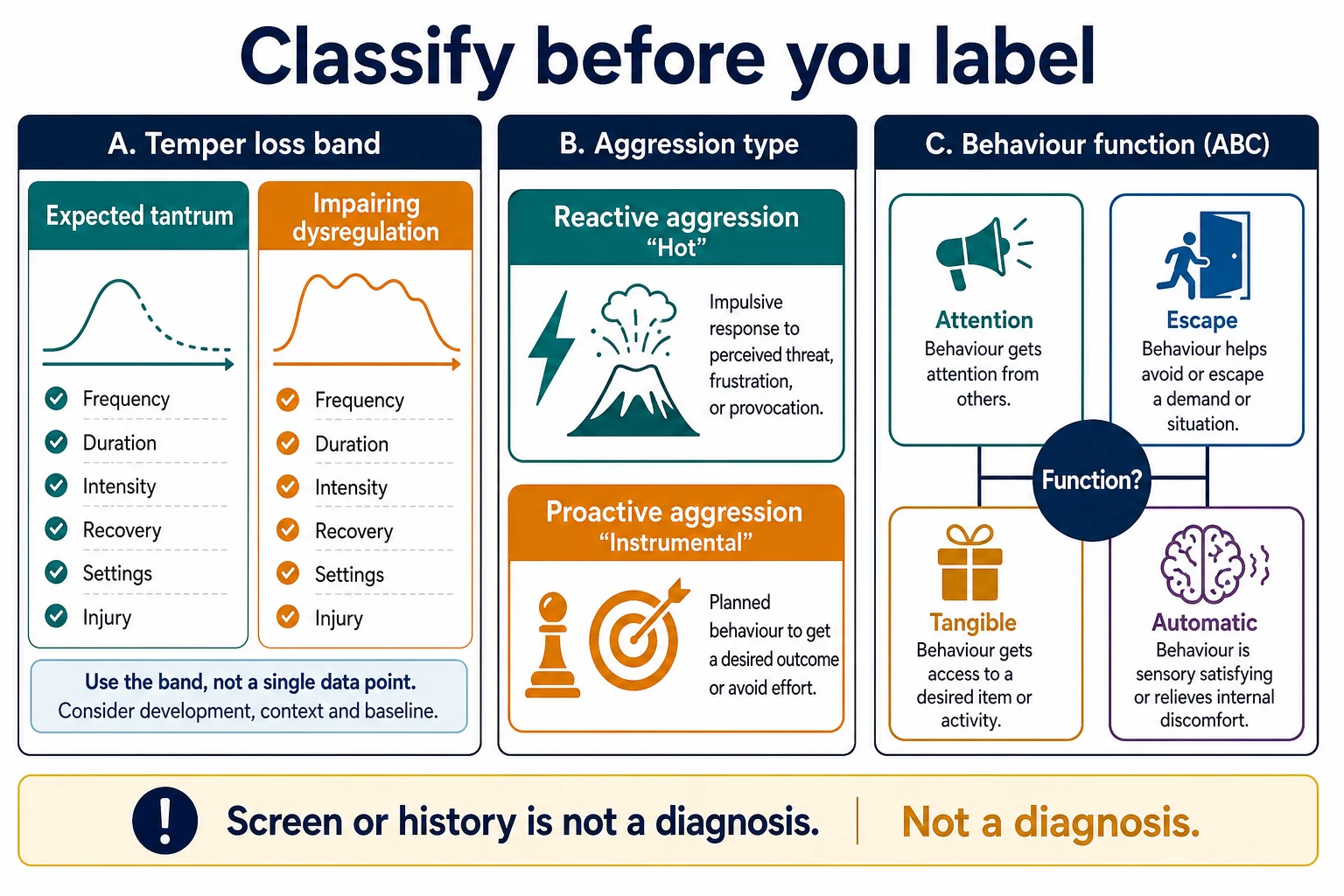
Classify four things before you reach for a label: severity band, aggression type, function, and context. [4] [15]
Severity band
| Band | What you hear and see | Typical first move |
|---|---|---|
| Expected tantrums | Brief, recoverable, often single-setting, no injury, development otherwise on track | Psychoeducation, routines, positive parenting |
| Impairing dysregulation | Frequent, prolonged, hard recovery, multi-setting, high caregiver distress | Structured assessment, parent training, treat drivers |
| High-risk aggression | Injury, self-injury, weapons/elopement risk, caregiver cannot keep safe | Safety plan now; urgent pathway if needed |
Aggression and function
Reactive aggression follows frustration, threat or overload. Proactive aggression is used to obtain a goal. Function often falls into attention, escape from demands, access to tangibles, or automatic/sensory reinforcement. You do not need a full specialist functional analysis every visit, but you do need ABC thinking: antecedent, behaviour, consequence. [15]
Expected tantrum versus impairing pattern
- Short duration with recovery
- Often linked to fatigue or limit-setting
- Mostly one setting
- No serious injury
- Development largely on track
- High frequency or long duration
- Slow recovery or residual anger
- Home plus childcare/school
- Property damage or injury risk
- Often co-occurring sleep, language or ADHD/ASD traits
Epidemiology & Risk Factors
Tantrums are common in early childhood. Population and clinic series have long documented high rates of temper outbursts in toddlers and preschoolers, with major caregiver impact when episodes are frequent. [1]
Risk of impairing behaviour rises with developmental delay, language impairment, ADHD traits, autism, chronic sleep debt, pain, family adversity and harsh or inconsistent discipline. Caregiver mental health and social supports shape both presentation and treatment capacity. [1] [3]
Children in out-of-home care, families living with violence, and families facing poverty are systematically more likely to present late, incomplete, or blamed. Equity is part of the clinical plan, not an afterthought. [1]
Pathophysiology
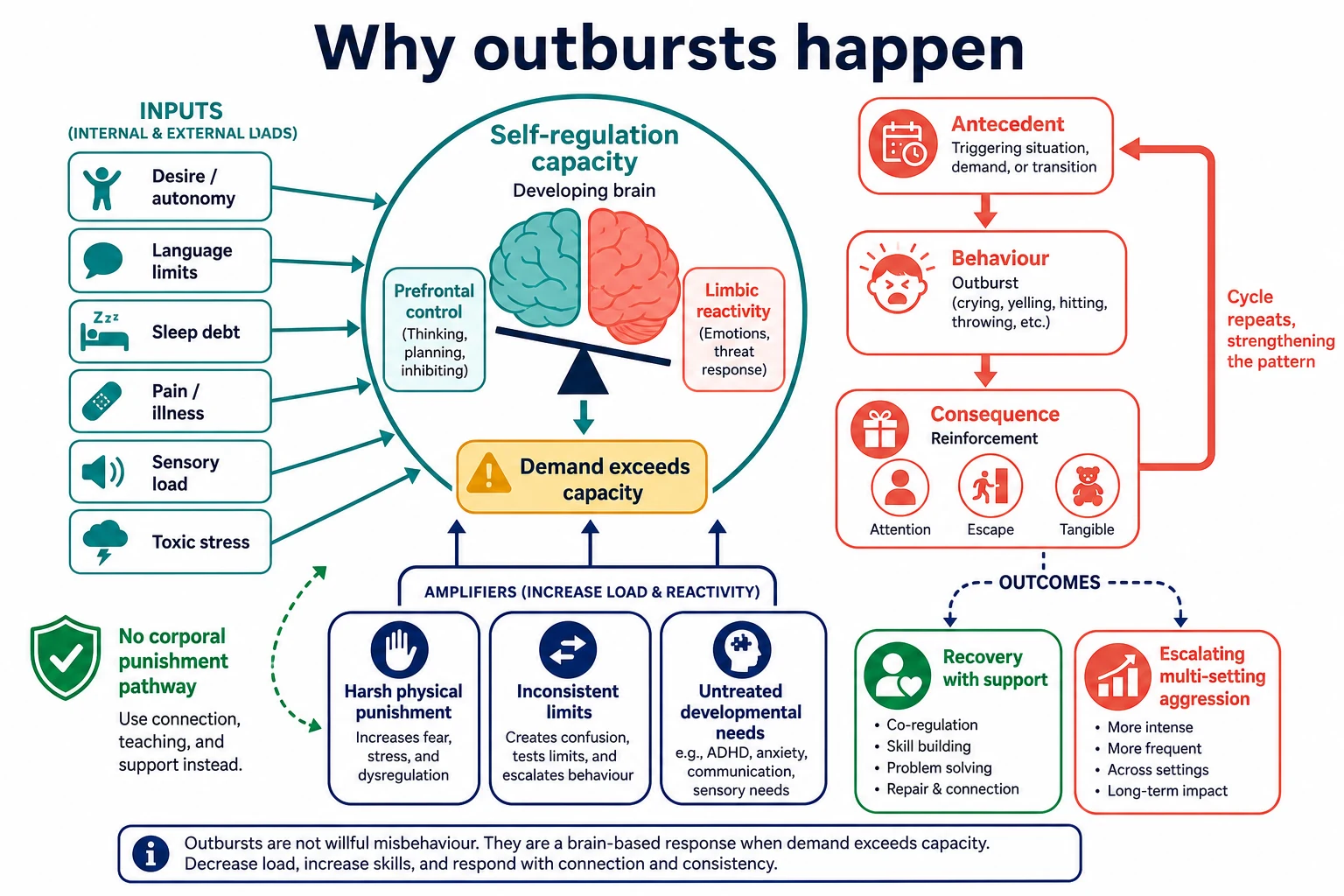
Picture a toddler who wants a biscuit now. Language is limited. Inhibitory control is immature. The limbic response is fast. When demand exceeds regulation capacity, the system tips into crying, thrashing or hitting. That is developmental biology, not moral failure. [4] [13]
Irritability research frames a spectrum from normative temper loss to impairing chronic irritability. Translational models link heightened threat reactivity and weaker regulatory control with clinical irritability phenotypes. [5] [13] [14]
Behaviour is also learned. If a tantrum reliably produces attention, escape from a demand, or a preferred item, the behaviour is reinforced. Planned ignoring of safe attention-seeking outbursts and consistent reinforcement of calm requests change the contingency. [15]
Sleep debt, pain, sensory overload and toxic stress lower the threshold for the next outburst. Harsh physical punishment is associated with worse child outcomes and does not teach regulation. [1] [3]
Clinical Presentation
Parents may describe “meltdowns over nothing,” hitting siblings, biting at childcare, or evening chaos after daycare. Ask what “all day” means in numbers: times per day, minutes per episode, recovery time, injuries, and which settings. [4]
In clinic the child may be charming. That does not disprove home reports. Multi-informant history matters. A child who is only dysregulated with one caregiver still needs help, but multi-setting impairment raises the stakes. [1] [5]
Atypical presentations include aggression as communication in language delay or intellectual disability; sensory-triggered meltdowns in autism; post-illness irritability; and hyperarousal after trauma. Adolescents may present with chronic angry mood rather than floor-dropping toddler tantrums. [11] [14]
Differential Diagnosis
Build the differential in layers: developmental expectation, neurodevelopmental conditions, medical mimics, mental health phenotypes, and safeguarding. [1]
| Pattern | Favours | Against / distinguish |
|---|---|---|
| Brief limit-linked toddler tantrums, good recovery | Expected temper loss | Multi-setting injury, regression |
| Inattention, impulsivity, emotional lability across settings | ADHD pathway | Purely situational with one adult only |
| Social communication differences, sensory overload meltdowns | Autism-related dysregulation | Purely instrumental aggression without autism signs |
| Frustration with limited words, improves with communication support | Language disorder pathway | Fluent language with planned proactive aggression |
| Chronic severe irritability with frequent temper outbursts | Irritability/DMDD-range thinking in older children | Toddler-only normative tantrums; do not force adult mood labels |
| Night waking, short sleep, snoring | Sleep-driven behaviour | Daytime-only pattern with excellent sleep |
| Fearful hypervigilance, startle, inconsistent stories | Trauma / adversity | Isolated supermarket tantrum in otherwise safe home |
| Unexplained injuries, coercive control, child terrified of caregiver | Safeguarding first | Pure skill-deficit tantrums with warm caregiving |
Medical contributors to keep active: pain, constipation, otitis, dental disease, iron deficiency risk factors, hearing or vision problems, medication side-effects, and rare neurologic events when red flags exist. Do not order shotgun panels for ordinary tantrums. [1]
Clinical & Bedside Assessment
Lead with safety. Then take a structured behaviour history you can defend in a viva. [1]
Bedside sequence
Safety and medical convert?
Injury risk, self-injury, weapons, encephalopathy, seizure, safeguarding.
Pattern metrics
Frequency, duration, intensity, recovery, settings, injuries.
ABC map
What happens before, during and after — attention, escape, tangible, automatic.
Development and communication
Language, social communication, play, school/childcare function.
Drivers and context
Sleep, pain, routines, screens, caregiver strategies, adversity.
Plan
Parenting strategies, treat drivers, refer, safety-net, close the loop.
Observe parent–child interaction without shaming. Note whether the adult narrates, threatens, hits, over-explains, or collapses. Ask directly and calmly about smacking or other physical punishment. Many caregivers will only disclose if you ask without contempt. [2] [3]
Assess caregiver mental health and capacity. A parent with untreated depression or housing crisis cannot run a perfect token chart tonight. Match the plan to real life. [1]
Investigations
For typical age-limited tantrums with normal examination and no red flags, laboratory tests are usually unnecessary. Your investigation is the history, developmental screen of concern, and multi-informant reports. [1]
Investigate when the story points somewhere. [1] Hearing and vision pathways matter when communication-linked aggression or speech delay is present. Use targeted medical review for pain, constipation, sleep-disordered breathing symptoms, or nutritional risk — not a universal iron panel for every tantrum. Standardised early behavioural/emotional screening tools help in primary care when programme design supports them (Gleason framework). Arrange developmental evaluation when global delay, autism signs, or multi-domain impairment appears. Convert to urgent medical workup for encephalopathy, seizure concern, trauma, or unexplained injury.
Neuroimaging and EEG are not first-line for behavioural outbursts without neurologic red flags. Do not invent proprietary questionnaire cut-offs; use local tool manuals. [1]
Management — Resuscitation
“Resuscitation” in behaviour presentations means immediate safety and medical conversion, not a drug bolus for crying. [1]
In the room: reduce stimulation, protect other children, avoid a public power struggle, and separate if needed. Document injuries. Create a same-day safety plan: supervision, remove unsafe objects, who to call, where to go. Use local crisis mental-health and child-protection pathways when thresholds are met — names and phone trees are jurisdiction-specific. [1]
Management — Definitive & Stepwise
Step 1 — Validate and reframe
Say the quiet part out loud: this is hard, the parent is not failing as a human, and the child is not “bad.” Behaviour is a skill problem plus context. Shame blocks learning. [1] [2]
Step 2 — Psychoeducation on norms and worry signs
Explain the developmental peak of temper loss and the dimensional spectrum of irritability. Teach when to return sooner: rising injury risk, multi-setting escalation, regression, or caregiver crisis. [4] [5]
Step 3 — First-line behavioural parenting
Group behavioural and cognitive-behavioural parenting programmes improve early-onset conduct problems in children aged 3–12 years. Parent–Child Interaction Therapy (PCIT) has meta-analytic and randomised evidence for young children’s behaviour problems. Telehealth and internet-delivered adaptations improve access when travel or waitlists block care. [6] [7] [8] [9] [10]
Core strategies to coach in clinic while waiting for a programme include predictable routines and clear short instructions; labelled praise for calm and compliant behaviour; planned ignoring of safe attention-seeking tantrums; consistent calm consequences with brief time-out or time-in without humiliation; special play time that rebuilds positive connection; and adult self-regulation, because the calmer adult is the intervention. [2] [6]
Step 4 — Explicitly reject corporal punishment
The AAP effective-discipline policy centres positive strategies and does not support corporal punishment. Meta-analytic evidence links spanking with detrimental child outcomes. If a caregiver asks for “stronger discipline,” teach stronger consistency and connection, not harder hits. [2] [3]
Step 5 — Treat modifiable drivers
Fix the amplifiers: sleep opportunity and sleep disorders, pain, constipation, sensory load, language access, literacy of instructions, and school/childcare fit. A behaviour plan fails if the child is exhausted or in pain. [1]
Step 6 — Coordinate supports and escalate
Refer early intervention, speech pathology, occupational therapy, psychology, developmental-behavioural paediatrics or CAMHS/mental health when impairment is multi-setting, severe, or diagnostically complex. For autism-related irritability, aggression or self-injury, pharmacological options exist in specialist literature and are not a general-paediatric first step for ordinary tantrums. [1] [16]
Close the loop: name the owner, date, interim plan and safety-net. Do not “refer and forget.” [1]

Specific Subtypes & Scenarios
Typical 2-year-old limit-testing. Short tantrums at “no,” normal development, warm caregiving. Educate, coach praise and planned ignoring, review sleep, safety-net. [2] [4]
Preschool multi-setting destruction. Daily long outbursts at home and childcare with property damage. Full ABC map, parent-training referral, childcare behaviour plan, developmental screen, closer follow-up. [1] [6]
Language delay with hitting. Aggression often communicates “I cannot say it.” Parallel speech/language pathway and visual supports, not punishment alone. [1]
Autism-related meltdown. Reduce sensory load, support communication, avoid framing every meltdown as wilful defiance; use specialist pathways for severe irritability. [16]
ADHD emotional impulsivity. Behaviour strategies plus ADHD assessment pathway; do not treat only the tantrum. [11] [14]
Sleep-debt evenings. Protect sleep opportunity before escalating labels. [1]
Trauma-exposed child. Safety and trauma-informed care first; aggression may be hyperarousal, not “naughty.” [1]
Rural access barrier. Use telehealth parent-training evidence and local hybrid models rather than passive waiting. [9] [10]
Caregiver using smacking. Address directly with AAP-aligned counselling and safer alternatives. [2] [3]
Complications & Pitfalls
- Over-pathologising normal toddler tantrums.
- Under-reacting to multi-setting injury risk.
- Starting medication for typical preschool tantrums.
- Recommending corporal punishment.
- Ignoring sleep, pain, hearing, language and safeguarding.
- Shame-based counselling that drives families away.
- Treating only the child while reinforcement patterns stay the same.
- Open-loop specialist referral with no interim plan.
- Diagnostic overshadowing in disability.
- Forcing adult mood-disorder labels onto early childhood temper loss.
Prognosis & Disposition
Most expected tantrums improve with maturation and consistent supportive parenting. Persistent high irritability and multi-setting aggression mark higher risk for later externalising and mood problems, which is why early parenting intervention matters. [5] [6] [12]
Disposition after typical tantrums: education, written strategies, safety-net, routine review. [1]
Disposition after impairing behaviour: parent-training pathway, treat drivers, developmental workup as indicated, medical-home interim coaching, timed follow-up. [1] [6]
Disposition after acute risk: safety plan, crisis/safeguarding pathway, same-day supports. [1]
Response markers: fewer episodes, shorter duration, faster recovery, fewer injuries, improved caregiver confidence, better childcare/school participation. [1] [6]
Special Populations
Toddlers need concrete language and routine coaching. School-age children need multi-informant school data. Adolescents need privacy, mood and risk assessment, and different language than “tantrum.” [11] [14]
Children with developmental disability may use aggression as communication. Autistic children need sensory and communication supports; specialist irritability pathways are separate from ordinary tantrum care. Indigenous, migrant and refugee families need culturally safe, non-stigmatising counselling and professional interpreters. Out-of-home care and family-violence contexts change both risk and who must be in the safety plan. Rural families need telehealth-capable options. [1] [9] [10] [16]
Evidence, Guidelines & Regional Differences
Key evidence anchors for exam defence: [1] [2]
- Gleason 2016 AAP clinical report — early childhood emotional/behavioural problems; medical-home role; caution on early psychopharmacology. [1]
- Sege 2018 AAP — effective discipline; positive parenting; no corporal punishment. [2]
- Gershoff 2016 — spanking associated with detrimental outcomes in meta-analyses. [3]
- Wakschlag 2012/2015 — dimensional temper loss and early irritability spectrum. [4] [5]
- Furlong Cochrane 2012 — group parenting programmes for early-onset conduct problems. [6]
- PCIT evidence — meta-analysis and RCT support; telehealth adaptations. [7] [8] [9] [10]
- Irritability reviews — Stringaris, Vidal-Ribas, Brotman, Leibenluft. [11] [12] [13] [14]
- Iffland Cochrane 2023 — specialist pharmacologic options for ASD irritability/aggression/self-injury. [16]
Use positive parenting and non-physical discipline principles. Local programme names (for example state positive-parenting services, child health nurse pathways, CAMHS thresholds) vary by jurisdiction — name the principle and the local service, do not invent statute numbers. Child-protection reporting thresholds are state/territory specific. [2]
Controversies: how early to label irritability phenotypes; waitlist ethics when parent training is scarce; telehealth fidelity; and when, if ever, medication is appropriate outside specialist autism/irritability pathways. [1] [14] [16]
Exam Pearls
TANTRUMS
- Expected tantrums peak when desire outruns language and self-regulation. [4]
- Worry with multi-setting, prolonged, injurious or developmentally red-flag patterns. [5]
- First-line for many early externalising problems is behavioural parenting, not medicine. [1] [6]
- Never recommend smacking. [2] [3]
- Telehealth parent training has randomised evidence when access is limited. [9] [10]
- ASD irritability pharmacology is specialist territory. [16]
References
- [1]Gleason MM Addressing Early Childhood Emotional and Behavioral Problems. Pediatrics, 2016.PMID 27940734
- [2]Sege RD Effective Discipline to Raise Healthy Children. Pediatrics, 2018.PMID 30397164
- [3]Gershoff ET Spanking and child outcomes: Old controversies and new meta-analyses. J Fam Psychol, 2016.PMID 27055181
- [4]Wakschlag LS Defining the developmental parameters of temper loss in early childhood: implications for developmental psychopathology. J Child Psychol Psychiatry, 2012.PMID 22928674
- [5]Wakschlag LS Clinical Implications of a Dimensional Approach: The Normal:Abnormal Spectrum of Early Irritability. J Am Acad Child Adolesc Psychiatry, 2015.PMID 26210331
- [6]Furlong M Behavioural and cognitive-behavioural group-based parenting programmes for early-onset conduct problems in children aged 3 to 12 years. Cochrane Database Syst Rev, 2012.PMID 22336837
- [7]Valero-Aguayo L Meta-analysis of the Efficacy and Effectiveness of Parent Child Interaction Therapy (PCIT) for Child Behaviour Problems. Psicothema, 2021.PMID 34668468
- [8]Bjørseth Å Effectiveness of Parent-Child Interaction Therapy (PCIT) in the Treatment of Young Children's Behavior Problems. A Randomized Controlled Study. PLoS One, 2016.PMID 27622458
- [9]Comer JS Remotely delivering real-time parent training to the home: An initial randomized trial of Internet-delivered parent-child interaction therapy (I-PCIT). J Consult Clin Psychol, 2017.PMID 28650194
- [10]Bagner DM Telehealth Treatment of Behavior Problems in Young Children With Developmental Delay: A Randomized Clinical Trial. JAMA Pediatr, 2023.PMID 36622653
- [11]Stringaris A Irritability in children and adolescents: a challenge for DSM-5. Eur Child Adolesc Psychiatry, 2011.PMID 21298306
- [12]Vidal-Ribas P The Status of Irritability in Psychiatry: A Conceptual and Quantitative Review. J Am Acad Child Adolesc Psychiatry, 2016.PMID 27343883
- [13]Brotman MA Irritability in Youths: A Translational Model. Am J Psychiatry, 2017.PMID 28103715
- [14]Leibenluft E Irritability in Youths: A Critical Integrative Review. Am J Psychiatry, 2024.PMID 38419494
- [15]Hanley GP Functional analysis of problem behavior: a review. J Appl Behav Anal, 2003.PMID 12858983
- [16]Iffland M Pharmacological intervention for irritability, aggression, and self-injury in autism spectrum disorder (ASD). Cochrane Database Syst Rev, 2023.PMID 37811711