Paeds · haematology-oncology-and-transfusion
Blood-component therapy in children
Also known as Paediatric transfusion · Red cell transfusion in children · Platelet transfusion in children · Fresh frozen plasma in children · Cryoprecipitate in children · Massive transfusion in children · Patient blood management in children
Fellowship guide to blood-component therapy in children, the deliberate, dose-based use of red cells, platelets, fresh frozen plasma and cryoprecipitate to correct deficits the body cannot correct itself. Covers the separation of one whole-blood donation into four targeted components, the restrictive transfusion philosophy of patient blood management, and the per-kilogram doses that define paediatric practice: packed red cells at 10 to 15 mL per kg to raise the haemoglobin, platelets at 10 to 20 mL per kg to lift the count, fresh frozen plasma at 10 to 15 mL per kg for multiple clotting-factor deficiency, and cryoprecipitate at 5 to 10 mL per kg for a low fibrinogen. Reviews the transfusion thresholds, from the restrictive haemoglobin of 70 g per litre in the stable critically ill child of the TRIPICU and Cochrane trials to the neonatal platelet threshold of 25 times ten to the nine per litre of the PlaNeT-2 MATISSE trial, the special products of leucodepletion, irradiation and cytomegalovirus-negative blood, the prevention and recognition of transfusion reactions including circulatory overload and acute lung injury, and the massive-transfusion protocol.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
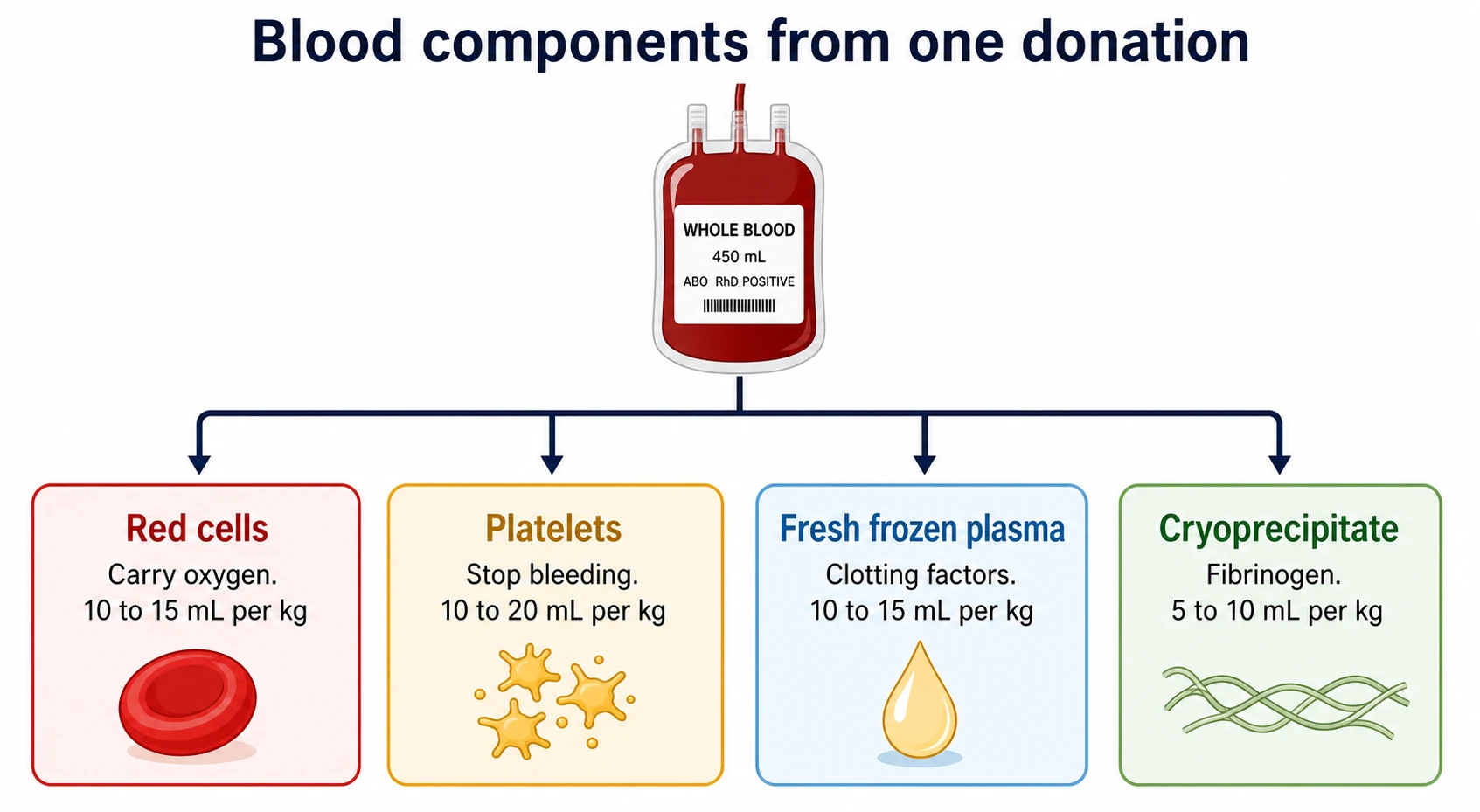
Blood-component therapy in children is the deliberate, dose-based use of the parts of donated blood to correct a deficit the child's own marrow or liver cannot correct quickly enough. One whole-blood donation is no longer transfused as a unit. Instead it is separated by centrifugation into four targeted components, each one prepared and stored to do a single job: red cells to carry oxygen, platelets to plug bleeding, fresh frozen plasma to supply clotting factors, and cryoprecipitate to deliver fibrinogen. The paediatric clinician transfuses the component the child lacks, at a weight-based dose, only when the benefit outweighs the risk. [2]
The philosophy that governs modern transfusion is patient blood management, and its core principle is restraint. A transfusion is a liquid transplant of living tissue from one person to another, and it carries real risks of immunological reaction, circulatory overload, infection and iron overload, so the default is not to transfuse but to treat the cause, to correct iron and vitamin deficiency, to minimise iatrogenic blood loss and to use alternatives such as tranexamic acid. When transfusion is needed, the child receives the smallest effective dose of the correct component, weighed to the kilogram, and observed for the reactions that can follow. The thresholds that trigger a transfusion have fallen steadily over three decades as the trials have shown that less is usually as good and sometimes better. [7][2]
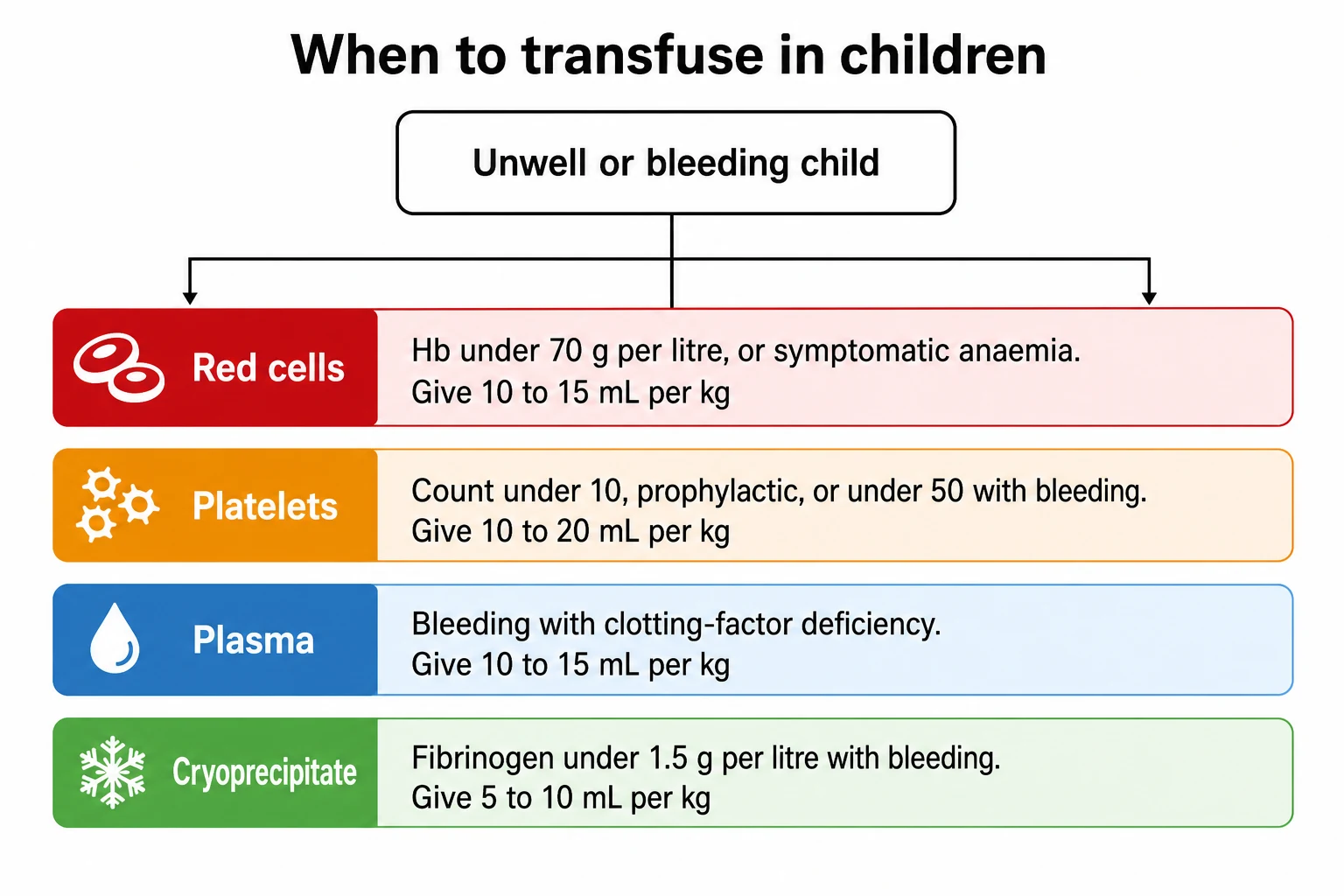
Three ideas make this topic central to the fellowship exam. The first is the per-kilogram dose, because the paediatric transfusion is a weight-based prescription and the candidate who cannot state that red cells run at 10 to 15 mL per kg, platelets at 10 to 20 mL per kg, plasma at 10 to 15 mL per kg and cryoprecipitate at 5 to 10 mL per kg cannot prescribe safely. The second is the threshold, because the restrictive haemoglobin of 70 g per litre in the stable critically ill child and the prophylactic platelet count of 10 times ten to the nine per litre are the evidence-based triggers most often examined. The third is safety, because the recognition and prevention of transfusion reactions, and the selection of special products for the neonate and the immunocompromised child, are the bedside skills that mark the safe paediatrician. [1][2]
Classification
Blood components sort by what they contain and by the job they do, and the single act of centrifuging a unit of whole blood yields the four products the fellow prescribes. Red cells, separated as packed cells, are the oxygen carriers, given to raise the haemoglobin and relieve the symptoms or the physiological consequences of anaemia. Platelets, separated as a pooled or apheresis concentrate, are the first responders of haemostasis, given to lift a low count or to support a child who is bleeding or about to undergo a procedure. Fresh frozen plasma is the liquid carrier of all the soluble clotting factors, given when several factors are deficient at once. Cryoprecipitate is the cold-insoluble fraction of plasma, rich in fibrinogen, given when the fibrinogen itself is low. Each is stored differently and measured differently, and each carries its own dose. [2]
A second axis of classification runs across these components and concerns how each unit is processed for a particular patient, because the child may need more than the standard unit. Leucodepleted components, with the white cells filtered out, are the default in most high-income countries because the white cells cause febrile reactions, carry cytomegalovirus and drive alloimmunisation. Cytomegalovirus-negative components are selected for the fetus, the neonate and the severely immunocompromised, in whom a primary cytomegalovirus infection can be devastating. Irradiated components are given to the profoundly immunocompromised child and to directed donations from family, because irradiation disables the donor white cells that could otherwise engraft and cause transfusion-associated graft-versus-host disease. Washed components remove plasma for the child with recurrent severe allergy or immunoglobulin A deficiency. These modifications are not optional refinements but safety requirements for the right patient, and the fellow names the indication for each. [2]
A third, practical distinction separates the components into those that must be ABO-identical and those that need only be ABO-compatible. Red cells carry the A and B antigens on their surface, so they must be ABO-compatible with the child's plasma, and ideally ABO-identical, to avoid an acute haemolytic reaction. Platelets carry ABO antigens too, but in a child with a normal count an ABO-compatible but non-identical unit is often given, reserving ABO-identical platelets for the child who is transfused often or who has become refractory. Plasma is the reverse: it carries the donor antibodies, so group AB plasma, which has neither anti-A nor anti-B, is the universal donor plasma used in the emergency where the child's group is unknown. Cryoprecipitate is likewise matched by ABO where feasible. The fellow who understands which product must match which way avoids the dangerous mismatch. [2]
Epidemiology & Risk Factors
Blood transfusion is one of the commonest procedures in hospitalised children, and the child most likely to receive one is the premature neonate, the child with a chronic haematological disease and the child in the intensive care unit. Preterm infants are transfused more than any other group, because their small circulating volume, their frequent blood sampling and their low erythropoietin together drive repeated red cell top-ups in the first weeks of life. Children with transfusion-dependent anaemias such as beta-thalassaemia major and sickle cell disease, and those receiving chemotherapy or stem cell transplant, account for a large share of the chronically transfused. The child in the paediatric intensive care unit or the emergency department with trauma, sepsis or surgical bleeding is the child at risk of needing an urgent or a massive transfusion. [2][1]
The risk of a transfusion is inseparable from its benefit, and the fellow weighs the two at every prescription. The commonest serious reaction is no longer infection but transfusion-associated circulatory overload, the volume overload that follows a transfusion given too fast or too large to a small circulation, and it is commonest at the extremes of size and of illness, in the neonate and the child with heart or kidney failure. Acute and delayed haemolytic reactions arise from immunological incompatibility, allergic reactions from plasma proteins, febrile reactions from cytokines, and the rare but feared transfusion-associated acute lung injury and graft-versus-host disease from donor white cells. Transfusion-transmitted infection has become rare in the screened, tested blood supply of high-income countries, but it has not vanished, and it remains a major risk in regions of variable blood safety. [2]
The single greatest determinant of transfusion safety and availability is the blood supply itself, and this varies sharply by region. A child treated in a system with a sufficiency of screened, leucodepleted, viral-tested, volunteer-donor blood receives transfusions that are among the safest in medicine, while a child in a region of scarcity or variable testing faces a higher risk of shortage, of ABO mismatch and of transfusion-transmitted infection. This gap explains why patient blood management, the strategy of minimising transfusion by treating the cause and the alternatives, is promoted as much for safety and stewardship as for cost, and why the fellow frames every transfusion as a resource decision as well as a clinical one. [7]
Pathophysiology
The rationale for component therapy rests on the simple physiology that the four parts of blood do four different jobs, and that giving whole blood to correct a single deficit burdens the child with volume and components it does not need. Centrifuging a unit of whole blood separates the dense red cells from the lighter platelet-rich plasma, and the plasma is then further separated into the frozen plasma and the cryoprecipitate that forms when frozen plasma thaws. Each fraction is then resuspended, tested and stored at the temperature that best preserves its function, so that the child with isolated anaemia receives only red cells, the child with thrombocytopenia receives only platelets, and the child with a coagulopathy receives only the factors it lacks. This fractionation turns one donation into four targeted therapies. [2]
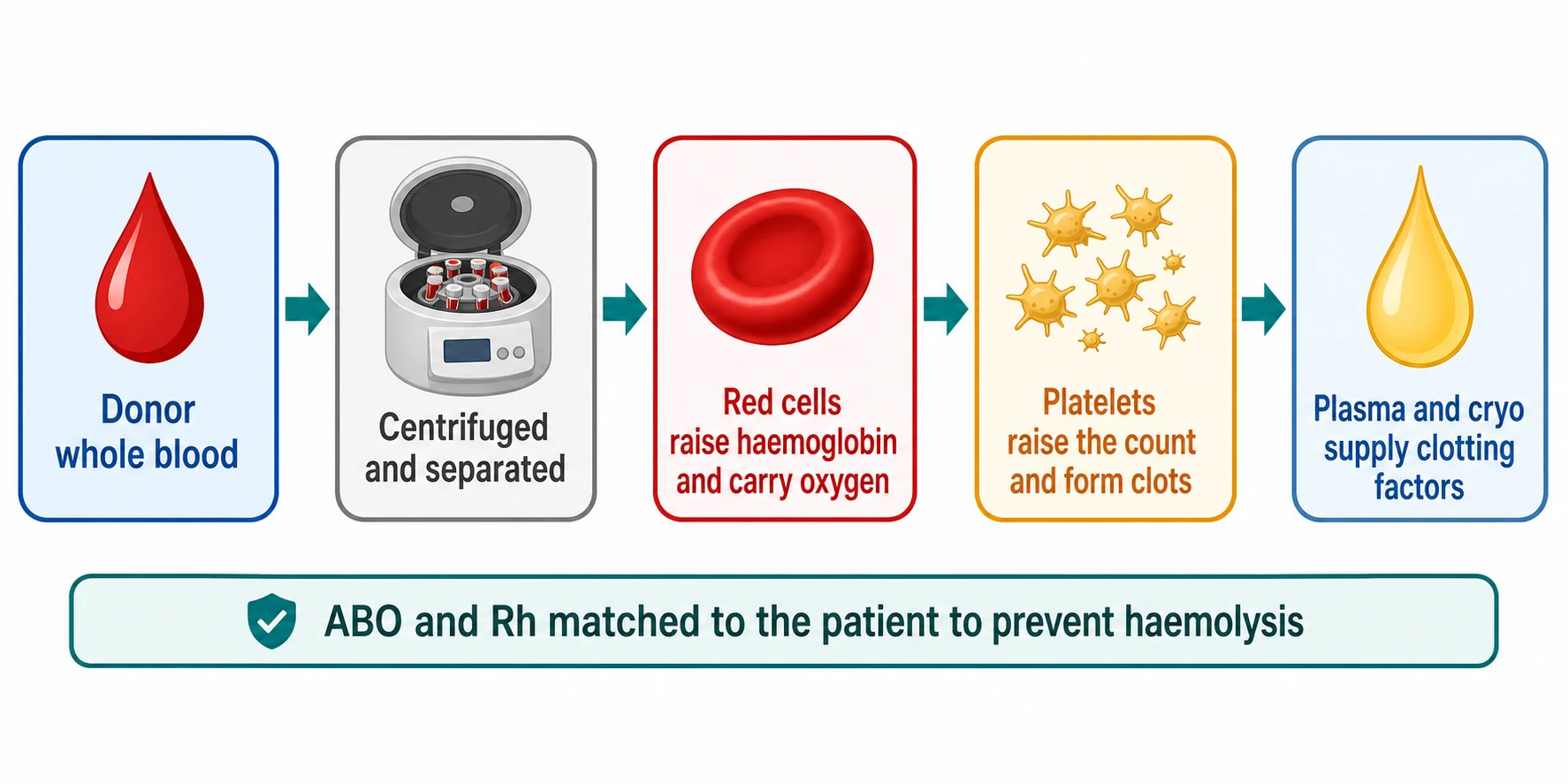
The physiology that demands ABO matching is the same immunology that explains the acute haemolytic reaction, and it is the physiology the fellow must know exactly. The A and B antigens sit on the red cell surface, and by early childhood the body has formed antibodies against the antigens it lacks, so a child with group A blood carries anti-B in the plasma. Transfused red cells of the wrong ABO group are recognised, agglutinated and lysed within minutes by the preformed antibody and complement, releasing cell contents that cause fever, hypotension, disseminated intravascular coagulation and acute kidney injury. Red cells are therefore matched to be ABO-compatible, and ideally ABO-identical, before they are ever hung. The Rh D antigen is matched in the same way, and a child who is Rh D negative receives Rh D negative red cells to avoid forming an anti-D that would complicate every future transfusion and every future pregnancy. [2]
The pathophysiology of the transfusion reactions themselves follows from the same logic of immunology and volume. Transfusion-associated circulatory overload is hydrostatic, the rise in atrial pressure that overflows the pulmonary capillaries when a transfusion outpaces a small or failing circulation. Transfusion-associated acute lung injury is immunological, the donor antibodies or active lipids that bind the recipient neutrophils and flood the alveoli with protein, a process indistinguishable from acute respiratory distress syndrome. Transfusion-associated graft-versus-host disease is the ultimate immunological disaster, the donor white cells that engraft in a child who cannot reject them and attack the skin, the gut and the marrow. Understanding the mechanism of each reaction is the key to recognising it at the bedside and to preventing it with the right special product. [2]
Clinical Presentation
The child who needs a red cell transfusion presents with the consequences of a low haemoglobin, and the decision to transfuse turns on the symptoms and the physiological strain rather than on a single number. The stable child with a haemoglobin above 70 g per litre and no symptoms does not need a transfusion, because the trials have shown that a restrictive strategy is as safe as a liberal one in this group. The child who is symptomatic, with exertional dyspnoea, heart failure or a haemoglobin falling fast from acute blood loss, is transfused regardless of the threshold. The chronically anaemic child, such as the one with thalassaemia major, is transfused on a programme that keeps the pre-transfusion haemoglobin at 90 to 100 g per litre, because the transfusion there is suppressing the marrow and enabling growth rather than rescuing a crisis. [1][7]
The child who needs platelets presents either with a low count at risk of bleeding or with active bleeding, and the threshold differs between the two. The child receiving intensive chemotherapy, whose marrow is suppressed and whose count has fallen below 10 times ten to the nine per litre, receives a prophylactic transfusion to prevent spontaneous bleeding, because the risk of a central nervous system haemorrhage rises sharply below this level. The child who is actively bleeding, or about to undergo a procedure with bleeding risk, is transfused to a higher threshold, commonly 50 times ten to the nine per litre, to secure haemostasis. The child with immune thrombocytopenia is the exception, because the transfused platelets are destroyed as fast as they are given, so platelets are reserved for the life-threatening bleed and the count is managed by medical therapy. [10][3]
The child who needs fresh frozen plasma presents with a coagulopathy of multiple factors at once, the picture of disseminated intravascular coagulation, of severe liver disease, or of the dilutional coagulopathy of massive transfusion. The child who needs cryoprecipitate presents with a fibrinogen that has fallen below about 1.5 g per litre in the setting of bleeding, the hypofibrinogenaemia of disseminated intravascular coagulation, of massive transfusion or of the inherited dysfibrinogenaemias. The child in major haemorrhage presents with all of these at once, the falling haemoglobin, the falling platelets and the falling fibrinogen of the consumption and dilution that define the bleeding emergency, and this is the child for whom the massive-transfusion protocol is activated. [4][2]
Differential Diagnosis
The first question before any transfusion is whether the child truly needs one, and the fellow distinguishes the deficit that demands blood from the one that is better treated another way. The child with iron deficiency anaemia, the commonest cause of a low haemoglobin in childhood, is treated with iron, not with blood, because the transfusion would carry risk without addressing the cause and the iron would restore the haemoglobin in weeks. The child with an acute anaemia from a treatable bleed is resuscitated with the control of the source and the smallest transfusion that restores perfusion, because the goal is oxygen delivery, not a normal haemoglobin. Patient blood management begins with the question of whether blood is the right tool at all. [7]
Red cells
oxygen deficit
- Packed red cells at 10 to 15 mL per kg over 2 to 4 hours
- Symptomatic anaemia or restrictive Hb threshold 70 g per litre
- Each 10 mL per kg raises haemoglobin by about 20 to 30 g per litre
- K-negative for girls, phenotype-matched for chronic use
Platelets
bleeding risk
- Apheresis or pooled platelets at 10 to 20 mL per kg
- Prophylactic threshold 10, bleeding or procedure threshold 50
- Raises count by 20 to 40 times ten to the nine per litre
- Reserve in ITP for life-threatening bleed only
Fresh frozen plasma
clotting factors
- Fresh frozen plasma at 10 to 15 mL per kg
- Multiple factor deficiency, DIC, liver disease, massive transfusion
- Not for volume expansion or a raised INR alone
- Group AB is the universal donor plasma
Cryoprecipitate
fibrinogen
- Cryoprecipitate at 5 to 10 mL per kg, about 1 pool for an adult
- Fibrinogen under 1.5 g per litre with bleeding
- Raises fibrinogen by about 1 g per litre
- Hypofibrinogenaemia of DIC and massive transfusion
The second question is which component the child needs, and the fellow matches the deficit to the product. A low haemoglobin alone points to red cells, a low platelet count to platelets, a raised clotting time with multiple factor deficiency to plasma, and a low fibrinogen to cryoprecipitate. The child with a single factor deficiency, such as haemophilia A, receives the specific factor concentrate rather than plasma, because the concentrate is safer, more effective and free of the volume and the infection risk of plasma. The child on warfarin receives prothrombin complex concentrate rather than plasma for urgent reversal. The child with immune thrombocytopenia receives medical therapy rather than platelets. Matching the deficit to the product is the essence of component therapy, and the wrong product is both wasteful and harmful. [2][3]
Clinical & Bedside Assessment
The safe transfusion begins long before the bag is hung, with the bedside assessment that confirms the indication, the correct component and the correct patient. The clinician confirms that the indication is sound, that the restrictive threshold has been respected, and that the child has been counselled on the reason, the benefit and the risk of the transfusion. The blood group, the antibody screen and the most recent full blood count and coagulation results are reviewed, and the prescription is written with the component, the volume in millilitres per kilogram, the rate and the duration. Special products, such as irradiated or cytomegalovirus-negative components, are prescribed where the indication exists, and diuretics or a slower rate are planned for the child at risk of overload. [2]
The bedside checks at the moment of transfusion are the last line of defence against the most dangerous error, the ABO mismatch, and they are performed by two clinicians at the bedside. The child is identified by name, date of birth and hospital number, and the details are checked against the compatibility label on the unit, the prescription and the child's identity band. The unit is inspected for clots, discolouration and damage, and the expiry date and the component type are confirmed. The intravenous line is patent, the child's baseline observations of temperature, pulse, respiratory rate and blood pressure are recorded, and the transfusion is begun slowly for the first 15 minutes, the window in which most acute reactions declare themselves. [2]
The safe paediatric transfusion, step by step
Confirm the indication, respect the restrictive threshold, and counsel the child and family on the reason and the risk
Check the group, the antibody screen, the full blood count and the coagulation, and write the component, the mL per kg, the rate and the duration
Prescribe special products, irradiated or CMV-negative, where indicated, and plan a diuretic or slower rate for the child at risk of overload
Perform the two-person bedside check of identity, compatibility label, unit integrity and expiry against the child and the prescription
Record baseline observations, run the first 15 minutes slowly, observe for fever, rash, dyspnoea or hypotension, and recheck observations at the end
The observations during the transfusion are the early-warning system for the reactions, and the nurse monitors them at defined intervals. The temperature, pulse and respiratory rate are checked at 15 minutes, and the blood pressure is rechecked, because a rise of temperature with hypotension is the signature of an acute haemolytic or a septic reaction. The child is asked about any new symptoms of itch, rash, rigors, breathlessness or anxiety, and the transfusion is slowed or stopped at the first sign of a reaction. A diuresis is encouraged or a diuretic is given to the child at risk of overload, and the response to the transfusion, in symptoms and in the post-transfusion haemoglobin or count, is documented once the unit is complete. [2]
Investigations
The investigation that precedes every transfusion is the group and screen, and it is the laboratory test that makes component therapy safe. The child's ABO and Rh D group is determined from the red cells, and the plasma is screened for the irregular antibodies that form after exposure to foreign red cell antigens, through transfusion, transplant or pregnancy. A negative antibody screen allows the laboratory to issue red cells that are ABO and Rh compatible without a full crossmatch, a process called electronic issue that speeds the supply in the routine case. A positive screen identifies the antibody and its specificity, and the laboratory selects antigen-negative units and performs a serological crossmatch to confirm compatibility before release. The group and screen is valid for a defined period, commonly three days in a child recently transfused, because new antibodies can form in that window. [2]
The investigations that guide the prescription are the full blood count and the coagulation profile, and they answer the questions of how much to transfuse and whether the transfusion worked. The haemoglobin and the platelet count, read against the restrictive thresholds, decide whether red cells or platelets are indicated and provide the baseline against which the response is measured. The prothrombin time, the activated partial thromboplastin time and the fibrinogen, read together, identify the coagulopathy that points to plasma or cryoprecipitate, and a fibrinogen below 1.5 g per litre in the bleeding child is the trigger for cryoprecipitate. The post-transfusion count, measured after the component has circulated, confirms the increment and guides the timing of the next dose. [2]
The way a unit is prepared and released varies by the blood service that supplies it, but the principle of leucodepletion as the default is now shared across high-income systems. Australia and Aotearoa New Zealand supply leucodepleted, cytomegalovirus-tested components through their national blood services, with cytomegalovirus-negative components reserved for the intrauterine, neonatal and severely immunocompromised recipient. The United Kingdom, the United States and Canada likewise provide leucodepleted components as standard, with irradiated components supplied on defined indication. In regions of variable blood safety the fellow weighs the risk of transfusion-transmitted infection more heavily, confirms the local testing of the supply, and leans harder on patient blood management to minimise exposure. The fellow names the local blood service and its testing policy when justifying a product choice.
[2]The investigation of a suspected transfusion reaction is its own protocol, and it begins the moment a reaction is suspected, with the transfusion stopped and the line kept open with saline. The unit and the giving set are returned to the laboratory with fresh blood and urine samples, the child is resuscitated and the reaction is reported to the haemovigilance system. A repeat group, a direct antiglobulin test, a full blood count and film, a coagulation screen and a renal and liver function are sent, and the unit is cultured if a bacterial contamination is suspected. The classification of the reaction, whether acute haemolytic, allergic, febrile, circulatory overload or acute lung injury, is made from the timing, the symptoms and these tests, and it determines the prevention of the next transfusion. [2]
Management — Resuscitation
The resuscitation of the bleeding child is the transfusion emergency, and it is the scenario in which the restrictive philosophy gives way to the rapid, ratio-based delivery of blood. The child in major haemorrhage, defined as the loss of one blood volume or the ongoing loss that will reach it, needs the immediate activation of a massive-transfusion protocol, a pre-agreed pathway that releases red cells, plasma and platelets in a balanced way while the source of bleeding is controlled. The protocol delivers red cells, fresh frozen plasma and platelets in a ratio that approximates whole blood, often with tranexamic acid and, in the trauma centre, with the surgical and interventional control of the source. The goal is the restoration of oxygen delivery, of circulating volume and of haemostasis together, because the replacement of red cells alone dilutes the clotting factors and the platelets and worsens the bleeding. [4]
The per-kilogram doses in the massive-transfusion protocol follow the same weight-based logic as the elective transfusion, scaled to the speed of the loss. Red cells are given in aliquots of 10 to 20 mL per kg, fresh frozen plasma in 10 to 15 mL per kg and platelets in 10 to 20 mL per kg, with the fibrinogen supported by cryoprecipitate at 5 to 10 mL per kg when it falls below 1.5 g per litre. Tranexamic acid is given early, within three hours of the bleed, at a loading dose followed by a maintenance infusion, because the early administration reduces death from bleeding. The child is warmed, because the hypothermia, the acidosis and the hypocalcaemia of the massive transfusion each worsen the coagulopathy, and calcium is replaced as the citrate in the transfused blood binds it. [4]
[4] [2]The child with an acute transfusion reaction is the second resuscitation emergency, and the first action is always the same, to stop the transfusion and keep the line open with saline. The airway, the breathing and the circulation are supported, the reaction is assessed for the fever-and-hypotension of haemolysis, the wheeze and the hypotension of anaphylaxis, and the breathlessness of circulatory overload, and the specific treatment follows the type. Anaphylaxis receives adrenaline, circulatory overload receives oxygen, diuretics and a slower future rate, and the suspected acute haemolytic or septic reaction receives aggressive fluid, renal support and the return of the unit to the laboratory. The child who has had any reaction is documented, reported and carefully planned for the next transfusion, with the special products and the premedication that prevent a recurrence. [2]
Management — Definitive & Stepwise
The definitive management of a child who needs a transfusion is the prescription of the correct component at the correct per-kilogram dose, and this is the core of the exam topic. Red cells are prescribed as leucodepleted packed cells at a volume of 10 to 15 mL per kilogram, run over two to four hours and never longer than four hours per unit, because the risk of bacterial growth rises beyond that window. A transfusion of 10 to 15 mL per kg typically raises the haemoglobin by about 20 to 30 g per litre, and the prescription is rounded to the nearest unit or the nearest age-appropriate pack. The red cells are matched for ABO and Rh, they are selected K-negative for girls and women of childbearing potential to prevent anti-D-forming sensitisation, and they are phenotype-matched for the child on a chronic transfusion programme to prevent alloimmunisation. [2]
Red cell transfusion in a child
Dose
Leucodepleted packed red cells at 10 to 15 mL per kg over 2 to 4 hours, raising the haemoglobin by about 20 to 30 g per litre for each 10 to 15 mL per kg, to a restrictive threshold of 70 g per litre in the stable critically ill child
Platelets are prescribed as an apheresis or pooled concentrate at a volume of 10 to 20 mL per kilogram, run over 30 to 60 minutes, and a standard paediatric dose raises the count by about 20 to 40 times ten to the nine per litre. The threshold is prophylactic at a count of 10 times ten to the nine per litre in the stable child at risk, raised to 50 times ten to the nine per litre for active bleeding, before surgery or in the neonate, and the dose is given to secure haemostasis rather than to reach a normal count. In the child with immune thrombocytopenia, platelets are reserved for the life-threatening bleed and given together with medical therapy, because the autoantibody destroys the transfused platelets within hours and a routine transfusion is both futile and wasteful. [10][3]
Platelet transfusion in a child
Dose
Apheresis or pooled platelets at 10 to 20 mL per kg over 30 to 60 minutes, raising the count by about 20 to 40 times ten to the nine per litre, to a prophylactic threshold of 10 times ten to the nine per litre or 50 with bleeding or a procedure
Fresh frozen plasma is prescribed at a volume of 10 to 15 mL per kilogram, run over 30 to 60 minutes, for the bleeding child with a deficiency of multiple clotting factors, in the disseminated intravascular coagulation, the severe liver disease and the dilutional coagulopathy of massive transfusion. It is not given to expand circulating volume, to correct an isolated raised international normalised ratio in the non-bleeding child, or to reverse warfarin, for which a prothrombin complex concentrate is preferred. Cryoprecipitate is prescribed at 5 to 10 mL per kilogram, given as one adult pool for a larger child, for the bleeding child whose fibrinogen has fallen below about 1.5 g per litre, and it raises the fibrinogen by about 1 g per litre. Both are matched by ABO where feasible, with group AB plasma the universal donor in the emergency. [2]
Fresh frozen plasma and cryoprecipitate in a child
Dose
Fresh frozen plasma at 10 to 15 mL per kg over 30 to 60 minutes for multiple clotting-factor deficiency; cryoprecipitate at 5 to 10 mL per kg, about one pool for a larger child, for a fibrinogen under 1.5 g per litre with bleeding, raising it by about 1 g per litre
The surveillance of the transfused child closes the loop, because the transfusion is a prescription that is monitored for its effect and its harm. The post-transfusion haemoglobin or count confirms the increment and guides the next dose, the iron stores are watched in the chronically transfused, and the child is reviewed for the reactions that can follow days as well as minutes. The child on a chronic transfusion programme is entered into a pathway that matches the phenotype, monitors the iron by ferritin and magnetic resonance imaging, and plans the transition to adult care. Patient blood management runs alongside, minimising the iatrogenic blood loss of sampling, correcting the iron and the nutrition, and reserving the transfusion for the indication that truly justifies it. [2][7]
Specific Subtypes & Scenarios
The neonate is the child for whom the transfusion thresholds differ most from those of the older child, and the fellow meets the neonatal evidence directly in the exam. The preterm infant on the neonatal unit is transfused red cells to a lower threshold than the older child, and the TOP trial of Kirpalani and colleagues found that a lower haemoglobin threshold was as safe as a higher one for the preterm infant, supporting a restrictive strategy that minimises donor exposure. The neonatal platelet transfusion was transformed by the PlaNeT-2 MATISSE trial of Curley and colleagues, which found that a higher platelet threshold of 50 times ten to the nine per litre caused more major bleeding and death than a lower threshold of 25, so the lower threshold is preferred. The meta-analysis of Fustolo-Gunnink and colleagues confirmed the benefit of the lower threshold, and the two-year follow-up of Moore and colleagues showed no neurodevelopmental advantage to the higher threshold. [8][9][5]
The evidence that drove the restrictive thresholds
The child on a chronic transfusion programme is the second scenario, and the lessons of thalassaemia major and sickle cell disease apply here in full. The chronically transfused child receives extended-phenotype-matched, leucodepleted red cells on a regular schedule to suppress the marrow or to prevent stroke, and every transfusion loads about 200 mg of iron that the body cannot excrete. The child is therefore entered into a pathway of iron surveillance by ferritin and magnetic resonance imaging, iron chelation once the ferritin exceeds 1000 micrograms per litre, and the anticipation of the endocrine and cardiac consequences of the iron. The fellow who prescribes a chronic transfusion prescribes the chelation and the surveillance at the same time, because the one is meaningless without the other. [2]
The immunocompromised child is the third scenario, and here the special products are the management. The child receiving chemotherapy, the stem cell transplant recipient and the child with congenital immunodeficiency receive irradiated cellular components to prevent transfusion-associated graft-versus-host disease, because their immune system cannot reject the donor white cells. The intrauterine, the neonatal and the cytomegalovirus-seronegative immunocompromised recipient receive cytomegalovirus-negative components to prevent a primary cytomegalovirus infection. The child with a history of severe allergic reaction or immunoglobulin A deficiency receives washed components to remove the offending plasma. The right product for the right child is the whole of the management in this group, and the fellow checks the special-product flag at every prescription. [2]
Complications & Pitfalls
The first and commonest complication is transfusion-associated circulatory overload, and it is the pitfall most likely to be missed because it masquerades as the underlying illness. The child develops respiratory distress, hypoxia and pulmonary oedema within six hours of the transfusion, the hydrostatic consequence of a volume given too fast or too large to a small or failing circulation, and it is commonest in the neonate, the child with cardiac or renal failure and the child transfused rapidly. The prevention is a weight-based dose, a slow rate with a diuretic for the at-risk child, and the vigilance to recognise the breathlessness early. The treatment is oxygen, sitting the child up, a diuretic and the cessation of the transfusion. [2]
[2]The second complication is the acute haemolytic transfusion reaction, and it is the pitfall that is almost always a preventable error. The child develops fever, hypotension, flank pain and disseminated intravascular coagulation within minutes of the start of an ABO-incompatible unit, the rapid intravascular lysis of the transfused red cells by preformed antibody. The cause is almost always a failure of identification, a unit hung on the wrong child, and the prevention is the rigorous two-person bedside check of the identity, the compatibility label and the unit. The treatment is to stop the transfusion at once, keep the line open with saline, support the circulation and the renal function, and return the unit to the laboratory for investigation. [2]
The third complication is transfusion-associated acute lung injury, the rare but severe immunological reaction in which donor antibodies or active lipids bind the recipient neutrophils and flood the alveoli with protein within six hours of the transfusion. The child develops hypoxia and bilateral pulmonary infiltrates without circulatory overload, the picture of acute respiratory distress syndrome, and the management is supportive, with oxygen and ventilation as needed. The prevention is the avoidance of unnecessary transfusion and, for the child who has had a reaction, the selection of plasma from male or never-pregnant donors and the avoidance of the implicated donor. [2]
The fourth complication is alloimmunisation and the refractory state, the pitfall of the chronically transfused child. The child forms antibodies against the donor red cell or platelet antigens, which makes future cross-matching harder, causes delayed haemolytic reactions, and in the platelet context renders the child refractory, with no increment after a transfusion. The prevention is the extended-phenotype matching of red cells for the child on a chronic programme, and the matching of human platelet antigen and ABO for the platelet-refractory child. The fellow who matches the phenotype from the start spares the child the refractory state later. [2]
Prognosis & Disposition
The outlook for a child who receives a correctly prescribed, matched and observed transfusion is excellent, because the modern blood supply and the restrictive philosophy together make transfusion among the safest of the high-risk procedures. The trials of three decades have shown that a restrictive strategy is as safe as a liberal one for the stable child, so the child receives fewer transfusions and therefore carries a lower cumulative risk of reaction, of alloimmunisation and of iron overload. The child who is transfused for an acute bleed recovers with the source control and the resuscitation, the child on a chronic programme lives into adulthood with the matching and the chelation, and the child with a reaction is managed and planned for the next transfusion. [7][2]
The disposition of the transfused child is shared between the prescribing team, the transfusion laboratory and the nursing staff, and the fellow coordinates the three. The prescribing team holds the indication and the threshold, the laboratory holds the group, the screen and the compatibility, and the nursing staff hold the bedside check, the observations and the recognition of the reaction. The child who is transfused in the ward or the intensive care unit is observed through the transfusion and for the hours that follow, and the child who is discharged on the day of a transfusion is advised on the symptoms of a delayed reaction. The reporting of every reaction to the haemovigilance system is the feedback that keeps the system safe. [2]
The transition of the chronically transfused child to adult care is the junction that decides whether the safe practice continues, and the fellow plans it over years. The young person is taught the diagnosis, the transfusion and the chelation schedule, the phenotype and the antibody history are handed over, and the connection to the adult haematology service is made before the transfer. The aim is a young person who reaches adult care connected to a service, who carries the knowledge of the transfusion and the iron, and who continues the safe practice into the adult years. [2]
Special Populations
The child of a family who decline blood products, most often a Jehovah Witness family, is the special population in whom the transfusion decision is also an ethical and a legal one. The fellow respects the informed refusal of the young person with capacity, works with the family on the alternatives of patient blood management, cell salvage, erythropoietin and tranexamic acid, and seeks the minimum necessary transfusion where one is unavoidable. In the life-threatening emergency in a child without capacity, where the transfusion is needed to save life or prevent serious harm and the refusal cannot be respected, the clinician treats in the best interest of the child and documents the decision carefully. The conversation is handled with respect, clarity and the involvement of the ethics and the legal teams where needed. [7]
The child in a rural or remote setting, far from the transfusion centre, is managed by the local team through shared protocols and retrieval. The local team holds the group and screen, the emergency units and the plan for the stable transfusion, and it activates the retrieval service for the major haemorrhage or the reaction it cannot manage alone. The fellow who works in such a setting values the local network, the pre-agreed massive-transfusion protocol and the cold chain that keeps the units viable, because the child who is transfused safely in the regional hospital does as well as the child who is retrieved. [2]
GIVE BLOOD
The migrant, the refugee and the child from a region of variable blood safety carries the double burden of a higher chance of an undiagnosed haemoglobinopathy and a higher chance of a transfusion-transmitted infection in their history. The fellow has a low threshold to investigate the unexplained anaemia of a child from a high-prevalence region, to screen for the irregular antibodies that may complicate cross-matching, and to weigh the safety of the local blood supply in the child who was transfused before arrival. The family with limited language or limited trust needs the transfusion plan explained with interpreter support and a clear written summary, because the adherence and the surveillance that keep the child safe depend on understanding. [2]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric transfusion is built on the trials that drove the thresholds downward and the guidelines that consolidated the doses. The TRIPICU trial of Lacroix and colleagues, published in the New England Journal of Medicine in 2007, showed that a restrictive haemoglobin threshold of 70 g per litre was as safe as a liberal threshold of 95 g per litre in stable critically ill children, and it founded the restrictive red cell strategy. The TOP trial of Kirpalani and colleagues extended the restrictive logic to the preterm infant, and the PlaNeT-2 MATISSE trial of Curley and colleagues transformed the neonatal platelet practice by showing that a lower threshold of 25 was safer than 50. The Cochrane review of Carson and colleagues, updated in 2025, confirmed that restrictive red cell thresholds are safe across the populations studied. [1][8][9][7]
TRIPICU - Lacroix 2007
Key finding
A restrictive red cell transfusion strategy, transfusing at a haemoglobin of 70 g per litre, was as safe as a liberal strategy at 95 g per litre in stable critically ill children, with no difference in multiple-organ dysfunction or outcome.
PlaNeT-2 MATISSE - Curley 2019
Key finding
In preterm neonates, a higher prophylactic platelet transfusion threshold of 50 times ten to the nine per litre resulted in more death or major bleeding than a lower threshold of 25.
TOP - Kirpalani 2020
Key finding
A lower haemoglobin transfusion threshold for preterm infants did not increase death or severe disability compared with a higher threshold, supporting a restrictive strategy in this group.
The guidelines that translate this evidence into practice differ by region, and the fellow names the one being followed. The British guideline of New and colleagues, published in the British Journal of Haematology in 2016, is the comprehensive standard for the transfusion of fetuses, neonates and older children, and it sets the per-kilogram doses, the thresholds and the special products. The AABB platelet transfusion guideline of Kaufman and colleagues sets the prophylactic platelet threshold, and the American Society of Hematology guideline of Neunert and colleagues governs the child with immune thrombocytopenia. The Australian and New Zealand practice follows the national blood service policies alongside these guidelines, and the regional access to safe, screened blood sets the ceiling of what is achievable. [2][10][3]
The chief controversy is the ratio of components in the massive-transfusion protocol and the place of whole blood in the resuscitation of the bleeding child. The balanced ratio of red cells, plasma and platelets approximates whole blood, and the use of cold-stored, low-titre group O whole blood in the pre-hospital and the trauma setting is gaining evidence in adults and is being studied in children. The fellow follows the local protocol, which defines the ratio, the tranexamic acid and the temperature and calcium management, and explains the rationale to the team. The principle is constant, the rapid restoration of oxygen, volume and haemostasis together, whatever the exact ratio. [4]
Exam Pearls
The single most testable set is the per-kilogram dose of each component, so learn it as a quartet. Red cells are 10 to 15 mL per kg over two to four hours, platelets are 10 to 20 mL per kg, fresh frozen plasma is 10 to 15 mL per kg and cryoprecipitate is 5 to 10 mL per kg. The candidate who can state these four doses, and who can pair the red cell dose with the 20 to 30 g per litre increment in haemoglobin and the platelet dose with the 20 to 40 times ten to the nine per litre increment in count, holds the prescription heart of the topic. [2]
The thresholds are the second high-yield set, and they turn on the restrictive philosophy. The restrictive haemoglobin is 70 g per litre in the stable critically ill child, the prophylactic platelet count is 10 times ten to the nine per litre, the bleeding or procedure platelet count is 50, the cryoprecipitate trigger is a fibrinogen under 1.5 g per litre, and the neonatal platelet threshold is 25 rather than 50. The candidate who can recite these thresholds, and who can name the TRIPICU and PlaNeT-2 MATISSE trials behind them, has the evidence heart of the topic. [1][9]
[9] [5]The special products and the reactions are the third high-yield set. Leucodepletion is the default, irradiation prevents graft-versus-host disease in the immunocompromised, cytomegalovirus-negative blood protects the intrauterine, neonatal and immunocompromised recipient, K-negative blood protects the girl from sensitisation, and phenotype matching prevents alloimmunisation in the chronically transfused. Transfusion-associated circulatory overload is the commonest serious reaction, the acute haemolytic reaction is the preventable never-event, and the management of any reaction begins with stopping the transfusion and keeping the line open. The candidate who holds the products, the doses, the thresholds and the safety together carries the topic. [2]
References
- [1]Lacroix J, Hebert PC, Hutchison JS Transfusion strategies for patients in pediatric intensive care units. N Engl J Med, 2007.PMID 17442904
- [2]New HV, Berryman J, Bolton-Maggs PH Guidelines on transfusion for fetuses, neonates and older children. Br J Haematol, 2016.PMID 27861734
- [3]Neunert C, Terrell DR, Arnold DM American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv, 2019.PMID 31794604
- [4]Diab YA, Wong EC, Luban NL Massive transfusion in children and neonates. Br J Haematol, 2013.PMID 23432321
- [5]Fustolo-Gunnink SF, Fijnvandraat K, van Klaveren D Preterm neonates benefit from low prophylactic platelet transfusion threshold despite varying risk of bleeding or death. Blood, 2019.PMID 31697817
- [6]Moore CM, D'Amore A, Fustolo-Gunnink S Two-year outcomes following a randomised platelet transfusion trial in preterm infants. Arch Dis Child Fetal Neonatal Ed, 2023.PMID 36810309
- [7]Carson JL, Stanworth SJ, Dennis JA Transfusion thresholds and other strategies for guiding red blood cell transfusion. Cochrane Database Syst Rev, 2025.PMID 41114449
- [8]Kirpalani H, Bell EF, Hintz SR Higher or Lower Hemoglobin Transfusion Thresholds for Preterm Infants. N Engl J Med, 2020.PMID 33382931
- [9]Curley A, Stanworth SJ, Willoughby K Randomized Trial of Platelet-Transfusion Thresholds in Neonates. N Engl J Med, 2019.PMID 30387697
- [10]Kaufman RM, Djulbegovic B, Gernsheimer T Platelet transfusion: a clinical practice guideline from the AABB. Ann Intern Med, 2015.PMID 25383671