Paeds · haematology-oncology-and-transfusion
Haematopoietic stem-cell transplantation
Also known as Bone marrow transplant · HSCT · Allogeneic stem-cell transplant · Autologous stem-cell transplant · Graft-versus-host disease · Sinusoidal obstruction syndrome
Fellowship guide to haematopoietic stem-cell transplantation in children. Covers the separation of autologous from allogeneic transplant, the donor hierarchy from the matched sibling through the matched unrelated and the haploidentical to the cord blood unit, the graft-versus-leukaemia effect and the graft-versus-host disease it produces, the myeloablative and reduced-intensity conditioning, the acute and chronic graft-versus-host disease and its prophylaxis with calcineurin inhibitors and post-transplantation cyclophosphamide, the hepatic sinusoidal obstruction syndrome and its treatment with defibrotide, the neutrophil and platelet engraftment milestones, the graft failure and the donor chimerism, and the supportive care of the febrile neutropenia and the opportunistic infection.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child relapses with leukaemia, or is born with a faulty haemoglobin, or fails to make any white cells at all, and the question becomes whether to replace the entire blood-forming system. That replacement is the haematopoietic stem-cell transplantation, and it sits at the most intensive end of paediatric medicine. The candidate who can hold the intent of the procedure, the donor choice, the conditioning and the complications together has the framework that organises a large block of the fellowship syllabus, because the transplant pulls in oncology, immunology, hepatology and infectious disease at the same time. The acuity is high, the course is long, and the complications are the everyday reality of the transplant ward. [1]
Haematopoietic stem-cell transplantation is the infusion of haematopoietic stem cells after conditioning chemotherapy, with or without radiation, to rescue the marrow and, in the allogeneic form, to confer a new immune system with a graft-versus-leukaemia effect. The procedure is split into the autologous transplant, in which the child's own cells are collected and reinfused, and the allogeneic transplant, in which the cells come from a donor. The autologous form is a rescue that allows the high-dose chemotherapy, while the allogeneic form is an immune replacement that carries the graft-versus-leukaemia benefit and the graft-versus-host disease. The single most important distinction the candidate holds is between these two, because every decision that follows, the donor search, the conditioning, the prophylaxis and the complications, flows from it. [1][5]
The allogeneic transplant dominates this topic because it generates the complications that the exam tests. The donor is the organising variable, and the search moves from the matched sibling donor, the preferred source, through the matched unrelated donor, the haploidentical family donor and the umbilical cord blood unit, each with its own matching requirement, cell dose and risk profile. The graft-versus-leukaemia effect is the immunological prize of the allogeneic transplant, and the graft-versus-host disease is its price, and the modern practice is a constant negotiation between the two. The conditioning, whether myeloablative or reduced-intensity, determines the toxicity, the engraftment speed and the risk of the hepatic sinusoidal obstruction syndrome. [2][3]
The survival after a paediatric transplant depends on the disease, the donor, the conditioning and the complications, and the contemporary outcomes range from over ninety percent for the matched sibling transplant of a benign disease to under forty percent for the refractory leukaemia with the severe graft-versus-host disease. The candidate who carries these numbers, alongside the recognition of the transplant emergencies, holds the reasoning the boards reward. The rash, the diarrhoea, the jaundice and the fever in the post-transplant child are never dismissed, because each maps to a complication that demands a specific response. [1][12]
Classification
Begin with the cell of origin, because the autologous-versus-allogeneic split is the organising principle of the whole topic. The autologous transplant collects the child's own stem cells, usually mobilised from the peripheral blood with a granulocyte colony-stimulating factor, and reinfuses them after the high-dose chemotherapy. Its role in paediatrics is narrow but important, chiefly the high-dose chemotherapy with the autologous rescue for the high-risk solid tumour such as the neuroblastoma, and it carries no graft-versus-host disease because the donor and the recipient are the same person. The allogeneic transplant takes the cells from a donor, and it is this form that confers the graft-versus-leukaemia effect and the graft-versus-host disease. [1]
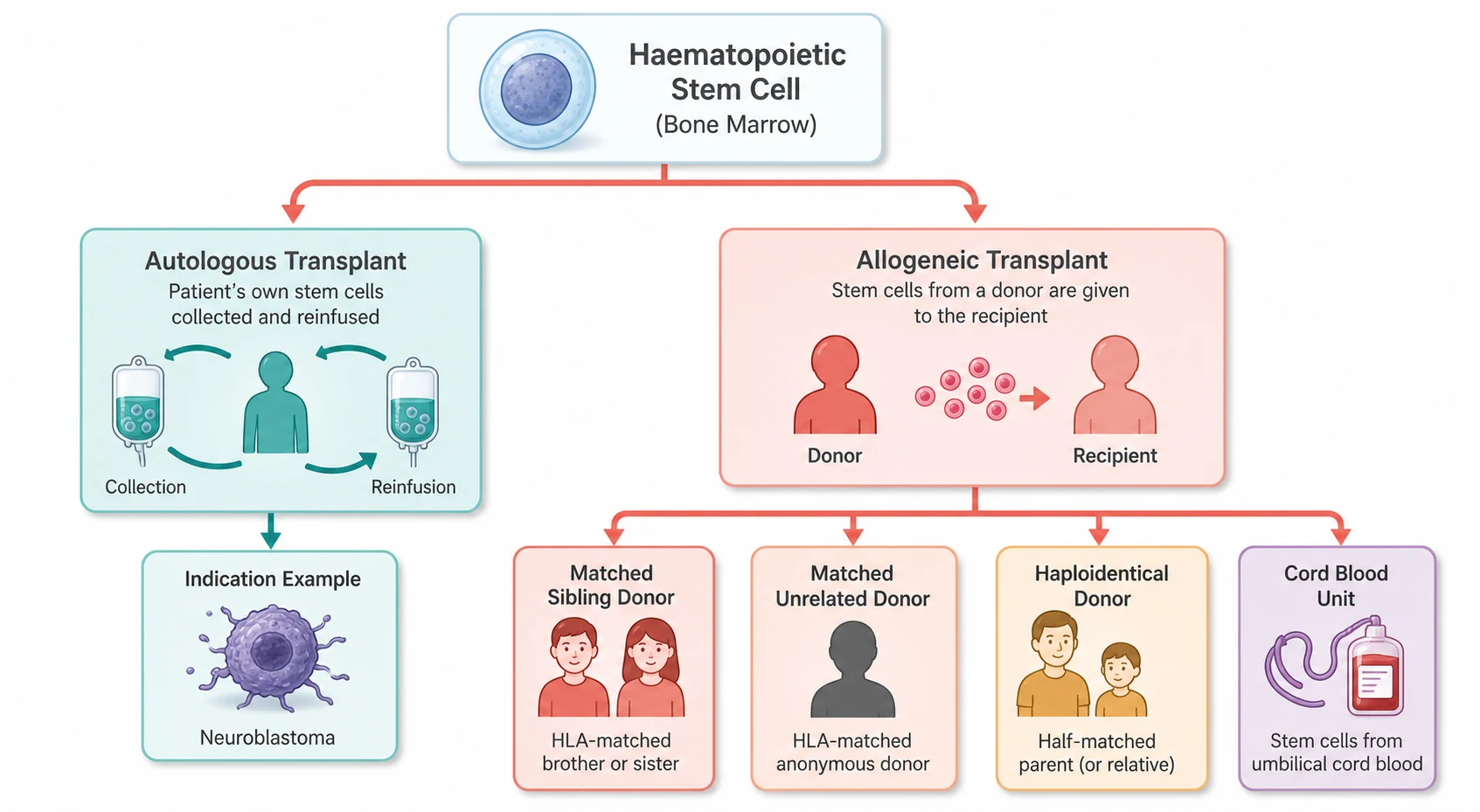
The allogeneic transplant is classified further by the donor source, and the donor hierarchy is a high-yield examination structure. The matched sibling donor remains the preferred source, because each child has roughly a one in four chance of a full HLA match with a sibling, and the matched sibling carries the lowest graft-versus-host risk and the best survival. When no matched sibling exists, the search moves to the matched unrelated donor through the international registries, then to the haploidentical family donor, the half-matched parent or sibling that the post-transplantation cyclophosphamide has made safe and common, and finally to the umbilical cord blood unit. Each source has its own cell dose, engraftment speed and immunological profile. [2][4]
The HLA matching is the laboratory basis of the donor choice, and the candidate must hold the essentials. The classical matching examines the human leucocyte antigen loci, the HLA-A, HLA-B, HLA-C and HLA-DRB1 at a minimum, so that an eight-out-of-eight match at these four loci is the standard for the adult and the unrelated donor, with the additional DQB1 and DPB1 refining the match to the ten-out-of-ten or the twelve-out-of-twelve. The cord blood, because of its immunological immaturity, tolerates a lower match, with a four-out-of-six match at the HLA-A, HLA-B and the antigen-level DRB1 often sufficient. The permissive mismatches at the DPB1 and the direction of the mismatch are the contemporary refinements that the modern donor-selection algorithms now apply. [2]
A third classification runs through the graft source, the tissue the cells are taken from. The bone marrow harvest, the original source, takes the cells from the posterior iliac crest under the general anaesthetic. The peripheral blood stem cell, mobilised into the blood with the granulocyte colony-stimulating factor and collected by the apheresis, is now the commonest source for the older child and the adult because it engrafts faster. The umbilical cord blood, collected at the birth and cryopreserved, carries the lowest cell dose but the lowest graft-versus-host risk and the highest tolerance for the mismatch. The choice of the source interacts with the donor choice to set the engraftment speed and the complication profile. [1][2]
Autologous transplant
the child's own cells
- High-dose chemotherapy with the stem-cell rescue
- Main paediatric role is the high-risk solid tumour such as neuroblastoma
- No graft-versus-host disease and no graft-versus-leukaemia effect
- Faster engraftment and lower early mortality
Allogeneic transplant
donor cells
- Confers the graft-versus-leukaemia effect
- Carries the graft-versus-host disease
- Donor hierarchy: sibling, unrelated, haploidentical, cord blood
- The standard for the high-risk and the refractory leukaemia
Cord blood transplant
umbilical cord unit
- Tolerates the lower HLA match, four of six often sufficient
- Lowest cell dose and the slowest engraftment
- Lowest graft-versus-host risk per the mismatch
- Double-cord strategies raise the cell dose
Epidemiology & Risk Factors
The epidemiology of the paediatric transplant is the epidemiology of the diseases it treats. The malignant indications, the high-risk and the relapsed leukaemia, the myelodysplasia and the lymphoma, account for roughly half of the allogeneic transplants in children, and the acute lymphoblastic leukaemia in relapse is the single commonest malignant indication. The non-malignant indications, the haemoglobinopathies of the sickle cell disease and the thalassaemia, the inherited marrow failure and the primary immunodeficiencies, account for the remainder, and the haemoglobinopathy share has risen sharply as the curative intent for the sickle cell disease has grown. The candidate should know that the transplant is a curated therapy reserved for the defined high-risk and the refractory disease, not a default. [1]
The risk factors for the poor outcome after the transplant are few but decisive. The disease status at the transplant is the single most powerful predictor, because the child transplanted in the remission does far better than the child transplanted with the active or the refractory disease. The donor choice is the next, with the matched sibling donor carrying the best survival and the haploidentical and the mismatched cord carrying the higher risk. The conditioning intensity, the comorbidity of the child and the age all shape the toxicity and the engraftment, and the occurrence of the severe graft-versus-host disease or the sinusoidal obstruction syndrome cuts the survival sharply. [1][3]
The risk factors for the complications themselves are the ones the exam tests most heavily. A high tumour burden and a bulky marrow raise the risk of the sinusoidal obstruction syndrome, and the prior hepatotoxic therapy, the iron overload from the chronic transfusion and the active liver inflammation each add to it. The degree of the HLA mismatch, the use of the peripheral blood rather than the marrow, the older donor and the female donor to the male recipient each raise the graft-versus-host risk. The T-cell replete graft, the haploidentical setting and the slow engraftment raise the infection risk, and the candidate who holds these predictors holds the preventive plan. [5][8]
Pathophysiology
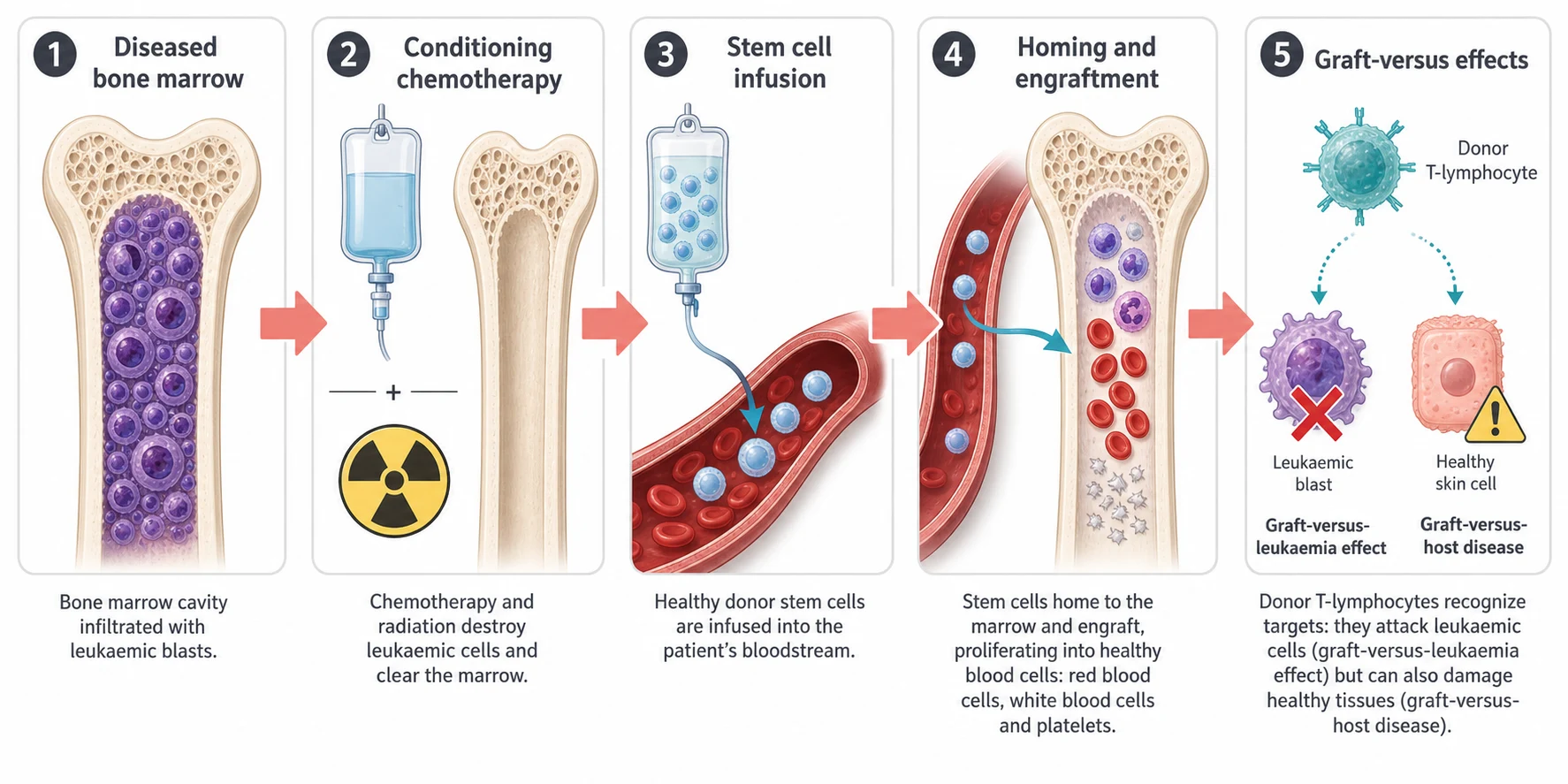
The transplant rests on three physiological ideas, and each drives a part of the management. The first is the conditioning, the chemotherapy and the radiation that empties the diseased marrow and makes space for the new stem cells. The second is the engraftment, the homing of the infused stem cells to the marrow niche and their proliferation into the new blood lineages. The third is the alloreactivity, the interaction between the donor immune cells and the recipient tissues that produces both the graft-versus-leukaemia effect and the graft-versus-host disease. The candidate who holds these three mechanisms holds the rationale for every intervention in the topic. [5]
The conditioning empties the marrow and suppresses the recipient immunity so that the donor cells are accepted, and it is classified by its intensity. The myeloablative conditioning, built on the total body irradiation or the busulfan at the high dose, causes the irreversible marrow ablation and the deepest graft-versus-leukaemia effect, and it carries the highest toxicity to the liver, the lungs, the growth and the fertility. The reduced-intensity conditioning, built on the fludarabine with the lower-dose alkylating agent, relies more on the graft-versus-leukaemia effect and less on the cytotoxic kill, and it is reserved for the child with the comorbidity or the slower-growing disease where the lower toxicity buys the engraftment without the full ablation. [3]
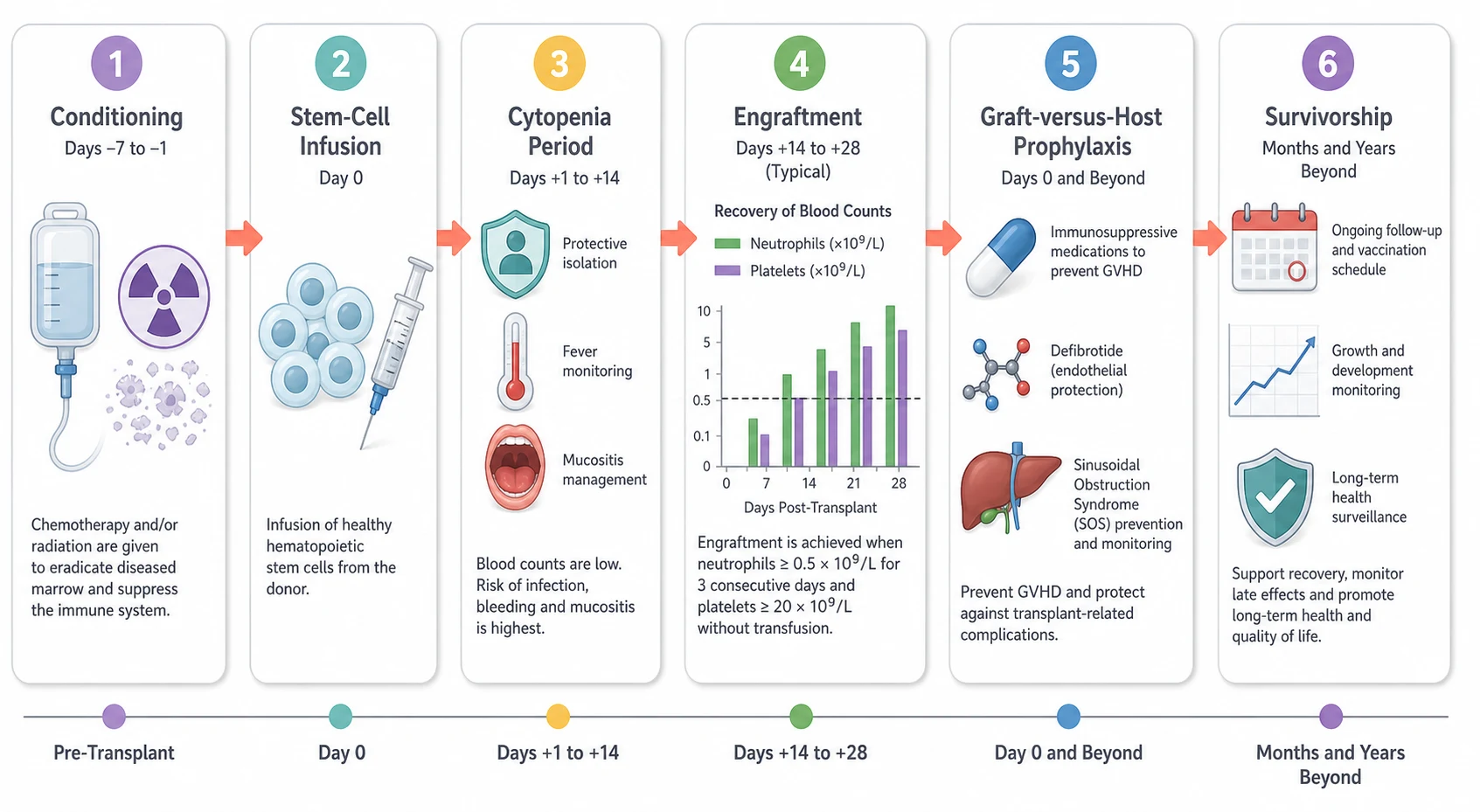
The engraftment is the homing of the infused stem cells to the marrow niche, where the CD34-positive cells lodge, divide and reconstitute the blood lineages. The neutrophil engraftment is the first milestone, defined as the first of three consecutive days with an absolute neutrophil count of zero point five times ten to the nine per litre or above, and it typically occurs between day ten and day twenty-eight depending on the graft source. The platelet engraftment follows, defined as seven consecutive days with a platelet count above twenty times ten to the nine per litre without the transfusion support. The cell dose, the CD34-positive cell content of the graft, is the chief determinant of the engraftment speed, and a low dose raises the graft failure risk. [11]
The alloreactivity is the engine of both the cure and the complication, and it deserves the candidate's full attention. The donor T-lymphocytes recognise the recipient tissues through the minor histocompatibility antigens and the major mismatches, and in the leukaemic cell this recognition drives the graft-versus-leukaemia effect that cures the disease. In the healthy skin, the gut and the liver, the same recognition drives the graft-versus-host disease, and the inflammatory cytokine cascade, the damage from the conditioning and the microbial signals from the disrupted gut barrier all amplify it. The chronic graft-versus-host disease adds a fibrotic, autoimmune-like process that scleroses the skin and dries the mucosa. The management of the transplant is the constant modulation of this alloreactivity. [5][6]
Clinical Presentation
The child who receives a transplant is on a defined timeline, and the clinical presentation is read against the day from the infusion, with the day of the stem-cell infusion set as day zero. The first two weeks are the conditioning and the cytopenia, with the mucositis, the diarrhoea and the fever dominating the picture, and the child is nursed in the protective isolation with the broad-spectrum empiric cover. The engraftment period, from day ten to day twenty-eight, brings the rising counts and the lifting of the cytopenia, but it is also the window for the acute graft-versus-host disease and the sinusoidal obstruction syndrome. The first hundred days carry the highest risk of the acute complications, and the first year carries the chronic complications and the opportunistic infection. [1][12]
The acute graft-versus-host disease presents in the skin, the gut and the liver, and the rash is usually the first sign. A maculopapular rash on the palms, the soles and the ears, often beginning around the time of the engraftment, is the classic presentation, and it may progress to the bullae and the desquamation of the severe form. The gut involvement presents with the anorexia, the nausea, the voluminous diarrhoea and the abdominal pain, and the liver involvement presents with the rising bilirubin. The severity is graded by the extent of the skin, the bilirubin level and the stool volume, and the diagnosis is confirmed by the biopsy because the differential of the post-transplant rash and diarrhoea is wide. [5]
The sinusoidal obstruction syndrome presents in the liver, and its timing is the clue. The onset is usually within the first twenty-one days after the conditioning, and the child develops the weight gain from the fluid retention, the tender hepatomegaly, the rising bilirubin and the ascites. The pathophysiology is the injury to the hepatic sinusoidal endothelium by the conditioning, with the sloughing of the cells into the terminal hepatic venules and the obstruction that backs up the blood and starves the hepatocytes. The severe form progresses to the multi-organ failure, the hepatorenal syndrome and the death, and the early recognition is the difference between the full recovery and the fatal course. [8][9]
The chronic graft-versus-host disease presents after day one hundred and takes a different shape, with the sclerotic and the lichenoid skin changes, the dry eyes and the dry mouth, the oral mucosal lesions and the sicca syndrome, and the pulmonary and the hepatic involvement. It resembles an autoimmune connective tissue disease, with the fasciitis, the joint stiffness and the contracture, and it is the chief driver of the late morbidity and the quality-of-life burden after the allogeneic transplant. The diagnosis rests on the distinctive clinical findings and the tissue biopsy, and the staging follows the National Institutes of Health criteria that grade each organ separately. [6][7]
The infectious presentation is woven through the whole course, and the timeline of the immune reconstitution predicts the organism. In the pre-engraftment cytopenia, the bacterial sepsis and the candidal infection dominate, and the fever is treated as the febrile neutropenia. After the engraftment, the cytomegalovirus reactivation, the adenovirus and the Epstein-Barr virus emerge, and the Pneumocystis and the encapsulated bacteria follow the slow reconstitution of the humoral immunity. The candidate who reads the day from the infusion alongside the symptom holds the likely organism and the empiric therapy. [12]
Differential Diagnosis
The differential of the post-transplant complication is short at the bedside because the transplant sets the context, but the candidate must separate the graft-versus-host from its mimics because the treatment diverges. The rash after the engraftment is the classic challenge, and the differential includes the drug eruption from the antibiotic or the prophylactic agent, the viral exanthem of the cytomegalovirus or the adenovirus, and the engraftment syndrome that accompanies the rising neutrophils. The skin biopsy with the immunohistochemistry settles the graft-versus-host from the drug eruption, and the viral studies settle the infection. [5]
The hepatic differential is the other classic trap, and it rests on the timing and the pattern. The sinusoidal obstruction syndrome presents early, within the first three weeks, with the weight gain and the tender liver, while the hepatic graft-versus-host presents later, often after the engraftment, with the jaundice and the gut involvement. The drug-induced liver injury from the antifungal or the antibiotic, the viral hepatitis from the cytomegalovirus or the hepatitis virus, and the iron overload from the chronic transfusion each add to the differential. The transaminase pattern, the bilirubin trend, the viral studies and the liver biopsy read together settle the cause. [8][9]
The diarrhoeal differential demands the same discipline, because the gut graft-versus-host mimics the infectious colitis and the conditioning mucositis. The stool is sent for the bacterial culture, the viral panel including the adenovirus and the cytomegalovirus, and the clostridioides difficile toxin, and the colonoscopy with the biopsy distinguishes the apoptotic crypt loss of the graft-versus-host from the viral inclusion and the neutropenic enterocolitis. The lesson is that no post-transplant symptom is attributed to the graft-versus-host without the tissue confirmation, because the empiric immunosuppression for a misdiagnosed infection is as harmful as the missed graft-versus-host. [5]
Acute GVHD
donor-versus-host
- Rash on palms and soles around the engraftment
- Diarrhoea and rising bilirubin within 100 days
- Skin and gut biopsy with the apoptotic crypt loss
- Treated with the glucocorticoid and the calcineurin inhibitor
Sinusoidal obstruction syndrome
hepatic, early
- Weight gain, tender liver and jaundice within 21 days
- Backs up the hepatic sinusoids after the conditioning
- Ultrasound with the reversal of the portal flow
- Treated with the defibrotide at 25 mg per kg per day
Engraftment syndrome
rising neutrophils
- Fever, rash and weight gain as the counts rise
- Around the engraftment, before day 21
- Resolves with the supportive care and the short glucocorticoid
- Excluded by the negative cultures and the biopsy
Drug eruption
reaction
- Rash after a new antibiotic or antifungal
- No the gut or the liver involvement usually
- Eosinophilia and the characteristic morphology
- Resolves with the withdrawal of the agent
Clinical & Bedside Assessment
The bedside assessment of the post-transplant child is a structured search for the complications, and it is read against the day from the infusion. The assessment begins with the airway, the breathing and the circulation, because the immunocompromised child with the fever and the cytopenia can deteriorate quickly. The focused history turns to the day from the transplant, the conditioning regimen, the donor type, the engraftment status, the current prophylaxis and the last chimerism result, because each frames the likely complication. The child on the calcineurin inhibitor is asked about the tremor, the headache and the thirst that flag the toxicity. [12]
The examination is systematic and each system carries weight. The skin is inspected for the rash of the graft-versus-host, the sclerotic changes of the chronic form, the line-site infection and the petechiae of the thrombocytopenia. The mouth is inspected for the mucositis, the lichenoid lesions and the dryness, and the abdomen for the hepatomegaly and the tenderness of the sinusoidal obstruction syndrome and the gut involvement. The weight is taken daily and the fluid balance kept strict, because the weight gain is the earliest sign of the hepatic and the capillary-leak complications. The chest is auscultated for the pneumonitis and the opportunistic infection. [5][8]
The focused examination of the post-transplant child
Note the day from the transplant, the donor type, the conditioning and the engraftment status before the examination begins
Inspect the skin for the graft-versus-host rash on the palms, soles and ears, and the sclerotic changes of the chronic form
Inspect the mouth for the mucositis, the lichenoid lesions and the sicca, and examine the line site for the infection
Examine the abdomen for the hepatomegaly and the tenderness, and weigh the child for the fluid-retention trend
Auscultate the chest for the pneumonitis and the opportunistic infection, and assess the oxygen saturation
Check the neurological status for the tremor, the headache and the posterior reversible encephalopathy of the calcineurin inhibitor
Review the daily bloods for the count, the liver function, the electrolytes and the drug levels, and plot the trends
The severity assessment at the bedside decides the urgency and the level of the care. The child with the hypotension, the hypoxia, the severe mucositis or the signs of the multi-organ failure is moved to the paediatric intensive care, and the empiric therapy is broadened and escalated. The child with the severe acute graft-versus-host, the grade three to four rash or the litres of the diarrhoea, is admitted for the intravenous immunosuppression. The teaching of the family is part of the assessment, because the post-transplant child is sent home with the strict instruction to return at once with the fever, the rash or the diarrhoea, and the neutropenic precautions are reinforced at every visit. [12]
Investigations
The investigation of the post-transplant child moves in two streams, the daily surveillance that tracks the engraftment and the complications, and the targeted workup that confirms the named complication. The daily panel through the cytopenia is the full blood count, the electrolytes, the renal and the liver function, the coagulation and the drug levels of the calcineurin inhibitor, with the C-reactive protein and the blood cultures taken with every fever. The film is examined for the engraftment and the signs of the haemolysis, and the lactate dehydrogenase and the bilirubin are tracked for the hepatic complications. [1][11]
The engraftment is tracked through the neutrophil and the platelet counts, and the donor chimerism is the laboratory confirmation that the engrafting cells are the donor's. The chimerism is measured by the short tandem repeat or the fluorescence in-situ hybridisation, and it is checked at the defined intervals, typically at day thirty, day one hundred and then periodically. A full donor chimerism confirms the engraftment, while a falling donor chimerism flags the graft rejection and the impending graft failure. The candidate should know that the chimerism is the arbiter of the engraftment success, not the count alone, because the recipient cells can re-emerge and crowd out the donor. [11]
The targeted workup confirms the named complication. The suspected acute graft-versus-host is confirmed by the skin, the gut or the liver biopsy, with the apoptotic keratinocytes and the crypt-cell loss the hallmark. The sinusoidal obstruction syndrome is supported by the liver ultrasound with the doppler showing the reversal of the portal flow and the elevated hepatic pressures, with the transjugular liver biopsy and the pressure measurement in the selected case. The viral reactivation is tracked by the quantitative polymerase chain reaction for the cytomegalovirus, the Epstein-Barr virus and the adenovirus, and the surveillance is built into the protocol. [5][8]
Management — Resuscitation
The unstable post-transplant child is resuscitated with the same discipline as any immunocompromised child, with the added layer of the transplant-specific complications. The fever in the child with a neutrophil count under zero point five times ten to the nine per litre is the febrile neutropenia, and the empiric antipseudomonal beta-lactam, such as the piperacillin-tazobactam, the ceftazidime or the meropenem, is given within one hour of the presentation after the blood cultures. The haemodynamically unstable child gets the empiric escalation with the aminoglycoside and the glycopeptide, and the child with the central line and the sepsis is assessed for the line removal. [12]
The blood products given to the post-transplant child are irradiated and leucodepleted throughout, and this is a non-negotiable rule that the exam tests relentlessly. Irradiation prevents the transfusion-associated graft-versus-host disease, in which the donor T-lymphocytes in the blood product engraft in the immunocompromised recipient and cause a fatal graft-versus-host reaction, and it is required for all the cellular products from the conditioning until at least six months after the transplant, or longer if the graft-versus-host disease persists. Leucodepletion reduces the cytomegalovirus transmission and the febrile reactions. The candidate who forgets the irradiation fails the question. [12]
Febrile neutropenia after the transplant
Dose
An antipseudomonal beta-lactam such as piperacillin-tazobactam, ceftazidime or meropenem as the empiric monotherapy, with the empiric addition of an aminoglycoside such as gentamicin and a glycopeptide such as vancomycin for the haemodynamically unstable child or when a resistant organism is suspected
The child with the severe sinusoidal obstruction syndrome is resuscitated for the fluid balance and the organ support while the defibrotide is started. The fluid restriction and the diuretics manage the ascites and the weight gain, the renal function is supported, and the child with the hepatorenal syndrome or the respiratory failure from the fluid overload is moved to the intensive care. The coagulopathy is corrected with the fresh frozen plasma and the vitamin K, and the thrombocytopenia is supported with the platelet transfusion. The defibrotide is the specific therapy, and it is started as soon as the diagnosis is made because the delay in the severe form is fatal. [9][10]
Management — Definitive & Stepwise
The definitive management of the transplant is the protocol-driven sequence of the conditioning, the infusion, the engraftment and the prophylaxis, delivered in the specialist centre over months to years. The conditioning begins the process, and the choice between the myeloablative and the reduced-intensity regimen is made by the disease, the comorbidity and the age. The myeloablative conditioning, with the total body irradiation or the high-dose busulfan, delivers the deepest graft-versus-leukaemia effect and is the standard for the aggressive leukaemia, while the reduced-intensity conditioning, with the fludarabine and the lower-dose alkylator, is reserved for the child with the comorbidity or the non-malignant disease where the full ablation is too toxic. [3]
[1] [11]The graft-versus-host prophylaxis is the centrepiece of the post-transplant management, and the candidate must hold the contemporary options. The traditional prophylaxis is the calcineurin inhibitor, the cyclosporine or the tacrolimus, combined with the short-course methotrexate, and it suppresses the alloreactive T-cells through the first months. The contemporary breakthrough is the post-transplantation cyclophosphamide, given at fifty milligrams per kilogram per day on days three and four after the infusion, which selectively kills the rapidly proliferating alloreactive T-cells while sparing the haematopoietic stem cells, and it has transformed the haploidentical transplant and now extends to the matched donor. The abatacept, added to the calcineurin inhibitor and the methotrexate, is approved for the prophylaxis in the unrelated donor transplant. [4][5]
Graft-versus-host disease prophylaxis
Dose
The calcineurin inhibitor such as cyclosporine or tacrolimus combined with the short-course methotrexate, or the post-transplantation cyclophosphamide at fifty milligrams per kilogram per day intravenously on days three and four, or the abatacept added to the calcineurin inhibitor and the methotrexate for the unrelated donor transplant
The established acute graft-versus-host disease is treated with the immunosuppression, and the severity determines the intensity. The grade one to two disease, the limited rash and the mild gut involvement, is treated with the topical glucocorticoid and the optimisation of the calcineurin inhibitor, while the grade three to four disease, the severe rash, the high stool volume and the bilirubin rise, is treated with the systemic glucocorticoid at one to two milligrams per kilogram per day of the methylprednisolone. The steroid-refractory disease, defined as the progression after a week or the failure to respond after two weeks, is treated with the ruxolitinib, the Janus kinase inhibitor approved for the steroid-refractory graft-versus-host disease, or the other second-line agents. [5]
The chronic graft-versus-host disease is treated with the systemic glucocorticoid as the first line, and the ruxolitinib is the approved second-line for the steroid-refractory disease. The management is multidisciplinary, because the sclerotic skin, the dry eyes, the oral lesions and the pulmonary involvement each demand the specialist input, and the physiotherapy, the ocular lubrication and the infection prophylaxis are woven through the long immunosuppression. The candidate should know that the chronic graft-versus-host disease is the chief driver of the late mortality and the quality-of-life burden, and that its prevention through the prophylaxis is better than its treatment. [6][7]
Defibrotide for the sinusoidal obstruction syndrome
Dose
Twenty-five milligrams per kilogram per day in four divided doses, given as the intravenous infusion over two hours every six hours, for a minimum of twenty-one days and continued until the resolution plus a further seven days
GATE
Specific Subtypes & Scenarios
The haploidentical transplant and the post-transplantation cyclophosphamide
The haploidentical transplant has moved from the experimental fringe to the mainstream, and the credit goes to the post-transplantation cyclophosphamide. A half-matched parent or sibling is available for almost every child, which solves the donor-shortage problem that once left the children without a matched donor untreated. The post-transplantation cyclophosphamide, given on days three and four, deletes the alloreactive T-cells after they have begun to proliferate, and it delivers the graft-versus-host prophylaxis that the mismatched setting demands. The candidate should know that the haploidentical transplant with the post-transplantation cyclophosphamide now approaches the outcomes of the matched unrelated transplant, and that the donor choice increasingly favours the readily available haploidentical family donor. [4]
The cord blood transplant
The cord blood transplant occupies the niche of the mismatched tolerance and the rapid availability. The cord unit, collected at the birth and cryopreserved, carries a lower cell dose and a slower engraftment than the adult donor, but its immunological immaturity tolerates the lower HLA match and reduces the graft-versus-host risk. The double-cord strategy, the infusion of two units, raises the cell dose and the engraftment speed, and the cord blood remains the option of choice for the child with the rare HLA type who lacks a matched adult donor. The slower engraftment extends the cytopenia and the infection risk, which is the trade-off the candidate must weigh. [2]
The transplant for the non-malignant disease
The transplant for the non-malignant disease is a growing share of the paediatric practice, and the candidate must hold its distinct logic. The severe aplastic anaemia, the inherited marrow failure and the primary immunodeficiencies are cured by the allogeneic transplant, and the sickle cell disease and the thalassaemia are increasingly transplanted with the curative intent. The conditioning for the benign disease often leans toward the reduced-intensity regimen to spare the fertility and the growth, and the graft-versus-leukaemia effect is irrelevant, so the graft-versus-host prophylaxis and the donor choice aim to minimise the complication rather than to exploit the alloreactivity. The matched sibling is the preferred donor, and the gene therapy is the emerging alternative for the haemoglobinopathy. [3][1]
The graft failure and the poor graft function
The graft failure is the failure of the donor cells to engraft or to sustain the engraftment, and it is a feared complication. The primary graft failure is the failure to reach the neutrophil engraftment by day twenty-eight, and the secondary graft failure is the loss of the counts after the initial engraftment. The workup demands the donor chimerism, the search for the rejection cause such as the viral infection or the alloimmune antibody, and the exclusion of the relapse. The management rests on the second transplant, the donor lymphocyte infusion or the boost, and the candidate should know that the poor graft function, the low counts with the full donor chimerism, is distinct from the graft failure and is managed with the cytokine support and the search for the suppressive cause. [11]
Complications & Pitfalls
The complications of the transplant are the early and the late, and the candidate must hold both because the late effects shape the survivorship. The early complications are the mucositis, the cytopenic sepsis, the acute graft-versus-host disease, the sinusoidal obstruction syndrome and the engraftment syndrome, and each is anticipated and managed through the first hundred days. The late complications are the chronic graft-versus-host disease, the opportunistic infection, the endocrine failure, the growth impairment, the infertility, the second malignancy and the cardiovascular disease, and the surveillance for these runs for life. The transplant is not over when the child leaves the ward, and the long-term follow-up is part of the management. [1][6]
The conditioning toxicity is the iatrogenic burden that the candidate must weigh against the curative intent. The total body irradiation damages the growth, the fertility, the thyroid and the lens, and it raises the second malignancy risk, which is why the contemporary paediatric protocols minimise its use. The busulfan and the cyclophosphamide carry the hepatic, the pulmonary and the gonadal toxicity, and the anthracycline adds the cardiotoxicity. The iron overload from the chronic transfusion adds to the hepatic burden, and the veno-occlusive risk is the sum of these. The endocrine late effects, the growth hormone deficiency, the hypothyroidism and the gonadal failure, are screened for in the late-effects clinic, and the fertility preservation is offered before the gonadotoxic conditioning. [3][9]
The infectious complications run the full spectrum, and the timeline is the clue. The bacterial sepsis and the candidal infection dominate the pre-engraftment cytopenia, the cytomegalovirus and the adenovirus emerge after the engraftment, and the Pneumocystis and the encapsulated bacteria follow the slow humoral reconstitution. The Epstein-Barr virus drives the post-transplant lymphoproliferative disease, especially in the T-cell deplete and the mismatched transplant, and the candidate should know the role of the rituximab and the reduction of the immunosuppression in its management. The prophylaxis with the aciclovir, the cotrimoxazole and the antifungal is protocol-driven and runs through the first year. [12]
Prognosis & Disposition
The prognosis after a paediatric transplant depends on the disease, the donor and the complications, and the candidate must carry the ranges. The matched sibling transplant of a benign disease in the remission carries a five-year survival of over ninety percent, while the unrelated or the haploidentical transplant of the refractory leukaemia with the severe graft-versus-host disease may sit under forty percent. The disease status at the transplant is the single most powerful predictor, and the child transplanted in the remission does far better than the child transplanted with the active disease. The severe graft-versus-host disease and the sinusoidal obstruction syndrome cut the survival sharply, and the infection remains the chief cause of the non-relapse mortality. [1][8]
The disposition of the post-transplant child is the specialist centre for the acute phase and the shared care for the long term. The conditioning, the infusion and the first hundred days are managed in the tertiary paediatric transplant centre, with the paediatric intensive care available for the complications. The child on the maintenance immunosuppression is followed in the outpatient clinic, with the shared care with the regional hospital and the primary care once the early complications have passed. The safety-net is the family taught to return at once with the fever, the rash or the diarrhoea, and the neutropenic precautions are reinforced at every visit. [12]
In Australia and Aotearoa New Zealand, the paediatric stem-cell transplant is delivered in the designated tertiary centres, with the Australian Bone Marrow Donor Registry and the international registries coordinating the unrelated donor search. The paediatric retrieval services transfer the unstable child from the regional hospital, and the shared-care model links the transplant centre with the regional oncology and the primary care for the long-term follow-up. The distance and the retrieval time are the regional realities that weight the early recognition and the stabilisation heavily in the exam, because a child far from the transplant centre depends on the regional hospital for the first response to the fever and the complication.
[1]The long-term survivor is followed in the late-effects clinic for life, and the surveillance is the reward of the cure. The annual review covers the growth and the endocrine function, the cardiac function after the anthracycline, the pulmonary function, the second malignancy surveillance, the iron overload and the bone health, and the fertility and the psychosocial support. The adolescent is counselled and transitioned into the adult late-effects service with the written survivorship plan and the named provider, and the chronic graft-versus-host disease is managed through the multidisciplinary clinic. The transplant, done well, is the start of a long and a monitored life. [6][7]
Special Populations
The immunocompromised child is the special population that defines the transplant, and the management is built around the prevention of the opportunistic infection. The bacterial sepsis, the fungal infection and the viral reactivation are the everyday threats, and the prophylaxis with the aciclovir, the cotrimoxazole and the antifungal runs through the cytopenia and the first year. The blood products are irradiated and the cytomegalovirus-safe throughout, and the child is monitored for the viral reactivations that suppress the marrow. The family is taught the neutropenic precautions and the strict return-with-fever rule, and the immunisation schedule is modified and delayed through the immune reconstitution. [12]
The infant and the very young child raise the distinct challenges of the conditioning toxicity and the growth. The total body irradiation is avoided where possible in the young child because of the devastating effect on the growth, the neurocognition and the second malignancy risk, and the busulfan-based myeloablative regimen is favoured. The infant with the primary immunodeficiency, such as the severe combined immunodeficiency, may be transplanted without the full conditioning in the urgency of the curative intent. The candidate should know that the age shapes the conditioning choice and the late-effects burden more than any other variable. [1][3]
The adolescent and the young adult are prepared for the transition to the adult service, and the reproductive and the fertility counselling are addressed before the gonadotoxic conditioning. The fertility preservation, the oocyte or the sperm cryopreservation, is offered before the transplant where the time and the pubertal stage allow, and the endocrine late effects and the second malignancy risk are discussed. The psychological burden of the long treatment, the adherence to the immunosuppression and the chronic graft-versus-host disease, and the educational and the vocational disruption are addressed before the handover. The young person leaves the paediatric service with the survivorship plan and the named adult provider. [6]
The socioeconomic disadvantage and the remoteness shape the access to the transplant and the long follow-up, and they are the reason the shared-care model and the retrieval system are so heavily emphasised. A child far from the transplant centre depends on the regional hospital and the primary care for the first response to the fever and the complication, and the adherence to the immunosuppression and the prophylaxis is a function of the social support. The indigenous, the migrant and the refugee child may face the additional barriers of the language, the health literacy and the donor availability, and the candidate who holds these in the plan demonstrates the holistic reasoning the boards reward. [1]
Evidence, Guidelines & Regional Differences
The landmark evidence that underpins the paediatric transplant is the product of decades of the international collaborative trials and the registry data, chiefly the Center for International Blood and Marrow Transplant Research and the European Society for Blood and Marrow Transplantation. The risk stratification of the transplant by the disease status and the donor, the refinement of the conditioning, the graft-versus-host prophylaxis and the defibrotide for the sinusoidal obstruction syndrome were all established through these registries and trials. The contemporary frontier is the post-transplantation cyclophosphamide, the abatacept, the ruxolitinib and the gene therapy, each of which has changed the practice within the last decade. [1][4]
The prophylaxis and the treatment of the graft-versus-host disease are the most rapidly evolving areas. The post-transplantation cyclophosphamide, validated in the haploidentical setting and now extended to the matched donor, has reduced the graft-versus-host incidence and the mortality across the donor types. The ruxolitinib, the Janus kinase inhibitor, is the approved therapy for the steroid-refractory acute and chronic graft-versus-host disease, and it has improved the outcomes of the disease that was once the chief cause of the non-relapse mortality. The abatacept, added to the calcineurin inhibitor and the methotrexate, is approved for the prophylaxis in the unrelated donor transplant. [4][7]
Across Australia, Aotearoa New Zealand, the United Kingdom, the United States and Canada, the allogeneic transplant is delivered in the designated centres with the donor search coordinated through the national and the international registries. The graft-versus-host prophylaxis, the conditioning intensity and the antimicrobial prophylaxis differ in their exact agents and timing between the international study groups, and the contemporary trend toward the post-transplantation cyclophosphamide is the common direction. The defibrotide for the sinusoidal obstruction syndrome and the ruxolitinib for the steroid-refractory graft-versus-host disease are broadly consistent across the regions, and the fellow should know the local protocol and the registry practice.
[1][4]The controversies in the field are the live ones. The optimal donor for the common indications, whether the matched unrelated or the haploidentical with the post-transplantation cyclophosphamide, is the question that the contemporary trials are settling in the paediatric leukaemia. The place of the gene therapy versus the transplant for the haemoglobinopathy is the emerging decision, and the reduced-intensity versus the myeloablative conditioning for the sickle cell disease is the trade-off of the toxicity and the graft stability. The candidate holds these as the open questions and cites the trials and the guidelines, rather than asserting a single answer where the evidence is still maturing. [3][4]
Exam Pearls
The high-yield facts for the exam are the ones that change a decision at the bedside. The neutrophil engraftment is the first of three consecutive days with an absolute neutrophil count of zero point five times ten to the nine per litre or above, and the platelet engraftment is seven consecutive days above twenty times ten to the nine per litre without the transfusion support. The acute graft-versus-host disease prophylaxis uses the calcineurin inhibitor with the methotrexate or the post-transplantation cyclophosphamide, never the glucocorticoid alone. The sinusoidal obstruction syndrome is treated with the defibrotide at twenty-five milligrams per kilogram per day in four divided doses, started early. [5][8]
Every blood product for the post-transplant child is irradiated and leucodepleted throughout, because the transfusion-associated graft-versus-host disease is fatal and preventable. The fever in the child with a neutrophil count under zero point five times ten to the nine per litre is the febrile neutropenia, and the antipseudomonal beta-lactam goes in within one hour after the blood cultures. The post-transplantation cyclophosphamide is given on days three and four, and its timing is what delivers the prophylaxis. The ruxolitinib is the approved therapy for the steroid-refractory acute and chronic graft-versus-host disease. [4][12]
The final pearls are the ones that catch the candidate who has learned the headline and forgotten the corner. The donor chimerism, not the count alone, confirms the engraftment. The chronic graft-versus-host disease, not the acute, is the chief driver of the late morbidity. The total body irradiation is avoided in the young child because of the growth and the second malignancy. The fertility preservation is offered before the conditioning, not after. The message for the exam is that the reasoning that holds the donor choice, the conditioning, the engraftment and the complications together is what carries the topic, and the candidate who reads the day from the infusion alongside the symptom has the framework for every post-transplant scenario. [6][11]
References
- [1]Kanate AS, Majhail NS, Savani BN Indications for Hematopoietic Cell Transplantation and Immune Effector Cell Therapy: Guidelines from the American Society for Transplantation and Cellular Therapy Biol Blood Marrow Transplant, 2020.PMID 32165328
- [2]Mangum DS, Caywood E A clinician's guide to HLA matching in allogeneic hematopoietic stem cell transplant Hum Immunol, 2022.PMID 35346535
- [3]Alsultan A, Abujoub R, Elbashir E The effect of intensity of conditioning regimen on the outcome of HSCT in children with sickle cell disease Clin Transplant, 2022.PMID 35929611
- [4]Bolaños-Meade J, Hamadani M, Wu J Post-Transplantation Cyclophosphamide-Based Graft-versus-Host Disease Prophylaxis N Engl J Med, 2023.PMID 37342922
- [5]Zeiser R, Blazar BR Acute Graft-versus-Host Disease - Biologic Process, Prevention, and Therapy N Engl J Med, 2017.PMID 29171820
- [6]Jagasia MH, Greinix HT, Arora M National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group report Biol Blood Marrow Transplant, 2015.PMID 25529383
- [7]Zeiser R, Polverelli N, von Bubnoff N Ruxolitinib for Glucocorticoid-Refractory Chronic Graft-versus-Host Disease N Engl J Med, 2021.PMID 34260836
- [8]Mohty M, Malard F, Alaskar AS Diagnosis and severity criteria for sinusoidal obstruction syndrome/veno-occlusive disease in adult patients: a refined classification from the European Society for Blood and Marrow Transplantation Bone Marrow Transplant, 2023.PMID 37095231
- [9]Larue M, Malard F, Alaskar AS Management of liver sinusoidal obstruction syndrome/veno-occlusive disease in adults: a 2025 perspective from an international expert group Bone Marrow Transplant, 2025.PMID 40263636
- [10]Aziz MT, Kakadiya PP, Kush SM Defibrotide: An Oligonucleotide for Sinusoidal Obstruction Syndrome Ann Pharmacother, 2018.PMID 28914546
- [11]Kharfan-Dabaja MA, Kumar A, Ayash L Standardizing Definitions of Hematopoietic Recovery, Graft Rejection, Graft Failure, Poor Graft Function, and Donor Chimerism in Allogeneic Hematopoietic Cell Transplantation Transplant Cell Ther, 2021.PMID 34304802
- [12]Lehrnbecher T, Robinson P, Fisher B Guideline for the Management of Fever and Neutropenia in Children With Cancer and Hematopoietic Stem-Cell Transplantation Recipients: 2017 Update J Clin Oncol, 2017.PMID 28459614