Paeds · haematology-oncology-and-transfusion
Febrile neutropenia and infection in oncology
Also known as Febrile neutropenia · Fever in the neutropenic child · Febrile neutropenic sepsis · Chemotherapy-induced febrile neutropenia · Empiric antibiotic therapy in paediatric oncology
Fellowship guide to febrile neutropenia and infection in the child with cancer. Covers the definition of fever in neutropenia, the absolute-neutrophil-count threshold of 0.5, the blunted-inflammatory-response mechanism that makes fever the only sign of bacteraemia, and the door-to-antibiotic-in-under-sixty-minutes principle. Details the first-hour empiric bundle of blood cultures from every central-line lumen and an anti-pseudomonal beta-lactam (ceftazidime, piperacillin-tazobactam, cefepime or meropenem) with vancomycin reserved for line infection, mucositis, instability or known MRSA. Reproduces the International Pediatric Fever and Neutropenia Guideline high-risk versus low-risk stratification that sets disposition and duration, the oral step-down (ciprofloxacin plus amoxicillin-clavulanate) for selected low-risk children, the persistent-fever pathway with empiric or pre-emptive antifungal therapy, the role of granulocyte colony-stimulating factor as prophylaxis not routine treatment, the management of central-line infection and the organisms that demand line removal, and the prophylaxis and supportive-care strategy across acute myeloid leukaemia, relapsed acute lymphoblastic leukaemia and the stem-cell transplant recipient.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A six-year-old boy midway through induction for acute lymphoblastic leukaemia is brought to the emergency department with a fever to 39.0 degrees Celsius. His blood count from that morning shows an absolute neutrophil count of 0.1 times ten to the ninth per litre. He looks well and is playing. The temptation is to wait for the cultures, the temptation that kills. This is febrile neutropenia, the commonest life-threatening complication of paediatric cancer treatment, and the child is presumed bacteraemic from the moment the temperature is taken. The skill this topic teaches is the same-hour reflex: recognise the syndrome, draw blood cultures, and give the empiric antibiotic within the first hour, every time, and then use risk stratification to decide what happens next. [2]
Febrile neutropenia is defined as fever together with significant neutropenia. Fever, in the paediatric oncology convention, is a single oral or axillary temperature of 38.5 degrees Celsius or higher, or a temperature of 38.0 degrees Celsius or higher sustained over one hour. Significant neutropenia is an absolute neutrophil count under 0.5 times ten to the ninth per litre, or under 1.0 with an expected fall, as set out in the 2017 International Pediatric Fever and Neutropenia Guideline. The absolute neutrophil count is calculated from the full blood count as the white cell count multiplied by the percentage of segmented neutrophils plus bands, all divided by one hundred. These two numbers, the temperature and the absolute neutrophil count, are the only things needed to trigger the pathway. [2][1]
Why fever in this child is different from fever in any other child is the heart of the topic. Chemotherapy has emptied the neutrophil reserve, the front-line phagocyte against pyogenic bacteria and fungi, and it has broken the mucosal barrier of the gut and mouth. The organisms that live harmlessly on the skin and in the bowel now cross the damaged mucosa into the blood, and there are no neutrophils to clear them. The inflammation that usually marks an infection, the pus, the swelling, the infiltrate on the chest film, is generated by neutrophils, so in their absence the signs are blunted and the child can look deceptively well. Fever is often the only signal. That is why the reflex is to treat first and ask questions after. [1][5]
[2] [1]Classification
The only classification that changes what you do is the risk classification, because risk sets the disposition and the duration of therapy. A child is either high-risk or low-risk, and the question that sorts them is not "how sick do they look" but "do they carry any of the features that track a bad outcome". The International Pediatric Fever and Neutropenia Guideline, representing the international paediatric oncology consensus, lays out the high-risk features, and any one of them is enough. [2]
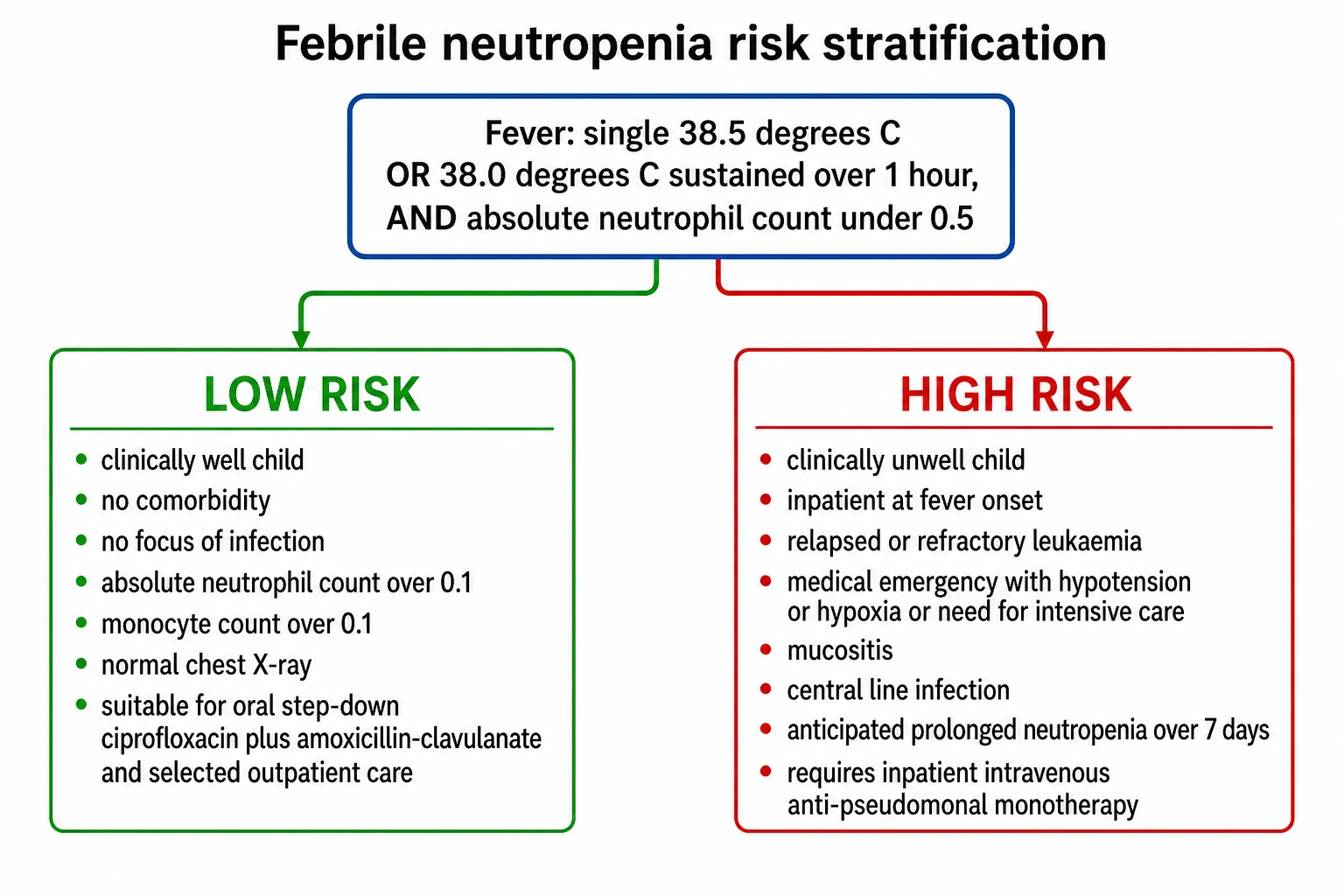
A child is high-risk if any of the following is present: the child is an inpatient at the time fever develops; the child is clinically unwell, with any sign of a significant medical emergency such as hypotension, hypoxia, or a need for critical care; the child has a comorbidity, including mucositis, impaired renal function, or impaired hepatic function; the neutropenia is anticipated to be prolonged, over seven days; the child has relapsed or refractory leukaemia; the child is on significant immunosuppression such as high-dose corticosteroids for graft-versus-host-disease; or there is a suspected serious focal infection such as a catheter infection. A child with none of these is low-risk. The split is sharp because the consequences are asymmetric: a missed high-risk child can die, while an over-treated low-risk child is merely inconvenienced. [2][6]
A second, smaller axis runs alongside the risk axis, and it is the likely source of the infection. The organisms now seen in paediatric oncology are divided between the Gram-positives, which have become the majority since central venous lines became routine, and the Gram-negatives, which carry the higher mortality. The Gram-positives include the coagulase-negative staphylococci of line infections, Staphylococcus aureus, the viridans streptococci seeded from oral mucositis, and the enterococci. The Gram-negatives include Escherichia coli, Klebsiella, Enterobacter, and the feared Pseudomonas aeruginosa. In prolonged neutropenia, the fungi Candida and Aspergillus and the mucorales join the list. Naming the organism families matters, because the empiric regimen has to cover them. [1][5]
Epidemiology & Risk Factors
Febrile neutropenia is the commonest life-threatening complication of paediatric cancer treatment. Most children receiving intensive chemotherapy for acute leukaemia will have at least one episode per induction cycle, and infection remains a leading cause of death in paediatric oncology despite modern antibiotics. The incidence tracks the intensity of the chemotherapy and the depth and duration of the neutropenia it produces, so the highest-risk windows are the induction of acute myeloid leukaemia, the intensification blocks of acute lymphoblastic leukaemia, and the pre-engraftment period of a stem-cell transplant. [5][2]
The risk factors for a severe or adverse outcome are the same features that define high-risk status. Profound neutropenia under 0.1 times ten to the ninth per litre carries more risk than a count of 0.4, and a prolonged neutropenia over seven days carries more risk than one of three days. Relapsed or refractory leukaemia, inpatient status at fever onset, mucositis, haemodynamic instability, and a recent stem-cell transplant all raise the probability of bacteraemia, intensive-care admission, and death. The prospective multicentre Swiss Paediatric Oncology Group SPOG 2003 FN study of Ammann and colleagues enrolled over a thousand episodes and quantified these as the predictors of adverse events, and it is the data backbone of contemporary risk stratification. [6]
A sobering and examinable fact is that the first-hour reflex is still not reliably delivered. The Children's Cancer and Leukaemia Group audit of Morgan and Phillips documented that a substantial fraction of UK children with febrile neutropenia did not receive their first antibiotic dose within the first hour, an avoidable failure that the audit cycle exists to close. The systematic review of Koenig and colleagues then linked the time to antibiotics to the clinical outcome, finding that a shorter interval is associated with better outcomes. An avoidable delay, in this topic, is an avoidable harm, and naming that on the viva is how the candidate shows they understand the urgency. [4][7]
Pathophysiology
The way to understand febrile neutropenia is to picture two defences failing at once in the same child. The first defence is the neutrophil, and chemotherapy empties the reserve by arresting myeloid production in the marrow. The absolute neutrophil count falls under 0.5 and often under 0.1, and because neutrophils turn over within hours, the count is a real-time read-out of an empty reservoir. The second defence is the mucosal barrier, and the same chemotherapy and conditioning regimens that suppress the marrow break the epithelium of the gut and oropharynx into the painful ulceration called mucositis. [1]
With both defences breached, the endogenous bacteria of the skin, mouth and gut, organisms a healthy child carries without symptoms, cross the damaged mucosa into the bloodstream. A coagulase-negative staphylococcus rides in through the central venous line; a viridans streptococcus seeds from the ulcerated mouth; an Escherichia coli translocates across the gut wall; a Pseudomonas aeruginosa finds a perianal crack. There are no neutrophils waiting to clear them, so the bacteria multiply, and a bacteraemia is established within hours. [1][5]
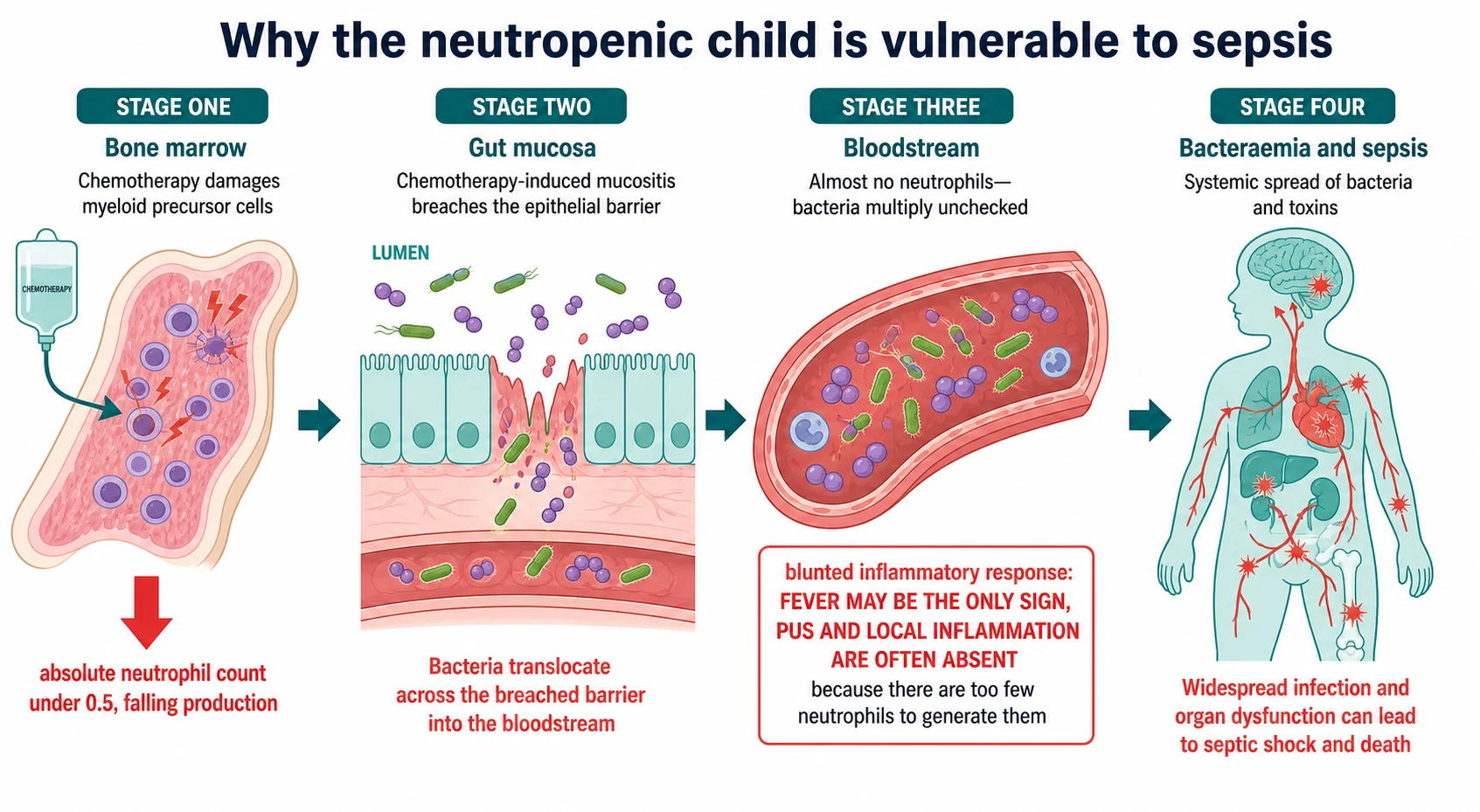
The clinical consequence of this mechanism is the central trap of the topic, and the trap that costs lives. The cardinal signs of infection, the pus, the swelling, the warmth, the infiltrate on the chest film, are all generated by neutrophils arriving at the site. When there are no neutrophils, these signs are blunted or absent. A lobar pneumonia may show no consolidation, a cellulitis may show no pus, and an abscess may show no fluctuance. The only reliable signal that a bacteraemia is brewing is the fever itself, and even the fever can be attenuated by paracetamol or by the immunosuppression of a transplant. That is why any febrile severely neutropenic child is presumed bacteraemic until proven otherwise, and why a well-looking child is never a reason to wait. [1][5]
A second consequence flows from the blunted response. The organisms that matter are the ones that exploit the empty reservoir and the broken barrier. Pseudomonas aeruginosa is feared because it can cause overwhelming sepsis and ecthyma gangrenosum within hours; the viridans streptococci are feared because they seed from oral mucositis and can trigger septic shock and the acute respiratory distress syndrome; the fungi Aspergillus and Candida are feared because they take hold in prolonged neutropenia and present only with persistent fever and an infiltrate. Knowing the mechanism tells the candidate which organisms to cover and which scenarios to anticipate. [1][11]
Clinical Presentation
The presentation is most often a single spike of fever in a child on chemotherapy for cancer, with or without a localising symptom. The parents are usually the first to notice, and they have often been told to bring the child in for any fever, which is the correct instruction. The fever meets the definition, 38.5 degrees Celsius or higher on one reading or 38.0 over an hour, and the full blood count confirms the absolute neutrophil count under 0.5. From this point the child is in the pathway. [2]
The focused search for a source is mandatory and is often revealing, because finding a source both refines the antibiotic choice and confirms the high-risk or low-risk status. Perioral pain, ulceration and dysphagia point to mucositis and to viridans streptococcal bacteraemia. Redness, tenderness or discharge at the central venous line exit site, or tenderness and induration tracking along the subcutaneous tunnel, point to a catheter infection. Perianal pain or cellulitis points to a perianal focus, and here the rule is to inspect but never to perform a rectal examination, because the instrument seeds infection into the traumatized tissue. Cough, tachypnoea and hypoxia point to pneumonia, and a new skin lesion, a black necrotic eschar or a tender erythematous nodule, can be ecthyma gangrenosum of Pseudomonas or a disseminated fungal lesion. [1][2]
The high-risk features must be sought actively and deliberately, because they change the management and because they can be subtle. Look for hypotension, a tachycardia out of proportion, a prolonged capillary refill, mottled or cool skin, an altered mental state, rigors, oliguria, and hypoxia. Any one of these makes the child high-risk and shifts the management toward inpatient intravenous therapy, early shock resuscitation, and escalation to intensive care. The absence of these signs in a child who looks well is reassuring for the low-risk designation, but it is never a reason to delay the first antibiotic. [1][6]
A presentation that is easy to miss is the afebrile but deteriorating child. In the profoundly neutropenic child, or in the child on high-dose corticosteroids for graft-versus-host-disease, the fever can be blunted or absent even with a genuine bacteraemia, and the only signs are the deterioration, the rigors, the falling saturations, or the abdominal pain of typhlitis. The lesson for the candidate is that the threshold to investigate and treat is the suspicion of infection in a neutropenic child, not the presence of a confirmatory fever. [2][5]
Differential Diagnosis
The first differential is whether the fever is from infection at all, because the child with cancer has several non-infective reasons to run a temperature. These include the tumour itself, a recent blood or platelet transfusion within the preceding 24 hours, a drug fever from agents such as bleomycin or cytarabine or from the cytokine colony-stimulating factors, a thrombotic or embolic event, and graft-versus-host-disease after a stem-cell transplant. The bedside discipline is to treat as infection first and to revise the diagnosis only with positive evidence, because missing an infection is the fatal error and the non-infective causes can be considered after the antibiotic is given. [2]
Within infection, the source is sought systematically across the body surfaces the neutrophil defends and the instrumentation breaches. The skin and the central line yield Staphylococcus aureus, the coagulase-negative staphylococci, the streptococci, Pseudomonas aeruginosa, and the atypical mycobacteria. The oropharynx and gut yield the viridans streptococci, the enterococci, the enteric Gram-negatives, and Candida. The lungs yield the pneumococci, the Gram-negatives, the respiratory viruses, Pneumocystis in the child not on co-trimoxazole prophylaxis, and the moulds in prolonged neutropenia. The urine yields Escherichia coli, Klebsiella, and Enterococcus. The perianal area yields the mixed gut flora and Pseudomonas. And the bloodstream, in roughly a third of bacteraemias, yields no identifiable focus at all. [1]
The mimic to name deliberately in the profoundly neutropenic child is invasive fungal infection. Aspergillus and the mucorales present with persistent fever, a pulmonary infiltrate or nodule with the characteristic halo sign, sinus pain or epistaxis, and skin lesions; candidiasis presents with persistent fever, hepatosplenic lesions on recovery from neutropenia, and retinal lesions on fundoscopy. These are high-risk complications that demand a different therapeutic strategy, the empiric or pre-emptive antifungal pathway, and they are the reason the persistent-fever threshold exists at 96 hours. [11][2]
Clinical & Bedside Assessment
Begin with a rapid sick-or-well assessment of airway, breathing and circulation. The febrile neutropenic child can deteriorate within minutes, and the signs of sepsis are blunted, so the assessment is brief, structured, and directed at finding the high-risk features and the source of infection. Look actively for hypotension, a tachycardia out of proportion, a prolonged capillary refill, mottled or cool peripheries, an altered mental state, hypoxia, oliguria, and rigors; any one of these makes the child high-risk and shifts the management to inpatient intravenous therapy and early shock resuscitation. [1][6]
A focused history then anchors the oncology context. Establish the underlying diagnosis, the current phase of treatment, the date of the last chemotherapy cycle and the expected neutrophil nadir, the presence and type of any central venous line, the recent transfusion history, and the prophylactic medications in use such as co-trimoxazole for Pneumocystis prophylaxis. Ask about the onset and pattern of the fever, any localising symptoms, any sick contacts, and the child's baseline performance and immune status. The chemotherapy phase matters because induction for acute lymphoblastic leukaemia and the intensification for acute myeloid leukaemia are the highest-risk windows. [2][5]
The focused examination searches for a source while protecting the child from further harm. Inspect the mouth for mucositis, grading it where the unit does so, because severe mucositis is both a source and a high-risk feature. Inspect the central venous line exit site and palpate along the tunnel for tenderness and induration, because a tunnel infection demands line removal. Inspect the skin, including the perianal area, but do NOT perform a rectal examination. Examine the chest for signs of pneumonia and the abdomen for tenderness, guarding or hepatosplenomegaly, remembering that right-lower-quadrant pain and fever in the neutropenic child can be typhlitis, a necrotising enterocolitis that is a surgical and infectious-disease emergency. Inspect the fundi if fungaemia is a possibility. [1]
[2] [6]Investigations
The investigations are sent after the blood cultures and must not delay the first antibiotic dose beyond the first hour. The blood cultures are the keystone: draw them from every lumen of any central venous line and from a peripheral site, before the antibiotic but never at the cost of the timing. The yield of a central-line culture that is two to two hours and a peripheral culture drawn at the same time lets the team later decide whether the line is the source. A urinalysis and a urine culture are sent, and a chest radiograph is taken when there are respiratory symptoms or as part of the high-risk work-up. [2][1]
The blood panel grades the neutropenia and assesses the organ function. A full blood count and differential confirms the absolute neutrophil count; the electrolytes, urea and creatinine assess renal function and guide drug dosing; the liver function tests screen for hepatic impairment, a high-risk comorbidity and a constraint on drug choice; the C-reactive protein gives a baseline to track; and a lactate detects early anaerobic sepsis and occult shock. A blood group and screen is held in case transfusion becomes necessary. These tests are processed in parallel with the antibiotic, not in series before it. [2][3]
In the high-risk child whose fever persists beyond 72 to 96 hours, the investigation escalates to look for the occult focus and the invasive fungus. Repeat the blood cultures, add a serum galactomannan assay and a beta-D-glucan for Aspergillus and other fungi, and obtain a high-resolution computed tomography of the chest and, where there are sinus symptoms, of the sinuses. A bronchoalveolar lavage is considered when there is a pulmonary lesion, and a fundoscopic examination is done to look for candidal endophthalmitis. The randomised trial of Santolaya and colleagues supports a pre-emptive strategy in which these results guide the start of antifungal therapy, rather than a blanket empirical start at a fixed hour. [11][2]
The risk stratification is then applied, using the clinical and laboratory data together. The high-risk criteria of inpatient onset, comorbidity, prolonged neutropenia and clinical instability are applied first, and the prospective SPOG 2003 FN model of Ammann and colleagues refines the prediction of bacteraemia and adverse events by adding the absolute monocyte count and other features. The point of the stratification is not academic; it sets whether the child stays on inpatient intravenous therapy for the duration of the neutropenia or steps down to oral therapy and, in selected cases, to outpatient care. [6][2]
Management — Resuscitation
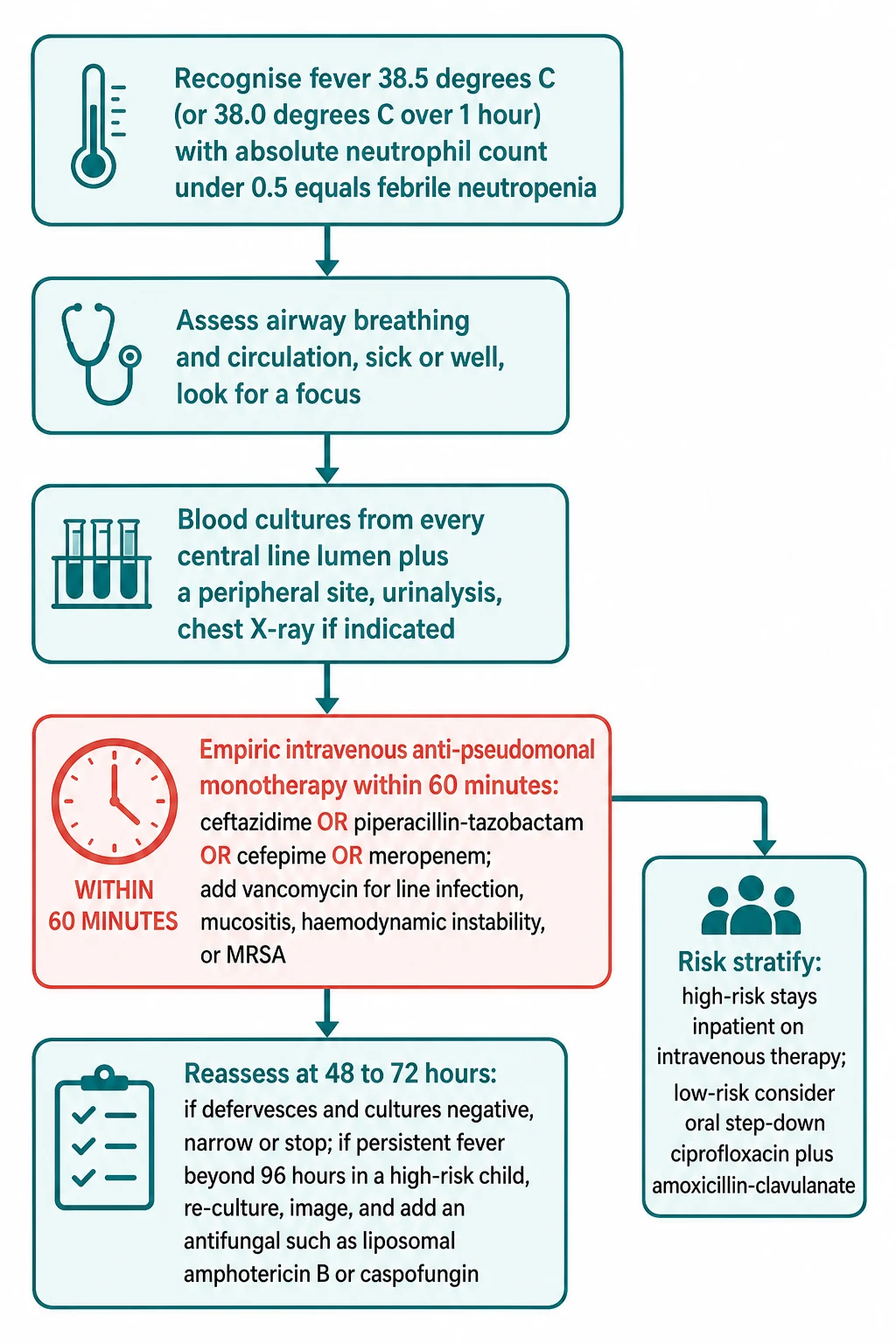
The single time-critical action is the first-hour empiric antibiotic. From the moment the syndrome is recognised, the clock is running, and the target is a door-to-antibiotic interval under sixty minutes. Recognise the fever and the neutropenia; assess the airway, breathing and circulation and look briefly for a focus and for the high-risk features; draw the blood cultures from every central-line lumen and peripherally, send the urinalysis, and take the chest film where indicated; then start the empiric intravenous anti-pseudomonal beta-lactam. The blood cultures are drawn before the dose, but they must never delay it. [2][1]
The first hour of febrile neutropenia
Recognise the syndrome: fever of 38.5 degrees Celsius or higher (or 38.0 degrees Celsius or higher over one hour) with an absolute neutrophil count under 0.5, and treat as presumed bacteraemia
Assess airway, breathing and circulation, and look briefly for a focus and for the high-risk features of hypotension, hypoxia, prolonged capillary refill and altered mental state
Draw blood cultures from every central line lumen and peripherally, send a urinalysis, and take a chest radiograph where indicated
Start empiric intravenous anti-pseudomonal monotherapy within the first hour: ceftazidime, piperacillin-tazobactam, cefepime or meropenem, weight-dosed by the oncology protocol
Add vancomycin (or teicoplanin, linezolid) only for suspected line infection, mucositis, a serious soft-tissue or pulmonary focus, haemodynamic instability, severe sepsis, or known methicillin-resistant Staphylococcus aureus
In shock, resuscitate with isotonic crystalloid boluses of 10 mL per kilogram titrated to perfusion and escalate to vasoactive support and intensive care
Risk stratify into high-risk and low-risk within the first hours, because risk sets the disposition and the duration of therapy
The standard empiric regimen is monotherapy with an anti-pseudomonal beta-lactam. The four options that cover Pseudomonas aeruginosa and the common Gram-positive and Gram-negative organisms are ceftazidime, piperacillin-tazobactam, cefepime, and meropenem, with imipenem-cilastatin as an alternative. They are given intravenously, weight-dosed by the local oncology protocol. The randomised trial of Sano and colleagues comparing piperacillin-tazobactam with cefepime monotherapy in children found both effective, and the choice between them is set by the local antibiogram and protocol. A carbapenem is preferred when there is a known or suspected resistant Gram-negative, or when the child has been on recent broad-spectrum antibiotics. [9][1]
Vancomycin is added, never substituted, when there is a defined indication. The indications are a suspected central-line infection, a serious soft-tissue or pulmonary focus, mucositis, haemodynamic instability, severe sepsis or septic shock, known colonisation with methicillin-resistant Staphylococcus aureus, or a local prevalence of resistant Gram-positive bacteraemia. Routine empiric vancomycin is not recommended, because it adds nephrotoxicity without a mortality benefit, and the stewardship principle is to add it for a reason and to stop it when the reason is gone. In shock, follow paediatric sepsis resuscitation with isotonic crystalloid boluses of 10 mL per kilogram titrated to perfusion, and escalate to vasoactive support and intensive care. [1][2]
The systematic review of Koenig and colleagues is the evidence that anchors the urgency. Pooling the available studies, the authors found that a shorter time to antibiotics is associated with better clinical outcomes in patients with fever and neutropenia during chemotherapy for cancer. The UK audit of Morgan and Phillips documented that this interval is still missed in a substantial fraction of children. The lesson for the candidate, and for the clinician, is that the first hour is not a target but a floor, and that the cultures and the panel are processed in parallel, never in series before the dose. [7][4]
Management — Definitive & Stepwise
The definitive management runs as a stepwise pathway from the first hour to discharge, and the cleanest way to hold it is as a ladder from the urgent to the de-escalated. At the top is the first-hour empiric intravenous anti-pseudomonal beta-lactam after the cultures, with vancomycin added for the defined indications. Below that is the risk stratification that sets the disposition and the duration. Below that is the reassessment at 48 to 72 hours that decides the step-down. At the bottom is the persistent-fever pathway and the antifungal decision, and the supportive-care strategy that prevents the next episode. [1][2]
[1] [2]The first step, the first-hour empiric antibiotic, has already been described. The second step is the risk stratification, applied within the first hours, because risk sets the disposition and the duration. The high-risk child is admitted, or remains an inpatient, on broad-spectrum intravenous monotherapy for the duration of the neutropenia, continuing at least until the child is afebrile and the absolute neutrophil count is recovering above 0.5 and rising. The low-risk child, by contrast, is the candidate for step-down oral therapy and, in carefully selected cases, for outpatient care. [2][6]
The third step is the reassessment at 48 to 72 hours. A child who defervesces, has negative cultures, and is low-risk can step down to oral therapy, with ciprofloxacin plus amoxicillin-clavulanate as the standard combination, or cefixime as an alternative, and in carefully selected and well-observed low-risk children may complete the course as an outpatient. The systematic review and meta-analysis of Teuffel and colleagues found that outpatient management of selected low-risk children is safe, with low rates of complications, provided the selection is rigorous and the safety-net of rapid re-presentation is real. The framework of Morgan and Phillips applies the antimicrobial-duration principle: narrow or stop when the cultures are negative and the child has recovered, and continue only as long as the indication persists. [12][3]
The fourth step addresses the high-risk child whose fever persists beyond 72 to 96 hours. Re-examine the child, repeat the blood cultures, image for a hidden focus, and add an empiric antifungal agent, with liposomal amphotericin B, an echinocandin such as caspofungin, or voriconazole as the options. Alternatively, follow a pre-emptive strategy in which the galactomannan, the beta-D-glucan, and the computed-tomography findings guide the start of a targeted antifungal, an approach supported by the randomised trial of Santolaya and colleagues in high-risk children. If a source is identified, narrow therapy to the organism and the site, and if a line infection persists or a line-demanding organism is grown, remove the line. [11][2]
The supportive-care strategy runs in parallel and is what prevents the next episode. Maintain meticulous oral hygiene with regular tooth brushing and antiseptic mouthwash to limit the mucositis that seeds viridans streptococci. Care for the central venous line with a strict aseptic technique. Avoid rectal examinations, rectal temperatures and suppositories, and avoid non-steroidal anti-inflammatory drugs that mask the fever and impair platelet function in a child who may be thrombocytopenic. Give antimicrobial prophylaxis to the highest-risk populations, as supported by the systematic review of Egan and colleagues, which found that antibiotic prophylaxis reduces the incidence of febrile neutropenia and bacteraemia in patients with cancer and stem-cell transplant recipients, with fluoroquinolones such as levofloxacin in the deepest-neutropenia groups and co-trimoxazole for Pneumocystis prophylaxis in all on chemotherapy. [10][1]
Granulocyte colony-stimulating factor has a precise and limited role. It is not used routinely for the treatment of established febrile neutropenia, because the evidence does not support a routine mortality benefit. The Cochrane review of Mhaskar and colleagues supports its use as primary prophylaxis in chemotherapy regimens with a high expected rate of febrile neutropenia, reducing the rate of febrile neutropenia and the infection-related mortality, and it is a considered adjunct in the high-risk child with pneumonia, invasive fungal infection, hypotension, or an expected prolonged profound neutropenia. Naming its correct role, prophylaxis in high-risk regimens and a considered adjunct, is how the candidate avoids the common error of reaching for it routinely. [8]
Specific Subtypes & Scenarios
The high-risk child is the archetype and the one the viva most often presents. The features that confer high risk are inpatient onset, clinical instability, comorbidity such as mucositis or renal or hepatic impairment, prolonged neutropenia over seven days, relapsed or refractory leukaemia, significant immunosuppression, or a serious focal infection. This child is managed as an inpatient on broad-spectrum intravenous monotherapy for the duration of the neutropenia, with vancomycin added where indicated and with the threshold low for the persistent-fever pathway and the antifungal escalation. [2][6]
The low-risk child is the candidate for the de-escalated pathway. Defined as clinically well, with none of the high-risk features, an absolute neutrophil count typically over 0.1 and a monocyte over 0.1 times ten to the ninth per litre, and a normal chest radiograph, this child can step down to oral ciprofloxacin plus amoxicillin-clavulanate after an initial period of observation, and in carefully selected and well-observed cases can complete the course as an outpatient. The systematic review and meta-analysis of Teuffel and colleagues underpins the safety of the outpatient option, provided the selection is rigorous, the observation is reliable, and the safety-net is real. The rural or remote child who would be managed as an outpatient low-risk must instead be admitted, because the safety-net of rapid re-presentation is absent. [12][2]
The central-line infection is its own scenario and the one that tests the candidate on line removal. A simple exit-site infection often clears with systemic antibiotics and local care, but a tunnel infection, a port-pocket abscess, or a catheter-related bloodstream infection that persists beyond 72 hours of appropriate antibiotics requires line removal. The same is true for bacteraemia with certain organisms that are poorly cleared through a line: Staphylococcus aureus, Pseudomonas aeruginosa, Candida, Bacillus, the atypical mycobacteria, and the vancomycin-resistant enterococci. The decision to remove a line is a combined surgical and infectious-diseases decision, and naming the organisms that demand it is the high-yield detail. [1]
Viridans streptococcal bacteraemia is an increasingly common and dangerous scenario, seeded from the ulcerated mouth in a child with mucositis. It can progress within hours to septic shock and the acute respiratory distress syndrome, and it is the reason meticulous oral hygiene and prompt empiric cover are part of management. The stem-cell transplant recipient in the pre-engraftment period is the highest-risk subtype of all, with a prolonged profound neutropenia of two weeks or more compounded by the cellular and humoral defects of the conditioning and the graft-versus-host-disease prophylaxis; this is a child for whom the threshold for broad empiric therapy and for antifungal cover is lowest and the duration longest. [2][5]
Complications & Pitfalls
The acute complications are the complications of uncontrolled sepsis in an undefended host. Septic shock, the acute respiratory distress syndrome (notably with viridans streptococcal and Pseudomonas aeruginosa bacteraemia), and invasive fungal infection in prolonged neutropenia are the principal ones, alongside line-related complications such as tunnel infection and septic thrombophlebitis, and organ dysfunction from the infection itself or from the nephrotoxic and hepatotoxic supportive drugs. Typhlitis, a neutropenic enterocolitis, presents with right-lower-quadrant pain and fever and is managed medically with bowel rest and broad-spectrum antibiotics, with surgery reserved for perforation. [1][2]
The principal pitfall, and the one that costs lives and exam marks, is delay. Drawing extensive investigations before giving the first antibiotic, waiting for a confirmatory count, or underestimating a well-looking child, are all variations of the same error, and the systematic review of Koenig and colleagues shows that a shorter time to antibiotics tracks better outcomes. The UK audit of Morgan and Phillips documented that this delay remains common in real practice. The second pitfall is over-reliance on appearance, because the blunted inflammatory response means that afebrile does not mean well and well does not mean safe. [7][4]
The third pitfall is adding vancomycin routinely when it should be reserved for the defined indications, a stewardship error that adds nephrotoxicity and selects for resistance. The fourth is performing a rectal examination or inserting a rectal suppository in the neutropenic child, which seeds infection into the traumatized tissue. The fifth is using a non-steroidal anti-inflammatory drug for the fever, which masks the only reliable vital sign and impairs platelet function in a child who may be thrombocytopenic. The sixth is missing a persistent low-grade fever that hides an invasive mould, and the seventh is failing to remove a central line when an organism or a tunnel infection demands it. [1][2]
[1] [2]Prognosis & Disposition
Prognosis is set by the risk stratification and by the organism. The low-risk febrile neutropenic child has an excellent prognosis, with low rates of bacteraemia and very low mortality, and is the population in whom step-down oral therapy and carefully selected outpatient management are safe. The systematic review and meta-analysis of Teuffel and colleagues supports the safety of the outpatient option in this group, provided the selection is rigorous. [12][6]
The high-risk child carries a measurable mortality that rises with shock, prolonged profound neutropenia, invasive fungal infection, and an organism such as Pseudomonas aeruginosa or a viridans streptococcus in shock. The prospective SPOG 2003 FN study of Ammann and colleagues quantified the predictors of an adverse outcome, including the depth of the neutropenia, the monocyte count, the inpatient status, and the comorbidity, and it is the basis for the contemporary risk model. The child with relapsed leukaemia or a recent stem-cell transplant sits at the worst end of the prognostic curve. [6]
Disposition follows the risk. Every child is admitted initially for the first-hour bundle and observation, because the first hours are when the deterioration happens. The high-risk child stays on inpatient intravenous monotherapy for the duration of the neutropenia, continuing at least until afebrile and recovering. The low-risk child who defervesces, has negative cultures, and has reliable follow-up can step down to oral therapy and, in selected cases, complete the course at home with a clear safety-net to return for any new fever, rigors, or clinical deterioration. The supportive-care strategy of prophylaxis, oral hygiene, line care, and the family-centred safety-netting is what closes the loop and prevents the next admission. [2][3]
Special Populations
The stem-cell transplant recipient is the highest-risk special population, and the one whose management tests the candidate's grasp of the depth of immunocompromise. The conditioning regimen produces a prolonged profound neutropenia of two weeks or more, and the graft-versus-host-disease prophylaxis and any acute graft-versus-host-disease add profound cellular and humoral immune defects on top. The threshold for empiric broad-spectrum therapy is lowest, the duration is longest, and the threshold for the antifungal pathway is lowest, because the invasive fungi take hold in this exact window. [2][10]
The child with acute myeloid leukaemia is at higher risk than the child with acute lymphoblastic leukaemia, because both the disease and the intensive induction produce deeper and more prolonged neutropenia and more mucositis. This is a population in whom antibacterial prophylaxis with a fluoroquinolone such as levofloxacin is supported by the systematic review of Egan and colleagues, which found that antibiotic prophylaxis reduces the incidence of febrile neutropenia and bacteraemia in patients with cancer and stem-cell transplant recipients, with the benefit concentrated in the deepest-neutropenia groups. Co-trimoxazole for Pneumocystis prophylaxis is standard across the leukaemias and the transplant population. [10][5]
The neonate and the infant with cancer are managed with weight-dosed antibiotics and close attention to volume, glucose and thermoregulation, and the smaller circulating volume makes the fluid resuscitation tighter and the escalation to intensive care earlier. The adolescent is engaged directly in adherence to the prophylaxis, the line care, and the safety-net, because the failure mode in this age group is often behavioural. The child from a rural or remote setting who would otherwise be a low-risk outpatient candidate is instead admitted, because the safety-net of rapid re-presentation is absent; this is a regional-equity issue, not a biological one. The child with known multidrug-resistant colonisation is managed with a locally tailored empiric regimen that covers the resistant organism, in consultation with the infectious-diseases team. [1][2]
Evidence, Guidelines & Regional Differences
The evidence base is anchored by two guideline documents and a set of systematic reviews. The International Pediatric Fever and Neutropenia Guideline update of Lehrnbecher and colleagues, the work of the International Pediatric Fever and Neutropenia Guideline Panel, sets the contemporary paediatric definition of fever in neutropenia, the high-risk and low-risk stratification, and the empiric management framework, and it is the primary reference the candidate should cite. The Infectious Diseases Society of America guideline of Freifeld and colleagues, written for adults and children together, sets the empiric monotherapy framework and the indications for vancomycin, and it is the secondary reference. [2][1]
The risk-prediction evidence rests on the prospective multicentre SPOG 2003 FN study of Ammann and colleagues. The timing-outcome evidence rests on the systematic review of Koenig and colleagues and the UK audit of Morgan and Phillips. The outpatient low-risk evidence rests on the systematic review and meta-analysis of Teuffel and colleagues, and the antimicrobial-duration framework on the review of Morgan and Phillips. The empiric-agent comparison rests on the randomised trial of Sano and colleagues comparing piperacillin-tazobactam with cefepime. The antifungal evidence rests on the randomised trial of Santolaya and colleagues comparing pre-emptive with empirical therapy, the prophylaxis evidence on the systematic review of Egan and colleagues, and the colony-stimulating-factor evidence on the Cochrane review of Mhaskar and colleagues. [6][7][4][12][3][9][11][10][8]
In Australia and Aotearoa New Zealand, febrile neutropenia is managed at the paediatric oncology centres under protocols aligned with the International Pediatric Fever and Neutropenia Guideline. The first-hour empiric anti-pseudomonal monotherapy is the standard, with ceftazidime, piperacillin-tazobactam, cefepime or meropenem chosen by the local antibiogram, and vancomycin added for the defined indications. The high-risk child is admitted for the duration of the neutropenia, the low-risk child is considered for oral step-down, and the rural and remote child is admitted rather than managed as an outpatient because the safety-net of rapid re-presentation is absent. Antimicrobial prophylaxis is delivered to the acute myeloid leukaemia, the relapsed acute lymphoblastic leukaemia, and the stem-cell transplant populations, and co-trimoxazole for Pneumocystis is standard across the chemotherapy regimens. Indigenous, Pacific, and migrant populations are supported with attention to travel, accommodation, and culturally safe communication through the family-centred oncology services.
The regional differences are real and examinable. The United Kingdom follows the Children's Cancer and Leukaemia Group pathway, with the audit of Morgan and Phillips documenting the persistent challenge of delivering the antibiotic within the first hour. The United States follows the Infectious Diseases Society of America framework. All share the first-hour antibiotic principle, and the live controversy is whether low-risk selected children should be managed as outpatients and whether a pre-emptive antifungal strategy guided by galactomannan and computed tomography should replace a blanket empirical antifungal start at a fixed hour of persistent fever. The evidence of Santolaya and colleagues supports the pre-emptive approach in high-risk children, and it is shifting practice. [4][11]
Exam Pearls
Febrile neutropenia is fever of 38.5 degrees Celsius or higher (or 38.0 degrees Celsius or higher sustained over one hour) in a child with an absolute neutrophil count under 0.5 times ten to the ninth per litre; the absolute neutrophil count is the white cell count times the percentage of segmented neutrophils plus bands divided by one hundred. The single most-tested action is empiric intravenous anti-pseudomonal monotherapy within the first hour, after blood cultures from every central-line lumen and peripherally: ceftazidime, piperacillin-tazobactam, cefepime or meropenem, with vancomycin added only for suspected line infection, mucositis, instability, severe sepsis, or known methicillin-resistant Staphylococcus aureus. [1][2]
FIRST-AID
High-risk means inpatient onset, clinical instability, comorbidity, prolonged neutropenia over seven days, relapsed or refractory leukaemia, significant immunosuppression, or a serious focal infection; low-risk is none of these, and it is the candidate for oral step-down with ciprofloxacin plus amoxicillin-clavulanate and, in selected cases, outpatient care. The feared organisms are Pseudomonas aeruginosa for its mortality, the viridans streptococci for shock and the acute respiratory distress syndrome from mucositis, and Aspergillus and Candida for persistent fever in prolonged neutropenia. Never perform a rectal examination, take a rectal temperature, give a rectal suppository, or give a non-steroidal anti-inflammatory in the neutropenic child. [2][12]
Persistent fever beyond 96 hours in a high-risk child means re-culture, image for an occult focus, and add or pre-emptively target an antifungal with liposomal amphotericin B, caspofungin or voriconazole. Granulocyte colony-stimulating factor is for prophylaxis in high-risk regimens and a considered adjunct, never a routine treatment of established febrile neutropenia. The line-removal organisms are Staphylococcus aureus, Pseudomonas aeruginosa, Candida, Bacillus, the atypical mycobacteria, and the vancomycin-resistant enterococci, alongside any tunnel infection or catheter-related bacteraemia persisting beyond 72 hours. [11][8][1]
[1] [7] [2] [1]References
- [1]Freifeld AG, Bow EJ, Sepkowitz KA, et al Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america. Clin Infect Dis, 2011.PMID 21258094
- [2]Lehrnbecher T, Robinson P, Fisher B, et al Guideline for the Management of Fever and Neutropenia in Children With Cancer and Hematopoietic Stem-Cell Transplantation Recipients: 2017 Update. J Clin Oncol, 2017.PMID 28459614
- [3]Morgan JE, Phillips B, Haeusler GM, et al Optimising Antimicrobial Selection and Duration in the Treatment of Febrile Neutropenia in Children. Infect Drug Resist, 2021.PMID 33833534
- [4]Morgan JE, Phillips B Winter 2017 Children's Cancer and Leukaemia Group febrile neutropenia audit. Arch Dis Child, 2018.PMID 29705724
- [5]Haeusler GM, Sung L Management of fever and neutropenia in paediatric cancer patients: room for improvement? Curr Opin Infect Dis, 2015.PMID 26381997
- [6]Ammann RA, Bodmer N, Hirt A, et al Predicting adverse events in children with fever and chemotherapy-induced neutropenia: the prospective multicenter SPOG 2003 FN study. J Clin Oncol, 2010.PMID 20231680
- [7]Koenig C, Schneider U, Corapcioglu F, et al Association of time to antibiotics and clinical outcomes in patients with fever and neutropenia during chemotherapy for cancer: a systematic review. Support Care Cancer, 2020.PMID 31264188
- [8]Mhaskar R, Redzepovic G, Kumar A, et al Colony-stimulating factors for chemotherapy-induced febrile neutropenia. Cochrane Database Syst Rev, 2014.PMID 25356786
- [9]Sano H, Kobayashi R, Suzuki D, et al Comparison between piperacillin/tazobactam and cefepime monotherapies as an empirical therapy for febrile neutropenia in children with hematological and malignant disorders: a prospective, randomized study. Pediatr Blood Cancer, 2015.PMID 25251104
- [10]Egan G, Hoenigl M, Haeusler GM, et al Efficacy of antibiotic prophylaxis in patients with cancer and hematopoietic stem cell transplantation recipients: A systematic review of randomized trials. Cancer Med, 2019.PMID 31274245
- [11]Santolaya ME, Salgado C, Makrides M, et al Efficacy of pre-emptive versus empirical antifungal therapy in children with cancer and high-risk febrile neutropenia: a randomized clinical trial. J Antimicrob Chemother, 2018.PMID 30010931
- [12]Teuffel O, Ethier MC, Alibhai SM, et al Outpatient management of cancer patients with febrile neutropenia: a systematic review and meta-analysis. Ann Oncol, 2011.PMID 21363878