Paeds · haematology-oncology-and-transfusion
Childhood cancer warning signs and diagnostic pathways
Also known as Childhood cancer · Paediatric malignancy · Signs of childhood cancer · Suspected cancer referral · Diagnostic delay in childhood cancer
Fellowship guide to the warning signs and diagnostic pathways of childhood cancer. Covers the rarity of childhood malignancy against a sea of benign presentations, the central principle that persistent or progressive symptoms are the red flags, the headline patterns of leukaemia, central nervous system tumours, abdominal masses, lymphadenopathy and leucocoria, the primary-care investigations and the urgent referral to a paediatric oncology centre, the diagnostic interval and the causes of delayed diagnosis, the oncologic emergencies that declare at presentation, the cancer predisposition syndromes that lower the threshold to investigate, and the global survival gap and survivorship.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child is brought back to the clinic for the third time in a month, still pale, still tired, still not right, and the temptation is to reassure the family and send them home. Childhood cancer is rare, and the individual symptoms overlap with the everyday benign illnesses of childhood, which is exactly why it is missed. The paediatric task at the front line is not to make a tissue diagnosis, it is to recognise the pattern that does not resolve, to name it a red flag, and to move the child into the urgent referral pathway before the window for curable, early-stage disease closes. [1]
Childhood cancer is the collective term for the malignant diseases of the zero-to-fourteen-year age band, with adolescents often included up to nineteen. It is biologically distinct from adult cancer, driven more by developmental errors of differentiation than by environmental carcinogenesis, and it is dominated by the haematological malignancies, the central nervous system tumours and the embryonal solid tumours rather than the epithelial carcinomas of adults. The central clinical principle is that any symptom or sign that is persistent, progressive, unexplained, or out of proportion to the expected benign course carries a small but real probability of cancer, and that probability is what justifies the referral. [2]
The survival of childhood cancer is one of the great successes of modern paediatrics, with five-year survival now exceeding eighty percent in high-income settings, but this success is entirely conditional on early diagnosis and prompt transfer to a treating centre. Globally the picture is reversed, with the majority of the world's children presenting late and dying of treatable disease, and the diagnostic pathway, not the chemotherapy, is the rate-limiting step. A clinician who internalises the warning signs and the pathway closes the gap between a curable early cancer and a lethal late one. [3]
Classification
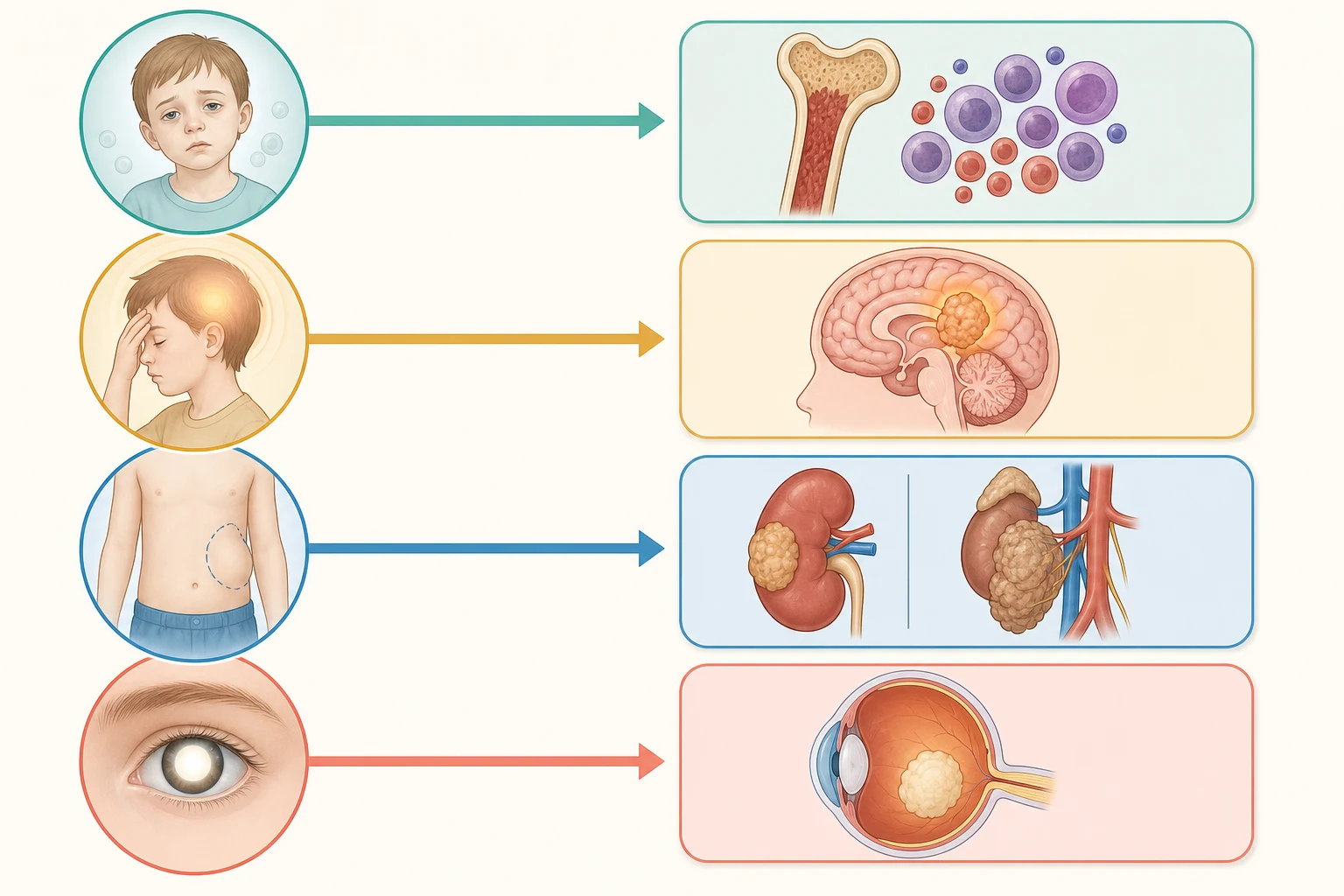
Childhood cancer is best grouped for the purposes of recognition by the tissue of origin and by the symptom complex the tumour produces, because the presenting pattern, more than the histology, is what the clinician meets first. The four headline groups are the leukaemias, the central nervous system tumours, the lymphomas, and the solid tumours, with the embryonal tumours of the kidney, the sympathetic nervous system, the eye and the soft tissues making up much of the solid-tumour burden. Each group declares itself through a recognisable cluster of warning signs. [1]
Childhood cancer groups and their presenting warning-sign patterns
The leukaemias account for roughly thirty percent of all childhood cancer, the central nervous system tumours about a quarter, the lymphomas around ten percent, and the remainder is distributed across the embryonal and the soft-tissue tumours. The order matters because it sets the prior probability when a clinician faces an undifferentiated presentation, but the discipline of the topic is to hold the rare diagnoses actively in mind whenever a symptom fails to resolve. [2]
Epidemiology & Risk Factors
The incidence of childhood cancer is around one hundred and forty to one hundred and fifty cases per million children per year, which translates to roughly one in every two hundred and eighty-five children developing cancer before the age of twenty. The absolute numbers are small against the ocean of benign childhood illness, which is the structural reason the diagnosis is delayed. The peak incidence for acute lymphoblastic leukaemia sits at two to five years, for Wilms tumour at one to five years, for neuroblastoma in the first two years of life, and for Hodgkin lymphoma and bone tumours in adolescence. [2]
Globally, an estimated four hundred thousand children up to the age of nineteen develop cancer each year, and the burden falls hardest on the low and middle income countries where nine in ten of the world's children live and where survival can be under thirty percent. The gap is not biological, it is a gap in recognition, referral, diagnostic capacity and access to treatment, and it is the reason the World Health Organization frames childhood cancer as a curable disease that is too often left uncured. [3]
The known risk factors for childhood cancer are few, because most cases arise sporadically, but the cancer predisposition syndromes materially raise the prior probability and lower the threshold to investigate. Down syndrome raises the risk of leukaemia ten to twenty-fold. Li-Fraumeni syndrome with a germline TP53 pathogenic variant predisposes to sarcomas, adrenocortical carcinoma, brain tumours and early breast cancer. Beckwith-Wiedemann syndrome predisposes to Wilms tumour and hepatoblastoma. Hereditary retinoblastoma with an RB1 variant predisposes to bilateral retinoblastoma and osteosarcoma, and neurofibromatosis type one predisposes to optic pathway glioma and other tumours. A known syndrome converts a low-probability symptom into a high-probability one. [10]
Pathophysiology
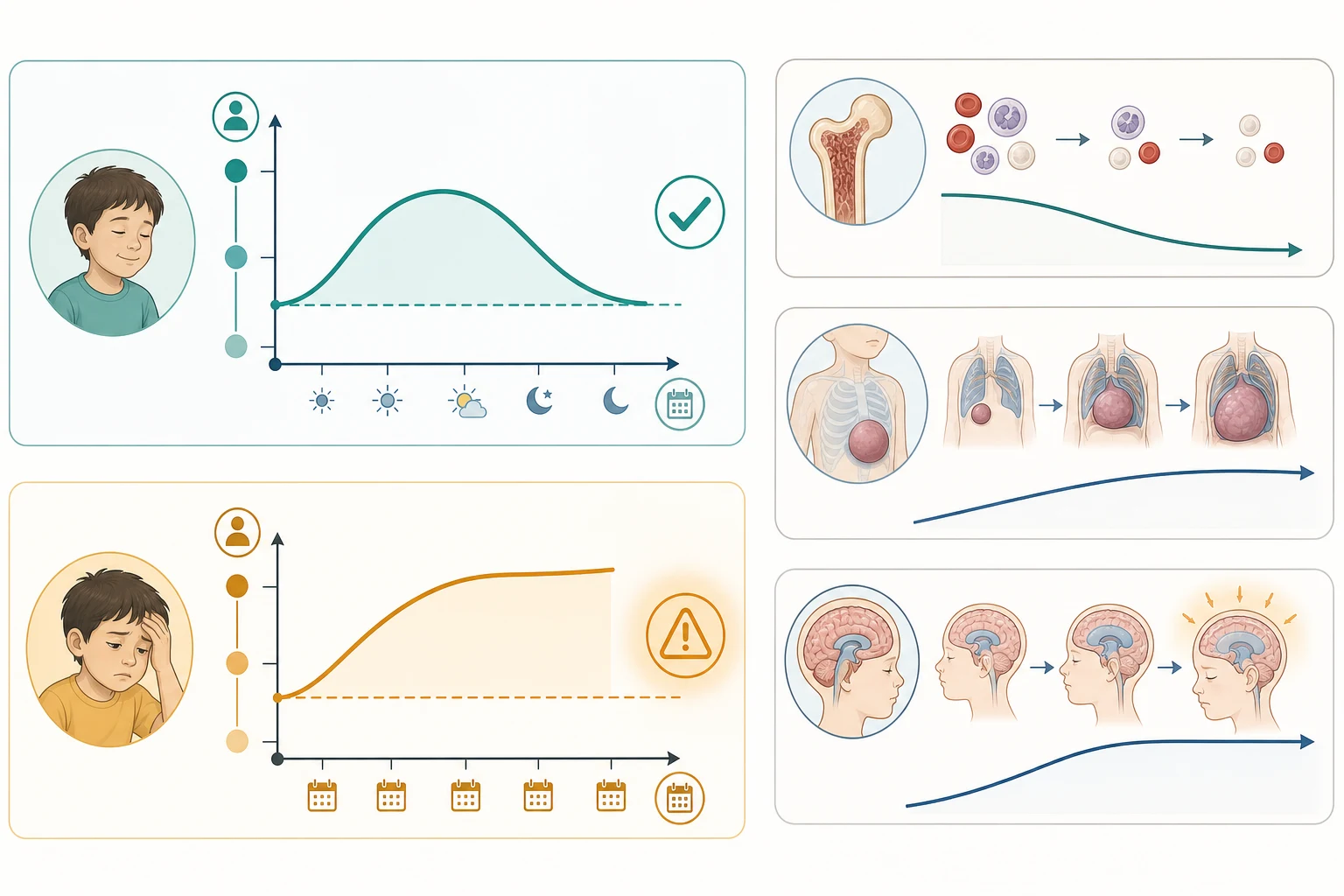
The biological principle that organises the recognition of childhood cancer is the distinction between a self-limiting process and one that is persistent or progressive. The common benign illnesses of childhood, the viral syndromes, the growing pains, the transient lymphadenopathy, run a defined course over days and resolve, whereas a malignant process accumulates. The symptom that fails to settle within the expected benign window, or that worsens week on week, is the symptom that earns investigation, and the duration threshold, rather than any single feature, is the most powerful discriminator the clinician has. [1]
The mechanism by which a tumour declares itself follows a small number of archetypes. Marrow infiltration by leukaemia or by metastatic solid tumour produces trilineage failure, with the pallor of anaemia, the bruising and petechiae of thrombocytopenia, and the fever and infection of neutropenia. A space-occupying mass produces its effect by compression, with the abdominal mass of Wilms tumour or neuroblastoma, the mediastinal mass of lymphoma compressing the airway or the superior vena cava, and the orbital or skull-base mass of neuroblastoma or sarcoma. Raised pressure within a rigid compartment produces the headache and morning vomiting of a posterior fossa tumour with hydrocephalus, or the proptosis of an orbital tumour. [1]
The hormonal and the paraneoplastic phenomena complete the picture. Neuroblastoma secretes catecholamines that produce hypertension and the classic urinary findings, and it drives the dancing-eye syndrome of opsoclonus-myoclonus-ataxia through an immune mechanism. Wilms tumour can secrete renin and present with hypertension. Retinoblastoma declares through the loss of the red reflex as the tumour fills the vitreous. Each archetype maps a pathophysiology to a bedside sign, and the clinician who knows the archetype sees the cancer behind the common complaint. [8]
Clinical Presentation
The clinical presentation of childhood cancer is built from a handful of symptom clusters, and the discipline is to ask, of every presentation, whether it has crossed the line from benign into persistent or progressive. The leukaemia cluster is the pale, bruising, febrile child with bone pain and lymphadenopathy, and the finding that converts concern into action is the full blood count with circulating blasts or a trilineage cytopenia. The duration is typically two to six weeks of worsening pallor and easy bruising, and the fever signals the neutropenia or the impending febrile neutropenia. [1]
The central nervous system cluster is the child with a progressive headache, a headache that is worse on waking, or a headache accompanied by early-morning vomiting. The accompanying signs are the papilloedema, the ataxia, the new squint, the regression in milestones or in school performance, and the abnormal eye movement. The HeadSmart principle is that a persistent or progressive headache in a child, especially with morning vomiting or a change in behaviour, is a brain tumour until imaged. The night pain, the worsening on lying flat and the failure of simple analgesia are the features that separate it from the common tension and migraine patterns. [1]
The abdominal mass cluster is the mass found by the parent at bathtime, usually painless, and the clinician must characterise it at the bedside. A Wilms tumour is a smooth, firm, flank mass that does not cross the midline in a one-to-five-year-old, while a neuroblastoma is a hard, irregular mass that frequently crosses the midline and may carry the raccoon-eye ecchymoses, the hypertension and the opsoclonus of catecholamine secretion. The lymphoma cluster is persistent painless lymphadenopathy, hard or fixed nodes, a node over two centimetres that persists beyond four weeks, night sweats and weight loss, and the mediastinal mass that may present with cough, stridor or superior vena cava obstruction. [1][8]
The eye cluster is the white pupil, the leucocoria seen by the family in a flash photograph, the new squint, or the loss of vision, and the red-reflex test is the single bedside manoeuvre that converts a parental observation into a diagnosis of retinoblastoma. The bone and soft-tissue cluster is persistent bone pain, especially pain at night that wakes the child and is unrelieved by rest, a limp that does not resolve, or a mass that keeps growing, and the threshold for imaging a soft-tissue mass is any lesion over five centimetres or one that is deep to the fascia. The general cluster of persistent unexplained fever, weight loss, night sweats and fatigue is the systemic flag that cuts across every tumour type. [1][4]
WARNING
Differential Diagnosis
The differential diagnosis of a suspected childhood cancer is the long list of benign conditions that mimic each cluster, and the task is to use the persistent-progressive principle and the targeted investigation to separate them safely. The pale, bruising child is most often iron deficiency anaemia with immune thrombocytopenia, but the circulating blasts or the trilineage cytopenia on the film make it leukaemia. The progressive headache is most often migraine or tension headache, but the morning vomiting, the papilloedema and the ataxia make it a tumour. [1]
The abdominal mass is most often a distended bladder, constipation, or an enlarged liver or spleen from infection, but the solid, non-reducing, firm mass at bathtime makes it a Wilms tumour or a neuroblastoma. The persistent lymphadenopathy is most often a reactive node from a viral or a bacterial infection, but the hard, fixed, painless node over two centimetres that persists beyond four weeks, or the supraclavicular node, makes it a lymphoma. The leucocoria is most often a cataract, Coat disease or a persistent fetal vasculature, but the family history and the ophthalmology assessment make it a retinoblastoma until excluded. [1][4]
The bone pain is most often the growing pains of early childhood, which by definition are bilateral, evening or nocturnal, and free of objective findings by day, and the distinction from a bone tumour rests on the unilateral, persistent, progressive pain, the night pain that wakes the child, the limp, and the mass. The danger is the premature closure onto the benign diagnosis, and the safety-net is the scheduled review of any child sent home with a presumed benign explanation for a symptom that could, on its persistence, be a cancer. [1]
Clinical & Bedside Assessment
The bedside assessment of a child with a suspected cancer is the structured search for the systemic and the focal features that define the cluster. The clinician measures the weight and plots it on the growth chart, because the crossing of centiles downward or the failure to gain weight is a red flag, and the height and the head circumference complete the picture. The general inspection looks for the pallor, the bruising, the petechiae, the lethargy and the cachexia, and the hands look for the finger clubbing, the pallor of the nail beds and any lymphangitis. [1]
The lymph node examination palpates the cervical, the supraclavicular, the axillary, the epitrochlear and the inguinal chains, and documents for every significant node the site, the size, the consistency, the mobility, the tenderness and the overlying skin. The node that is hard, fixed, painless, rubbery, larger than two centimetres, in the supraclavicular fossa, or persisting beyond four weeks is the node that earns referral. The abdominal examination palpates for the liver, the spleen and any mass, and characterises a mass by its size, its consistency, its mobility, whether it crosses the midline, and whether it moves with respiration, with the smooth flank mass of Wilms tumour distinguished from the hard crossed-midline mass of neuroblastoma. [1][8]
The neurological examination looks for the papilloedema on the fundoscopy, the cranial nerve deficits, the abnormal eye movements including the opsoclonus, the nystagmus and the new squint, the ataxia on the gait and the heel-to-toe walking, the focal weakness, and the regression in the milestones or the school performance. The eye examination performs the red-reflex test from a distance of around thirty centimetres in a dimmed room, looking for the white reflex of leucocoria, the asymmetry between the two eyes, and the opacity, and any abnormality is referred urgently to ophthalmology. [1][4]
Investigations
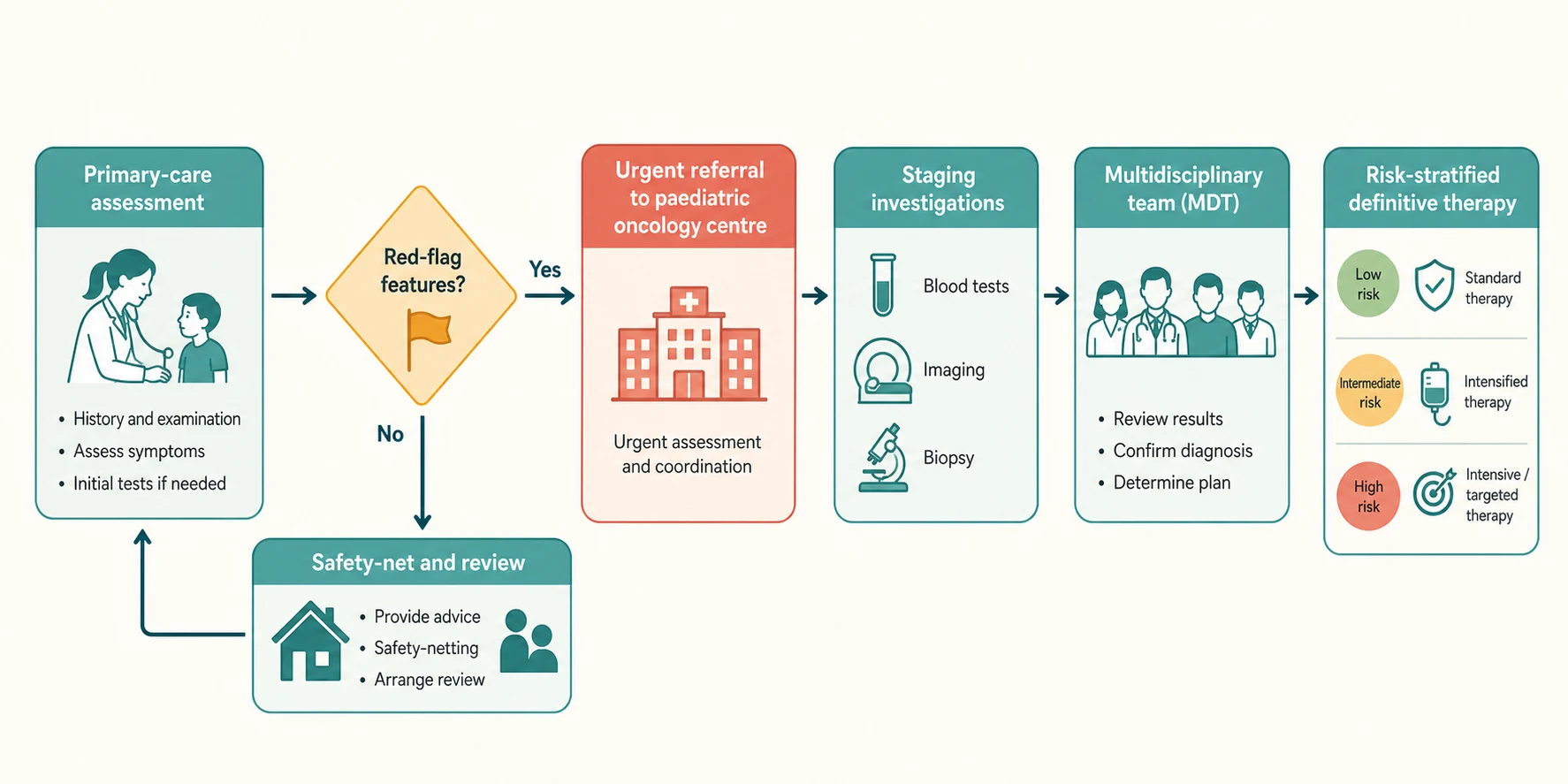
The primary-care investigation of a suspected cancer is deliberately limited, because the aim is to confirm the suspicion and to triage, not to stage the disease. The first-line panel for the pale, bruising or febrile child is the full blood count and the peripheral blood film, and the film is the single most powerful test because it shows the blasts of leukaemia or the trilineage failure of marrow infiltration. The C-reactive protein, the lactate dehydrogenase and the urate are added when a malignancy is suspected, and the lactate dehydrogenase is a marker of cell turnover that rises in the lymphomas and the high-burden tumours. [1]
The abdominal mass is assessed urgently with an ultrasound as the first imaging, which distinguishes the solid from the cystic lesion and the renal from the adrenal or the retroperitoneal origin, and the urinary catecholamines, the vanillylmandelic acid and the homovanillic acid, are sent to separate the neuroblastoma from the Wilms tumour. A suspected central nervous system tumour is imaged with a magnetic resonance imaging of the brain and the spine, with the computed tomography reserved for the acute presentation where a shunt or an emergency decompression is contemplated. A suspected bone tumour is imaged with a plain radiograph first, looking for the periosteal reaction, the sunburst pattern or the onion-skin appearance of an osteosarcoma or an Ewing sarcoma, followed by the magnetic resonance imaging. [1][8]
The definitive diagnosis, the staging and the risk stratification are the work of the paediatric oncology centre, and the primary-care role ends with the referral. The bone marrow aspirate with the flow cytometry and the cytogenetics confirms the leukaemia, the biopsy with the histology and the molecular studies confirms the solid tumour, the lumbar puncture assesses the central nervous system involvement, and the cross-sectional imaging with the computed tomography or the magnetic resonance and the functional imaging complete the staging. The clinician at the front line must not delay the referral to perform tests that the treating centre will repeat. [1]
Management — Resuscitation
The child who presents with a cancer and an oncologic emergency is resuscitated before the diagnosis is pursued, and the emergencies that declare at the presentation are the same whatever the tumour type. The fever in a child with a suspected or a known cancer is treated as febrile neutropenia until the count is known. A neutrophil count under zero point five times ten to the nine per litre with a fever over thirty-eight point three degrees Celsius, or thirty-eight degrees sustained over an hour, earns the empiric antipseudomonal beta-lactam within one hour of presentation after the blood cultures. [9]
The tumour lysis syndrome is anticipated in any high-burden or high-turnover tumour, and especially in the T-cell lymphoblastic lymphoma, the Burkitt lymphoma and the high-white-cell leukaemia. It is prevented before the chemotherapy with the hyperhydration using an isotonic fluid without potassium, the rasburicase for the high-risk child, and the four-to-six-hourly biochemistry, with the rasburicase contraindicated in the glucose-6-phosphate dehydrogenase deficiency. The child with a white cell count over one hundred times ten to the nine per litre risks the leukostasis of the brain and the lungs and needs the urgent cytoreduction. [9]
The mediastinal mass of a lymphoma that compresses the airway or the superior vena cava is an anaesthetic catastrophe, and no sedation or general anaesthesia is given until the airway is secured, because the loss of the negative intrathoracic pressure on induction can collapse the airway. The spinal cord compression from a tumour, the neuroblastoma, the lymphoma or the sarcoma, presents with the back pain, the weakness, the sensory level and the bowel and bladder dysfunction, and it is an emergency that earns the urgent imaging and the steroids to preserve the neurological function. The raised intracranial pressure from a posterior fossa tumour earns the elevation of the head of the bed, the hypertonic saline or the mannitol, and the urgent neurosurgical referral. [9]
Management — Definitive & Stepwise
The definitive management of childhood cancer is delivered in a specialist paediatric oncology centre by a multidisciplinary team, and the role of the referring clinician is the prompt recognition, the stabilisation of the emergencies, and the safe transfer. The principle of centralisation is that the outcomes are better and the survival higher when the child is treated on a national or an international protocol in a centre that sees enough volume, which is why the suspected-cancer referral is to a centre, not to a general ward. [7]
The stepwise pathway moves from the confirmation of the diagnosis, through the staging and the risk stratification, to the risk-adapted therapy. The therapy is multi-modal and combines the chemotherapy, the surgery and the radiotherapy in sequences determined by the tumour type and the protocol, with the supportive care of the transfusion, the growth factors, the infection prophylaxis and the symptom control woven through. The leukaemias and the lymphomas are treated predominantly with the chemotherapy, the central nervous system tumours with the surgery and the radiotherapy alongside the chemotherapy, and the solid tumours with the combination of the surgery and the chemotherapy, with the radiotherapy reserved for specific indications. [7]
The survivorship begins at the diagnosis, because the late effects of the treatment shape the rest of the child's life. The anthracycline cardiotoxicity, the radiation effects on the growth and the endocrine function, and the second malignancy risk are all monitored through the long-term follow-up. The fertility impairment and the neurocognitive effects of the central nervous system-directed therapy join the surveillance, and the transition from the active treatment to the survivorship clinic is a planned handover rather than a drift. The clinician who refers early gives the child the best chance not only of survival but of a life lived without the burden of avoidable late effects. [7]
Specific Subtypes & Scenarios
The specific scenarios that the candidate must hold are the presentations that are easily missed. The retinoblastoma scenario is the family who reports a white glow in the child's eye on a flash photograph, or the health visitor who notes a squint, and the red-reflex test that shows the white pupillary reflex is the finding that triggers the urgent ophthalmology referral. The median age at the presentation of retinoblastoma is under two years for the bilateral disease and slightly older for the unilateral, and the leucocoria, the new squint, the red eye or the poor vision are the modes of presentation, with the late presentation with a painful red eye or a proptosis carrying the worst prognosis. [4]
The neuroblastoma scenario is the infant with the abdominal mass that crosses the midline, the raccoon eyes of the orbital metastasis, the opsoclonus-myoclonus of the paraneoplastic syndrome, or the hypertension of the catecholamine secretion, and the urinary catecholamines confirm the diagnosis. The Wilms tumour scenario is the one-to-five-year-old with the smooth, firm, painless flank mass found at bathtime, with the hypertension and the haematuria as the occasional accompanying features. The lymphoma scenario is the older child or the adolescent with the persistent painless cervical or supraclavicular lymphadenopathy, the night sweats and the weight loss, or the younger child with the mediastinal mass and the respiratory compromise. [8]
The cancer predisposition scenario is the child whose family history or syndrome raises the prior probability of a tumour, and lowers the threshold to investigate any persistent symptom. The child with the Down syndrome who develops the pallor or the bruising has a leukaemia until excluded. The child with the Li-Fraumeni syndrome who develops a new mass or a persistent bone pain has a sarcoma or a tumour until excluded. The child with the Beckwith-Wiedemann syndrome has the scheduled abdominal ultrasound surveillance for the Wilms tumour and the hepatoblastoma, and the child with the hereditary retinoblastoma has the lifelong surveillance for the second tumours. [10]
Complications & Pitfalls
The complications of a missed or a delayed diagnosis of childhood cancer are the presentation at a later stage, the larger tumour burden, the metastatic disease, the harder and the more toxic treatment, and the lower survival. The diagnostic interval, the time from the first symptom to the diagnosis, is the measure of this delay, and it is driven by the patient and the family factors, the clinician factors, and the health-system factors. The clinician factors are the ones in the candidate's control, and they are the failure to recognise the persistent-progressive pattern, the premature reassurance, the absence of a safety-net, and the failure to follow up an abnormal result. [5][6]
The common pitfalls are the conditions misattributed to a benign cause. The leukaemia is mislabelled as the iron deficiency anaemia, the immune thrombocytopenia or the viral illness, and the film is the defence. The brain tumour is mislabelled as the migraine, the tension headache or the school avoidance, and the morning vomiting with the papilloedema is the defence. The abdominal mass is mislabelled as the constipation or the distended bladder, and the firm, non-reducing mass at bathtime is the defence. The bone tumour is mislabelled as the growing pains, the sports injury or the Osgood-Schlatter, and the unilateral, progressive, night pain with the mass is the defence. [1]
The retinoblastoma is mislabelled as the cataract or the strabismus, and the red-reflex test is the defence. The safety-netting is the structured arrangement that closes the loop, and it is the explicit scheduled review of any child sent home with a presumed benign diagnosis for a symptom that could, on its persistence, be a cancer. The clinician who sets the review, who tells the family what to watch for, and who acts on the non-resolution, is the clinician who catches the cancer early, and the clinician who relies on the single reassurance is the clinician who catches it late. [1]
Prognosis & Disposition
The prognosis of childhood cancer is dominated by the stage at the diagnosis, the biology of the tumour, and the access to the specialist treatment, and all three are improved by an early and an accurate referral. The five-year survival in the high-income settings now exceeds eighty percent across all childhood cancer combined, and it reaches above ninety percent for the standard-risk acute lymphoblastic leukaemia, but it remains under thirty percent in many low and middle income countries where the late presentation and the treatment abandonment drive the mortality. [3]
The global survival gap is the single largest inequity in paediatric oncology, and the cure-all target of the World Health Organization is built on the recognition that the childhood cancer is curable when it is recognised and treated. The pillars of the global response are the capacity building, the referral pathways, the access to the diagnostics and the essential medicines, and the abandonment-free treatment. The clinician in the high-income setting contributes through the early recognition and the survivorship, and the clinician in the low-resource setting contributes through the same early recognition against a heavier burden of competing disease. [3]
The disposition of a child with a suspected cancer is the urgent referral to the paediatric oncology centre, with the transfer arranged by the retrieval service when the child is unstable, and the communication to the family that is honest, hopeful and clear. The family is told that the suspicion is present, that the tests will be done at the centre, and that the modern treatment offers a high probability of cure, and the clinician remains the link to the family and the primary care through the treatment and the survivorship. [7]
Special Populations
The cancer predisposition syndromes are the special populations in whom the threshold to investigate is lowest and the surveillance is scheduled. The Li-Fraumeni syndrome, caused by a germline pathogenic variant in the TP53 gene, predisposes to the soft-tissue and the bone sarcomas, the adrenocortical carcinoma, the brain tumours, and the early-onset breast cancer, and it carries the scheduled whole-body and the brain surveillance into adult life. The family history of a sarcoma in childhood, a breast cancer under thirty, or an adrenocortical carcinoma in a child is the flag that raises the Li-Fraumeni possibility. [10]
The Down syndrome is the commonest chromosomal predisposition to the childhood leukaemia, with a ten-to-twenty-fold increased risk of the acute lymphoblastic and the acute myeloid leukaemia, and the transient myeloproliferative disorder of the neonate that resolves in most but that carries the risk of the later megakaryoblastic leukaemia. The child with the Down syndrome who develops the pallor, the bruising or the persistent fever has a leukaemia until the count and the film exclude it, and the surveillance of the affected neonate is the scheduled monitoring. [1]
The hereditary retinoblastoma, the Beckwith-Wiedemann syndrome, the neurofibromatosis type one and the Fanconi anaemia each carry their own tumour spectrum and their own surveillance schedule, and the child with one of these syndromes has a named pathway that the primary care and the paediatrician follow. The migrant, the refugee and the asylum-seeking child, the child in the out-of-home care, and the child in the rural and the remote setting are the populations in whom the barriers to the recognition and the referral are highest, and the proactive clinician closes the gap by lowering the threshold and by arranging the follow-up. [3]
Evidence, Guidelines & Regional Differences
The evidence base for the early recognition of childhood cancer is built on the population-based registries, the international incidence studies, and the cohort studies of the diagnostic interval. The International Incidence of Childhood Cancer study established the baseline incidence of one hundred and forty to one hundred and fifty per million per year and the dominance of the leukaemias, and it set the standard for the registry reporting that underpins the surveillance. The diagnostic interval studies demonstrated the contribution of the clinician factors to the delay and the harm, and they drove the campaigns that lowered the threshold to investigate. [2][5]
The guidelines differ by the region but share the principle of the urgent suspected-cancer referral. The Australian and the New Zealand pathway is the urgent referral to the paediatric oncology centre for any persistent, progressive or unexplained symptom with a red flag, with the primary-care investigations limited to the triage. The United Kingdom pathway is the suspected-cancer referral with the defined waiting-time targets, supported by the HeadSmart campaign for the brain tumour recognition and the public-awareness campaigns for the leukaemia and the abdominal mass. The North American pathway is the referral to the children's oncology group centre, with the primary-care anticipatory guidance. [1]
The controversies are the balance between the over-investigation of the common benign presentations and the missed diagnosis of the rare cancer, and the resolution is the disciplined application of the persistent-progressive principle and the safety-netting. The regional differences are the access to the diagnostics and the treatment, and the centralisation of the care in the specialist centres, with the survivorship and the late-effects follow-up increasingly recognised as the standard of care across all the high-income settings. The candidate who holds the global inequity alongside the local pathway has the framework for the whole topic. [3]
Exam Pearls
The high-yield facts for the exam are the ones that change a decision at the bedside. Childhood cancer is rare, with an incidence around one hundred and forty to one hundred and fifty per million per year, but it is the persistence or the progression of a symptom, not its rarity, that earns the investigation. Leukaemia is the commonest group at around thirty percent, the central nervous system tumours a quarter, and the lymphomas around ten percent. The five-year survival exceeds eighty percent in the high-income settings but is under thirty percent in much of the world, and the diagnostic pathway is the rate-limiting step. [1][3]
The red flags that must be named are the leucocoria of retinoblastoma and the progressive headache with the morning vomiting of a brain tumour. The abdominal mass of Wilms tumour or neuroblastoma and the persistent painless lymphadenopathy of a lymphoma join them. The pale and bruising child with the blasts of leukaemia and the persistent bone pain at night of a sarcoma complete the set. The primary-care investigations are the full blood count and film, the lactate dehydrogenase and urate, the abdominal ultrasound, and the urinary catecholamines, with the urgent imaging of the suspected central nervous system or bone tumour. The febrile neutropenia gets the antipseudomonal beta-lactam within one hour. [9]
Incidence and groups
The persistent-progressive principle
Red-flag clusters
Primary-care tests
Oncologic emergencies at presentation
Predisposition syndromes
The final pearls are the ones that catch the candidate who learned the headline and forgot the corner. Growing pains are bilateral, evening and free of daytime findings, and the unilateral, progressive, night pain with a mass is never a growing pain. The supraclavicular node is malignant until proven otherwise. The red-reflex test is performed at every well-child visit in the first two years. The mediastinal mass is never sedated before the airway is secured. The child with the Down syndrome and the pallor has a leukaemia until the film excludes it. The message for the exam is that the discipline of the persistent-progressive principle, the safety-net, and the urgent referral is what carries the topic from the front line to the cure. [1]
References
- [1]Fragkandrea I, Nixon JA, Panagopoulou P Signs and symptoms of childhood cancer: a guide for early recognition Am Fam Physician, 2013.PMID 23939697
- [2]Steliarova-Foucher E, Colombet M, Ries LAG International incidence of childhood cancer, 2001-10: a population-based registry study Lancet Oncol, 2017.PMID 28410997
- [3]Bhakta N, Force LM, Allemani C Childhood cancer burden: a review of global estimates Lancet Oncol, 2019.PMID 30614477
- [4]Global Retinoblastoma Study Group, Fabian ID, Abdallah E Global Retinoblastoma Presentation and Analysis by National Income Level JAMA Oncol, 2020.PMID 32105305
- [5]Vasquez L, Oscanoa M, Tello M Factors associated with the latency to diagnosis of childhood cancer in Peru Pediatr Blood Cancer, 2016.PMID 27394036
- [6]Verma N, Bhattacharya S Time to Diagnosis and Treatment of Childhood Cancer Indian J Pediatr, 2020.PMID 32056193
- [7]Erdmann F, Frederiksen LE, Bonaventure A Childhood cancer: Survival, treatment modalities, late effects and improvements over time Cancer Epidemiol, 2021.PMID 32461035
- [8]Maris JM Recent advances in neuroblastoma N Engl J Med, 2010.PMID 20558371
- [9]Prusakowski MK, Cannone D Pediatric Oncologic Emergencies Hematol Oncol Clin North Am, 2017.PMID 29078932
- [10]Frebourg T, Bajalica Lagercrantz S, Oliveira C Guidelines for the Li-Fraumeni and heritable TP53-related cancer syndromes Eur J Hum Genet, 2020.PMID 32457520