Paeds · haematology-oncology-and-transfusion
Full blood count and blood-film interpretation in children
Also known as Paediatric full blood count · Paediatric haemogram · Blood film interpretation in children · Paediatric FBC interpretation · Age-specific blood count ranges
A fellowship approach to reading the full blood count and blood film in a child: children are not small adults, so every parameter is read against age-specific ranges, the physiological anaemia of infancy is kept in mind, the mean cell volume sorts the anaemias, and a short list of blood-film findings triggers an urgent haematology or oncology referral.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A full blood count lands on your screen. The haemoglobin is flagged low, the mean cell volume is small, and the platelet count looks odd. Before you reach for a diagnosis, ask three questions. Whose blood is this — a neonate, a toddler, an adolescent — because the normal range moves more across childhood than most clinicians remember? Does the picture fit the child in front of you, or is the number an artefact? And does anything on the film demand action today? [1] [4]
This page owns the interpretation logic for the paediatric haemogram and blood film. It pairs with the disease-specific leaves: iron deficiency and the anaemias, immune thrombocytopenia, sickle cell disease, and the presentation of childhood leukaemia. The point here is the reading of the count, not the management of each disease — but a few film findings demand an emergency response, and those are named explicitly below. [5] [8]
R.E.A.D. the paediatric haemogram
Overview & Definition
Picture two reports side by side. One belongs to a healthy six-week-old breastfed infant, the other to a fifteen-year-old girl. Both carry a haemoglobin of 105. On adult ranges the teenager is anaemic and the infant looks dire; on paediatric ranges the infant is normal and the teenager is mildly anaemic. The same number means opposite things. That is the entire reason a paediatric interpretation exists as a distinct skill. [1] [2]
The full blood count, or haemogram, measures the cellular components of blood — haemoglobin, red cell count and indices such as the mean cell volume, the total white cell count with a differential, and the platelet count. The modern automated analyser also produces derived numbers such as the red cell distribution width and flags populations it cannot classify. Celkan frames the haemogram as the single most informative bedside blood test in paediatrics, because one sample carries information about oxygen carriage, host defence, clotting and marrow health at once. [4]
The blood film is the manual examination of a stained peripheral smear. It is not redundant in the age of automation; it is the arbitrator. Automated analysers count cells and flag abnormalities, but they cannot reliably identify a blast, a sickle cell or a schistocyte, and they are fooled by clumped platelets and abnormal red cell shapes. Courville and colleagues, in a systematic review, confirmed that automated criteria detect many smear abnormalities but miss clinically important morphology, so a flagged or discordant result is an indication for a human review of the film. [8]
The decisive interpretive principle is that a value is only meaningful against the right age band, read with the film, and matched to the child. A flagged number alone is not a diagnosis. [1] [4]
Classification
Sort the abnormal count in two moves, not twenty. [4] [6]
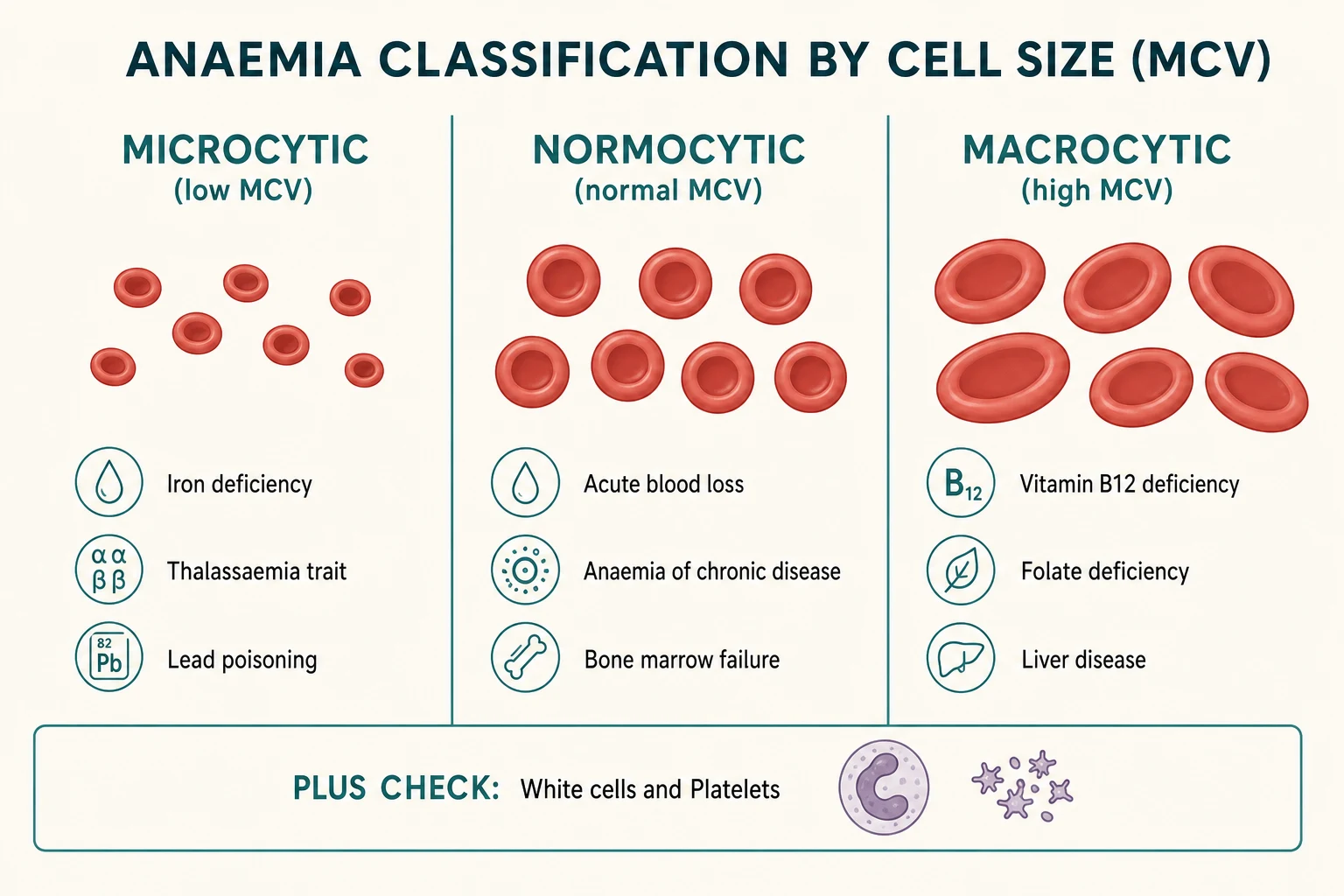
Move 1 — sort the red cells by size. The mean cell volume is the single most useful index because it partitions the anaemias into three families that each have their own differential. Microcytic, a small mean cell volume, points to iron deficiency, thalassaemia and the haemoglobinopathies. Normocytic, a normal volume, points to acute blood loss, anaemia of chronic disease, haemolysis and marrow failure. Macrocytic, a large volume, points to B12 or folate deficiency, liver disease and drug effects. The reticulocyte count then splits the normocytic group further: a high reticulocyte count means the marrow is responding to loss or destruction, a low count means the marrow is not keeping up. [4] [6]
Move 2 — read the white cells and the platelets in parallel. The red cells rarely tell the whole story. A combined drop in haemoglobin, neutrophils and platelets — pancytopenia — redirects the whole work-up towards marrow failure or marrow infiltration, no matter what the mean cell volume shows. An isolated thrombocytopenia in a well child points to immune thrombocytopenia, while thrombocytopenia with fragmented red cells points to a microangiopathic process. A neutropenia is read against ethnicity and infection risk before it is called a disease. [9] [12]
Epidemiology & Risk Factors
Iron deficiency is the commonest nutritional deficiency in childhood and the commonest cause of microcytic anaemia worldwide. It concentrates in two age bands: the rapid-growth window from six months to three years, when dietary iron demand outstrips intake, and adolescent girls, where menstruation meets a growth spurt. Early introduction of unmodified cow's milk, prematurity, low birth weight, and exclusive breastfeeding beyond six months without iron supplementation all raise the risk. Wang sets out these risk factors plainly for primary care. [6]
The global burden is large and inequitable. Maternal and child undernutrition, including iron deficiency, remains a leading cause of lost disability-adjusted life-years in low- and middle-income settings, and anaemia in infancy carries developmental consequences that extend well beyond the blood count. Raleigh and colleagues give a contemporary evaluation and treatment framework that foregrounds screening and early oral iron. [5]
The artefacts that distort a paediatric count have their own epidemiology. Capillary samples in neonates read higher and more variably than venous samples. EDTA-dependent platelet clumping produces a spuriously low platelet count in roughly one in a thousand samples and is the commonest reason a well child is wrongly labelled thrombocytopenic. Cold agglutinins, more frequent in viral seasons, inflate the mean cell volume and deflate the haemoglobin. Knowing how often these artefacts occur is what stops an unnecessary bone marrow test in a healthy child. [4] [8]
Benign ethnic neutropenia is common and frequently misread as pathology. In people of African and Middle Eastern ancestry, an absolute neutrophil count that sits between 1.0 and 1.5 — below the conventional paediatric neutropenia threshold — is a normal variant carried by a substantial minority, reflects a Duffy-antigen-receptor variant, and carries no excess infection risk. Lakhotia and Ortiz both characterise this in children and warn against over-investigation. [11] [12]
Pathophysiology
To read a paediatric count you have to hold the normal trajectory of blood values across childhood in your head, because the numbers move as the child grows. [1] [2]
A term neonate is born relatively polycythaemic, with a high haemoglobin and a high mean cell volume because the red cells are large and stuffed with fetal haemoglobin. Over the first weeks of life the haemoglobin falls steadily as the rapid expansion of blood volume outpaces red cell production, fetal haemoglobin is switched off in favour of adult haemoglobin, and the neonatal red cell lifespan of about eighty days is much shorter than the adult one hundred and twenty. The haemoglobin reaches its trough, the physiological anaemia of infancy, around two to three months in a term baby at roughly 95 to 110. In a preterm infant the fall is earlier and deeper — the anaemia of prematurity — because growth is faster and erythropoietin output is lower. After the trough, erythropoietin drives recovery and the haemoglobin climbs slowly through childhood, with the mean cell volume settling into the low adult range by school age. [1] [4]
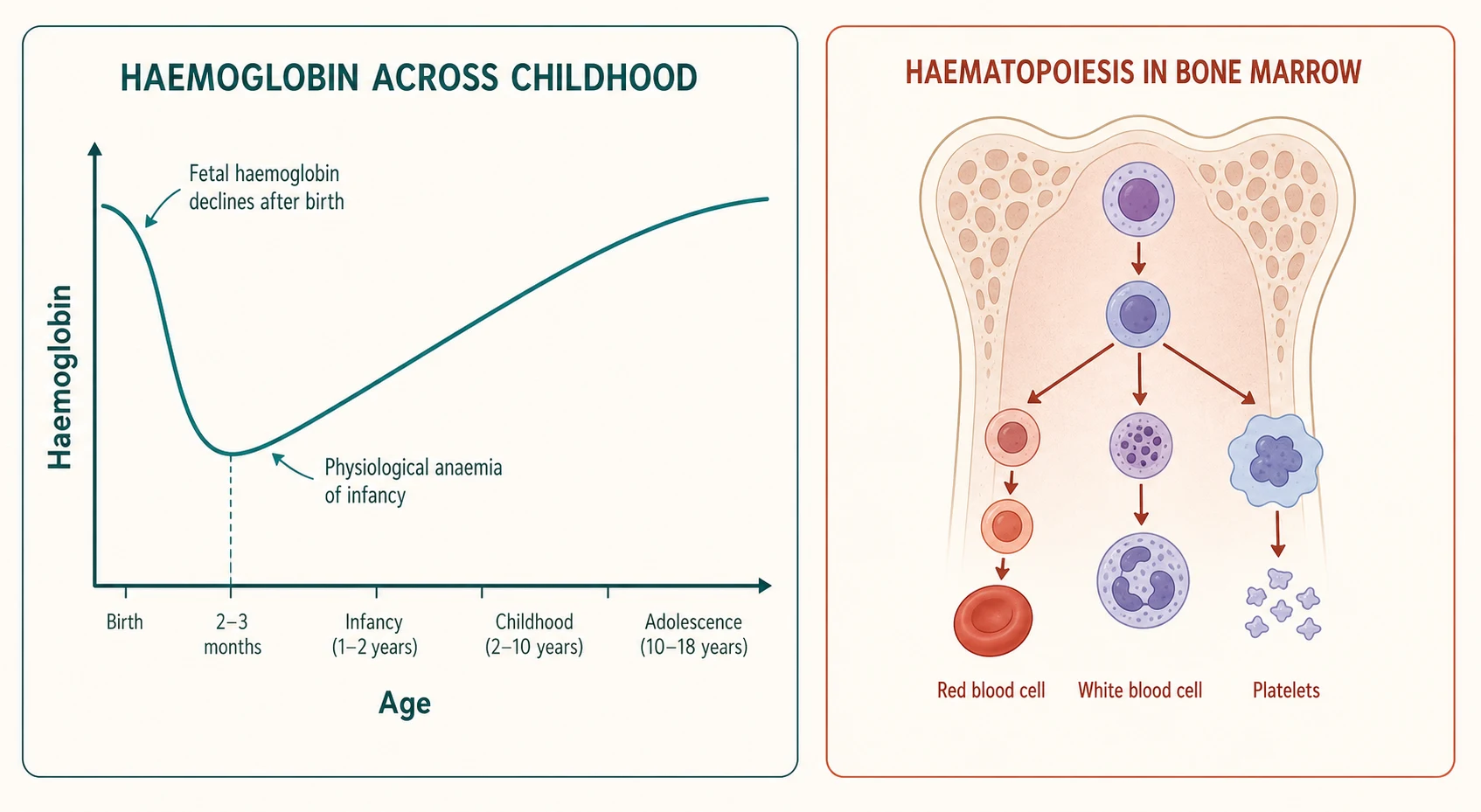
The white cell differential also moves with age. Neonates are neutrophil-dominant for the first days of life, then a lymphocyte predominance takes over and persists until about four to six years, after which neutrophils again become the majority — the adult pattern. A lymphocyte count that looks 'high' on adult ranges is simply the normal pattern of a toddler. The platelet count, by contrast, is comparatively stable across childhood, sitting in the same 150 to 450 band from infancy onward. [1] [2]
Iron deficiency works through supply and demand. In the high-growth window the marrow's appetite for iron outruns dietary intake, so the cells it produces become progressively smaller and less coloured — microcytic and hypochromic — and the red cell distribution width rises as the population becomes uneven. Ferritin, the storage iron, falls first, followed by the transferrin saturation, while the total iron-binding capacity rises. Only later do the haemoglobin and the mean cell volume drop, which is why iron deficiency can be biochemically present before the count looks abnormal. [6]
When the marrow is infiltrated, as in leukaemia, the problem is not supply but factory failure. Malignant blasts crowd the marrow, so production of all three normal cell lines falls together, producing the pancytopenia that is the haematological signature of advanced disease — even though blasts may also spill into the blood and inflate the white cell count. [10]
Clinical Presentation
The count rarely speaks for itself; it confirms what the history and examination suggest. The clinical picture tells you which abnormality to take seriously and which to file as physiological. [4] [5]
Pallor, fatigue and effort intolerance are the classic anaemia symptoms, but in infants they show as poor feeding, listlessness and poor weight gain rather than a complaint of tiredness. A parent who says the child has 'gone white' is often right. Bruising, petechiae and bleeding point to thrombocytopenia; isolated petechiae in an otherwise well child two weeks after a viral illness is the textbook immune thrombocytopenia story. Recurrent infection, fever and mucosal ulceration point to neutropenia, while bone pain, limp, lymphadenopathy and hepatosplenomegaly raise the alarm for leukaemia. [9] [10]
Jaundice, dark urine and splenomegaly point to haemolysis; in a neonate this is the pathway to haemolytic disease of the newborn and the question of exchange transfusion. Dietary history is doing haematology — the volume of cow's milk, the age at which it was introduced, the duration of exclusive breastfeeding, and whether the preterm infant received iron supplementation all change the prior probability of iron deficiency before any cell is counted. [5] [6]
A well child with an isolated, odd number is a different problem. The asymptomatic child with a 'low' platelet count that does not match petechiae-free skin should have the sample repeated, because platelet clumping is the most likely explanation. A febrile child with a high lymphocyte count and atypical cells is more likely to have a viral illness than a leukaemia, but the film settles it. [8]
Differential Diagnosis
Hold the common and the catastrophic together for every abnormal result. [5] [10]
Must-not-miss at any age: acute leukaemia presenting with blasts and pancytopenia, aplastic anaemia and other marrow failure syndromes, sickle cell disease in crisis, haemolytic uraemic syndrome with schistocytes, and severe autoimmune haemolytic anaemia. These stay open for every unexplained cytopenia until the film and the clinical picture clear them. [9] [10]
Microcytic anaemia differential is a short list distinguished by a few tests. Iron deficiency is commonest and shows a high red cell distribution width, low ferritin and a low transferrin saturation. Thalassaemia trait shows microcytosis out of proportion to the anaemia, a normal or near-normal red cell distribution width, a high red cell count, and a Mentzer index — the mean cell volume divided by the red cell count — above 13 that favours thalassaemia over iron deficiency, confirmed by electrophoresis showing a raised haemoglobin A2 in beta-thalassaemia trait. Lead poisoning and chronic inflammation complete the list. [6] [7]
Normocytic anaemia differential splits on the reticulocyte count. A high reticulocyte count means acute blood loss or haemolysis; a low count means underproduction from anaemia of chronic disease, marrow failure or early iron deficiency. Macrocytic anaemia differential runs to B12 or folate deficiency, hypothyroidism, liver disease, and drug effects including chemotherapy. [5]
Isolated thrombocytopenia differential is led by immune thrombocytopenia in the well child, but the film must exclude blasts and schistocytes that would re-point the diagnosis to leukaemia or a microangiopathy. Neutropenia differential runs from benign ethnic neutropenia and post-viral transient neutropenia through to congenital neutropenias and marrow infiltration, separated by the pattern over time, the ethnicity and the clinical phenotype. [11] [12]
Clinical & Bedside Assessment
1. Read the child before the count. Growth, pallor, jaundice, bruising, petechiae, hepatosplenomegaly and lymphadenopathy reframe any number. A thriving, well-appearing toddler with a mildly low haemoglobin is a different problem from a listless, pale infant with the same value. [4] [5]
2. Anchor the age band explicitly. State the child's age aloud before you interpret, then read each value against the correct paediatric range. The single most common error in paediatric haematology is reading a value against an adult reference. [1] [2]
3. Take a dietary and growth history. For any anaemia, ask about cow's milk volume and timing, breastfeeding duration, prematurity, birth weight, and dietary diversity. Plot the weight and length, because faltering growth reframes an isolated anaemia. [5] [6]
4. Ask the family and ethnic questions. Consanguinity, a family history of anaemia, splenectomy or early gallstones points to inherited haemolysis or thalassaemia. Ethnicity reframes a neutrophil count through benign ethnic neutropenia, and it drives the sickle-cell and thalassaemia screening question. [11] [12]
5. Examine for the must-not-miss. Lymphadenopathy, hepatosplenomegaly, bony tenderness and bruising out of proportion to the count raise the alarm for malignancy or marrow failure and lower the threshold for an urgent film and review. [10]
6. Match the number to the phenotype and repeat if discordant. If the platelet count does not fit a child with no petechiae, repeat the sample, ask the lab for a citrate or capillary film, and look for clumping before any intervention. [8]
7. Read the film with the count. The film is part of the bedside assessment, not a deferred laboratory step, whenever the count is abnormal or the child is unwell. [8]
Investigations
Tests should confirm a clinical hypothesis, not generate a list. Read them in the order the problem presents. [5] [7]
Confirm the anaemia and sort it by size. The haemoglobin confirms the anaemia, the mean cell volume sorts it, and the red cell distribution width separates the even microcytosis of thalassaemia from the uneven microcytosis of iron deficiency. [6]
Add iron studies for the microcytic anaemia. Ferritin, transferrin saturation, iron and total iron-binding capacity settle the iron-deficiency question, with the caveat that ferritin is an acute-phase reactant and can be falsely normal with inflammation, so a concurrent C-reactive protein helps interpretation. A stepwise diagnostic approach, as modelled by Aly and colleagues for resource-limited settings, uses these basic indices to triage efficiently before reaching for electrophoresis. [7]
Use the reticulocyte count to read the marrow. A high reticulocyte count means the marrow is responding — to blood loss or to haemolysis — and points you toward a haemolysis screen of bilirubin, lactate dehydrogenase and a direct antiglobulin test. A low reticulocyte count with anaemia means underproduction and points back to the marrow. [5]
Order a blood film whenever the analyser flags or the story is discordant. The film finds the cells the machine cannot — blasts, sickle cells, schistocytes, spherocytes, target cells and basophilic stippling — and it confirms or refutes a spurious count. Courville's review shows automated criteria miss clinically important morphology, so a smear review is the standard response to a flagged result. [8]
Confirm specific diagnoses with targeted tests. Haemoglobin electrophoresis for thalassaemia and the haemoglobinopathies, a direct antiglobulin test for immune haemolysis, a bone marrow aspirate and trephine for suspected leukaemia or marrow failure, and lead levels where the exposure history fits. [10]
Confirm a spuriously low platelet count before treatment. Ask the laboratory to review the film for clumping and to run a sample in an alternative anticoagulant, because treating EDTA clumping as real thrombocytopenia exposes a child to needless risk. [8]
Management — Resuscitation
Most abnormal counts are not emergencies, but a short list of findings demands an immediate, time-critical response. When one of these appears, stop reading the printout and act. [8] [10]
Blasts or circulating immature cells, especially with pancytopenia, is acute leukaemia until proven otherwise. The child needs urgent paediatric oncology referral, a central line of care for fever, and a prompt bone marrow assessment; do not delay while arranging elective outpatient review. Rose-Inman frames the emergency-department presentation of acute leukaemia around exactly this haematological pattern. [10]
Schistocytes with thrombocytopenia and acute kidney injury is a microangiopathic haemolytic anaemia, most commonly haemolytic uraemic syndrome in children. This is a paediatric emergency with fluid, blood-pressure, renal and transfusion considerations handled in parallel, not a routine anaemia work-up. [8]
Sickle cells on the film, with pain, dactylitis, splenic sequestration or acute chest syndrome, is a sickle crisis pathway with analgesia, hydration, oxygen and infection cover, and an awareness that functional asplenia makes fever dangerous. [8]
Severe thrombocytopenia with active bleeding needs urgent discussion with haematology and platelet support tailored to the cause, remembering that immune thrombocytopenia rarely bleeds catastrophically while a leukaemic marrow might. [9]
Severe haemolysis in a neonate, with a rapidly falling haemoglobin and rising bilirubin, is the exchange-transfusion pathway for haemolytic disease of the newborn. [5]
Management — Definitive & Stepwise
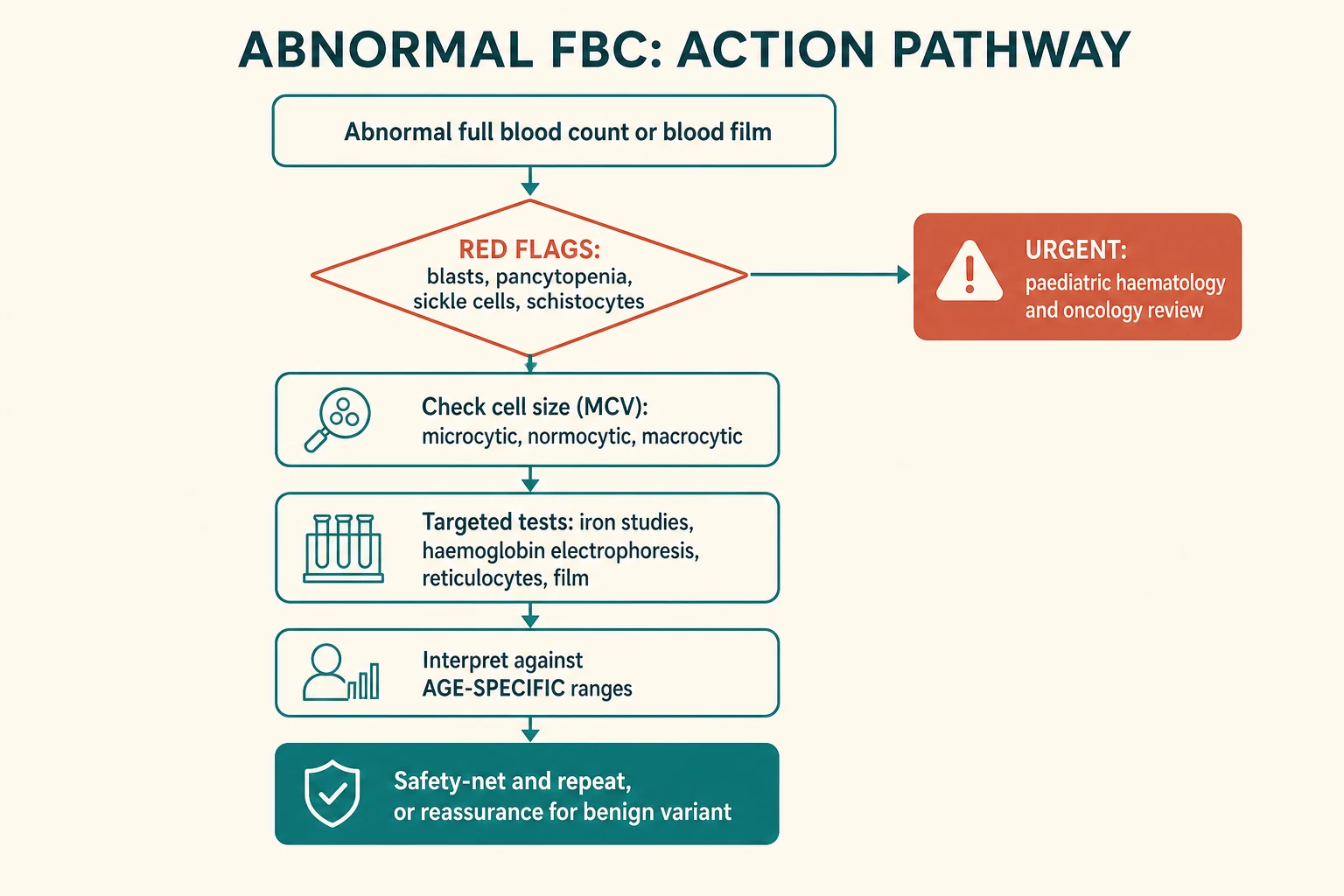
Step 1 — Screen for red flags on the film. Before anything else, confirm there are no blasts, sickle cells, schistocytes or a pancytopenia. If any are present, take the urgent pathway above. This gate overrides every routine step. [8] [10]
Step 2 — Read every value against the correct age band. State the age, then interpret haemoglobin, mean cell volume, white cells and platelets against paediatric reference intervals such as those from CALIPER, not adult ranges. A value normal for age needs no further work-up. [1] [2]
Step 3 — Sort the anaemia by size and reticulocytes. Microcytic, normocytic or macrocytic, then high or low reticulocyte count, frames the differential and the next test. [4] [6]
Step 4 — Treat the common thing first and watch the response. For iron deficiency, give oral elemental iron at 3 to 6 milligrams per kilogram per day, counsel on cow's milk reduction, and expect a reticulocyte rise within seven to ten days and a haemoglobin climbing by about 10 to 20 per week; continue for three months after correction to replete stores. A documented response confirms the diagnosis and avoids unnecessary electrophoresis. [6]
Step 5 — Reassure the benign variants. A well child of African or Middle Eastern ancestry with a stable absolute neutrophil count between 1.0 and 1.5, no infection history and a normal film has benign ethnic neutropenia and needs no marrow test. Document the label, give a fever safety-net, and discharge from haematology. [11] [12]
Step 6 — Manage immune thrombocytopenia to the phenotype. In a well child with immune thrombocytopenia, observation is often appropriate; treatment with steroids or intravenous immunoglobulin is reserved for bleeding or very low counts, guided by the American Society of Hematology 2019 guidelines. [9]
Step 7 — Safety-net and repeat. Give a written safety-net for new bruising, bleeding, pallor, fever or systemic illness, and repeat the count at an interval matched to the abnormality, because the single most informative test in paediatric haematology is often the trend. [4] [5]
Specific Subtypes & Scenarios
The well two-month-old with a low haemoglobin. Check it is the physiological nadir of infancy — a thriving, asymptomatic breastfed infant at two to three months with a haemoglobin around 100 and normal indices needs no work-up. Prematurity, symptomatic pallor or an abnormal film redirect to a haemolysis or iron work-up. [1] [4]
The toddler with microcytic anaemia and a heavy milk intake. This is iron deficiency until proved otherwise. Confirm with iron studies, start oral iron at 3 to 6 milligrams per kilogram per day of elemental iron, reduce cow's milk to under 500 millilitres a day, and document a reticulocyte response. Thalassaemia trait enters only if the red cell distribution width is normal or the iron studies are replete. [5] [6]
The well child with an isolated low platelet count and petechiae. This is immune thrombocytopenia after a viral illness, provided the film shows no blasts or schistocytes and the haemoglobin and white cells are normal. The ASH 2019 guidelines drive the decision to observe or treat. [9]
The child with fatigue, bruising, blasts and pancytopenia. This is acute leukaemia. Urgent oncology referral, fever precautions for the inevitable neutropenia, and a prompt marrow assessment; do not delay. [10]
The child of African ancestry with a stable low neutrophil count. Benign ethnic neutropenia, defined by a chronic absolute neutrophil count between 1.0 and 1.5, a normal film and no infection history, needs reassurance and a fever safety-net rather than investigation. [11] [12]
The child whose platelet count does not fit the picture. EDTA clumping is the likely culprit. Repeat in citrate and review the film before any transfusion or marrow test. [8]
The neonate with jaundice, pallor and a high reticulocyte count. This is haemolysis — haemolytic disease of the newborn, ABO incompatibility or a red-cell membrane defect — and the pathway runs to blood-group typing, a direct antiglobulin test and phototherapy or exchange transfusion thresholds. [5]
Complications & Pitfalls
- Reading a paediatric value against an adult range and over-calling a normal infant as anaemic, or missing real disease in an older child. [1] [2]
- Treating a spuriously low platelet count from EDTA clumping as real thrombocytopenia, exposing a well child to transfusion or marrow biopsy. [8]
- Missing blasts on a film because the automated count looked 'only mildly abnormal' — the film, not the printout, finds leukaemia. [8] [10]
- Calling a normal lymphocyte predominance in a toddler 'leukaemia' because the white cell count looks high on adult ranges. [1]
- Over-investigating benign ethnic neutropenia and labelling a well child with a chronic illness. [11] [12]
- Using a single ferritin in the face of inflammation and missing iron deficiency, because ferritin is an acute-phase reactant. [6]
- Forgetting that the reticulocyte count is the marrow's own answer to whether anaemia is from loss, destruction or underproduction. [4]
Prognosis & Disposition
Most abnormal paediatric counts are benign or treatable. Iron deficiency responds briskly to oral iron, with a reticulocyte rise within a week and full correction in weeks, provided the dietary cause is addressed. Immune thrombocytopenia in a well child usually resolves spontaneously over weeks to months, with chronic disease in a minority. Benign ethnic neutropenia is lifelong but harmless. [5] [9]
The burden of morbidity sits with the must-not-miss diagnoses. Acute leukaemia, marrow failure, sickle cell disease and the microangiopathies carry the risk, which is why the film and the trend exist — to separate the reassuring from the urgent. A single normal count never closes the door on a deteriorating child; the trend and the clinical picture do. [10]
Disposition is matched to the diagnosis and the trend. A well child with iron deficiency or benign ethnic neutropenia leaves with advice, iron, and a repeat count. Immune thrombocytopenia may be observed at home with a safety-net if the count is safe and bleeding is absent. Any blast, any pancytopenia, any microangiopathy, or any sickle crisis belongs in urgent paediatric haematology or oncology hands. Unresolved discordance between the count and the child is never discharged to a distant waitlist. [8] [9]
Special Populations
Neonates and infants: the lowest threshold for age-specific interpretation, because the physiological nadir and the high mean cell volume of the neonate are the two commonest sources of misread counts. [1] [4]
Adolescent girls: menstruation superimposed on a growth spurt makes iron deficiency common, and a dietary and menstrual history changes the prior before any test. [5]
Children of African, Middle Eastern, Mediterranean and South Asian heritage: benign ethnic neutropenia reframes a low neutrophil count, and the carrier frequencies for thalassaemia and sickle trait drive the electrophoresis question. [11] [12]
Indigenous, refugee and socioeconomically disadvantaged children: higher rates of iron deficiency from dietary and environmental factors, language-discordant safety-netting, and the need for interpreter-mediated explanation of benign variants. [5] [6]
Children with complex chronic disease and technology dependence: repeated sampling, central lines, chemotherapy and chronic inflammation all distort the count, so the trend matters more than any single value, and the film is read against the treatment context. [10]
Children in remote and rural settings: a delayed film review changes the threshold for retrieval, and a clear safety-net and a repeat count locally must bridge the gap to specialist haematology. [7]
Evidence, Guidelines & Regional Differences
The CALIPER initiative — Adeli's white paper and the Tahmasebi and Higgins haematology reference standards — is the contemporary foundation for harmonised, age- and sex-specific paediatric reference intervals, and it underpins why an infant and an adolescent cannot share a range. [1] [2] [3]
Celkan's review frames the haemogram as the most informative single test in paediatrics and walks through the interpretation of each parameter. Courville's systematic review confirms that automated analyser criteria detect many smear abnormalities but miss clinically important morphology, justifying the manual film as the arbitrator for any flagged or discordant result. [4] [8]
Raleigh and Wang give the primary-care frameworks for evaluating and treating anaemia and iron deficiency in infants and children, and Aly offers a stepwise approach tuned to resource-limited settings. The American Academy of Pediatrics guidance on iron-deficiency screening and the World Health Organization haemoglobin thresholds for anaemia anchor the screening cut-offs. [5] [6] [7]
The American Society of Hematology 2019 immune thrombocytopenia guidelines set the contemporary standard for managing the commonest isolated paediatric thrombocytopenia, balancing observation against treatment by bleeding phenotype rather than count alone. Rose-Inman frames the emergency presentation of acute leukaemia. Lakhotia and Ortiz characterise benign ethnic neutropenia in children and warn against over-investigation of a harmless variant. [9] [10] [11] [12]
Australian and New Zealand laboratories report age-specific paediatric ranges and offer rapid film review through state pathology networks, with retrieval systems that shorten the time to specialist review for remote children. Care for Aboriginal and Torres Strait Islander, Māori and Pasifika families must be culturally safe and equity-aware, with a lower threshold to screen for iron deficiency given higher prevalence. The high carrier frequency for thalassaemia and haemoglobinopathies across the region keeps electrophoresis central to the microcytic-anaemia work-up. [1] [5] [6]
UK laboratories report age-adjusted paediatric reference ranges and follow British Society for Haematology standards for blood-film review and anaemia assessment. NICE quality standards on transfusion and RCPCH guidance frame the safe use of blood products and the recognition of serious haematological disease in children. [4] [8]
The American Academy of Pediatrics recommends universal anaemia screening around twelve months, and the American Society of Hematology guidelines shape immune thrombocytopenia management. The ABP content outline weights haematology and oncology at 6 per cent. Sickle-cell screening is universal on the newborn blood spot in most states. [6] [9]
Canadian laboratories use CALIPER-derived reference intervals, the initiative itself a Canadian creation, and the RCPSC EPAs anchor recognition of deteriorating children and haematological competence. Newborn screening for sickle cell disease and the haemoglobinopathies is province-dependent. [1] [10]
Exam Pearls
- A child is read against age-specific ranges, never adult ranges; the physiological anaemia of infancy makes a haemoglobin around 100 normal at two months and anaemic at ten years. [1] [4]
- The mean cell volume sorts the anaemia into microcytic, normocytic and macrocytic, and the reticulocyte count then splits the normocytic group. [4] [6]
- Iron deficiency is the commonest cause of microcytic anaemia in childhood; oral elemental iron is 3 to 6 milligrams per kilogram per day, with a reticulocyte rise in seven to ten days. [6]
- The Mentzer index — mean cell volume divided by red cell count — above 13 favours thalassaemia trait over iron deficiency. [6] [7]
- Blasts plus pancytopenia is acute leukaemia until proven otherwise and needs urgent oncology referral. [10]
- Schistocytes with thrombocytopenia and acute kidney injury is haemolytic uraemic syndrome, a paediatric emergency. [8]
- Immune thrombocytopenia is isolated thrombocytopenia in a well child with a normal film; observe unless bleeding. [9]
- Benign ethnic neutropenia is an absolute neutrophil count between 1.0 and 1.5 in a well child of African or Middle Eastern ancestry with a normal film — reassure, do not investigate. [11] [12]
- A spuriously low platelet count that does not fit the child is EDTA clumping until a citrate sample and a film prove otherwise. [8]
- Ferritin is an acute-phase reactant; a concurrent C-reactive protein helps read it, and iron deficiency can be present before the haemoglobin falls. [6]
High-yield anchors
References
- [1]Adeli K; Higgins V; Seccombe D; et al The Canadian laboratory initiative on pediatric reference intervals: A CALIPER white paper. Crit Rev Clin Lab Sci, 2017.PMID 29017389
- [2]Tahmasebi H; Trajtman A; Adeli K; et al CALIPER Hematology Reference Standards (I). Am J Clin Pathol, 2020.PMID 32561916
- [3]Higgins V; Truong D; White-Al Habeeb NMA; et al CALIPER Hematology Reference Standards (II). Am J Clin Pathol, 2020.PMID 32525543
- [4]Celkan TT What does a hemogram say to us? Turk Pediatri Ars, 2020.PMID 32684755
- [5]Raleigh MF; Chaffin M; O'Connor K Anemia in Infants and Children: Evaluation and Treatment. Am Fam Physician, 2024.PMID 39700365
- [6]Wang M Iron Deficiency and Other Types of Anemia in Infants and Children. Am Fam Physician, 2016.PMID 26926814
- [7]Aly NH; et al A stepwise diagnostic approach for undiagnosed Anemia in children: A model for low-middle income country. Blood Cells Mol Dis, 2023.PMID 37558589
- [8]Courville EL; et al Performance of Automated Hematology Analyzer Criteria in Detecting Peripheral Blood Smear Abnormalities: A Systematic Literature Review. Int J Lab Hematol, 2026.PMID 42115681
- [9]Neunert C; Terrell DR; Arnold DM; et al American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv, 2019.PMID 31794604
- [10]Rose-Inman H; Farmen J Acute leukemia. Emerg Med Clin North Am, 2014.PMID 25060251
- [11]Lakhotia R; et al Natural history of benign ethnic neutropenia in individuals of African ancestry. Blood Cells Mol Dis, 2019.PMID 30909074
- [12]Ortiz MV; Robbins A; Meyers PA Identification and Clinical Characterization of Children With Benign Ethnic Neutropenia. J Pediatr Hematol Oncol, 2016.PMID 26925714