Paeds · haematology-oncology-and-transfusion
Disseminated intravascular coagulation
Also known as DIC · Consumptive coagulopathy · Defibrination syndrome · Sepsis-induced coagulopathy · Purpura fulminans · Overt DIC
Fellowship guide to disseminated intravascular coagulation in children. Covers the acquired syndrome of systemic intravascular coagulation driven by sepsis, malignancy, trauma, and the obstetric causes, the ISTH overt-disseminated intravascular coagulation score that totals the platelet count, the fibrinogen, the D-dimer, and the prothrombin time and calls overt disease at five points or more, the bleeding-and-thrombosis paradox of microvascular fibrin with platelet and factor consumption, the management that treats the underlying cause first and adds platelet, plasma, and cryoprecipitate or fibrinogen concentrate for the bleeding child at platelets under fifty times ten to the nine per litre and fresh-frozen plasma at ten to fifteen millilitres per kilogram, the role of heparin in thrombosis-dominated purpura fulminans, and the withdrawal of drotrecogin alfa in 2011.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A previously well three-year-old presents with fever and a purpuric rash that has turned into large black stellate patches on the limbs, and the blood test shows a platelet count that has halved, a prothrombin time that is prolonged, and a fibrinogen that is lower than it should be for a child this sick. This is the face of disseminated intravascular coagulation in paediatrics, and it is one of the most feared emergencies in the intensive-care unit, because the same child bleeds from every line while the skin and the digits turn ischaemic. The fellow who understands that the bleeding and the thrombosis are two faces of the one process, and who reaches first for the cause rather than for the blood bank, is the fellow who manages this well. [4][5]
Disseminated intravascular coagulation, always abbreviated DIC, is an acquired syndrome in which the coagulation system is switched on systemically throughout the circulation, rather than locally at a wound. The Scientific and Standardisation Committee of the International Society on Thrombosis and Haemostasis, in the consensus statement of Taylor and colleagues, defined it as an intravascular activation of coagulation that is no longer localised, and that arises from a clinical trigger and may cause organ damage. [1][2]
Three ideas make this topic central to the fellowship exam, and each is a deliberate principle rather than a reflex. The first is that DIC never exists alone, because it is always secondary to a trigger, and the triggers in children are sepsis, malignancy, major trauma, and the obstetric and neonatal catastrophes. The second is the scoring system, because the ISTH overt-DIC score of five points or more is the recognised way to turn a handful of abnormal blood tests into a working diagnosis. The third is the management, because the definitive treatment is to treat the cause, while the blood components and the anticoagulants are supportive measures that buy time. [3][5]
Classification
DIC is sorted in two ways, by whether it is overt and by the tempo of its course, and each sort changes the way the fellow reads the blood tests and the way the team sets the priorities. The classification that matters most for the exam is the ISTH distinction between non-overt and overt disease, because it is the one the scoring system is built on. Non-overt DIC is the early, still-compensated state in which the clotting is systemic but the body has not yet run out of platelets and factors, and the standard tests may look near-normal. Overt DIC is the decompensated state in which the consumption has outstripped the production, the platelets and the fibrinogen fall, the clotting times lengthen, and the bleeding and the thrombosis appear. [1][6]
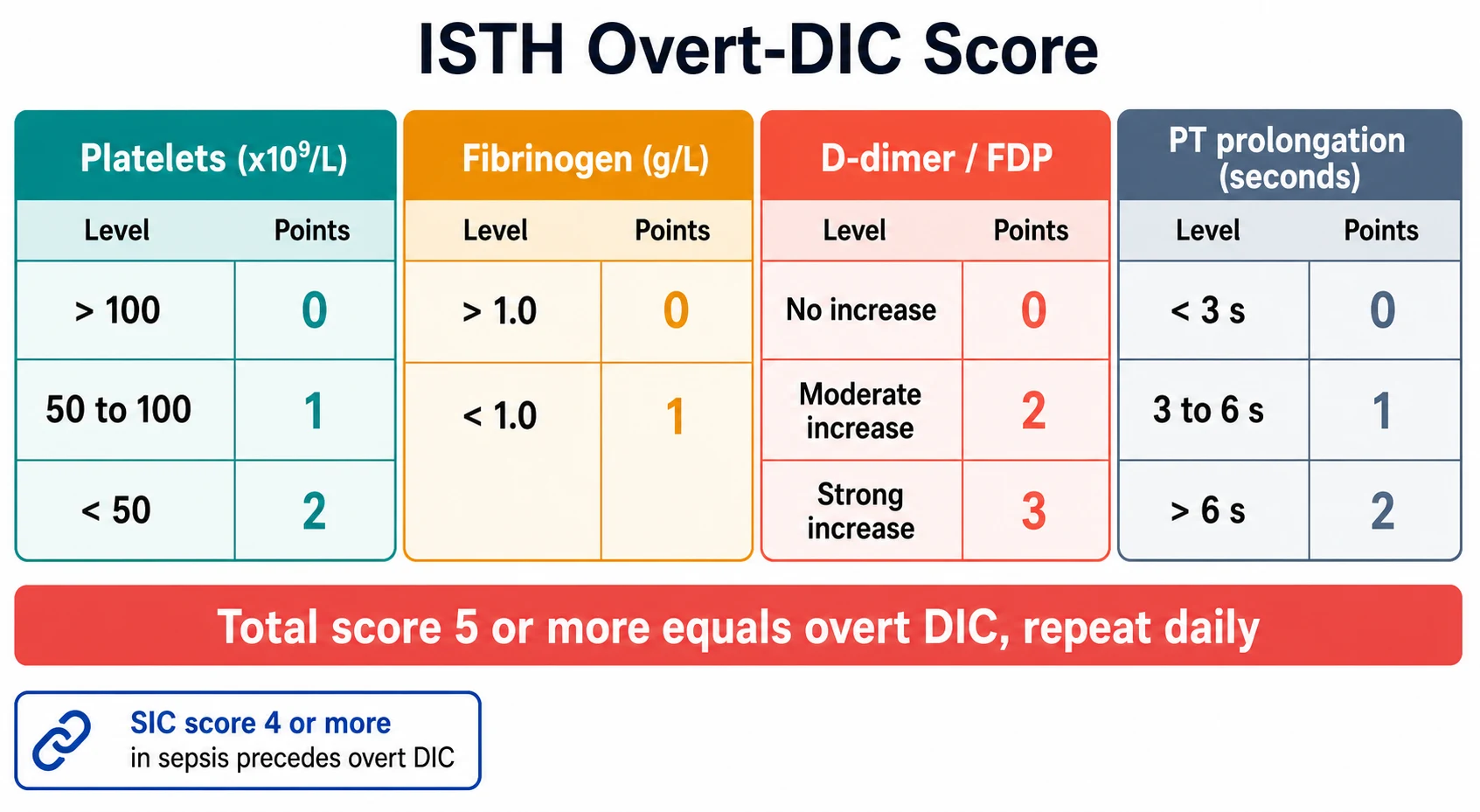
The ISTH overt-DIC score is the framework the fellow must hold cold, because it is the recognised bedside tool and it is the most testable. The score adds four numbers, and each comes from a routine test. The platelet count scores two points when it is under fifty times ten to the nine per litre, one point between fifty and one hundred, and zero above one hundred. The fibrinogen scores one point when it is under one gram per litre and zero above it. The D-dimer or the fibrin-degradation products score three for a strong rise, two for a moderate rise, and zero for no rise. The prothrombin-time prolongation scores two points above six seconds, one between three and six, and zero below three. A total of five points or more, in a child with a compatible trigger, is compatible with overt DIC, and the score is repeated daily to follow the course. [1][3]
A second scoring system, the sepsis-induced coagulopathy score of Iba and colleagues, sits upstream of the ISTH score and the fellow should know its place. It combines the platelet count, the international normalised ratio, and the organ-dysfunction score, and a total of four points or more in a child with sepsis defines sepsis-induced coagulopathy. The sepsis-induced coagulopathy state is the precursor that precedes the ISTH overt-DIC state, and Iba and colleagues showed that it predicts the high mortality that follows. The two scores are not rivals but stages on a continuum, and the fellow who reads both holds the whole course of the illness. [7][8]
The classification by tempo separates the acute, fulminant picture from the chronic, low-grade one, and the separation matters because the management differs. The acute, fulminant form is the paediatric emergency, the child with meningococcal sepsis or acute promyelocytic leukaemia who decompensates over hours, and it dominates this topic. The chronic, low-grade form is the child with a solid tumour, a large vascular anomaly such as a Kasabach-Merritt haemangioma, or a chronic aortic aneurysm, in whom the consumption is smouldering and the blood tests are mildly abnormal for weeks. The acute form is a resuscitation, and the chronic form is a diagnostic problem that resolves when the underlying lesion is treated. [4][5]
Epidemiology & Risk Factors
The incidence of DIC in children is hard to pin to a single number, because it is defined by the trigger and the population studied, but the fellow holds the pattern rather than the decimal. DIC is commonest in the paediatric intensive-care unit among children with severe sepsis and septic shock, and it is rare in the well child on the ward. Rajagopal and colleagues, in the paediatric review in Archives of Disease in Childhood, set out the triggers that dominate the paediatric picture, and they differ from the adult list in ways the fellow must know. [5]
Above all the triggers, the infection dominates the paediatric picture, and the meningococcal septicaemia is the one the fellow meets most often in the intensive-care unit. The first and the largest is infection, and in children the standout is meningococcal septicaemia, the Neisseria meningitidis that produces the purpura fulminans, followed by the pneumococcus, the gram-negative sepsis, and the severe viral infections. The second is malignancy, and the standout is acute promyelocytic leukaemia, the M3 subtype of acute myeloid leukaemia, in which DIC is present at diagnosis in the majority of children and is the chief cause of the early fatal haemorrhage. The third is massive tissue injury, the major trauma, the burns, and the heat stroke that release tissue factor in bulk. The fourth is the obstetric and neonatal group, the placental abruption, the pre-eclampsia, the birth asphyxia, and the necrotising enterocolitis that bring the neonate to DIC. [4][5]
The risk of death from DIC is high, and the fellow carries this number into the counselling of the family. The mortality sits around a quarter to a half in the severe, intensive-care cases, and it is driven more by the underlying cause than by the coagulopathy itself. The child with treatable meningococcal sepsis who receives the antibiotics and the critical care has a better outlook than the child with refractory leukaemic marrow failure, and the fellow who addresses the cause gives the child the best chance. The ISTH score and the sepsis-induced coagulopathy score both rise with the mortality, and a climbing score is a warning the fellow acts on. [3][8]
Pathophysiology
The simplest way to picture DIC is that the clotting switch is stuck on, and the whole circulation clots until the clotting factors and the platelets run out, and this picture is correct as far as it goes, but the fellowship-level answer must hold the five linked events that produce the paradox. The trigger, whether it is the bacterial endotoxin, the tissue factor from the damaged tissues, or the leukaemic blast, exposes tissue factor to the blood. The tissue factor ignites the extrinsic pathway and generates thrombin in bulk, far more than a local wound would generate. The thrombin converts fibrinogen to fibrin throughout the microvasculation, and the fibrin forms the microthrombi that block the small vessels of the kidneys, the lungs, the skin, and the brain. [4][6]
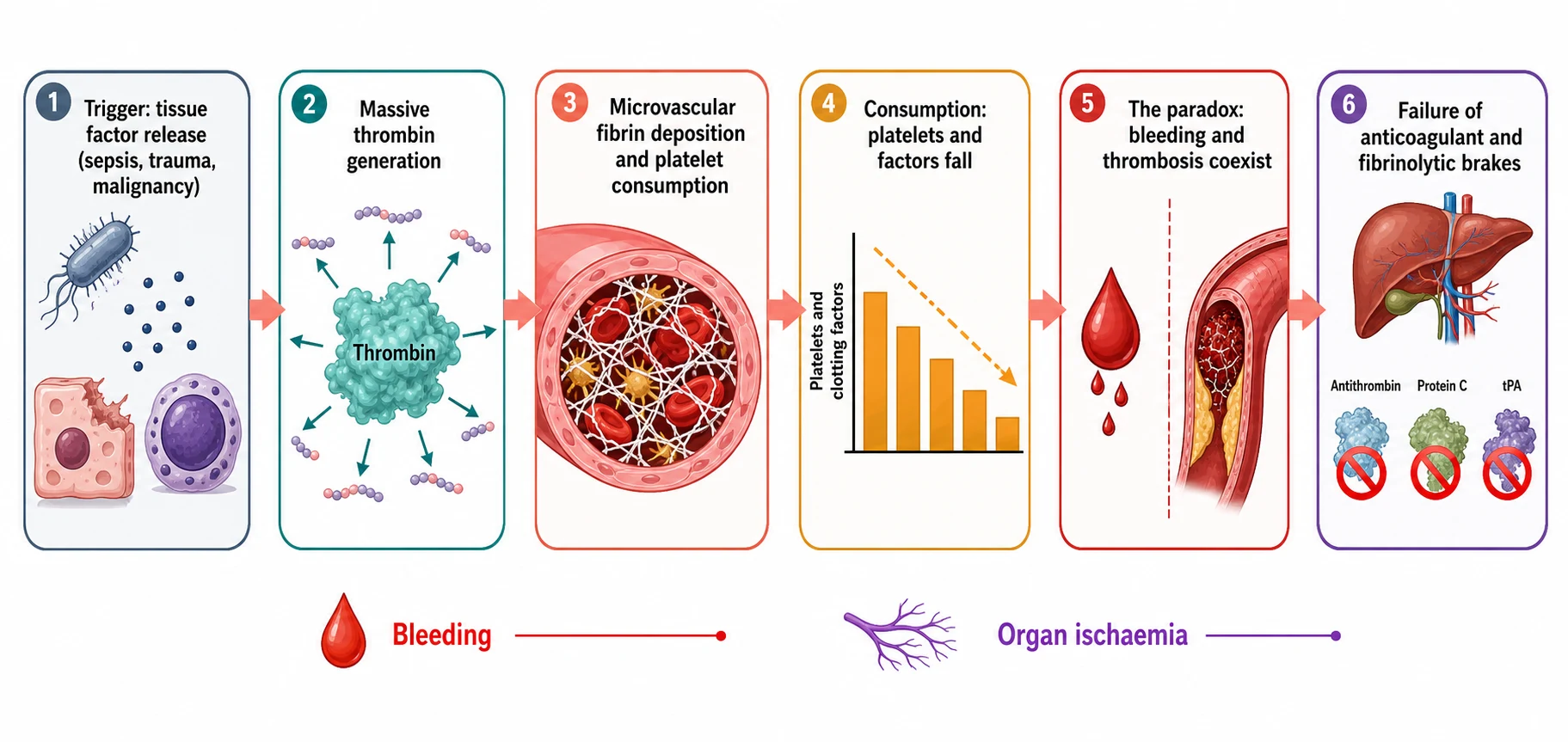
The fourth event is the consumption, and it is the event that turns the clotting into bleeding. The platelets are trapped in the microthrombi and the clotting factors are used up faster than the liver and the marrow can replace them, so the platelet count falls, the fibrinogen falls, and the prothrombin and partial thromboplastin times lengthen. The child now bleeds, from the venepuncture sites, the mucosa, the gut, and the rare but feared intracranial bleed. This is the heart of the paradox, that the same child bleeds and thromboses at once, because the consumption causes the bleeding while the microthrombi cause the organ failure. [4]
The fifth event, and the one that the modern understanding adds, is the failure of the three natural brakes that normally shut the clotting down. The antithrombin is consumed and its synthesis falls, so the thrombin runs unchecked. The protein C system fails, because the septic endothelium loses its thrombomodulin and cannot activate the protein C that would inactivate the factors five and eight. The fibrinolysis is switched off, because the injured endothelium releases the plasminogen-activator inhibitor type one that blocks the tissue plasminogen activator, so the microthrombi are not cleared. Thachil, in the review of the new pathophysiological concepts, sets out these three failures, and they are the reason the new therapies, the recombinant thrombomodulin and the antithrombin concentrate, were designed to replace the missing brakes. [6]
The endothelium is the organ that ties the five events together, because it is the endothelium that presents the tissue factor, loses the thrombomodulin, releases the plasminogen-activator inhibitor, and holds the glycocalyx that the septic injury strips away. The septic child has an endotheliopathy, and the DIC is one face of it, alongside the capillary leak and the vasoplegia. The fellow who holds the endothelium as the common thread understands why the sepsis-induced coagulopathy and the overt DIC are part of a single thrombo-inflammatory process, and not a separate clotting problem bolted onto the sepsis. [6][8]
Clinical Presentation
The child with DIC is a sick child, and the contrast with the well child who has immune thrombocytopenia is the single most important contrast the fellow makes at the bedside. The child with DIC has the features of the trigger, the fever and the rash of sepsis, the bruising and the pallor of leukaemia, or the burn and the trauma, and the coagulopathy is layered on top. The child is hypotensive, tachycardic, and peripherally shut down, and the examination shows the bleeding and the thrombosis together. [4][5]
The bleeding is the sign that brings the coagulopathy to light, and the fellow looks for it in the right places. The venepuncture sites and the central lines ooze, the gums and the nose bleed, there is blood in the gastric aspirate, the stool, or the urine, and the surgical wounds and the procedural sites reopen. The skin shows the petechiae and the purpura of the platelet lack, and the rare intracranial bleed presents with the sudden severe headache, the vomiting, and the altered consciousness that demand the immediate imaging and the combined replacement. [4]
The thrombosis is the partner sign, and the fellow who looks only for the bleeding misses the half of the picture. The skin and the digits turn ischaemic, with the cool, mottled, purplish extremities and the lines of demarcation that signal the microvascular occlusion. The purpura fulminans is the dramatic example, the large stellate purpuric lesions that turn necrotic over hours, classically in meningococcal but also in pneumococcal and severe gram-negative sepsis. The organs fail in the pattern the microthrombi produce, the acute kidney injury, the acute respiratory distress, and the hepatic dysfunction, and these are the thrombotic signs that drive the mortality. [4][5]
The child with sepsis and the bleeding-and-thrombosis paradox is recognised the same way in Australia, Aotearoa New Zealand, the United Kingdom, the United States, and Canada, and the ISTH score and the cause-driven management are followed across the English-speaking fellowship regions. The meningococcal purpura fulminans is the classic presentation in the temperate regions, while the snake bite and the severe dengue are added triggers in the tropical and the rural regions the fellow may serve. The access to the recombinant thrombomodulin and the fibrinogen concentrate varies by the health system, and the fellow checks the local formulary and the local massive-transfusion protocol before the emergency arrives. [3][5]
The chronic, low-grade DIC presents differently, and the fellow holds the contrast. The child with the Kasabach-Merritt haemangioma, the large vascular anomaly that traps the platelets, presents with the isolated thrombocytopenia and the mild coagulopathy that smoulder for weeks rather than hours. The child with the chronic disseminated malignancy shows the mildly low platelets and the raised D-dimer that the fellow picks up on the staging bloods. These children do not bleed catastrophically, and the management is the treatment of the underlying lesion, the embolisation, the resection, or the chemotherapy, rather than the resuscitation. [5]
Differential Diagnosis
The diagnosis of DIC is made in a child with a compatible trigger and a positive ISTH score, and the differential is the set of disorders that also derange the coagulation screen, each of which the fellow must separate at the bedside. The first and the most important is the isolated severe thrombocytopenia, the immune thrombocytopenia, because it also produces the bruising and the petechiae, but it leaves the clotting times and the fibrinogen normal. The separation rests on the trigger and the screen, because DIC sits in a sick child with a trigger, while immune thrombocytopenia sits in a well child after a virus. [5]
Disseminated intravascular coagulation
trigger-driven consumptive coagulopathy
- Sick child with sepsis, malignancy, trauma, or obstetric cause
- Platelets low, prothrombin time prolonged, fibrinogen low
- D-dimer strongly raised, schistocytes on the film
- ISTH overt-DIC score five points or more
Immune thrombocytopenia
isolated thrombocytopenia
- Well child one to four weeks after a viral illness
- Isolated platelet count under one hundred times ten to the nine per litre
- Normal prothrombin time, normal fibrinogen, large platelets, no schistocytes
- No trigger, no organ failure, score not applicable
Liver failure
synthetic failure
- Both prothrombin and partial thromboplastin times prolonged
- Fibrinogen low when severe, but D-dimer only mildly raised
- Abnormal liver function and the synthetic markers
- No schistocytes, no microvascular thrombosis
Vitamin K deficiency
factor deficiency
- Prolonged prothrombin time, later partial thromboplastin time
- Normal platelets, normal fibrinogen, normal D-dimer
- The exclusively breast-fed or antibiotic-treated infant
- Responds to vitamin K
The liver disease is the second trap, because the failing liver under-produces the clotting factors and the picture can mimic DIC. The failing liver shows the prolonged prothrombin and partial thromboplastin times and the low fibrinogen, but the D-dimer is only mildly raised, the schistocytes are absent, and the liver function and the synthetic markers point to the liver. The fellow who reads the D-dimer and the film, alongside the liver panel, separates the two, because the liver disease does not have the massive fibrin turnover that defines DIC. [3][6]
The vitamin K deficiency and the warfarin effect are the third group, and they are common in the breast-fed infant and the child on the long antibiotics. The vitamin K lack produces the factor two, seven, nine, and ten deficiency that prolongs the prothrombin time, but the platelets and the fibrinogen and the D-dimer are normal, and the picture resolves with the vitamin K. The massive transfusion coagulopathy is the fourth, because the child who receives the large volumes of the crystalloid and the red cells dilutes the clotting factors and the platelets, and the fellow who has the transfusion history separates the dilutional coagulopathy from the consumption. [5]
Clinical & Bedside Assessment
The assessment of the child with suspected DIC runs in parallel with the resuscitation, because the sick child is not the child who waits for the full workup. The history establishes the trigger, the fever and the rash of sepsis, the bruising of leukaemia, the trauma or the burn, and the obstetric or the neonatal catastrophe. The examination grades the shock and the organ failure, and it searches for the bleeding and the thrombosis together. The fellow looks at the venepuncture sites and the lines, the skin and the digits, the abdomen and the urine output, and the Glasgow coma score, because the DIC declares itself in the places it damages. [4][5]
The structured assessment of the child with suspected disseminated intravascular coagulation
Identify and begin to treat the trigger, the sepsis, the malignancy, or the trauma
Grade the shock and the organ failure, and start the resuscitation and the critical care
Look for the bleeding at the lines, the mucosa, the gut, and the urine
Look for the thrombosis in the skin, the digits, and the failing organs
Send the full blood count, the prothrombin and partial thromboplastin times, the fibrinogen, and the D-dimer
Calculate the ISTH overt-DIC score and repeat it daily to follow the course
The bleeding is graded by the site and the severity, because the grade drives the decision to give the blood components. The oozing line and the petechiae are mild, the mucosal and the gastrointestinal bleeding are moderate, and the uncontrolled haemorrhage and the intracranial bleed are severe. The thrombosis is graded by the extent, because the purpura fulminans and the digital ischaemia shift the plan toward the anticoagulation. The fellow who grades both the bleeding and the thrombosis holds the two faces of the process, and the grade of each sets the balance between the components and the heparin. [3]
The examination excludes the alternative diagnoses at the same time. The hepatomegaly and the splenomegaly point to the liver disease or the storage disorder, the lymphadenopathy points to the leukaemia, and the bruising disproportionate to the sepsis raises the immune thrombocytopenia. The fellow who finds the large vascular anomaly of the Kasabach-Merritt lesion, or the solid tumour, holds the chronic, low-grade DIC rather than the acute, fulminant form. The assessment is the one encounter at which the fellow sets the trigger, the grade, and the differential, and the blood tests follow from it. [5]
Investigations
The investigation of DIC rests on four core tests, and the fellow who runs them together holds the diagnosis. The full blood count shows the falling platelet count, and the blood film shows the fragmented red cells, the schistocytes, that signal the microangiopathic haemolysis. The prothrombin time and the partial thromboplastin time are prolonged, because the factors are consumed. The fibrinogen is low, and the D-dimer or the fibrin-degradation products are strongly raised, because the fibrin is turned over in bulk. The four results together, in a child with a trigger, are the diagnosis, and the ISTH score is built directly from them. [1][3]
[3] [6]The ISTH overt-DIC score is the test that turns the four results into a diagnosis, and the fellow calculates it at the bedside. The score adds the points from the platelet count, the fibrinogen, the D-dimer, and the prothrombin time, and a total of five points or more, in a child with a trigger, is compatible with overt DIC. The score is repeated daily, because the course of DIC is dynamic and the score that falls signals the recovery, while the score that climbs signals the worsening and the higher mortality. The sepsis-induced coagulopathy score is added in the septic child, and a score of four points or more defines the precursor that precedes the overt disease. [1][7]
The additional tests are selective and they support the cause and the complications. The blood culture, the lactate, and the arterial gas grade the sepsis, and the renal and the liver function grade the organ failure. The blood film is examined for the blast cells of the leukaemia, and the bone marrow aspirate is done for the leukaemia when the trigger is the malignancy. The thrombin time is prolonged, and the antithrombin level is low in the severe case, but neither changes the immediate management. The fibrinogen is followed serially, because the trend drives the cryoprecipitate and the fibrinogen concentrate, and the D-dimer is followed because the trend tracks the fibrin turnover. [3][5]
Management — Resuscitation
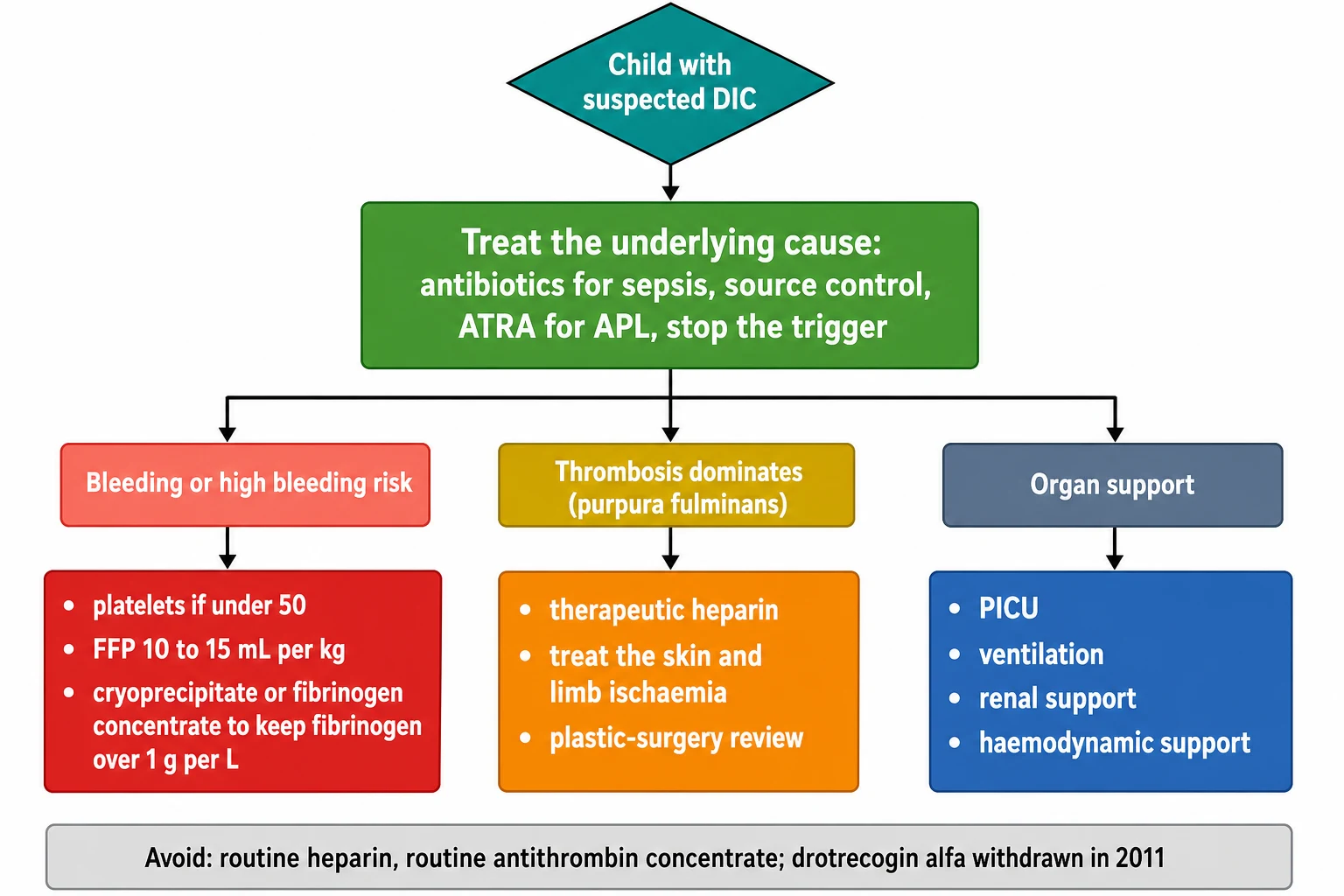
DIC is always a resuscitation when it is acute and fulminant, and the resuscitation has three concurrent aims, to treat the trigger, to support the organs, and to control the bleeding. The first and the overriding aim is to treat the trigger, because DIC does not resolve until the trigger is removed, and every other measure buys time for the cause treatment to work. The septic child receives the broad-spectrum antibiotics within the first hour, the fluid resuscitation, and the source control. The leukaemic child receives the all-trans retinoic acid for the acute promyelocytic leukaemia started immediately, and the child with the trauma and the burns receives the surgical control. [3][5]
The bleeding child receives the blood components, and the trigger for each component is the active bleeding or the high bleeding risk, not the score alone. The platelet transfusion is given to the child who bleeds with a platelet count under fifty times ten to the nine per litre, and the British Committee for Standards in Haematology guideline of Levi and colleagues sets this threshold. The fresh-frozen plasma is given at ten to fifteen millilitres per kilogram for the bleeding child with the prolonged clotting times, and the cryoprecipitate or the fibrinogen concentrate is given to hold the fibrinogen over one gram per litre. The components treat the bleeding, and they are not given prophylactically to the child who is not bleeding, because the prophylactic transfusion does not change the outcome and it carries its own volume and transfusion risks. [3]
[3]The severe or the life-threatening bleed, and the feared intracranial haemorrhage, demand the combined replacement given urgently. The platelets, the fresh-frozen plasma, and the cryoprecipitate or the fibrinogen concentrate are given together, alongside the urgent imaging and the neurosurgical and the critical-care referral, because the cost of waiting for the response to one component is the catastrophic progression of the bleed. The aim is to raise the platelet count over fifty times ten to the nine per litre and to hold the fibrinogen over one gram per litre, and the child is managed in the intensive-care setting throughout. The severe bleed is the reason the fellow holds the local massive-transfusion protocol and the rapid access to the components. [3][10]
The thrombosis-dominated picture, the purpura fulminans and the digital ischaemia, shifts the resuscitation toward the anticoagulation, and the fellow meets it with the same discipline. The unfractionated heparin is the agent the fellow reaches for, because it is titratable and it is reversible, and it is given to the child with the thrombosis-dominated course while the components and the cause treatment continue. The heparin does not replace the cause treatment or the components, and it is reserved for the thrombosis-dominated picture, because the routine heparin for the bleeding-dominated DIC is not supported by the evidence. [3][11]
Management — Definitive & Stepwise
The definitive management of DIC is the cause treatment, supported by the components and the organ support, and the stepwise plan the fellow holds runs from the cause through the bleeding to the thrombosis. The cause treatment is the first and the non-negotiable step, and it is the only step that resolves the DIC. The broad-spectrum antibiotics and the source control for the sepsis, the all-trans retinoic acid and the arsenic for the acute promyelocytic leukaemia, and the surgical control for the trauma are the definitive measures, and the fellow who treats the cause first holds the central principle that the guidelines endorse. [3][5]
[3]The blood components are the second step, and the fellow holds the indications and the doses. The platelet transfusion is given to the bleeding child under fifty times ten to the nine per litre, and the standard paediatric dose is one single-donor apheresis unit, or ten to fifteen millilitres per kilogram of the pooled platelets. The fresh-frozen plasma is given at ten to fifteen millilitres per kilogram to the bleeding child with the prolonged clotting times, and it corrects the factor deficiency. The cryoprecipitate or the fibrinogen concentrate is given to hold the fibrinogen over one gram per litre, and the fibrinogen concentrate, where available, is preferred because it carries a lower volume and a faster correction. [3][10]
Fresh-frozen plasma for the bleeding child with DIC
Dose
Ten to fifteen millilitres per kilogram intravenously, for the child with active bleeding and the prolonged prothrombin and partial thromboplastin times
Cryoprecipitate or fibrinogen concentrate for DIC
Dose
Cryoprecipitate to hold the fibrinogen over one gram per litre, or fibrinogen concentrate at the weight-based dose, for the child with active bleeding and a low fibrinogen
The anticoagulation is the third step, and the fellow holds the narrow indication and the broad caution. The unfractionated heparin is given to the thrombosis-dominated child, the purpura fulminans and the digital ischaemia, and it is given as a therapeutic infusion titrated to the partial thromboplastin time or the anti-factor ten level. The routine heparin for the bleeding-dominated DIC is not recommended, because the trials have not shown a survival benefit and the bleeding risk is real. The American College of Chest Physicians guideline on the antithrombotic therapy in children, of Monagle and colleagues, sets out the paediatric heparin dosing, and the fellow checks the local protocol. [10][11]
The antithrombin concentrate and the recombinant activated protein C are the two therapies the fellow must know as historical or unsettled, because the examiners ask about them and the wrong answer loses the marks. The antithrombin concentrate, given to replace the consumed antithrombin, has not shown a survival benefit in the controlled trials, and it is not recommended routinely. The recombinant activated protein C, the drotrecogin alfa, was withdrawn in 2011 after the PROWESS-SHOCK trial showed no benefit, and it is no longer available. The recombinant soluble thrombomodulin, the ART-123 that replaces the missing endothelial brake, is the newer agent, and the meta-analysis of Valeriani and colleagues suggested a benefit in the sepsis-associated coagulopathy with the overt DIC, though the paediatric data remain limited. [3][9]
Specific Subtypes & Scenarios
The acute promyelocytic leukaemia scenario is the one the fellow must know cold, because it carries the highest malignancy-related DIC risk and the early fatal haemorrhage. The acute promyelocytic leukaemia, the M3 subtype of the acute myeloid leukaemia, releases the procoagulant granules from the leukaemic blasts, and the DIC is present at the diagnosis in the majority of children. The bleeding, especially the intracranial bleed, is the chief cause of the early death, and the management is the immediate all-trans retinoic acid, started the moment the diagnosis is suspected, before the confirmatory marrow, alongside the components and the heparin for the thrombosis-dominated picture. The fellow who delays the all-trans retinoic acid for the marrow result exposes the child to the catastrophic early bleed. [5][6]
The purpura fulminans scenario is the second, and it is the thrombosis-dominated face of the meningococcal sepsis. The purpura fulminans presents with the large stellate purpuric lesions that turn necrotic over hours, the cool mottled extremities, and the digital ischaemia, on the background of the septic shock. The management is the components for the bleeding, the unfractionated heparin for the thrombosis, and the urgent plastic-surgical review for the skin and the limb salvage, alongside the antibiotics and the critical care. The purpura fulminans carries the high mortality, and the survivor may face the amputations and the skin grafting. [4][5]
The first twenty-four hours of a child with sepsis-induced disseminated intravascular coagulation
The Kasabach-Merritt scenario is the third, and it is the chronic, low-grade DIC of the large vascular anomaly. The Kasabach-Merritt haemangioma, the tufted angioma or the kaposiform haemangioendothelioma, traps the platelets within its vascular channels, and the child presents with the isolated thrombocytopenia and the mild coagulopathy that smoulder. The management is the treatment of the lesion, the propranolol, the sirolimus, the embolisation, or the resection, rather than the resuscitation, and the fellow involves the vascular-anomaly service early. [5]
The neonatal scenario is the fourth, and the fellow holds the neonatal triggers. The neonate with the birth asphyxia, the sepsis, the necrotising enterocolitis, the respiratory distress, or the placental abruption develops the DIC on the background of the physiologically immature neonatal haemostasis. The management follows the same principle, the cause treatment first and the components for the bleeding, with the attention to the volume and the cytomegalovirus status. The neonate is the population in which the vitamin K deficiency and the inherited factor deficiencies are also held, and the fellow runs the differential at the same time. [5][10]
Complications & Pitfalls
The first pitfall is treating the score rather than the bleeding child, and it is the error the cause-driven principle is built to correct. The fellow who transfuses the platelets and the plasma for every climbing ISTH score, regardless of the bleeding, exposes the child to the volume and the transfusion risks without the benefit, because the prophylactic transfusion does not change the outcome. The score is followed, but the transfusion is driven by the bleeding, and the fellow who holds this distinction has the central principle of the modern management. [3]
The second pitfall is missing the acute promyelocytic leukaemia, and it is the error with the highest cost. The child with the acute promyelocytic leukaemia may present with the bruising and the bleeding before the leukaemia is suspected, and the delay in the all-trans retinoic acid is the catastrophic early haemorrhage. The fellow examines the blood film for the blast cells, sends the coagulation screen, and starts the all-trans retinoic acid the moment the diagnosis is suspected, even before the confirmatory marrow, because the early treatment is the single measure that prevents the early fatal bleed. [5][6]
[3]The third pitfall is the over-use of the heparin, and the fellow who gives the routine heparin to every child with the DIC exposes the bleeding child to the worsening bleed. The heparin is reserved for the thrombosis-dominated picture, the purpura fulminans and the digital ischaemia, and the unfractionated heparin is the titratable and the reversible choice. The antithrombin concentrate, given in the hope of replacing the consumed antithrombin, is not recommended routinely, because the survival benefit has not been shown. [3][11]
The fourth pitfall is the misreading of the fibrinogen, and it is the trap that catches the team that reassures itself on one normal value. The fibrinogen is an acute-phase reactant, and it rises in the septic child, so a fibrinogen that is normal or only mildly low may already be inappropriately low. The fellow repeats the fibrinogen across the two or three samples, reads the trend, and treats the falling trend, because the single value understates the consumption. [3][6]
Prognosis & Disposition
The outlook for the child with DIC is dominated by the underlying cause, and the fellow carries this into the counselling. The mortality sits around a quarter to a half in the severe, intensive-care cases, and it is driven more by the cause than by the coagulopathy itself. The child with the treatable meningococcal sepsis, who receives the early antibiotics and the critical care, has the better outlook, while the child with the refractory leukaemic marrow failure carries the worse. The ISTH score and the sepsis-induced coagulopathy score both correlate with the mortality, and the climbing score is the warning the fellow acts on. [3][8]
The factors that predict the worse outcome are the higher ISTH score, the sepsis-induced coagulopathy score, the refractory or the multi-trigger picture, and the delay in the cause treatment. The child who reaches the intensive-care unit late, with the multiorgan failure and the climbing score, is the child at the highest risk, and the fellow who recognises the high-risk profile escalates early. The chronic, low-grade DIC of the Kasabach-Merritt lesion or the chronic tumour carries the better outlook once the underlying lesion is treated. [5][8]
The disposition of the child is shared between the intensive-care team and the haematology service, and the fellow coordinates the two. The acute, fulminant DIC is managed in the paediatric intensive-care unit, with the haematology and the cause-specialty input, and the retrieval service for the child in the rural or the remote setting. The child is discharged when the trigger is treated, the bleeding is controlled, the score has fallen, and the organ function has recovered, and the family is given the written advice on the safety-net and the follow-up. [3][10]
Special Populations
The neonate is the first special population, and the fellow holds the neonatal triggers and the neonatal haemostasis. The neonate with the birth asphyxia, the sepsis, the necrotising enterocolitis, or the placental abruption develops the DIC on the background of the physiologically immature neonatal clotting factor synthesis. The management follows the same principle, the cause treatment first and the components for the bleeding, with the attention to the volume, the cytomegalovirus status, and the lower fibrinogen baseline of the neonate. The vitamin K deficiency bleeding, the inherited factor deficiencies, and the neonatal alloimmune thrombocytopenia are the differential the fellow runs alongside the DIC. [5][10]
The child with the oncology and the immunocompromise is the second population, and the acute promyelocytic leukaemia is the standout, but the other leukaemias, the solid tumours, and the stem-cell transplant also carry the DIC and the bleeding risk. The child on the chemotherapy has the impaired marrow reserve, and the transfusion thresholds are adjusted to the bleeding and the procedural risk. The fellow coordinates with the oncology and the haematology service, and the all-trans retinoic acid for the acute promyelocytic leukaemia is the measure that prevents the early fatal bleed. [5]
DIC
The child in the rural or the remote setting is the third population, and the fellow values the retrieval service and the telehealth link. The local team holds the antibiotics, the first hour of the resuscitation, and the local component supply, and it ships the child to the intensive-care centre for the definitive care. The telehealth link to the haematology and the intensive-care service lets the local team hold the bleeding child while the retrieval is en route, and the fellow who works in the rural setting rehearses the massive-transfusion protocol before the emergency arrives. [3][10]
The child with the chronic, low-grade DIC is the fourth population, and the fellow distinguishes it from the acute, fulminant form. The Kasabach-Merritt haemangioma and the chronic tumour are managed by the treatment of the underlying lesion, the sirolimus, the embolisation, the resection, or the chemotherapy, and the resuscitation is not the issue. The fellow involves the vascular-anomaly service or the oncology service, and the coagulopathy resolves as the lesion is treated. [5]
Evidence, Guidelines & Regional Differences
The evidence base for the diagnosis and the management of DIC rests on the ISTH scoring system, the British Committee for Standards in Haematology guideline, and the sepsis-induced coagulopathy work, and the fellow who holds these three has the framework. The consensus statement of Taylor and colleagues in 2001, and the five-year overview of Toh and colleagues in 2007, established the ISTH overt-DIC score and validated it against the mortality, and it remains the bedside tool the fellow uses. The guideline of Levi and colleagues in 2009, from the British Committee for Standards in Haematology, set out the cause-driven management and the component thresholds, and it is the source the fellow quotes in the exam. [1][2][3]
ISTH overt-DIC score - Taylor 2001 and Toh 2007
Key finding
The Scientific and Standardisation Committee of the International Society on Thrombosis and Haemostasis proposed the overt-disseminated intravascular coagulation score that totals the platelet count, the fibrinogen, the D-dimer, and the prothrombin time, with a threshold of five points or more. The five-year overview confirmed that the score predicts the mortality.
BCSH guideline - Levi 2009
Key finding
The British Committee for Standards in Haematology guideline set out the cause-driven management of disseminated intravascular coagulation, with the blood components reserved for the bleeding child and the heparin reserved for the thrombosis-dominated course, and it recommended against the routine antithrombin concentrate.
The sepsis-induced coagulopathy work is the modern addition, and the fellow holds its place. Iba and colleagues, in the nationwide survey of 2017, derived the sepsis-induced coagulopathy score that combines the platelet count, the international normalised ratio, and the organ-dysfunction score, with a threshold of four points or more in the child with sepsis. The follow-up work of Iba and colleagues in 2020 showed that the sepsis-induced coagulopathy state precedes the ISTH overt-DIC state and predicts the high mortality, and it gave the fellow the upstream marker that warns before the overt disease. [7][8]
The chief controversies are the place of the heparin, the recombinant thrombomodulin, and the antithrombin concentrate, and the fellow follows the local guideline. The heparin is reserved for the thrombosis-dominated picture, because the routine heparin has not shown the survival benefit, and the review of Umemura and colleagues in 2023 set out the anticoagulant evidence. The recombinant soluble thrombomodulin, the ART-123, is the newer agent, and the meta-analysis of Valeriani and colleagues in 2020 suggested a benefit in the sepsis-associated coagulopathy with the overt DIC, though the paediatric data remain limited and the agent is not available in every region. The recombinant activated protein C, the drotrecogin alfa, was withdrawn in 2011 after the PROWESS-SHOCK trial showed no benefit, and the fellow who quotes it as current loses the marks. [3][9][11]
Exam Pearls
The single most testable fact is the definition and the ISTH score, and the fellow learns it cold. Disseminated intravascular coagulation is an acquired, trigger-driven syndrome of the systemic intravascular coagulation, and the ISTH overt-DIC score of five points or more, built from the platelet count, the fibrinogen, the D-dimer, and the prothrombin time, is the recognised diagnosis. The fellow who can state the score, the four parameters, and the five-point threshold has the diagnosis. The sepsis-induced coagulopathy score of four points or more is the precursor that precedes the overt disease. [1][7]
The cause-driven management is the second most testable fact, and it is asked as a principle. The definitive treatment is the treatment of the trigger, the antibiotics for the sepsis, the all-trans retinoic acid for the acute promyelocytic leukaemia, and the source control for the trauma. The blood components treat the bleeding, and the heparin treats the thrombosis, and neither replaces the cause treatment. The fellow who transfuses for the score, or who cannot state the cause-driven principle, loses the marks. [3]
[4] [6]The component thresholds and the doses round out the high-yield set. The platelet transfusion is for the bleeding child under fifty times ten to the nine per litre, the fresh-frozen plasma is ten to fifteen millilitres per kilogram, and the cryoprecipitate or the fibrinogen concentrate holds the fibrinogen over one gram per litre. The unfractionated heparin is reserved for the purpura fulminans. The antithrombin concentrate is not routine, the recombinant activated protein C was withdrawn in 2011, and the recombinant thrombomodulin is the newer agent with the limited paediatric data. The acute promyelocytic leukaemia is the malignancy with the highest DIC risk, and the all-trans retinoic acid is started immediately. The fellow who holds these five sets of facts carries the whole topic. [3][5][9]
References
- [1]Taylor FB Jr, Toh CH, Hoots WK, Wada H Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb Haemost, 2001.PMID 11816725
- [2]Toh CH, Hoots WK, SSC on Disseminated Intravascular Coagulation of the ISTH The scoring system of the Scientific and Standardisation Committee on Disseminated Intravascular Coagulation of the International Society on Thrombosis and Haemostasis: a 5-year overview. J Thromb Haemost, 2007.PMID 17096704
- [3]Levi M, Toh CH, Thachil J, Watson HG Guidelines for the diagnosis and management of disseminated intravascular coagulation. British Committee for Standards in Haematology. Br J Haematol, 2009.PMID 19222477
- [4]Levi M, Ten Cate H Disseminated intravascular coagulation. N Engl J Med, 1999.PMID 10451465
- [5]Rajagopal R, Thachil J, Monagle P Disseminated intravascular coagulation in paediatrics. Arch Dis Child, 2017.PMID 27540263
- [6]Thachil J Disseminated intravascular coagulation - new pathophysiological concepts and impact on management. Expert Rev Hematol, 2016.PMID 27314681
- [7]Iba T, Di Nisio M, Levy JH, Kitamura N, Thachil J New criteria for sepsis-induced coagulopathy (SIC) following the revised sepsis definition: a retrospective analysis of a nationwide survey. BMJ Open, 2017.PMID 28963294
- [8]Iba T, Arakawa M, Di Nisio M, Gando S, Thachil J Newly proposed sepsis-induced coagulopathy precedes International Society on Thrombosis and Haemostasis overt-disseminated intravascular coagulation and predicts high mortality. J Intensive Care Med, 2020.PMID 29720054
- [9]Valeriani E, Squizzato A, Gallo A, Porreca E Efficacy and safety of recombinant human soluble thrombomodulin in patients with sepsis-associated coagulopathy: a systematic review and meta-analysis. J Thromb Haemost, 2020.PMID 32237269
- [10]Monagle P, Chalmers E, Chan A, DeVeber G, Kirkham F, Massicotte P, Michelson AD Antithrombotic therapy in neonates and children: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest, 2008.PMID 18574281
- [11]Umemura Y, Nishida T, Yamakawa K, Ogura H Anticoagulant therapies against sepsis-induced disseminated intravascular coagulation. Acute Med Surg, 2023.PMID 37670904