Paeds · haematology-oncology-and-transfusion
Anaemia: diagnostic approach
Also known as Pediatric anemia workup · MCV-based anaemia classification · Anaemia evaluation in children · Low haemoglobin diagnostic approach · Red cell indices interpretation
Fellowship MCV-based diagnostic approach to confirmed paediatric anaemia: age-specific haemoglobin thresholds, the microcytic or normocytic or macrocytic grid combined with reticulocyte kinetics and the peripheral film, directed second-line testing, and how to avoid the common traps of over-treating iron and missing marrow failure.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A low haemoglobin is a pattern, not a verdict. The child in front of you drank a litre of cow's milk a day, or just finished a viral illness, or carries thalassaemia trait silently, or has a marrow that has stopped making cells. Each story produces the same abnormal number but demands a different next step. This leaf owns the laboratory reasoning that converts that number into a mechanism, then into a directed investigation. [1] [2]
The bedside sign of pallor and the threat-first stabilisation of the sick child sit in a companion leaf; this page begins once the full blood count is in your hand. Cross-link the pallor page for recognition across skin tones and the disease-specific leaves for iron deficiency, haemolysis and macrocytic anaemia protocols. [1]
M.C.V. + R.E.T.I.C.
Overview & Definition
Anaemia is a laboratory definition. The World Health Organization sets age- and sex-specific haemoglobin cut-offs below which anaemia exists. For children aged six months to under five years the threshold is a haemoglobin below 110 g per litre; for children five to eleven years it is below 115 g per litre; for children twelve to fourteen years and for non-pregnant females aged fifteen years and older it is below 120 g per litre. Pregnancy and altitude lower and raise these bands respectively. [2]
A haemoglobin value alone tells you nothing about cause. The job of the diagnostic approach is to move from "the number is low" to "here is the mechanism", using red-cell size, marrow response and morphology. The same haemoglobin of 70 g per litre can mean dietary iron deficiency in a toddler, acute autoimmune haemolysis in a school-age child, or aplastic anaemia in an adolescent, and the next investigation differs for each. [1] [6]
Severity is graded against the same age bands. For a child under five years, haemoglobin of 100 to 109 g per litre is mild, 70 to 99 g per litre is moderate, and below 70 g per litre is severe. Severe anaemia is a medical urgency regardless of cause, because oxygen delivery and cardiac reserve are compromised. [2]
Classification
Two intersecting grids sort the differential. The first uses red-cell size: microcytic, normocytic or macrocytic, judged by the mean corpuscular volume against an age-adjusted reference range. The second uses marrow kinetics: is the reticulocyte count high, showing the marrow compensating for loss or destruction, or inappropriately low, showing production failure? [1] [6]
For practical teaching, adults anchor microcytic at a mean corpuscular volume below 80 femtolitres and macrocytic above 100 femtolitres, with the normocytic band between. Infants and young children run slightly lower normal volumes, so always read the value against the age-specific reference range supplied by your laboratory rather than a single adult number. [6]
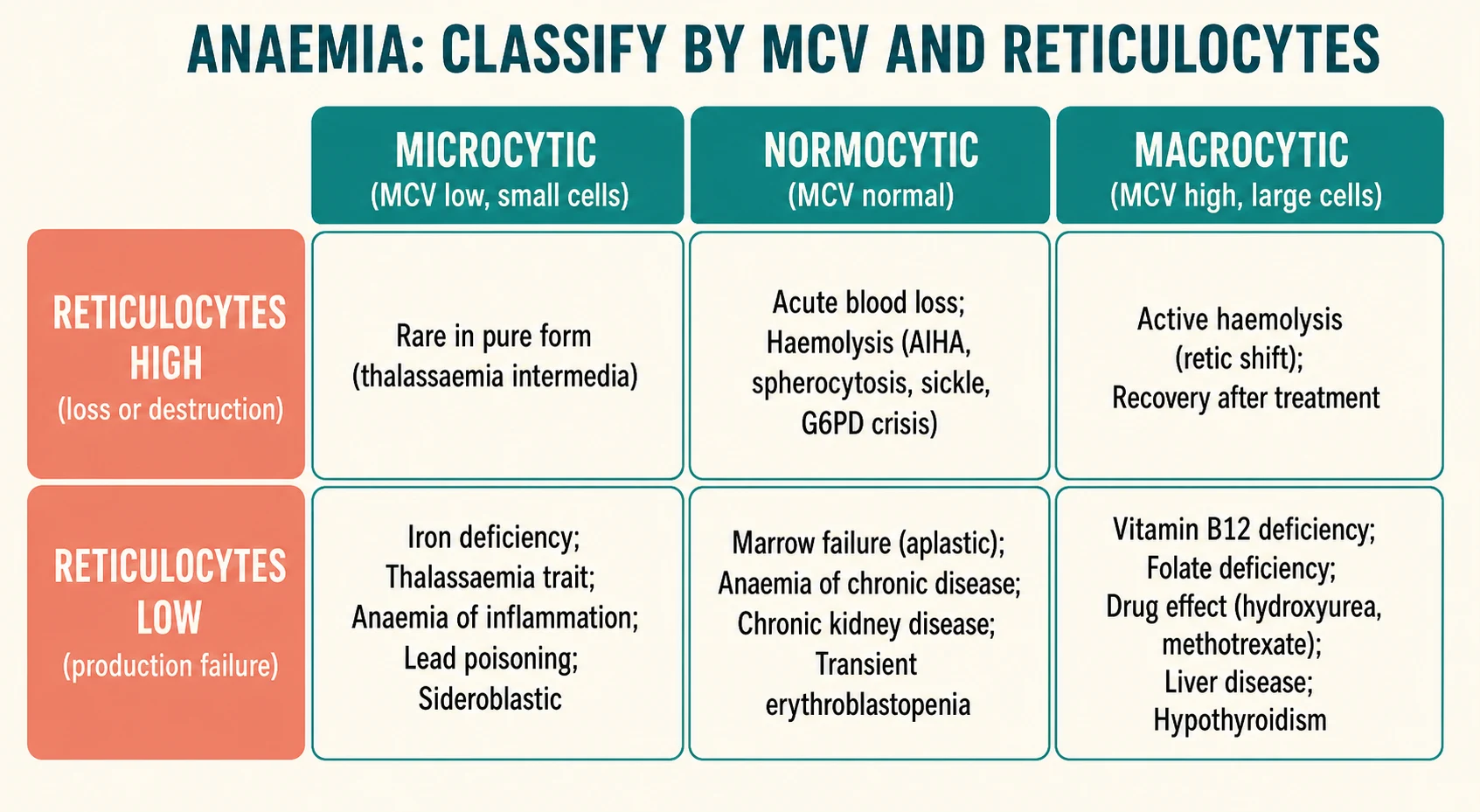
Microcytic anaemia is the busiest cell. Iron deficiency dominates, but the same small pale red cells appear in thalassaemia trait and disease, anaemia of chronic inflammation, lead poisoning, sideroblastic anaemia and rarely copper deficiency. The reticulocyte count in pure microcytic iron deficiency is usually low or normal, because the marrow is starved of substrate. [1] [7] [8]
Normocytic anaemia holds the acute and the mixed. Acute blood loss reads normocytic for the first day or two until the marrow catches up and reticulocytes rise. Haemolysis is usually normocytic with a high reticulocyte count. Anaemia of chronic disease is typically normocytic and mild, occasionally microcytic. Marrow failure and infiltration are normocytic with inappropriately low reticulocytes. [1] [11]
Macrocytic anaemia is the least common but the most likely to be missed. Vitamin B12 or folate deficiency, drug effects such as hydroxyurea or anticonvulsants, liver disease, hypothyroidism, marked reticulocytosis from active haemolysis, and marrow stress including Down-syndrome-associated transient abnormal myelopoiesis all push the mean corpuscular volume upward. [9] [10]
Epidemiology & Risk Factors
Iron deficiency anaemia is the most common anaemia of childhood worldwide. Risk concentrates where iron demand from rapid growth outruns supply, which peaks in later infancy and again in adolescence. Premature birth halves iron stores at birth, exclusive prolonged breastfeeding beyond six months without an iron source, early and excessive cow's milk feeding, restrictive or low-iron diets, and food insecurity all raise the odds. [1] [3] [4]
Adolescent females add menstrual loss to growth demand, and restrictive eating or heavy periods can tip a borderline store into deficiency. Chronic inflammatory disease, chronic kidney disease and recurrent blood loss from surgery or sampling in a child with medical complexity all shift iron handling and suppress erythropoiesis. [3] [11]
Inherited red-cell disorders carry strong ancestry and geography. Alpha and beta thalassaemia trait are common in people of Mediterranean, Middle Eastern, South Asian, Southeast Asian and African ancestry. Sickle cell disease and G6PD deficiency cluster across sub-Saharan African, Mediterranean and Middle Eastern populations, and hereditary spherocytosis is the most common inherited haemolytic anaemia in northern European populations. Use ancestry to choose which tests to add, never to assume a diagnosis. [7] [8]
Lead exposure remains a cause of microcytic anaemia in children with pica, old housing with deteriorating paint, or industrial and folk-medicine exposures. The burden has fallen in countries with public health programmes, but pockets persist, and a child with unexplained microcytosis and basophilic stippling deserves a blood lead level. [12]
Marrow failure and leukaemia are far less common than iron deficiency, yet they present through the same clinic door. Multi-lineage cytopenias, fever, bone pain and organomegaly are the warning signs that move a child from a routine iron pathway to same-day escalation. [2]
Pathophysiology
Haemoglobin carries oxygen, so a falling haemoglobin lowers oxygen delivery and the heart raises output to compensate. Tachycardia, a flow murmur, fatigue and reduced exercise tolerance appear as the haemoglobin drifts down. When the fall is rapid or severe, high-output cardiac strain and tissue hypoxia tip into heart failure and shock. [1] [3]
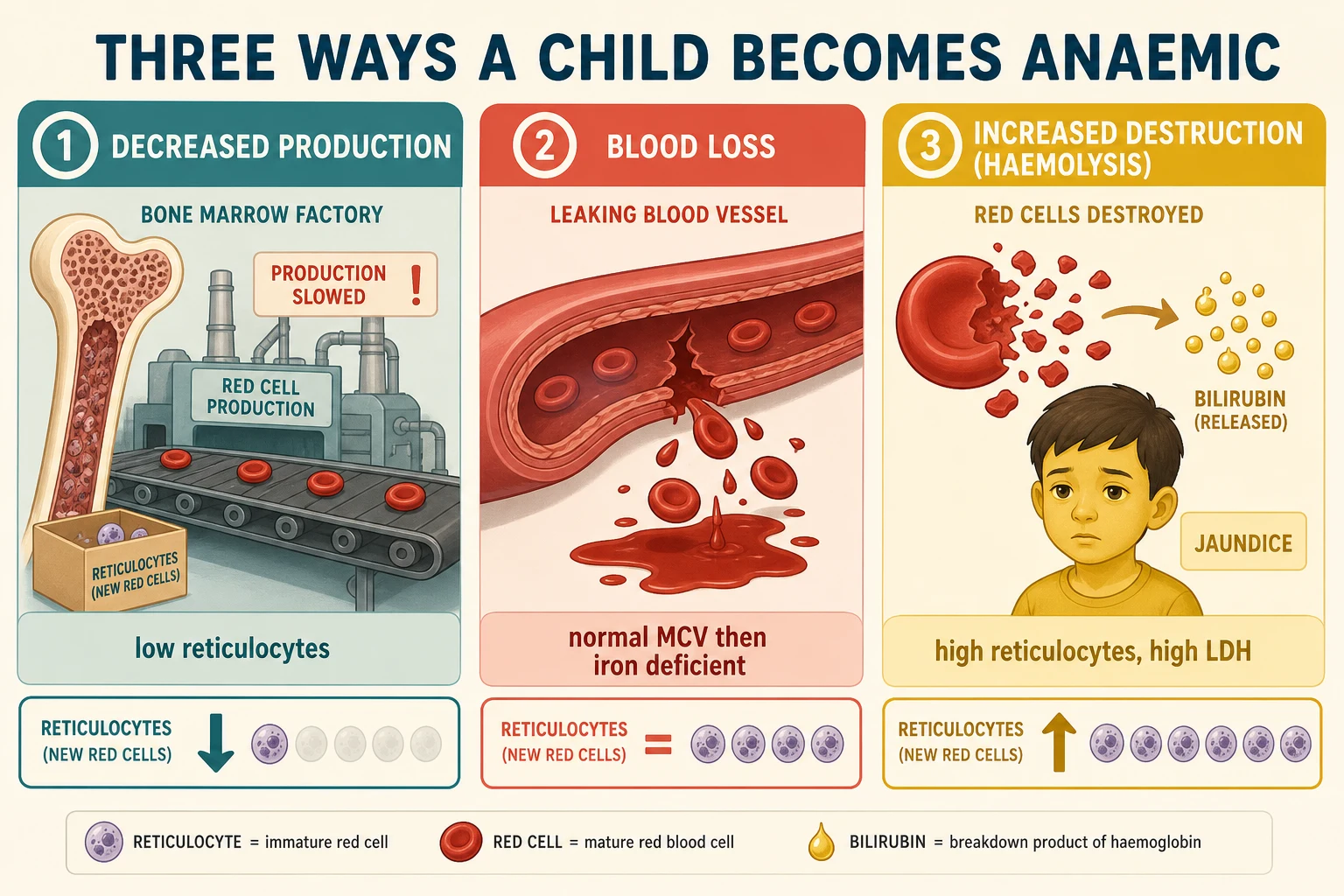
The marrow responds to any anaemia by releasing reticulocytes, the young red cells that still carry residual ribonucleic acid. A reticulocyte count that rises appropriately means the marrow is healthy and iron is available, and the problem lies outside the marrow in loss or destruction. A reticulocyte count that stays flat in the face of significant anaemia means the marrow cannot keep up, because of substrate lack, marrow failure, infiltration or suppressed erythropoiesis. [6]
Iron deficiency starves haemoglobin synthesis specifically. Red cells leave the marrow small and pale, described as microcytic and hypochromic, and the red cell distribution width rises early because cells of many sizes coexist. Iron also serves muscle and brain enzymes, which is why prolonged deficiency in infancy carries developmental consequences beyond the blood count. [3] [4]
Haemolysis shortens red-cell survival and provokes a compensatory reticulocytosis. Cell breakdown releases lactate dehydrogenase and indirect bilirubin, consumes haptoglobin in intravascular forms, and can darken the urine with haemoglobinuria. Membrane disorders such as hereditary spherocytosis, enzyme defects such as G6PD deficiency, immune destruction such as autoimmune haemolytic anaemia, and haemoglobinopathies such as sickle cell disease each destroy cells by a different route. [1]
Production failure empties the marrow. Aplastic anaemia, marrow infiltration by leukaemia or solid tumour, transient erythroblastopenia of childhood, and severe substrate lack all leave reticulocytes inappropriately low. When two or three cell lines fall together, the problem is almost certainly within the marrow rather than the periphery. [2]
Clinical Presentation
Children rarely volunteer "I am anaemic". Parents describe tiredness, less energy on the playground, poor feeding or tiring mid-feed in an infant, breathlessness on stairs, or pica for ice and dirt. Teachers may flag school fatigue. The history often arrives only after a routine count returns abnormal. [1] [4]
Gradual iron deficiency can look deceptively well even at a surprisingly low haemoglobin, because the body compensates over weeks. Irritability, pallor and a systolic flow murmur are common. Very severe or rapid-onset anaemia instead declares itself with breathlessness, poor perfusion, breath-holding or cardiac failure signs. [3]
Acute haemolysis looks different again. Sudden pallor, jaundice, dark or tea-coloured urine, abdominal or back pain, and sometimes fever follow a trigger such as infection or an oxidant drug in G6PD deficiency. A family history of neonatal jaundice, early gallstones or splenectomy points toward a chronic haemolytic disorder such as hereditary spherocytosis. [1]
Marrow pathology adds its own signature. Fever, bruising, petechiae, bone pain, limp, lymphadenopathy or hepatosplenomegaly alongside anaemia collapses the timeline to same-day investigation. Isolated mild anaemia without these features does not exclude serious disease, but their presence removes any room for a wait-and-see approach. [2]
Differential Diagnosis
Rank threats and likelihood together. The life threats are acute massive haemorrhage, fulminant haemolysis, severe anaemia with cardiac compromise, sepsis with marrow suppression, leukaemia with neutropenic infection risk, and aplastic anaemia. Common causes are dietary iron deficiency, thalassaemia trait, anaemia of chronic disease and transient blood loss. [1] [2]
The MCV and reticulocyte grid places each cause in a cell. Microcytic and low reticulocyte holds iron deficiency, thalassaemia, anaemia of inflammation, lead poisoning and sideroblastic anaemia. Normocytic with high reticulocyte holds haemolysis and acute blood loss after the first day. Normocytic with low reticulocyte holds marrow failure, infiltration, anaemia of chronic disease and transient erythroblastopenia. Macrocytic holds B12 or folate deficiency, drug effects, liver disease, hypothyroidism and active haemolysis with a reticulocyte shift. [1] [9] [10]
Age shifts the prior probabilities. Infants push toward haemolysis and congenital marrow failure. Toddlers push toward dietary iron deficiency and lead. School-age children raise the proportion of chronic disease and marrow pathology. Adolescents add menstrual loss, restrictive eating and the inherited haemoglobinopathies declared by screening or symptoms. [2]
Clinical & Bedside Assessment
A sick-looking child with severe anaemia is stabilised before the laboratory reasoning begins. Assess appearance, work of breathing, circulation and conscious level against age-normal vital signs. Tachycardia, a gallop, hepatomegaly, poor perfusion or breathlessness at rest signal decompensation and move the child toward oxygen, cautious volume support and urgent senior input. [1]
In the stable child, take a history that changes the diagnostic branch. Ask about diet and milk volume, gestation and birthweight, growth and development, family blood disorders and ancestry, jaundice and dark urine, medications including oxidants, menstrual pattern, stool colour and bleeding, pica, lead exposure, travel, and the trajectory of symptoms. Use a professional interpreter when language differs, because diet and bleeding histories are easily lost in translation. [2]
Examine for the cause as much as for the anaemia. Check growth parameters, lymphadenopathy, liver and spleen size, cardiac murmur and failure signs, jaundice, glossitis and koilonychia, bruising and petechiae, and any dysmorphism suggesting a syndrome. Observe the child playing: a child who is genuinely limited by breathlessness tells you more than a single colour judgment. [1]
Investigations
The first three tests are the map. A full blood count with red-cell indices, a reticulocyte count, and a peripheral blood film organise almost every case before any second-line test is ordered. Read the white cell and platelet lines at the same time, because multi-lineage cytopenias redirect the workup toward the marrow. [1] [6]
Directed second-line tests follow the grid. For a microcytic pattern, order iron studies: ferritin, serum iron, transferrin or total iron-binding capacity, and transferrin saturation. Low ferritin with low iron and high binding capacity confirms iron deficiency. Add a haemoglobinopathy screen when the microcytosis is disproportionate, the red cell count is high, iron studies are discordant, or ancestry or family history suggest thalassaemia, so that trait is not mistaken for iron deficiency. [1] [7]
For a normocytic pattern with high reticulocytes suggesting haemolysis, add a direct antiglobulin test, lactate dehydrogenase, haptoglobin, unconjugated bilirubin, and a haemoglobinopathy and enzyme screen as guided by the film and history. For a normocytic pattern with low reticulocytes and other cytopenias, prepare for marrow examination including aspirate and trephine with cytogenetics. [1] [2]
For a macrocytic pattern, measure serum vitamin B12 and red-cell or serum folate, and review the film for hypersegmented neutrophils and oval macrocytes. Add liver and thyroid function when the picture fits. Macrocytosis from a marked reticulocytosis is itself a clue to active haemolysis rather than a primary deficiency. [9] [10]
Iron studies that change the branch
When lead is plausible, send a venous blood lead level; the peripheral film may show basophilic stippling. Current public-health reference values set the blood lead reference level at 3.5 micrograms per decilitre, and any elevated result triggers source identification and follow-up. Always confirm with a venous sample rather than a capillary one before acting. [12]
One timing pitfall deserves emphasis. During acute haemolysis in G6PD deficiency, the most deficient older cells have already lysed, so a single normal enzyme assay at the crisis can be falsely reassuring; retest weeks later if suspicion remains. Draw diagnostic samples before any transfusion when the child is stable enough, because transfused blood will obscure the film, the reticulocyte count and special tests. [1]
Management — Resuscitation
An unstable anaemic child receives the same first actions as any critically ill child: secure the airway, give oxygen for hypoxia or respiratory distress, support breathing, restore the circulation with cautious fluid boluses, check glucose if consciousness is altered, and call for senior help early. Severe anaemia can present as high-output failure, and over-rapid volume expansion in a chronic, compensated anaemia can precipitate pulmonary oedema, so resuscitation follows local paediatric critical-care guidance rather than an adult recipe. [2]
Transfusion is a decision about physiology, not a number. Transfuse for symptomatic anaemia with cardiac compromise or ongoing loss, and withhold it from a well-compensated child while the diagnosis is pursued, because a single restrictive threshold does not fit every paediatric context. When transfusion is needed urgently, do not delay rescue blood to perfect a pre-transfusion panel, but sample first whenever it is safe to do so. Leucodepleted, cross-matched and cytomegalovirus-safe products and local transfusion thresholds apply; follow your hospital's paediatric blood bank rules. [2]
Acute haemolysis needs trigger removal when known, monitoring for acute kidney injury, and haematology input. Autoimmune haemolytic anaemia and suspected aplastic or malignant marrow disease are haematology emergencies once recognised. Fever with neutropenia and anaemia is treated as a time-critical infection risk with empirical broad-spectrum antibiotics while the diagnosis is clarified. [1]
Management — Definitive & Stepwise
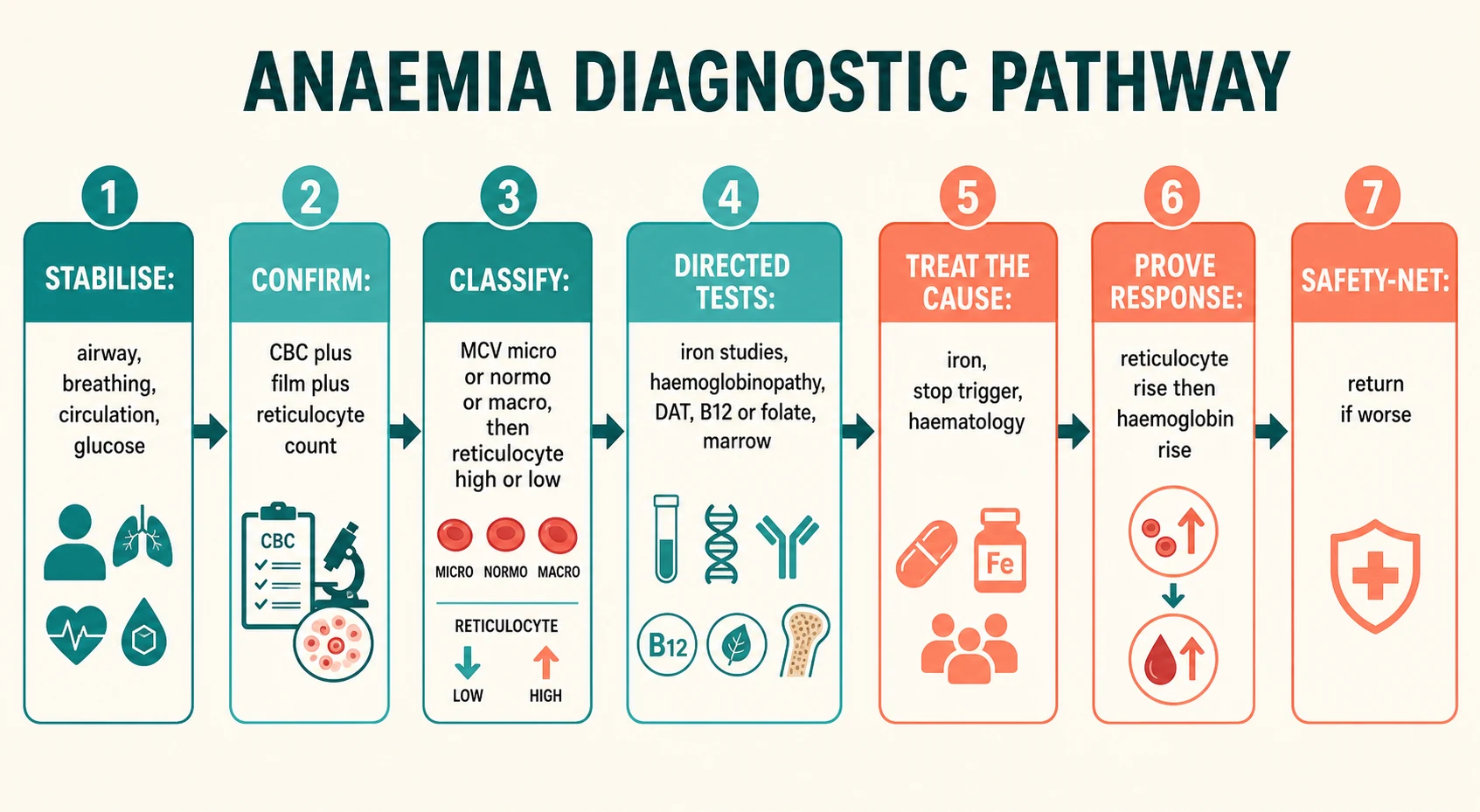
Step one is to stabilise and decide the location of care. A well toddler with mild microcytic anaemia can be worked up as an outpatient. A child with severe symptoms, a very low haemoglobin, active haemolysis, suspected marrow failure or unsafe follow-up goes to hospital. [1]
Step two is to confirm and classify. Read the full blood count, reticulocyte count and film together, and write a one-line problem representation such as "eighteen-month-old with dietary risk, microcytic hypochromic anaemia, low ferritin, no red flags for marrow disease". That sentence should name the cell size, the marrow response and the threat level in one breath. [1] [6]
Step three is to treat the confirmed cause. For iron deficiency, correct the driver such as excess cow's milk or occult loss, start oral elemental iron at 3 to 6 milligrams per kilogram per day, plan a response check, and address diet. A reticulocyte rise should appear within seven to ten days, followed by a haemoglobin rise over subsequent weeks. The exact product and salt follow your local formulary. [1] [5]
Step four is to avoid iron-blinding yourself. If the microcytosis is out of proportion, the iron studies are normal, or the red cell count is high, investigate thalassaemia trait and the other microcytic mimics before committing a child to indefinite iron. Empiric iron in a non-iron-deficient thalassaemia carrier risks overload and teaches the wrong mechanism. [7] [8]
Step five is to engage the haemolysis and marrow pathways. Autoimmune haemolysis, hereditary spherocytosis, sickle cell disease, aplastic anaemia and leukaemia need haematology partnership and disease-specific protocols, which live in their own leaves. [1] [2]
Step six is to prove the response and safety-net. Recheck the full blood count at the expected interval. A failure of the haemoglobin to rise after an adequate iron course means the diagnosis is wrong, loss is ongoing, adherence is poor, or malabsorption is present, and the workup restarts rather than the iron dose simply climbing. Give clear written and verbal advice to return for worse pallor, dark urine, bleeding, fever or breathlessness. [4] [5]
Specific Subtypes & Scenarios
Toddler dietary iron deficiency. High milk volume displacing solids, microcytic hypochromic anaemia, low ferritin and a raised red cell distribution width. Reduce milk to about 500 millilitres a day, improve iron-rich solids, start oral iron, and recheck for response. [1] [4]
Thalassaemia trait. Mild microcytosis with a high red cell count and normal or near-normal ferritin, often found on screening or family study. Confirm with haemoglobin electrophoresis or high-performance liquid chromatography and counsel the family, including reproductive implications at the right moment. Trait needs no iron unless iron deficiency coexists and is proven. [7] [8]
Anaemia of chronic disease. Normocytic or mildly microcytic anaemia in a child with inflammation, infection, autoimmunity or chronic kidney disease, with normal or high ferritin and low iron-binding capacity. Treat the underlying disease; iron is rarely the answer and can feed infection or inflammation. [11]
Lead-associated microcytic anaemia. Microcytosis with basophilic stippling and an elevated blood lead level in a child with pica or exposure. Identify and remove the source, address nutrition especially iron and calcium, and follow public-health guidance on chelation thresholds. [12]
Macrocytic anaemia from B12 or folate lack. Oval macrocytes and hypersegmented neutrophils on the film, with low vitamin levels. Identify and treat the cause, which in children includes dietary restriction, malabsorption, pernicious anaemia and rare inborn errors, and replace the missing vitamin under specialist guidance. [9] [10]
Transient erythroblastopenia of childhood. A previously well toddler or preschool child with a normocytic anaemia and very low reticulocytes but normal neutrophils and platelets, recovering spontaneously over weeks. Distinguish from Diamond-Blackfan anaemia, which presents earlier in infancy and often with other features. [2]
Leukaemia and marrow failure. Anaemia with fever, bruising, bone pain, organomegaly or multi-lineage cytopenias needs same-day film and senior review, not an iron trial. Marrow examination confirms the diagnosis. [2]
Complications & Pitfalls
- Treating every microcytosis as iron deficiency and missing thalassaemia trait, lead or inflammation. [7] [11]
- Relying on a single ferritin in inflammation, which reads falsely normal because ferritin is an acute-phase reactant. [11]
- Trusting a normal G6PD assay drawn during acute haemolysis. [1]
- Missing multi-lineage cytopenias by reading only the haemoglobin and ignoring platelets and white cells. [2]
- Transfusing a well-compensated child for a number alone, or withholding rescue blood from a decompensating child for a perfect panel. [2]
- Over-rapid volume expansion in chronic severe anaemia causing pulmonary oedema. [2]
- Failing to recheck response to iron, so ongoing loss, wrong diagnosis or non-adherence goes unnoticed. [4]
Prognosis & Disposition
Most dietary iron deficiency resolves fully when both the cause and the replacement are handled and adherence is real. The expected laboratory course is a reticulocyte rise within the first week or two followed by a steady haemoglobin climb, and failure of that pattern restarts the diagnostic reasoning rather than ending it. [1] [4]
Haemolytic and marrow disorders follow disease-specific trajectories, and early haematology involvement improves safety. Prolonged severe anaemia in infancy carries developmental and cardiac risk, which is one reason a child with months of progressive limitation is not dismissed as "just pale". [2] [3]
Safe discharge needs a named review plan, a clear safety-net, access to medicines, and a family who can return. When food insecurity, chaotic housing or transport barriers block iron and diet change, treat the social determinants as part of the prescription. [5]
Special Populations
Infants need iron stores and haemolysis considered together, and prematurity lowers the iron reserve at birth. [3]
Adolescents deserve a confidential menstrual and dietary history, including restrictive eating. [4]
Children with medical complexity may carry chronic disease anaemia, procedural blood-loss burden and altered iron handling at once. [11]
Ancestry-linked risk guides which tests to add, with respectful counselling rather than racialised assumption. [7] [8]
Indigenous families in Australia and New Zealand deserve culturally safe conversations about diet, access and the higher burden of iron deficiency in remote settings. [3]
Migrant and refugee children need catch-up screening, diet history through an interpreter, and non-stigmatising haemoglobinopathy testing. [2]
Children in food-insecure households should have social drivers addressed alongside any iron prescription. [4]
Evidence, Guidelines & Regional Differences
Allali's expert review frames the prevalence, causes and diagnostic work-up of anaemia in children and remains a high-yield map for the fellowship answer. Wang's practical review and the updated Leung review reinforce an MCV-first, cause-directed approach to iron deficiency. Short's evaluation-and-management article anchors cause correction plus replacement rather than tablets alone. [1] [2] [4] [5]
Pasricha's Lancet review places iron deficiency in its global biological and developmental context, explaining why this common problem still damages growth and cognition. Celkan's hemogram primer supports bedside reading of the full blood count and indices. [3] [6]
The thalassaemia reviews by Muncie and Baird prevent the iron-for-everyone error. Stabler and Socha anchor the macrocytic pathway, and Weiss grounds the anaemia of chronic disease. Lanphear's current New England Journal review keeps lead on the differential for unexplained microcytosis. [7] [8] [9] [10] [11] [12]
Local hospital anaemia and transfusion pathways, newborn screening panels and culturally safe care for Aboriginal, Torres Strait Islander and Māori whānau shape real practice. Use Royal Children's Hospital Melbourne guidance as an operational anchor where applicable. [1]
British Society for Haematology guidelines and National Health Service anaemia pathways, with regional haemoglobinopathy services, often structure the clinic answer. [10]
American Academy of Pediatrics iron screening ages and universal lead testing shape the outpatient workup, with institutional transfusion committees setting thresholds. [4] [12]
Provincial newborn screening and paediatric haematology networks determine haemoglobinopathy detection and referral flow. [8]
Exam Pearls
- A low haemoglobin is a pattern; classify it by MCV then reticulocytes. [6]
- Microcytic plus low reticulocyte: iron deficiency, thalassaemia, inflammation, lead. [1]
- Normocytic plus high reticulocyte: haemolysis or acute blood loss. [1]
- Normocytic plus low reticulocyte with other cytopenias: marrow failure or infiltration. [2]
- Macrocytic with hypersegmented neutrophils: B12 or folate. [9]
- High red cell distribution width favours iron deficiency; normal width with high red cell count favours trait. [1]
- Oral elemental iron is 3 to 6 milligrams per kilogram per day; expect a reticulocyte rise first. [1]
- Never trial iron in a febrile, bruised child with cytopenias. [2]
References
- [1]Wang M Iron Deficiency and Other Types of Anemia in Infants and Children. American family physician, 2016.PMID 26926814
- [2]Allali S Anemia in children: prevalence, causes, diagnostic work-up, and long-term consequences. Expert review of hematology, 2017.PMID 29023171
- [3]Pasricha SR Iron deficiency. Lancet (London, England), 2021.PMID 33285139
- [4]Leung AKC Iron Deficiency Anemia: An Updated Review. Current pediatric reviews, 2024.PMID 37497686
- [5]Short MW Iron deficiency anemia: evaluation and management. American family physician, 2013.PMID 23317073
- [6]Celkan TT What does a hemogram say to us? Turkish archives of pediatrics, 2020.PMID 32684755
- [7]Baird DC Alpha- and Beta-thalassemia: Rapid Evidence Review. American family physician, 2022.PMID 35289581
- [8]Muncie HL Jr Alpha and beta thalassemia. American family physician, 2009.PMID 19678601
- [9]Stabler SP Clinical practice. Vitamin B12 deficiency. New England Journal of Medicine, 2013.PMID 23301732
- [10]Socha DS Severe megaloblastic anemia: Vitamin deficiency and other causes. Cleveland Clinic journal of medicine, 2020.PMID 32127439
- [11]Weiss G Anemia of chronic disease. New England Journal of Medicine, 2005.PMID 15758012
- [12]Lanphear B Lead Poisoning. New England Journal of Medicine, 2024.PMID 39476342