Paeds · haematology-oncology-and-transfusion
Germ-cell tumours
Also known as Paediatric germ cell tumours · Childhood germ cell tumour · Sacrococcygeal teratoma · Yolk sac tumour · Dysgerminoma · Intracranial germinoma · Nongerminomatous germ cell tumour · Nonseminomatous germ cell tumour
Fellowship guide to germ cell tumours in children. Covers the primordial germ cell origin and the midline distribution from sacrococcygeal teratoma through mediastinal and gonadal sites to the intracranial pineal and suprasellar region, the bimodal age peaks of the infant teratoma and the adolescent gonadal tumour, the tumour markers alpha-fetoprotein from the yolk sac and immature elements and beta-human chorionic gonadotropin from the choriocarcinoma and the syncytiotrophoblastic germinoma, the Altman classification of the sacrococcygeal teratoma and the imperative of the coccygectomy, the urgent serum marker and imaging pathway, the platinum-based PEB chemotherapy, and the contrast between the highly curable germinoma and the more guarded nongerminomatous intracranial tumour.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A newborn is found at the routine examination to have a large firm mass at the base of the spine, and the question at the bedside is whether this is a simple sacral swelling or the commonest solid tumour of the newborn. Germ cell tumours are a group of neoplasms that arise from the primordial germ cells, the embryonic precursors of the sperm and the egg, and they share a common origin that scatters them along the midline of the body from the sacrococcygeal region through the mediastinum and the gonads to the pineal and the suprasellar region of the brain. They make up about three percent of the childhood cancers, they are among the most curable of the paediatric malignancies, and the single thing that separates the child who is cured from the child who is harmed is how fast the clinician reaches the serum markers, the imaging and the specialist centre. [1][12]
A germ cell tumour in a child is a mass of abnormal cells derived from the primordial germ cell, and its behaviour is set by two things: where it sits and what it secretes. The location sorts the tumour into the gonadal, the ovarian and the testicular, and the extragonadal, the sacrococcygeal, the mediastinal, the retroperitoneal and the intracranial, and the secreted tumour markers sort it into the benign and the malignant. The alpha-fetoprotein and the beta-human chorionic gonadotropin are the two markers that carry the diagnosis, because the yolk sac tumour and the immature teratoma secrete the alpha-fetoprotein, the choriocarcinoma secretes the beta-human chorionic gonadotropin, and the germinoma secretes little or none of either. The histology and the markers together build the named diagnosis that drives the treatment. [3][6]
The first task at the bedside is not to name the tumour but to judge whether the child is in danger, from the high-output cardiac failure of the large sacrococcygeal teratoma, from the airway compromise of the mediastinal mass, or from the hydrocephalus of the intracranial lesion. The second task is to send the serum markers and to image the mass, and the third is to build the multidisciplinary plan that runs paediatric oncology, paediatric surgery, urology, gynaecology and radiation oncology together. The bimodal age distribution, the infant teratoma and the adolescent gonadal tumour, is the reason this topic spans the neonatal and the adolescent medicine, and a candidate who can read the location, the markers and the age is demonstrating exactly the reasoning the boards test. [1]
Classification
The most useful way to classify a paediatric germ cell tumour at the bedside is by where it sits, because the location predicts the presentation, the surgical approach and the urgency. The gonadal tumours divide into the ovarian and the testicular, and the extragonadal tumours sit along the midline where the primordial germ cells once migrated, in the sacrococcygeal region, the retroperitoneum, the mediastinum and the intracranial pineal and suprasellar region. The sacrococcygeal teratoma is the commonest tumour of the newborn, the ovarian germ cell tumour is the commonest ovarian neoplasm of the adolescent girl, and the intracranial germ cell tumour sits in the midline of the brain, classically in the pineal region with the Parinaud syndrome or in the suprasellar region with the diabetes insipidus. [1][6]
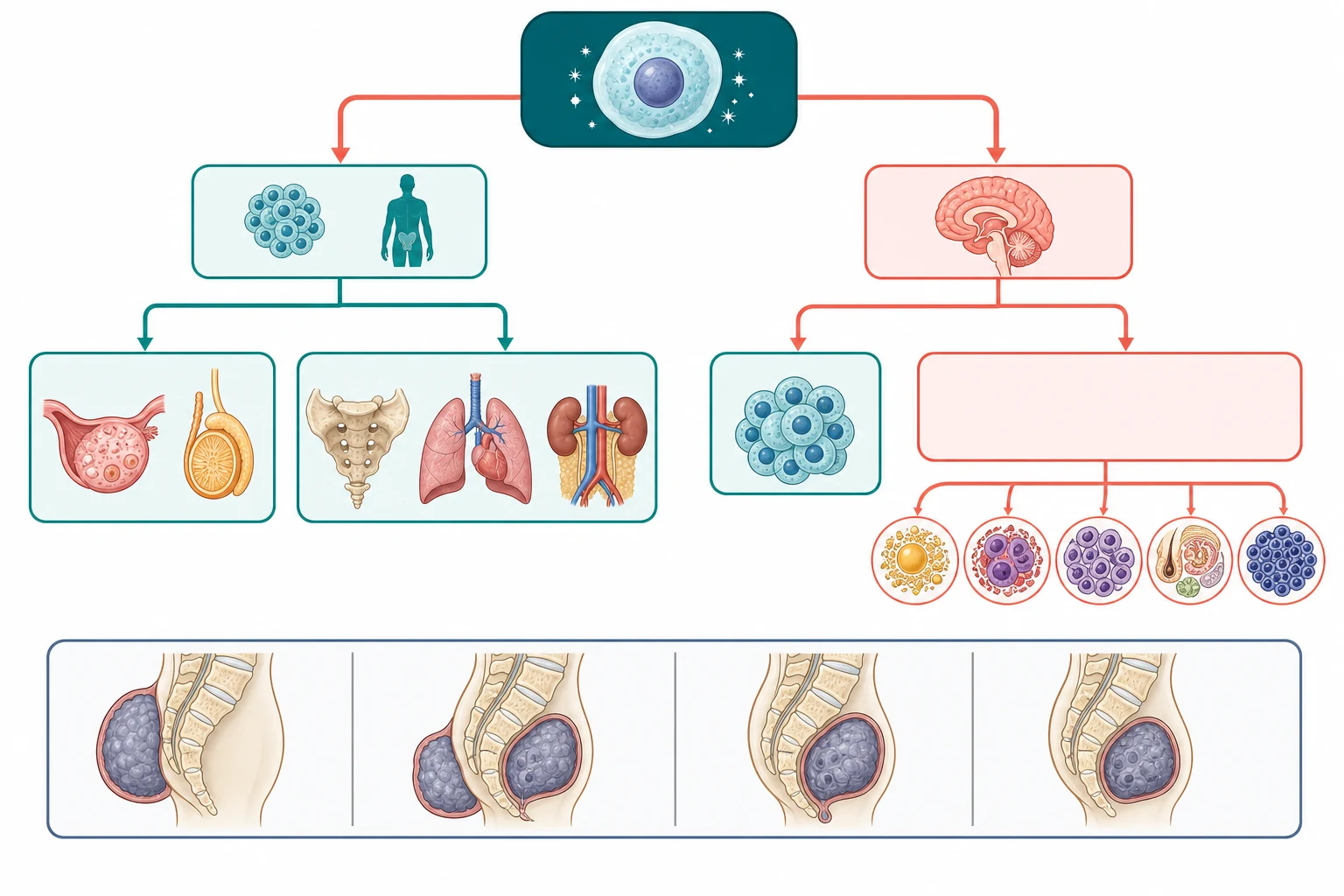
A parallel classification runs through the histology and the markers, and it sorts the germ cell tumours into the benign and the malignant in a way that changes everything. The mature teratoma is the benign lesion, composed of the fully differentiated tissues such as the skin, the hair, the teeth and the cartilage, and it is cured by the complete surgical resection. The germinoma, called the dysgerminoma in the ovary and the seminoma in the testis, is the malignant tumour of the uniform undifferentiated germ cells, and it is the most treatment-sensitive of the malignant germ cell tumours. The nongerminomatous tumours are the more aggressive group, led by the yolk sac tumour, the choriocarcinoma, the embryonal carcinoma and the immature teratoma, and they are the tumours that secrete the alpha-fetoprotein and the beta-human chorionic gonadotropin that the diagnosis and the surveillance depend on. [2][3]
The sacrococcygeal teratoma carries its own classification, the Altman system, and it sorts the tumour by the balance of the external and the internal components because the balance predicts the surgical approach and the risk. The type one is the predominantly external tumour and it is the commonest, the type two has the external component with a significant intrapelvic extension, the type three is predominantly abdominal and intrapelvic with a small external component, and the type four is the entirely presacral tumour with no external component that declares late and carries the highest risk of the malignant transformation. The Altman type and the completeness of the resection together decide the recurrence risk, and the fellow who knows the system can explain why the coccygectomy is non-negotiable. [11]
Mature teratoma
benign, any site
- Fully differentiated tissues: skin, hair, teeth, cartilage
- No marker secretion, alpha-fetoprotein normal
- Curable by complete surgical resection
- Sacrococcygeal form is the commonest newborn tumour
Germinoma
dysgerminoma, seminoma
- Uniform undifferentiated germ cells
- Alpha-fetoprotein normal, beta-hCG mildly raised in some
- Highly chemo- and radiosensitive
- Best prognosis of the malignant group
Yolk sac tumour
nongerminomatous
- The commonest malignant GCT of childhood
- Secretes alpha-fetoprotein
- Aggressive, needs platinum chemo
- Marker fall with treatment tracks the response
Choriocarcinoma
nongerminomatous
- Secretes beta-human chorionic gonadotropin
- May bleed, intracranial form carries bleeding risk
- Aggressive, needs platinum chemo
- Rare but the most marker-defined
Immature teratoma
intermediate
- Contains immature neuroepithelial tissue
- May secrete alpha-fetoprotein
- Graded by the amount of immature tissue
- Surgery plus chemo for higher grade or stage
Epidemiology & Risk Factors
The epidemiology of the childhood germ cell tumour is the story of two diseases bound together by the primordial germ cell. Germ cell tumours make up about three percent of the paediatric malignancies, and they show a characteristic bimodal age distribution that the fellow must carry. The first peak sits in the infant and the young child, dominated by the teratomas and the extragonadal tumours, with the sacrococcygeal teratoma presenting in the newborn at a rate of about one in thirty-five thousand to forty thousand live births and a female predominance of about four to one. The second peak sits in the adolescent, dominated by the gonadal tumours, with the testicular germ cell tumour the commonest solid tumour of the adolescent male and the ovarian germ cell tumour the commonest ovarian neoplasm of the adolescent girl. [1][9]
The location distribution follows the midline migration of the primordial germ cell, and it is the reason the tumours cluster where they do. About half of the paediatric germ cell tumours are gonadal, and the other half are extragonadal, in the sacrococcygeal region, the mediastinum and the retroperitoneum. The intracranial germ cell tumours make up about three percent of the paediatric central nervous system tumours, they cluster in the pineal and the suprasellar region, and they show a male predominance for the pineal lesion and a more equal sex distribution for the suprasellar lesion. The sacrococcygeal teratoma is overwhelmingly a disease of the newborn and the infant, while the gonadal tumours declare in the adolescent. [6][7]
The risk factors cluster around the disorders of the gonadal development and the prior germ cell tumour, and the fellow must name them because they change the counselling and the surveillance. The gonadal dysgenesis and the disorders of sex development carry a markedly raised risk of the gonadoblastoma and the malignant transformation, and the child with the Y-chromosome material and the streak gonad is offered the prophylactic gonadectomy. The cryptorchidism raises the risk of the testicular germ cell tumour, and the Klinefelter syndrome raises the risk of the mediastinal germ cell tumour. The prior germ cell tumour raises the risk of the contralateral and the metachronous tumour, and the family history of the germ cell tumour is recognised in a subset of the cases. [9][10]
The environmental and the modifiable risk factors are weaker and less consistent, and the fellow should not overstate them. The reported associations with the maternal exposures and the environmental agents have not held up in the larger studies, and the bulk of the childhood germ cell tumours arise without an identifiable environmental cause. The strong and the actionable risk factors are the gonadal dysgenesis, the cryptorchidism and the prior tumour, and they are the ones that drive the surveillance and the prophylactic surgery. [1]
Pathophysiology
The pathophysiology of the germ cell tumour is best understood as the story of a cell that set out on a journey and never arrived. The primordial germ cells arise in the yolk sac of the early embryo and they migrate along the midline of the body toward the gonadal ridges, where they are meant to settle and to differentiate into the sperm and the egg. A subset of these cells fail to complete the migration or fail to undergo the programmed cell death at the ectopic sites, and they persist along the midline as the potential seed of the tumour. This single mechanism explains why the extragonadal germ cell tumours cluster at the sacrococcygeal region, the retroperitoneum, the mediastinum and the intracranial pineal and suprasellar region. [8]
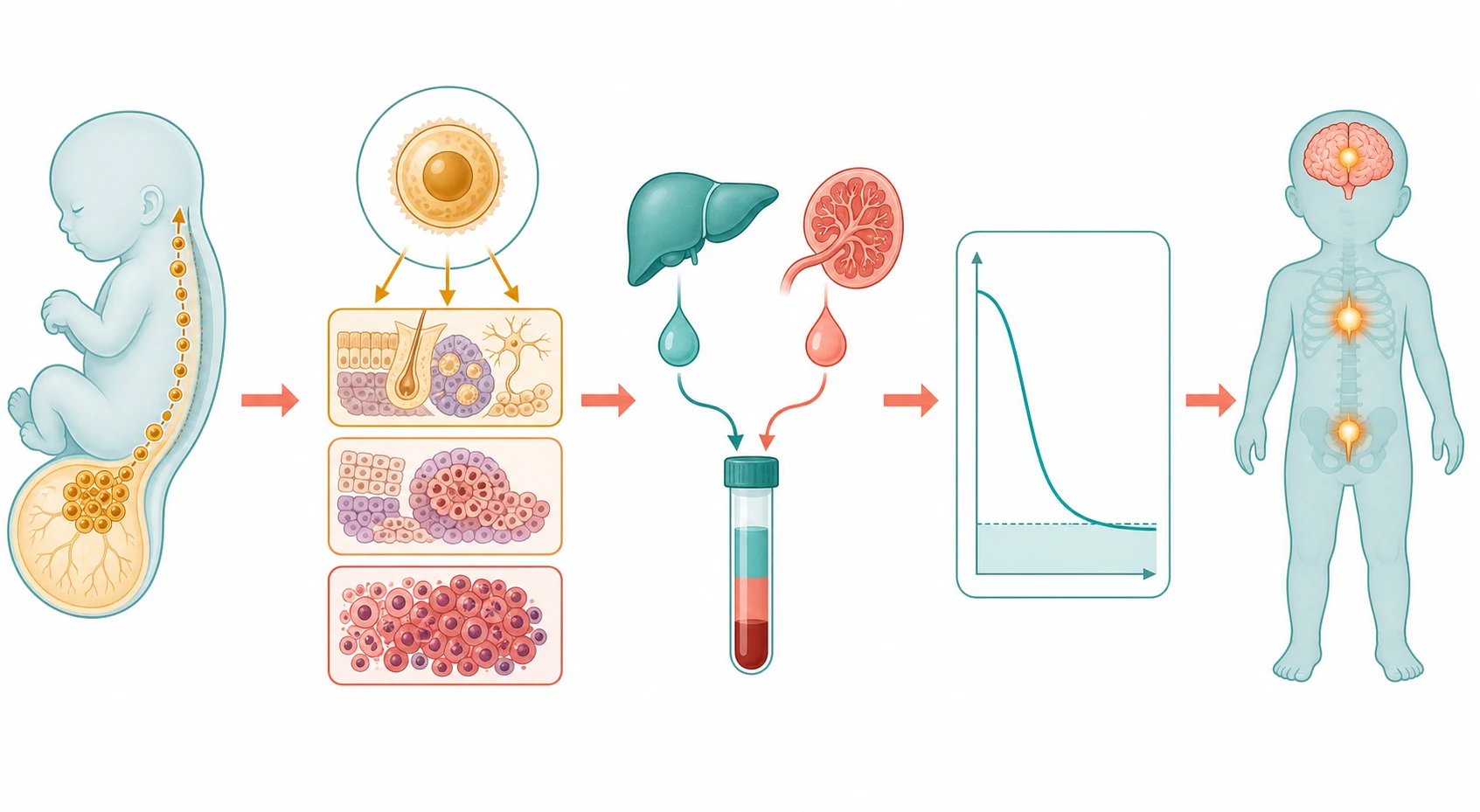
A second mechanism explains the tumour markers, and the markers are the single most useful clinical tool in this topic because they carry the diagnosis and they track the response. The yolk sac tumour secretes the alpha-fetoprotein, the immature teratoma secretes the alpha-fetoprotein, and the embryonal carcinoma may secrete it, while the choriocarcinoma secretes the beta-human chorionic gonadotropin and the germinoma secretes little or none of either unless it carries the syncytiotrophoblastic cells that raise the beta-human chorionic gonadotropin mildly. The lactate dehydrogenase is a non-specific marker of the cell turnover that is used alongside the two specific markers. The marker profile at the diagnosis narrows the histology before the biopsy, and the marker fall during the treatment confirms the response, while the marker rise after the treatment signals the recurrence early. [3]
The single most dangerous pitfall in the interpretation of the alpha-fetoprotein is the physiological elevation of the neonate, and the fellow must hold it at the centre of every assessment of the young infant. The alpha-fetoprotein is very high at birth, in the range of tens of thousands of nanograms per millilitre, and it falls with a half-life of about five to seven days to reach the adult range of under about ten nanograms per millilitre by the age of eight to twelve months. This means that a markedly raised alpha-fetoprotein in a three-month-old infant may be entirely physiological, and it must be interpreted against the age-related reference range, serially if needed, before the malignancy is concluded. The failure to recognise the physiological neonatal alpha-fetoprotein is the classic source of the over-diagnosis and the unnecessary investigation of the young infant. [3]
The pathophysiology of the late effects is the cost of the platinum-based chemotherapy that cures the child, and the fellow must hold it alongside the cure. The cisplatin produces the sensorineural hearing loss and the nephrotoxicity, and the bleomycin produces the pulmonary fibrosis, and these are the toxicities that shape the surveillance of the survivor. The radiotherapy, used in the intracranial disease, produces the neurocognitive and the endocrine late effects. Understanding these mechanisms is what allows the survivorship plan to anticipate the audiology, the pulmonary function and the renal monitoring rather than to react after the harm is done. [4][5]
Clinical Presentation
The child with a germ cell tumour presents in one of four ways, and the recognition of the pattern at the bedside is the skill that decides the speed of the workup. The first is the mass lesion, the sacrococcygeal mass of the newborn, the abdominal or the scrotal mass of the adolescent, or the mediastinal mass on the chest imaging. The second is the endocrine disturbance, the precocious puberty or the diabetes insipidus of the intracranial lesion. The third is the acute complication, the torsion or the rupture of the ovarian tumour, or the high-output cardiac failure of the large sacrococcygeal teratoma. The fourth is the incidental finding on the imaging performed for another reason. [1][6]
The sacrococcygeal teratoma is the paradigm of the neonatal presentation, and it is the tumour the fellow must know in detail. The tumour often declares before the birth, on the prenatal ultrasound, and the large and the highly vascular tumour can produce the high-output cardiac failure and the hydrops fetalis that threaten the fetus. After the birth, the tumour presents as the firm mass at the gluteal cleft, and the type four presacral tumour presents later in the infant or the child as the constipation, the urinary obstruction or the discovered mass, and it carries the higher risk of the malignant transformation. The lesson is that any mass at the base of the spine of a newborn is a sacrococcygeal teratoma until imaging proves otherwise. [11]
The ovarian germ cell tumour presents in the adolescent girl with the abdominal or the pelvic pain, the palpable mass, or the acute complication of the torsion or the rupture that mimics the surgical abdomen. The dysgerminoma is the commonest malignant ovarian germ cell tumour of the adolescent, the immature teratoma and the yolk sac tumour follow, and the hormone-secreting tumour may declare with the precocious puberty or the menstrual disturbance. The testicular germ cell tumour presents in the adolescent boy with the painless scrotal mass, and the prepubertal testicular tumour is more often the benign teratoma that may be managed with the testis-sparing surgery. The mediastinal germ cell tumour presents with the respiratory symptoms, the cough and the dyspnoea, and the large lesion may produce the superior vena cava obstruction. [9][10]
The clinical features that change the urgency are the signs of the acute compromise, and they are the ones that move the child from an elective workup to an emergency. The newborn with the large sacrococcygeal teratoma and the signs of the high-output cardiac failure is at risk of the cardiovascular collapse, and the lesion with the rapid growth or the rupture is a surgical emergency. The child with the mediastinal mass and the stridor, the orthopnoea or the superior vena cava obstruction is at risk of the airway collapse under the anaesthesia, and the biopsy is planned with the greatest care. The child with the pineal lesion and the hydrocephalus is at risk of the herniation. These are the presentations that the fellow recognises at the bedside and escalates without delay. [6]
Differential Diagnosis
The differential of the child with a suspected germ cell tumour is built around the site of the mass, and the serum markers and the imaging are the tests that resolve it. The sacrococcygeal mass sits on a differential that includes the sacral lipoma, the anterior meningocele, the neuroblastoma and the rhabdoid tumour, and the magnetic resonance imaging and the serum markers separate the germ cell tumour from the rest. The ovarian mass sits on a differential that includes the functional cyst, the mature cystic teratoma, the epithelial tumour and the torsion, and the ultrasound and the markers narrow the picture. The testicular mass sits on a differential that includes the hydrocele, the varicocele, the torsion and the epididymitis. [2]
The benign causes that mimic the malignant germ cell tumour must be excluded, because treating the benign lesion as a malignant one is as harmful as missing the malignant one. The mature cystic teratoma of the ovary, the dermoid cyst, is the benign lesion that is cured by the surgical resection without the chemotherapy, and it is distinguished from the malignant tumour by the imaging, the markers and the histology. The sacrococcygeal mass in the newborn is most often the teratoma, but the lipoma and the meningocele are the benign mimics that the imaging resolves. The key is that the normal alpha-fetoprotein and the normal beta-human chorionic gonadotropin favour the benign lesion, while the markedly raised marker favours the malignant tumour. [2]
The chief diagnostic pitfalls for the fellow are the cases in which the diagnosis is delayed because the pattern is misread or the marker is misinterpreted. The child whose sacrococcygeal teratoma is resected without the coccygectomy is the classic recurrence pitfall, because the residual coccyx harbours the cells that regrow the tumour. The infant whose raised alpha-fetoprotein is labelled a marker of the malignancy without the age correction is the classic over-diagnosis pitfall. The adolescent boy whose painless testicular mass is attributed to the hydrocele or the trauma without the ultrasound is the classic delayed diagnosis, and the lesson is to image every painless testicular mass. [3][11]
The differential of the intracranial midline lesion is the one that turns most on the serum markers, because the germinoma and the nongerminomatous tumour share the location with the craniopharyngioma, the pineal parenchymal tumour and the pineoblastoma. The raised alpha-fetoprotein or the beta-human chorionic gonadotropin in the child with the pineal or the suprasellar lesion makes the nongerminomatous germ cell tumour the working diagnosis, and it may spare the biopsy when the markers are diagnostic. The normal markers leave the germinoma and the non-germ-cell tumour in the differential, and the magnetic resonance imaging and the biopsy resolve the question. [6][7]
Clinical & Bedside Assessment
The bedside assessment of the child with a suspected germ cell tumour is a search for the mass, the markers of the acute compromise and the stigmata of the predisposing syndromes. The assessment begins with the airway, the breathing and the circulation, and with the recognition of the high-output cardiac failure in the newborn with the large sacrococcygeal teratoma and the airway compromise in the child with the mediastinal mass. Once the child is safe, the focused history turns to the tempo of the mass, the endocrine symptoms such as the diabetes insipidus and the precocious puberty, the growth and the developmental history, and the disorders of the sex development and the cryptorchidism. [1]
The examination is systematic and takes only a few minutes, but each finding carries weight. The sacrococcygeal mass is examined for the size, the consistency, the skin covering and the relationship to the anus, and the type is estimated at the bedside. The abdomen is examined for the ovarian or the retroperitoneal mass and for the distension. The testis is examined for the mass, and the transillumination distinguishes the hydrocele from the solid tumour. The child with the intracranial lesion is examined for the visual signs, the endocrine signs and the signs of the raised pressure. The puberty is staged, because the precocious puberty is the sign of the hormone-secreting tumour. [6][10]
The focused assessment of the child with a suspected germ cell tumour
Assess the airway, breathing and circulation first, looking for the high-output cardiac failure of the large sacrococcygeal teratoma and the airway compromise of the mediastinal mass
Examine the sacrococcygeal mass for the size, the consistency, the skin covering and the relationship to the anus, and estimate the Altman type
Examine the abdomen for the ovarian or the retroperitoneal mass and the distension, and the testis for the solid mass that does not transilluminate
Examine the child with the intracranial lesion for the visual signs, the endocrine signs and the raised pressure, and stage the puberty
Seek the stigmata of the predisposing syndromes: the gonadal dysgenesis, the cryptorchidism and the Klinefelter features
Send the serum alpha-fetoprotein, beta-human chorionic gonadotropin and lactate dehydrogenase, and arrange the cross-sectional imaging
The severity of the compromise and the speed of the workup are judged at the bedside, and they decide the urgency of the imaging and the surgery. The newborn with the large sacrococcygeal teratoma and the signs of the cardiac failure is moved to the neonatal intensive care, the cardiovascular support and the urgent surgical planning. The child with the mediastinal mass and the airway compromise is managed with the least invasive airway manoeuvres and the urgent imaging, and the general anaesthesia is avoided until the safe plan is built. The child with the pineal lesion and the hydrocephalus is managed with the emergency neurosurgical measures. The child with the stable mass is worked up electively, and the family is counselled on the plan. [1]
Investigations
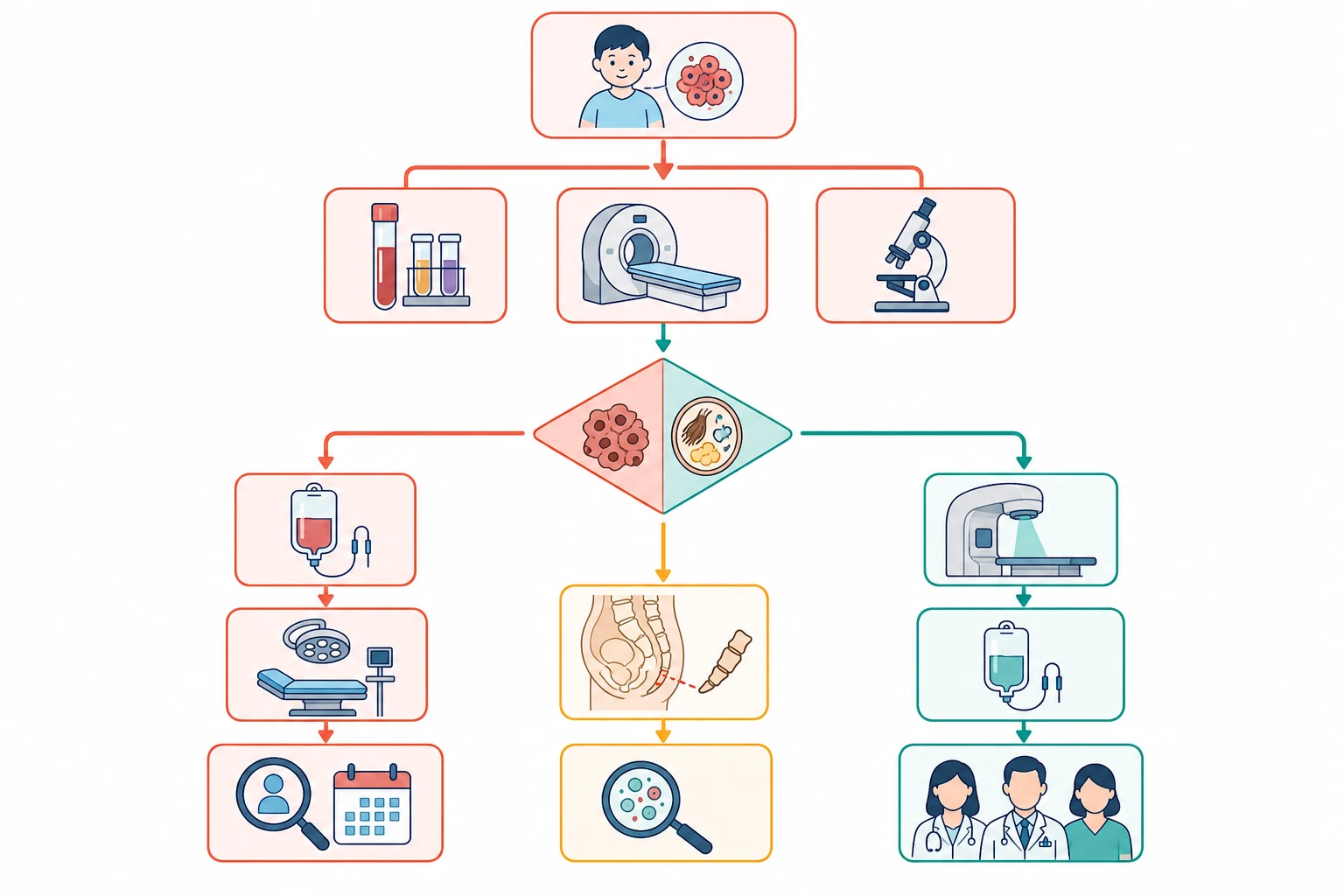
The investigation of a suspected germ cell tumour moves in three steps, the serum markers that narrow the diagnosis, the imaging that localises and stages the tumour, and the histology that delivers the named diagnosis. The first test is the serum alpha-fetoprotein, the beta-human chorionic gonadotropin and the lactate dehydrogenase, sent before any surgery because the marker profile carries the diagnosis and the baseline for the surveillance. The alpha-fetoprotein is raised in the yolk sac tumour, the immature teratoma and the embryonal carcinoma, the beta-human chorionic gonadotropin is raised in the choriocarcinoma and the syncytiotrophoblastic germinoma, and the lactate dehydrogenase is the non-specific marker of the turnover. [3]
The imaging is tailored to the site, and it localises the tumour and stages the disease. The ultrasound is the first test for the gonadal and the sacrococcygeal lesion, because it is quick and accessible and it confirms the solid mass. The magnetic resonance imaging is the standard for the sacrococcygeal, the retroperitoneal and the intracranial lesion, because it shows the relationship to the critical structures in the way the ultrasound cannot. The computed tomography of the chest is performed for the staging of the malignant tumour, to look for the lung metastases, and the bone scan or the magnetic resonance of the spine is added when the symptoms suggest the bony disease. [6]
Across Australia, Aotearoa New Zealand, the United Kingdom, the United States and Canada, the serum alpha-fetoprotein, the beta-human chorionic gonadotropin and the lactate dehydrogenase, with the ultrasound and the magnetic resonance imaging of the primary site and the computed tomography of the chest, form the standard diagnostic workup for a paediatric germ cell tumour. The staging system differs between the international study groups, with the Children's Oncology Group using a surgical-pathological stage and the European and the United Kingdom groups using the TNM-based system. The fellow should know the local protocol and the regional cooperative group.
[4][6]The histological diagnosis is made on the tumour tissue, obtained at the surgery or, in selected cases of the intracranial lesion with the diagnostic markers, deferred. The histology confirms the subtype, the germinoma, the yolk sac tumour, the choriocarcinoma, the immature teratoma or the mature teratoma, and it grades the immature tissue. The molecular studies, including the chromosome 12p amplification and the methylation profiling, are increasingly used to refine the diagnosis and the prognosis, and they are the contemporary layer that sits on the histology. In the intracranial lesion with the markedly raised markers, the diagnosis may be made without the biopsy, and the treatment is begun on the marker profile. [7][8]
Management — Resuscitation
The child with a germ cell tumour may need resuscitation before the definitive plan, and the resuscitation rests on the recognition of the acute complications. The newborn with the large sacrococcygeal teratoma and the high-output cardiac failure is managed with the cardiovascular support, the fluid management and the urgent surgical planning, because the vascular steal through the tumour is the threat to the circulation. The rupture of the tumour and the bleeding into the lesion are managed with the transfusion and the emergency surgery. The paediatric surgery, the neonatology and the oncology are alerted at once. [11]
The child with the mediastinal germ cell tumour and the airway compromise is the one who needs the most careful anaesthetic planning, because the general anaesthesia can collapse the airway and produce the cardiovascular collapse. The child is kept upright, the least invasive airway manoeuvres are used, and the imaging is performed without the general anaesthesia wherever possible. The biopsy, when needed, is planned with the anaesthetist, the surgeon and the oncologist together, and the intensive care and the emergency airway equipment are at the bedside. The lesson is that the mediastinal mass is never anaesthetised lightly. [1]
The child with the intracranial germ cell tumour and the obstructive hydrocephalus is managed with the emergency neurosurgical measures, the external ventricular drain, the endoscopic third ventriculostomy or the shunt, to relieve the raised pressure before the definitive therapy. The pineal lesion that obstructs the aqueduct produces the acute hydrocephalus that can progress to the herniation, and the recognition of the headache, the vomiting and the falling consciousness moves the child to the emergency scan and the neurosurgical referral. The serum markers are sent at once, because a markedly raised alpha-fetoprotein or beta-human chorionic gonadotropin may make the diagnosis without the biopsy. [6]
The ovarian germ cell tumour with the torsion or the rupture is managed with the emergency surgery, and the acute abdominal pain and the mass in the adolescent girl are worked up as the surgical abdomen until the imaging settles the cause. The torsion threatens the ovary, and the rupture may produce the haemorrhage and the peritonitis, and the timing of the surgery is the determinant of the ovarian salvage. The fertility-sparing approach is preferred wherever the imaging and the markers allow, because the unilateral disease is curable with the ovarian preservation. [10]
Management — Definitive & Stepwise
The definitive management of the paediatric germ cell tumour is built around the two modalities of the surgery and the platinum-based chemotherapy, with the radiotherapy added for the intracranial disease, and the combination is tailored to the histology, the stage, the location and the age of the child. The overarching principle is that the complete surgical resection is the foundation of the cure for the localised tumour, that the platinum-based chemotherapy is added for the malignant and the metastatic disease, and that the completely resected early-stage tumour may be managed with the surgery and the surveillance alone to spare the child the toxicity. [4][5]
[4] [7]The mature teratoma is the benign lesion that is cured by the complete surgical resection, and the sacrococcygeal teratoma is the paradigm. The resection includes the complete removal of the coccyx, the coccygectomy, because the residual coccyx harbours the cells that regrow the tumour and the failure to remove it is the single strongest predictor of the recurrence. The ovarian mature teratoma is managed with the ovarian-preserving surgery, the cystectomy or the unilateral salpingo-oophorectomy, and the testicular tumour is managed with the radical inguinal orchiectomy, with the testis-sparing surgery reserved for the selected benign prepubertal lesion. The completely resected mature teratoma needs no chemotherapy, and the surveillance imaging and the marker monitoring follow. [2][11]
Platinum-based PEB chemotherapy for malignant germ cell tumours
Dose
The standard regimen is the combination of bleomycin, etoposide and cisplatin (PEB), given in three to four cycles for the intermediate and the higher-stage disease. The low-risk and the completely resected early-stage tumour may be managed with the surgery and the surveillance alone, or with the carboplatin-based regimen, to spare the cisplatin and the bleomycin toxicity
The intracranial germ cell tumour is the subgroup where the radiotherapy joins the chemotherapy, and the management turns on the germinoma versus the nongerminomatous distinction. The germinoma is the highly treatment-sensitive tumour, and the contemporary approach uses the platinum-based chemotherapy to shrink the tumour followed by the reduced-dose or the focal radiotherapy, to maintain the excellent survival while reducing the neurocognitive and the endocrine late effects. The nongerminomatous intracranial tumour is the more aggressive lesion that needs the chemotherapy and the craniospinal irradiation, and the prognosis is more guarded. The contemporary survival of the germinoma exceeds ninety percent, while the nongerminomatous tumour sits around seventy percent. [7][8]
The risk-adapted strategy is the modern principle that runs through the whole topic, and it is built around the staging and the marker response. The low-risk tumour, the completely resected stage one or two malignant tumour and the mature teratoma, is managed with the surgery and the surveillance, with the chemotherapy reserved for the recurrence. The intermediate-risk tumour receives the standard PEB chemotherapy. The high-risk and the metastatic tumour receives the more intensive chemotherapy, and the contemporary trials test the accelerated BEP regimen of the P3BEP trial against the standard regimen to improve the survival of the poor-risk disease. The fellow who holds the risk groups together demonstrates the reasoning the boards reward. [4][5]
Specific Subtypes & Scenarios
The sacrococcygeal teratoma
The sacrococcygeal teratoma is the commonest tumour of the newborn, and it is the tumour that brings the whole topic together because it spans the fetal, the neonatal and the infantile medicine. The tumour often declares on the prenatal ultrasound, and the large and the vascular lesion may produce the high-output cardiac failure and the hydrops that threaten the fetus and drive the prenatal intervention. After the birth, the tumour presents as the mass at the gluteal cleft, and the Altman type predicts the surgical approach and the risk. The principle that the fellow must carry is the coccygectomy, because the complete removal of the coccyx at the primary resection is the single most important determinant of the cure and the prevention of the recurrence. [11]
The malignant transformation of the sacrococcygeal teratoma is the feared complication, and it is most often the yolk sac tumour that declares in the older infant or the child with the type four presacral lesion. The raised alpha-fetoprotein at the presentation, after the age correction, makes the malignant transformation the working diagnosis, and the management adds the platinum-based chemotherapy to the surgery. The lesson is that the sacrococcygeal teratoma is not a single disease, that the newborn presentation is most often benign and the older presentation is more often malignant, and that the coccygectomy and the marker surveillance are the two measures that prevent the recurrence and the missed transformation. [3][11]
SCTCM
The ovarian germ cell tumour
The ovarian germ cell tumour is the commonest ovarian neoplasm of the adolescent girl, and the dysgerminoma is the commonest malignant subtype. The tumour presents with the abdominal or the pelvic pain, the mass or the acute complication of the torsion, and the surgery is the first step. The fertility-sparing surgery, the unilateral salpingo-oophorectomy with the preservation of the uterus and the contralateral ovary, is the standard for the young patient, because the unilateral disease is curable with the ovarian preservation and the future fertility is protected. The higher-stage and the nongerminomatous tumour receives the platinum-based chemotherapy, and the gonadal dysgenesis carries the worse prognosis that demands the careful counselling. [10]
The testicular germ cell tumour
The testicular germ cell tumour presents in two peaks, the prepubertal tumour that is more often the benign teratoma and the adolescent tumour that is more often the malignant yolk sac tumour or the mixed tumour. The surgery is the radical inguinal orchiectomy for the malignant tumour, and the testis-sparing surgery is reserved for the selected benign prepubertal lesion. The completely resected stage one prepubertal tumour is managed with the surgery and the surveillance, and the chemotherapy is reserved for the higher stage and the metastatic disease, because the COG approach spares the child the toxicity wherever the surgery is curative. The adolescent tumour follows the principles of the adult disease, with the PEB chemotherapy for the higher stage. [9]
The intracranial germ cell tumour
The intracranial germ cell tumour sits in the midline of the brain, classically in the pineal or the suprasellar region, and the germinoma and the nongerminomatous tumour behave very differently. The germinoma is the commonest intracranial subtype, it presents with the diabetes insipidus, the Parinaud syndrome or the precocious puberty, and it is the highly treatment-sensitive tumour that is cured in over ninety percent with the chemotherapy and the reduced-dose radiotherapy. The nongerminomatous tumour, marked by the raised alpha-fetoprotein or the beta-human chorionic gonadotropin, is the more aggressive lesion that needs the chemotherapy and the craniospinal irradiation, and the prognosis sits around seventy percent. The contemporary research explores the biology of the methylation profile and the place of the targeted therapy. [7][8]
Complications & Pitfalls
The complications of the paediatric germ cell tumour divide into the disease-related and the treatment-related, and the fellow must hold both because the treatment toxicity can rival the disease. The disease-related complications are the high-output cardiac failure of the large sacrococcygeal teratoma, the torsion and the rupture of the ovarian tumour, the airway compromise of the mediastinal mass, and the hydrocephalus and the herniation of the intracranial lesion. These are the complications that drive the resuscitation and that are anticipated from the moment the tumour is seen on the scan. [1][6]
The treatment-related complications are the cost of the platinum-based chemotherapy that cures the child, and they shape the surveillance of the survivor. The bleomycin produces the pulmonary fibrosis, the dose-dependent injury that is monitored with the pulmonary function tests and that is worsened by the smoking and the high inspired oxygen. The cisplatin produces the sensorineural hearing loss and the nephrotoxicity, and the audiology and the renal function are monitored through the treatment and the follow-up. The myelosuppression and the infection risk are the acute toxicities of each cycle. The radiotherapy, used in the intracranial disease, produces the neurocognitive and the endocrine late effects, and the growth and the puberty are monitored. [4][5]
The recurrence of the sacrococcygeal teratoma and the malignant transformation are the long-term pitfalls that the surveillance is built to catch. The recurrence is most often at the primary site, and it follows the incomplete resection or the retained coccyx, and the alpha-fetoprotein surveillance and the magnetic resonance imaging catch it early. The malignant transformation of the residual or the recurrent teratoma into the yolk sac tumour is the feared late event, and it is the reason the long-term surveillance is maintained. The second malignancy in the contralateral gonad and the leukaemia after the chemotherapy are the rarer late events that the fellow should know exist. [11][12]
Prognosis & Disposition
The prognosis of a child with a germ cell tumour is among the best in the paediatric oncology, and it is the reason the topic carries a hopeful tone. The survival of the localised malignant germ cell tumour exceeds ninety percent, and the metastatic disease carries a survival around seventy to eighty percent with the contemporary chemotherapy. The mature teratoma is cured by the complete resection. The intracranial germinoma carries a survival over ninety percent, and the nongerminomatous intracranial tumour carries a survival around seventy percent. The prognosis is driven by the stage, the histology, the marker level and the completeness of the resection, and the contemporary trials continue to refine the risk-adapted therapy. [4][7]
The disposition of the child is determined by the diagnosis and the stability, and the management is delivered in the specialist paediatric oncology centre. The child with the newly diagnosed germ cell tumour is referred to the tertiary centre with the paediatric oncology, the paediatric surgery, the urology, the gynaecology and the radiation oncology, and the regional or the rural hospital is responsible for the recognition, the serum markers and the stabilisation before the retrieval. The newborn with the large sacrococcygeal teratoma is managed in the neonatal surgical centre, and the child with the intracranial lesion is managed in the paediatric neuro-oncology centre. [1]
In Australia and Aotearoa New Zealand, the child with a newly diagnosed germ cell tumour is managed in a tertiary paediatric oncology centre, with the paediatric retrieval services transferring the unstable child from the regional or the rural hospital. The treatment is delivered on the national and the international cooperative group protocols, and the ANZUP P3BEP trial of the accelerated versus the standard BEP chemotherapy is the contemporary study for the intermediate and the poor-risk metastatic disease. The long distances and the retrieval times are the reason the early recognition and the serum markers in the referring hospital are so heavily weighted in the exam.
[5]The long-term surveillance of the survivor is the reward and the burden of the cure, because the late effects of the therapy are common and they shape the future health. The survivor has the marker surveillance for the recurrence, the audiology for the cisplatin hearing loss, the renal function for the nephrotoxicity, and the pulmonary function for the bleomycin injury. The intracranial survivor has the endocrine and the neurocognitive surveillance, and the fertility and the reproductive counselling are addressed in the adolescence. The transition to the adult late-effects service is prepared with the survivorship plan and the named adult provider, and the fellow who builds it demonstrates the care that extends beyond the cure. [12]
Special Populations
The child with the disorder of sex development and the gonadal dysgenesis holds a special position in this topic, because the Y-chromosome material and the streak gonad carry a markedly raised risk of the gonadoblastoma and the malignant transformation. The gonadal dysgenesis is associated with the worse outcome in the ovarian nongerminomatous tumour, and the prophylactic gonadectomy is offered to the child with the Y-chromosome material and the streak gonad to prevent the malignancy. The counselling is sensitive, and it is delivered with the endocrinology, the genetics, the psychology and the family together, and the gender and the sexual diversity of the adolescent is respected through the fertility and the reproductive discussion. [10]
The newborn and the young infant are the special population that the age-correction of the alpha-fetoprotein is built for, and the fellow must hold the physiological elevation at the centre of every assessment. The alpha-fetoprotein is very high at birth and it falls to the adult range by the age of eight to twelve months, and the young infant with the raised marker is interpreted against the age-related reference range before the malignancy is concluded. The large sacrococcygeal teratoma of the newborn is managed in the neonatal surgical centre with the cardiovascular support, and the prenatal diagnosis allows the planned delivery in the specialist centre. [3][11]
The socioeconomic disadvantage, the remoteness and the migrant or the refugee status shape the access to the diagnosis and the treatment, and they are the reason the early recognition in the primary care and the regional hospital is so heavily emphasised. A child far from the specialist centre may first present to a clinician who sees few such cases, and the sacral mass or the painless testicular mass that flags the tumour is the bridge to the retrieval and the specialist care. The language and the cultural barriers are addressed with the interpreter and the cultural support, and the family is supported through the long and the unfamiliar treatment. [1][12]
The adolescent and the young adult with a germ cell tumour is prepared for the transition to the adult service with the counselling and the documentation that make it safe. The reproductive and the fertility counselling, the fertility preservation before the gonadotoxic therapy, the late effects of the chemotherapy, and the vocational and the educational support are addressed before the handover. The testicular tumour of the adolescent follows the principles of the adult disease, and the fertility and the contralateral tumour surveillance are part of the survivorship plan. The young person leaves the paediatric service with a survivorship plan and a named adult provider. [9]
Evidence, Guidelines & Regional Differences
The landmark evidence that underpins the modern treatment of the paediatric germ cell tumour is the product of the successive international cooperative trials, and it is the reason the survival has risen to the contemporary excellent figures. The platinum-based chemotherapy transformed the outlook of the malignant germ cell tumour, and the contemporary trials refine the balance of the efficacy and the toxicity. The Malignant Germ Cell International Consortium compared the cisplatin and the carboplatin in the paediatric extracranial disease and established the role of the cisplatin in the higher-risk tumour and the carboplatin in the low-risk regimen, and the marker response was confirmed as the predictor of the outcome. [4][3]
The contemporary evidence tests the optimisation of the chemotherapy and the reduction of the radiotherapy. The ANZUP P3BEP trial of the accelerated versus the standard BEP chemotherapy tests whether the compressed regimen improves the survival of the intermediate and the poor-risk metastatic disease, building on the adult evidence and the paediatric adaptation. The intracranial germinoma trials test the chemotherapy and the reduced-dose radiotherapy to maintain the excellent survival while sparing the neurocognitive and the endocrine late effects. The biology research, including the methylation profiling that confirms the primordial germ cell origin of the germinoma, is the contemporary layer that refines the classification. [5][8]
The chemotherapy backbone of the platinum-based regimen is universal across Australia, Aotearoa New Zealand, the United Kingdom, the United States and Canada, with the cisplatin and the carboplatin used in the risk-adapted combinations. The radiotherapy practice for the intracranial disease varies, with the reduced-dose and the focal radiotherapy increasingly preferred for the germinoma to reduce the late effects, and the craniospinal irradiation reserved for the nongerminomatous tumour. The staging system and the surveillance protocol differ between the Children's Oncology Group and the European cooperative groups, and the fellow should know the local protocol.
[4][7]The controversies and the open questions are the live ones. The optimal management of the completely resected early-stage malignant tumour, balancing the surveillance alone against the adjuvant chemotherapy, is one. The role of the testis-sparing surgery in the prepubertal tumour is another. The optimal reduction of the radiotherapy in the intracranial germinoma, balanced against the recurrence risk, is the third. The fellow holds these as the open questions and cites the trials and the guidelines rather than the dogma, and the survival differences by the ethnicity and the access remain the equity challenge that the public health addresses. [7][12]
Exam Pearls
The high-yield facts for the exam are the ones that change a decision at the bedside, and they are worth carrying as sharp statements. Germ cell tumours arise from the primordial germ cells and they follow the midline from the sacrococcygeal region to the pineal and the suprasellar brain, with the bimodal age peak of the infant teratoma and the adolescent gonadal tumour. The yolk sac tumour and the immature teratoma secrete the alpha-fetoprotein, the choriocarcinoma secretes the beta-human chorionic gonadotropin, and the germinoma secretes little or none of either. The sacrococcygeal teratoma is the commonest tumour of the newborn and the coccygectomy is mandatory. [1][3]
The mature teratoma is cured by the complete resection, and the malignant tumour is cured by the surgery and the platinum-based PEB chemotherapy of the cisplatin, the etoposide and the bleomycin. The intracranial germinoma is the highly curable tumour treated with the chemotherapy and the reduced-dose radiotherapy, and the nongerminomatous tumour needs the craniospinal irradiation and carries the more guarded prognosis. The bleomycin causes the pulmonary fibrosis, the cisplatin causes the ototoxicity and the nephrotoxicity, and the alpha-fetoprotein is physiologically high in the neonate and falls to the adult range by the age of eight to twelve months. [4][7]
The final pearls are the ones that catch the candidate who has learned the headline and forgotten the corner. The physiological neonatal alpha-fetoprotein is the single most tested nuance, and the age correction is never optional. The mediastinal mass is never anaesthetised lightly because of the airway collapse. The coccygectomy is non-negotiable at the primary resection of the sacrococcygeal teratoma. The contralateral and the metachronous tumour is watched in the testicular survivor. The message for the exam is that the markers, the location and the age are the three coordinates that organise the whole topic, and the reasoning that holds them at the centre is the one the boards reward. [3][11]
References
- [1]Hendricks M, Cois A, Geel J Malignant extracranial germ cell tumours: A first national report by the South African Children's Cancer Study Group Pediatr Blood Cancer, 2022.PMID 34971072
- [2]Mann JR, Gray ES, Thornton C Mature and immature extracranial teratomas in children: the UK Children's Cancer Study Group Experience J Clin Oncol, 2008.PMID 18541896
- [3]O'Neill AF, Xia C, Krailo MD alpha-Fetoprotein as a predictor of outcome for children with germ cell tumors: A report from the Malignant Germ Cell International Consortium Cancer, 2019.PMID 31355926
- [4]Frazier AL, Stoneham S, Rodriguez-Galindo C Comparison of carboplatin versus cisplatin in the treatment of paediatric extracranial malignant germ cell tumours: A report of the Malignant Germ Cell International Consortium Eur J Cancer, 2018.PMID 29859339
- [5]Lawrence NJ, Chan H, Toner G Protocol for the P3BEP trial (ANZUP 1302): an international randomised phase 3 trial of accelerated versus standard BEP chemotherapy for adult and paediatric male and female patients with intermediate and poor-risk metastatic germ cell tumours BMC Cancer, 2018.PMID 30157803
- [6]Echevarria ME, Fangusaro J, Goldman S Pediatric central nervous system germ cell tumors: a review Oncologist, 2008.PMID 18586924
- [7]Liu AP, Takami H, Abdelbaki MS Germinoma: Presentation, Management, and Recent Advances Adv Cancer Res, 2025.PMID 41198339
- [8]Fukushima S, Yamashita S, Kobayashi H Genome-wide methylation profiles in primary intracranial germ cell tumors indicate a primordial germ cell origin for germinomas Acta Neuropathol, 2017.PMID 28078450
- [9]Gobel U, Calaminus G, Haas R Testicular germ cell tumors in adolescents - results of the protocol MAHO 98 and the identification of good risk patients Klin Padiatr, 2014.PMID 25431864
- [10]Dicken BJ, Billmire DF, Krailo M Gonadal dysgenesis is associated with worse outcomes in patients with ovarian nondysgerminomatous tumors: A report of the Children's Oncology Group AGCT 0132 study Pediatr Blood Cancer, 2018.PMID 29286555
- [11]Yao W, Li K, Zheng S Analysis of recurrence risks for sacrococcygeal teratoma in children J Pediatr Surg, 2014.PMID 25487496
- [12]Williams LA, Frazier AL, Poynter JN Survival differences by race/ethnicity among children and adolescents diagnosed with germ cell tumors Int J Cancer, 2020.PMID 31304572