Paeds · haematology-oncology-and-transfusion
Leukaemia in children
Also known as Acute lymphoblastic leukaemia · Acute myeloid leukaemia · Childhood leukaemia · ALL · AML · Tumour lysis syndrome
Fellowship guide to leukaemia in children. Covers the separation of acute lymphoblastic from acute myeloid leukaemia, the peak age of two to five years, the presentation of pallor, bruising, fever and bone pain with circulating blasts, the recognition and prevention of tumour lysis syndrome with hyperhydration and rasburicase, the risk stratification by age, white cell count, cytogenetics and minimal residual disease, the risk-adapted multi-agent chemotherapy through induction, consolidation and maintenance, the central nervous system-directed therapy, the Down syndrome transient myeloproliferative disorder and myeloid leukaemia, and the oncologic emergencies of hyperleukocytosis, mediastinal mass and febrile neutropenia.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child is brought in pale, covered in bruises, with a fever that will not settle, and the blood film shows blasts. This is leukaemia until the bone marrow proves otherwise, and the first task at the bedside is to recognise the emergency and to move the child from an elective workup into a resuscitation. Leukaemia is the commonest malignancy of childhood, and the acuity of the presentation, with its threat of bleeding, sepsis and the metabolic disaster of tumour lysis, is what makes the first hours decisive. A delay of days can change the outcome, which is why every paediatrician must hold the diagnosis actively in mind. [9]
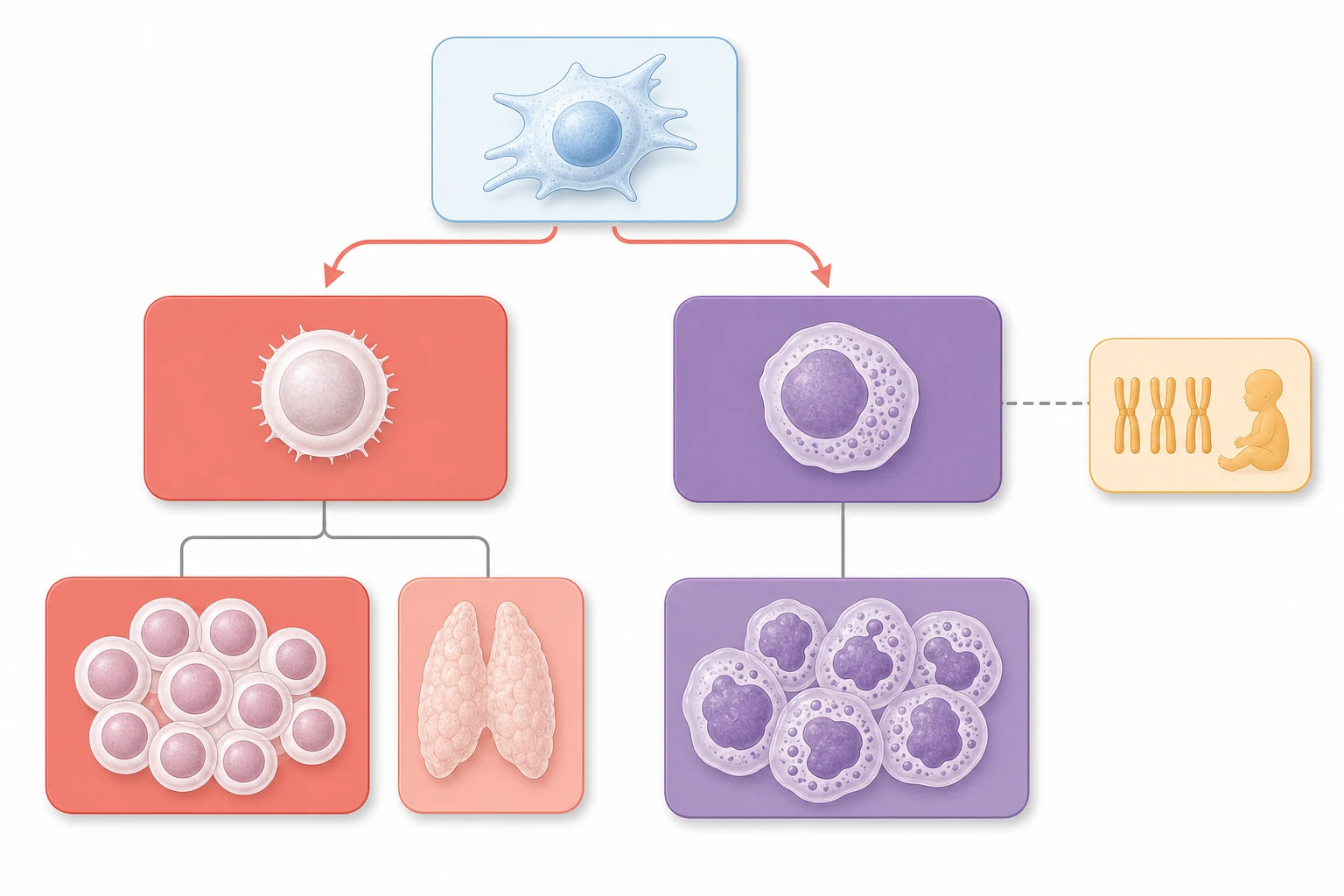
Leukaemia is a clonal malignancy of the haematopoietic precursor cell in which the normal maturation of a single lineage is arrested and the immature blast accumulates in the bone marrow. The accumulation crowds out the normal red cell, white cell and platelet precursors, producing the trilineage failure that explains almost every symptom, and the blasts spill into the peripheral blood. The disease is defined by the lineage of the arrested cell, and the separation into the lymphoid and the myeloid forms is the single most important early distinction because it determines the chemotherapy, the prognosis and the supportive care. [1]
The acute leukaemias dominate childhood, and of these acute lymphoblastic leukaemia is by far the commonest, accounting for roughly three quarters to four fifths of all childhood leukaemia. Acute myeloid leukaemia is less common but more evenly spread across the paediatric age range, and it carries a distinctive neonatal presentation in the infant with Down syndrome. The chronic leukaemias are rare in children and fall outside the everyday paediatric encounter, which is why this topic is built around the two acute forms and the emergencies they bring. [1]
The gravity of the diagnosis, and the remarkable improvement in its outlook, are why the topic sits at the centre of the fellowship examination. A candidate who can recognise the presentation, read the count and the film, chart the urgent diagnostic pathway, anticipate and prevent the oncologic emergencies, and explain the risk-adapted therapy to a family is demonstrating exactly the reasoning the boards reward. The contemporary survival of childhood acute lymphoblastic leukaemia now exceeds ninety percent in the best protocols, and the candidate who carries that number, alongside the humility of the emergencies, has the framework for the whole topic. [1][5]
Classification
Begin with the cell of origin, because the lineage is the organising principle of the whole topic. A lymphoblast gives rise to acute lymphoblastic leukaemia, and a myeloblast gives rise to acute myeloid leukaemia, and the two demand entirely different drugs, durations and supportive strategies. Within the lymphoid form the next split is between the B-cell precursor, which is the commonest childhood leukaemia of all, and the T-cell form, which tends to affect older boys with a high white cell count and a mediastinal mass. The myeloid form is subtyped by the degree and the direction of differentiation, from the undifferentiated to the megakaryocytic. [1]
A second, equally important classification runs through the genetics, because the cytogenetic and molecular lesion now drives the risk group more than any clinical feature. The favourable lesions in acute lymphoblastic leukaemia are the ETV6-RUNX1 fusion, once called TEL-AML1, and the high hyperdiploidy of more than fifty chromosomes, and together they account for a large share of standard-risk disease. The unfavourable lesions are the KMT2A rearrangement, once called MLL, which dominates the infant leukaemias, the hypodiploidy of fewer than forty-four chromosomes, the intrachromosomal amplification of chromosome twenty-one, and the BCR-ABL1 fusion of the Philadelphia chromosome. [1]
The clinical risk grouping fuses these genetic findings with two simple bedside features, the age and the initial white cell count, to produce the framework every candidate must carry. Standard risk, by the National Cancer Institute criteria, is a child aged one to under ten years with an initial white cell count under fifty times ten to the nine per litre, and high risk is anything outside that, the older child, the higher count, or the infant. The favourable and unfavourable genetics then refine the group further, and the minimal residual disease at the end of induction has the final word on the intensity that follows. [5]
B-cell precursor ALL
about 85 percent of ALL
- Commonest childhood cancer, peak two to five years
- Standard or high risk by age and white cell count
- Favourable ETV6-RUNX1 and high hyperdiploidy
- Minimal residual disease drives the risk group
T-cell ALL
about 15 percent of ALL
- Older boys, high white cell count
- Anterior mediastinal mass and superior vena cava obstruction
- Higher intensity protocols, central nervous system disease
- Airway compromise is an anaesthetic trap
Acute myeloid leukaemia
myeloid lineage
- Even age spread, neonatal peak in Down syndrome
- Intensive anthracycline and cytarabine blocks
- Acute promyelocytic leukaemia needs retinoic acid urgently
- Stem cell transplant for high-risk disease
Epidemiology & Risk Factors
The epidemiology of childhood leukaemia is dominated by a single peak that every paediatrician learns. Acute lymphoblastic leukaemia has its highest incidence between two and five years of age, at roughly three to four new cases per one hundred thousand children per year, and it remains the commonest malignancy of childhood across every studied population. Acute myeloid leukaemia is far less common, accounts for roughly fifteen to twenty percent of childhood leukaemia, and shows no single age peak, instead spreading across the paediatric range with a small neonatal cluster in the infant with Down syndrome. The male sex is slightly over-represented across the leukaemias. [1]
The predispositions that matter for the exam are few but high-yield. Down syndrome is the strongest single inherited predisposition, carrying a ten to twenty-fold raised lifetime risk of leukaemia and a unique neonatal presentation, the transient myeloproliferative disorder. The inherited bone marrow failure syndromes, including Fanconi anaemia, dyskeratosis congenita and Shwachman-Diamond syndrome, each carry a raised risk of myelodysplasia and acute myeloid leukaemia across childhood and young adulthood. Prior exposure to chemotherapy or radiation, the Li-Fraumeni and Noonan syndromes, and the ataxia-telangiectasia genotypes each add a background risk on which leukaemia may declare itself. [6]
The environmental contributors are weaker and less certain, and the candidate should hold them lightly. Ionising radiation is the best-established external cause, and a handful of chemotherapy agents, chiefly the alkylating agents and the topoisomerase inhibitors, raise the later risk of therapy-related myeloid neoplasia. The role of infections in the causation of childhood acute lymphoblastic leukaemia remains a hypothesis, with the delayed-exposure model proposing that a delayed and dysregulated response to a common infection drives the leukaemic clone in the susceptible child. The message for the exam is that most cases arise without an identifiable cause. [1]
Pathophysiology
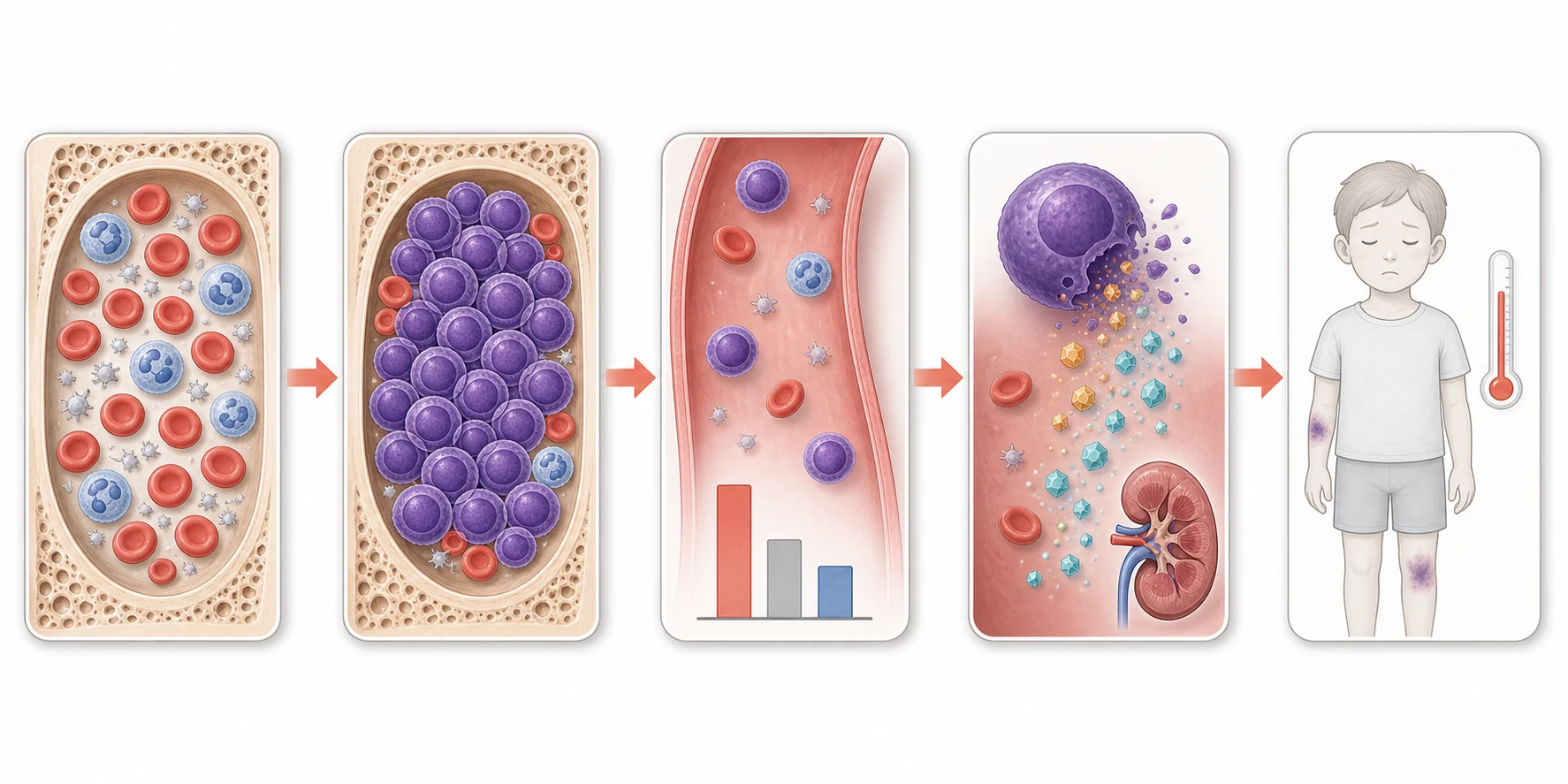
The disease begins in a single haematopoietic precursor cell that has acquired the genetic lesions that arrest its maturation and confer a survival and proliferative advantage. The arrested cell cannot complete its normal development into a mature lymphocyte or granulocyte, and instead it divides and accumulates as a blast. The expanding clone displaces the normal haematopoietic tissue from the marrow space, distorting the niche and the signalling that governs normal blood formation, and the trilineage failure of red cells, neutrophils and platelets is the direct consequence. The marrow failure, not the disease name, is what the child feels at the bedside. [1]
The characteristic cytogenetic and molecular lesions are not incidental, they are the engines of the disease and the targets of the modern therapy. The ETV6-RUNX1 fusion fuses two transcription factor genes and produces a leukaemia with an unusually favourable biology and a low relapse rate. The KMT2A rearrangements of infancy fuse the gene to one of many partners and produce an aggressive leukaemia of the very young that demands high-intensity therapy. The BCR-ABL1 fusion of the Philadelphia chromosome drives a constitutively active tyrosine kinase, and the contemporary treatment adds a kinase inhibitor to the chemotherapy to rescue a disease that was once uniformly fatal. [1]
The oncologic emergencies are pure pathophysiology, and they are the reason the first hours matter. The rapid turnover of a bulky tumour releases intracellular potassium, phosphate and urate faster than the kidneys can clear them, and the tumour lysis syndrome that follows can kill through arrhythmia and acute kidney injury within hours. A very high white cell count, over one hundred times ten to the nine per litre, makes the blood too viscous for the microcirculation and risks leukostasis in the brain and the lungs. The compromised marrow leaves the child defenceless against bacteria, so fever becomes an emergency in its own right. [3][7]
Clinical Presentation
The child with leukaemia walks in carrying the symptoms of the failing marrow, and the history usually tells the story before the count returns. The anaemia declares itself as pallor, tiredness, breathlessness on exertion, and in the young child as a new reluctance to walk or to feed. The thrombocytopenia declares itself as bruising out of proportion to the injury, petechiae over the lower limbs and the pressure points, epistaxis, gum bleeding, and heavy menstrual bleeding in the adolescent girl. The neutropenia declares itself as fever, mouth ulcers and bacterial infections that fail to settle. The tempo is often only a few weeks, and a parent will describe a child who was entirely well a month before. [9]
The physical signs refine the diagnosis, and the size of the liver, the spleen and the lymph nodes is the single most useful finding. An enlarged spleen and liver alongside lymphadenopathy point to extramedullary disease, because the leukaemic cells populate the reticuloendhelial system as they spread. Bone pain, a limp and a refusal to weight-bear are under-recognised presentations, often misattributed at first to trauma or to a transient synovitis, and they bring the child to the orthopaedic clinic or the emergency department before the blood count is ever checked. A testicular mass in the boy is a recognised site of relapse and is sought on every examination. [9]
The subtle and the atypical presentations are the ones that catch the unwary, and the boards test them deliberately. A child with a rheumatic-like limp, a normal or near-normal count, and a high sedimentation rate may have leukaemia with a low blast burden and is the classic mimic of juvenile idiopathic arthritis. An isolated thrombocytopenia labelled immune thrombocytopenia can be the first glimpse of an evolving leukaemia, which is why any child with a low platelet count has a full blood count and film examined for the other lineages and for blasts. The message is that the count and the film are checked personally, and that the unexplained or the atypical cytopenia is never dismissed. [9]
The central nervous system involvement is usually silent at diagnosis but is decisive for the treatment, because the cerebrospinal fluid is a sanctuary site that the standard chemotherapy cannot reach. A cranial nerve palsy, a new squint, headache, vomiting or a papilloedema raise the possibility of meningeal disease, and the diagnostic lumbar puncture both detects and treats it through the intrathecal therapy. The contemporary protocols deliver central nervous system-directed therapy to every child regardless of the initial status, because the prevention of the meningeal relapse is one of the great successes of the modern era. [1]
Differential Diagnosis
The differential of a child with circulating blasts is short, because the blasts settle it, but the differential of a child with an unexplained cytopenia and a count not yet back is where the errors are made. The first separation is between the marrow malignancies and the marrow failure, between a full marrow and an empty one. Acute leukaemia fills the marrow with blasts, while acquired aplastic anaemia empties it and leaves fat, and the bone marrow aspirate and trephine biopsy settle the question within hours. The solid tumours that seed the marrow, neuroblastoma above all, produce the small-round-blue-cell picture rather than a sheet of uniform blasts. [1]
The benign mimics of leukaemia must be excluded, because treating them as malignancy is as harmful as missing a malignancy. A severe viral infection, an Epstein-Barr mononucleosis or a parvovirus B19, can produce an atypical lymphocytosis and a transient cytopenia that resolves as the child recovers. A profound megaloblastic anaemia from folate or vitamin B12 deficiency can drop all three lines and shows macrocytosis and hypersegmented neutrophils on the film. A transient leucemoid reaction from a severe infection or a haemolysis can raise the white cell count impressively but shows a mature neutrophilia rather than blasts. [9]
Acute lymphoblastic leukaemia
full marrow, lymphoblasts
- Sheets of uniform blasts on the marrow aspirate
- Flow cytometry defines the lymphoid lineage
- Hepatosplenomegaly, lymphadenopathy, mediastinal mass
- Cytogenetics and molecular testing drive the risk group
Acute myeloid leukaemia
myeloblasts, granules
- Myeloperoxidase-positive blasts with Auer rods
- Acute promyelocytic leukaemia causes disseminated coagulation
- More intensive blocks over a shorter course
- Stem cell transplant for high-risk cytogenetics
Aplastic anaemia
empty marrow
- Hypocellular marrow with fat replacement, no clone
- No organomegaly and no circulating blasts
- Defined by the Camitta severity criteria
- Treated by transplant or immunosuppression
Neuroblastoma marrow disease
small round blue cell
- Clumps of small round blue cells in the marrow
- Adrenal or paraspinal primary mass
- Raised urinary catecholamines
- Raccoon eyes from orbital metastasis
The chief diagnostic pitfall for the fellow is the case that sits on the border. The child with evolving aplastic anaemia may first present with an isolated thrombocytopenia that is labelled immune thrombocytopenia, and only a careful blood film and a marrow biopsy weeks later settle the question. The infant with the transient myeloproliferative disorder of Down syndrome may show blasts indistinguishable from a true leukaemia, and the distinction rests on the natural history and the surveillance, not on the single film. The lesson is that the marrow aspirate with the full ancillary panel, read with the film and the clinical picture, is the arbiter. [6]
Clinical & Bedside Assessment
The bedside assessment of the child with suspected leukaemia is a search for the clues that confirm the direction and that flag the unstable child who needs resuscitation before investigation. The assessment begins with the airway, the breathing and the circulation, because a child with a mediastinal mass, a severe anaemia, or an active bleed is in danger before any diagnosis is reached. Once the child is safe, the focused history turns to the tempo of the symptoms, the bleeding and the fever, the bone and the joint pain, the drug and toxin exposures, and the family history of cancer or marrow failure. [9]
The examination is systematic and takes only a few minutes, but each finding carries weight. The skin is inspected for pallor, bruising, petechiae, and the cafe-au-lait and pigmentary changes of the inherited marrow failure syndromes. The lymph node chains are palpated for size, consistency and distribution, the abdomen for the liver and the spleen, and the chest for the signs of a mediastinal mass, an effusion or a consolidation. The testes are examined in the boy, and the nervous system for the cranial nerve palsies of meningeal disease. The growth is plotted, and the stigmata of Down syndrome are sought. [9]
The focused examination of the child with suspected leukaemia
Assess the airway, breathing and circulation first, looking for stridor, respiratory distress, and the pallor and tachycardia of severe anaemia
Inspect the skin for pallor, bruising, petechiae and the pigmentary stigmata of inherited marrow failure
Inspect the mouth for mucosal bleeding, ulceration and gum hypertrophy
Palpate all lymph node chains and examine the abdomen for hepatosplenomegaly
Auscultate the chest for a mediastinal mass, effusion or consolidation, and assess for superior vena cava obstruction
Examine the testes in the boy and perform a focused neurological examination for cranial nerve palsies
Plan the urgent blood tests, secure venous access, and arrange transfer to the specialist centre
The severity of the bleeding and the haemodynamic consequences of the anaemia are judged at the bedside and decide how fast the transfusion must be given. Active mucosal bleeding, a rapidly falling haemoglobin, or signs of shock override any plan for an elective workup and demand immediate stabilisation. The teaching of the family is part of the examination, because a child sent home or transferred while awaiting the marrow result must be told to return at once with fever or new bleeding. The neutropenic precautions, the avoidance of rectal temperatures, and the need for urgent presentation with any fever are explained before the family leaves. [7]
Investigations
The investigation moves in two steps, the bedside blood tests that confirm the direction, and the bone marrow examination that delivers the named diagnosis and the risk group. The first-line panel is the full blood count with the differential, the peripheral blood film, the reticulocyte count, the blood group and screen, the coagulation screen, and the electrolytes, renal and liver function, together with the lactate dehydrogenase, the urate, the calcium and the phosphate. The film is read personally by the clinician with the haematologist, because the presence of blasts can change the working diagnosis in seconds. [1]
The blood count patterns at presentation are varied, and the candidate must know them all. A low haemoglobin, a low neutrophil count and a low platelet count with circulating blasts is the classic pattern, but a normal or even a high white cell count with blasts is equally consistent with leukaemia, and the occasional child presents with a near-normal count and a misleading film. The lactate dehydrogenase is raised in proportion to the tumour burden, and the urate is raised in the high-turnover disease, and together they flag the child at risk of the tumour lysis syndrome. The coagulation screen is essential, because the acute promyelocytic leukaemia carries a high risk of disseminated intravascular coagulation. [1][3]
The bone marrow aspirate and trephine biopsy together are the diagnostic standard, and they are performed at the posterior iliac crest once the child is stable. The aspirate provides the cells for the morphology, for the flow cytometry that defines the lineage and the immunophenotype, and for the cytogenetics and the molecular panel that drive the risk stratification. The trephine biopsy provides the architecture and the cellularity, and it is especially valuable when the aspirate yields a dry tap. The diagnosis rests on the integration of the morphology, the immunophenotype and the genetics, and the contemporary classification is built on all three. [1]
Across Australia, Aotearoa New Zealand, the United Kingdom, the United States and Canada, the bone marrow aspirate with flow cytometry and conventional cytogenetics is the standard diagnostic procedure for a suspected childhood leukaemia. The molecular panel sent on the marrow, and the specific risk-stratification genes, differ between the international ALL and AML study groups, and the fellow should know the local protocol. The lumbar puncture with the intrathecal therapy is performed at diagnosis in the specialist centre, and the cerebrospinal fluid is examined for the blast cells of the central nervous system disease.
[1][2]Management — Resuscitation
The unstable child with leukaemia is resuscitated before the diagnosis is pursued, and the resuscitation rests on three legs: the transfusion of red cells and platelets, the prevention and the treatment of the oncologic emergencies, and the empiric cover of the febrile neutropenia. Red cell transfusion is given for the symptomatic anaemia or a haemoglobin that is falling fast, and it is given slowly in the chronically severely anaemic child to avoid the circulatory overload that a rapid rise can precipitate. [7]
The blood products given to a child with a suspected leukaemia must be irradiated and leucodepleted. Irradiation prevents the transfusion-associated graft-versus-host disease, a fatal complication in which the donor T-lymphocytes engraft in the immunocompromised recipient, and it is required for all the cellular products in the child with a known or suspected malignancy. Leucodepletion reduces the febrile and the cytomegalovirus-transmission risk. Platelet transfusion is held for a platelet count under ten times ten to the nine per litre in the stable child, under twenty in the febrile or the bleeding child, and at a higher threshold for the active bleeding or before a procedure. [7]
Tumour lysis syndrome is anticipated and prevented from the moment a high-risk leukaemia is suspected, before the first dose of chemotherapy. Hyperhydration with an isotonic fluid without potassium, started early and run to maintain a high urine output, is the foundation. Rasburicase, a recombinant urate oxidase, is given to the high-risk child to break down the urate already formed, and it is far more effective than the allopurinol, which only blocks the new urate formation. The potassium, the phosphate, the calcium and the creatinine are measured every four to six hours, and the urine output is maintained with a careful fluid balance and the strict avoidance of potassium in the fluids. [3][4]
Tumour lysis prophylaxis for a high-risk leukaemia
Dose
Hyperhydration with isotonic fluid without potassium at two to three litres per square metre per day to keep the urine output above two millilitres per kilogram per hour, with rasburicase at zero point one five or zero point two milligrams per kilogram as a single dose or daily for up to five days, or allopurinol at ten milligrams per kilogram per day in divided doses for the low-risk child
The child with a fever and a neutrophil count under zero point five times ten to the nine per litre has the febrile neutropenia, and the empiric antibiotic is given within one hour of the presentation. An antipseudomonal beta-lactam, such as the piperacillin-tazobactam, the ceftazidime or the meropenem, is the standard monotherapy, and an aminoglycoside and a glycopeptide are added for the haemodynamically unstable child or when a resistant organism is suspected. The blood cultures are drawn before the first dose, and the child is monitored closely for the first twenty-four hours. For the child with the hyperleukocytosis and the signs of the leukostasis, a white cell count over one hundred times ten to the nine per litre with the respiratory or the neurological compromise, the cytoreduction with the leukapheresis or the hydroxyurea is coordinated with the specialist team, and the red cell transfusion is withheld until the count falls to avoid worsening the viscosity. [7]
Management — Definitive & Stepwise
The definitive therapy is risk-stratified and multi-agent, and it begins the moment the bone marrow delivers the named diagnosis and the risk group. The treatment of the acute lymphoblastic leukaemia runs through the phases of the remission induction, the consolidation, the interim maintenance, the delayed intensification and the maintenance, over two to three years, with the central nervous system-directed therapy woven through every phase. The backbone includes the glucocorticoids, the vincristine, the asparaginase and the anthracyclines, and the minimal residual disease at the end of the induction is the key determinant of the intensity that follows. The contemporary survival now exceeds ninety percent for the standard-risk disease. [1][5]
[1] [7]The induction phase achieves the remission in over ninety-five percent of the children within four weeks, and it rests on the glucocorticoid, the vincristine, the asparaginase and the anthracycline, with the intrathecal therapy from day one. The consolidation and the intensification phases that follow deepen the remission and target the residual disease, and the maintenance phase, typically two years for the girls and three for the boys, sustains the remission with the daily mercaptopurine and the weekly methotrexate. The minimal residual disease, measured by the flow cytometry or the molecular method at the end of the induction, stratifies the child into the standard, the medium and the high risk, and it guides the escalation or the de-escalation of the therapy. [5]
VADA
The acute myeloid leukaemia is treated with the intensive blocks of the anthracycline and the cytarabine, over a much shorter course of roughly six months, and it carries a higher early mortality and a lower overall survival than the lymphoblastic form. The stem cell transplant in the first complete remission is reserved for the high-risk cytogenetics, the refractory disease and the relapse, because the modern chemo-therapy cures the intermediate-risk disease without it. The acute promyelocytic leukaemia is the exception that proves the rule, because its distinctive coagulopathy makes it an emergency and its distinctive biology makes it exquisitely sensitive to the all-trans retinoic acid and the arsenic trioxide, which are started on suspicion, not after confirmation. [2]
Acute lymphoblastic leukaemia induction backbone
Dose
A four-week induction with vincristine, a glucocorticoid of dexamethasone or prednisone, pegaspargase as the asparaginase, and daunorubicin added for the high-risk disease, with intrathecal cytarabine or methotrexate from day one
Specific Subtypes & Scenarios
Down syndrome and the transient myeloproliferative disorder
The neonate with Down syndrome holds a unique position in this topic, because the extra chromosome twenty-one carries a set of mutations in the GATA1 gene that uniquely predispose to a self-limiting neonatal leukaemoid reaction and to a true leukaemia. The transient myeloproliferative disorder affects roughly one in ten newborns with the trisomy twenty-one and presents in the first weeks of life with blasts in the blood, often with the jaundice, the hepatosplenomegaly and a leukocytosis, and it resolves spontaneously in most. A minority, however, develop a life-threatening complication of the hepatic fibrosis, and roughly ten to twenty percent of the survivors go on to develop the acute megakaryoblastic leukaemia within the first few years of life. [6][8]
WATCH
The acute megakaryoblastic leukaemia of Down syndrome is treated with a tailored protocol that exploits its remarkable sensitivity to the cytarabine, and the outcomes are now among the best in the paediatric acute myeloid leukaemia when the diagnosis is made correctly. The pitfall for the fellow is to mistake the transient disorder for a true leukaemia and to over-treat the neonate, or to miss the later leukaemia by lapsing the surveillance. Every Down syndrome neonate with the blasts is referred to the paediatric haematology for the monitoring that distinguishes the two. [6]
The infant leukaemia
The infant under one year with the leukaemia is a special scenario because the biology, the genetics and the treatment are all distinct from the older child's. The KMT2A rearrangement dominates the infant leukaemia and confers an aggressive biology that demands the high-intensity therapy, and the infant steroid toxicity and the infection risk demand a careful supportive care. The contemporary infant protocols have improved the outcome, but the infant leukaemia remains one of the highest-risk presentations in the paediatric oncology. [1]
The Philadelphia chromosome positive leukaemia
The BCR-ABL1 fusion of the Philadelphia chromosome, once a uniformly fatal lesion in the childhood acute lymphoblastic leukaemia, has been transformed by the addition of the tyrosine kinase inhibitor to the chemotherapy. The imatinib and the dasatinib, added to the standard backbone, have raised the survival of this disease into the range of the other high-risk leukaemias, and the lesson is that the molecular diagnosis now directly enables the targeted therapy. The kinase inhibitor is continued through the maintenance, and the stem cell transplant is reserved for the refractory disease. [1][10]
The relapse
The relapsed acute lymphoblastic leukaemia remains the commonest cause of the death from the childhood cancer, and it most often declares itself in the marrow, with the central nervous system and the testis as the other sanctuary sites. The detection rests on the marrow surveillance and the minimal residual disease monitoring, and the treatment rests on the re-induction, the risk stratification, and the stem cell transplant for the high-risk relapse. The contemporary immunotherapies, including the blinatumomab and the chimeric antigen receptor T-cell therapy, have transformed the outlook of the relapsed B-cell disease. [10]
Complications & Pitfalls
The complications of the childhood leukaemia divide into the disease-related and the treatment-related, and the fellow must hold both in mind because the iatrogenic harm can rival the disease. The disease-related complications are the bleeding from the thrombocytopenia, the infection from the neutropenia, the anaemic failure of the heart and the brain, and the organ infiltration that produces the superior mediastinal syndrome, the leukostasis and the tumour lysis. These are the complications that drive the resuscitation, and each is anticipated from the moment the count is seen. [7]
The treatment-related complications are the costs of the therapy that saves the child. The mucositis and the profound neutropenic sepsis of each chemotherapy cycle demand the aggressive supportive care and the rapid empiric antibiotics. The anthracycline cardiotoxicity is cumulative and dose-dependent, and the contemporary protocols cap the lifetime dose to protect the heart. The second malignancies of the alkylating agents and the topoisomerase inhibitors, the endocrine late effects of the cranial radiation, and the neurocognitive late effects of the central nervous system therapy are the late costs that shape the survivorship plan. [1][5]
The procedural complications of the marrow sampling and the central line are few but real. The bone marrow aspirate and trephine biopsy are the safe procedures in the trained hands, with the posterior iliac crest the standard site, and the chief risks are the bleeding in the thrombocytopenic child, the infection in the neutropenic child, and the rare anaesthetic complication in the child with the mediastinal mass. The central line is the lifeline of the therapy, and its infection and its occlusion are the everyday complications of the long treatment. [1]
Prognosis & Disposition
The prognosis of the childhood leukaemia is one of the great successes of the modern oncology, and the candidate must carry the numbers. The contemporary five-year survival of the acute lymphoblastic leukaemia exceeds ninety percent in the best protocols, with the standard-risk disease approaching ninety-five percent, and the survival of the acute myeloid leukaemia sits around sixty-five to seventy percent. The infant leukaemia, the relapse and the unfavourable cytogenetics remain the chief challenges, and the cure of these drives the contemporary research. These numbers are the background against which the family is counselled and the plan is built. [1][2]
The disposition of the child is determined by the diagnosis and the stability. The unstable child and every child with a new diagnosis of leukaemia are managed in a specialist paediatric oncology centre, with the paediatric intensive care available for the oncologic emergencies. The child on the maintenance therapy is followed in the outpatient clinic, with the home administration of the mercaptopurine and the methotrexate and the regular review of the count and the marrow. The safety-net is the family taught to return at once with the fever or the new bleeding. [7]
In Australia and Aotearoa New Zealand, the child with a new diagnosis of leukaemia is managed in a tertiary paediatric oncology centre, with the paediatric retrieval services transferring the unstable child from the regional or the rural hospital. The family is supported by the paediatric oncology group, the social work and the educational liaison, and the long-term survivor is followed in the late-effects clinic. The regional differences are chiefly in the distance and the retrieval time, which is why the early recognition and the stabilisation in the referring hospital are so heavily weighted in the exam.
[1]The long-term surveillance of the survivor is one of the most rewarding parts of the specialty, because the late effects can be caught and managed. The survivor has an annual review of the heart for the anthracycline cardiotoxicity, the endocrine function for the growth and the fertility, and the neurocognition for the central nervous system therapy, and the second malignancy surveillance runs throughout the life. The adolescent is counselled and transitioned into the adult late-effects service with a written survivorship plan and a named provider. [5]
Special Populations
The neonate with Down syndrome is the special population that sits at the heart of this topic, and the screening for the transient myeloproliferative disorder is built into the newborn care of these infants. A full blood count with a differential is performed in the first weeks of life, and any blast excess is referred to the paediatric haematology for the GATA1 testing and the surveillance that follows. The family is counselled on the self-limiting nature of the transient disorder in most, on the risk of the later leukaemia, and on the surveillance plan. [8]
The immunocompromised child, whether on the chemotherapy, after the stem cell transplant, or with a primary immunodeficiency, holds a special position because the marrow suppression and the opportunistic infection are intertwined. The bacterial sepsis, the fungal infection and the viral reactivation are the everyday threats, and the management rests on the prophylaxis, the surveillance and the rapid empiric therapy. The blood products are irradiated and the cytomegalovirus-safe throughout, and the child is monitored for the viral reactivations that can suppress the marrow. [7]
The socioeconomic disadvantage, the remoteness, and the migrant or the refugee status shape the access to the diagnosis and the treatment, and they are the reason the early recognition in the primary care and the regional hospital is so heavily emphasised. A child far from a specialist centre may first present to a clinician who sees few such cases, and the count and the film that flag the leukaemia are the bridge to the retrieval and the specialist care. The adherence to the long maintenance therapy is itself a function of the social support, and it is addressed proactively in the family plan. [9]
The adolescent with the leukaemia is prepared for the transition to the adult service with the counselling and the documentation that make it safe. The reproductive and the fertility counselling, the endocrine late effects, the second malignancy risk, and the psychological burden of the diagnosis are addressed before the handover. The adolescent is offered the fertility preservation before the gonadotoxic therapy, and the young person leaves the paediatric service with a survivorship plan and a named adult provider. [5]
Evidence, Guidelines & Regional Differences
The landmark evidence that underpins the modern treatment of the childhood acute leukaemia is the product of half a century of successive international collaborative trials, and it is the reason the survival has risen from a uniformly fatal disease to a ninety percent cure in the lymphoblastic form. The risk stratification by the age, the initial white cell count, the cytogenetics and the early response, the backbone of the therapy with the glucocorticoids, the vincristine, the asparaginase and the anthracyclines, and the central nervous system-directed therapy, were all refined through these trials. The molecular classification and the minimal residual disease monitoring are the contemporary frontier. [1][5]
The treatment of the acute myeloid leukaemia in children rests on the intensive multi-agent chemotherapy built around the anthracycline and the cytarabine, with the stem cell transplant reserved for the high-risk and the refractory disease, and the supportive care that manages the profound marrow suppression of each cycle. The distinctive biology of the Down syndrome myeloid leukaemia, with its GATA1 mutation and its cytarabine sensitivity, is treated on a tailored protocol that exploits its favourable profile. The acute promyelocytic leukaemia is transformed by the all-trans retinoic acid and the arsenic trioxide. [2]
The transfusion thresholds and the blood product selection in the child with the leukaemia are broadly consistent across Australia, Aotearoa New Zealand, the United Kingdom, the United States and Canada, with the irradiated and the leucodepleted products the standard for the immunocompromised child. The risk-adapted protocols differ in their exact drugs and their timing, and the choice of the rasburicase versus the allopurinol for the tumour lysis prophylaxis is settled by the risk stratification but varies in the cost and the availability by region. The fellow should know the local protocol and the regional blood service guidance.
[3][4]The controversies in the field are the live ones. The optimal duration and the intensity of the maintenance therapy, the role of the stem cell transplant in the high-risk disease, the place of the novel immunotherapies in the front-line treatment, and the timing of the tyrosine kinase inhibitor in the Philadelphia positive disease are the questions that occupy the contemporary trials. The fellow holds these as open questions, and cites the trials and the guidelines, rather than asserting a single answer where the evidence is still maturing. [1][10]
Exam Pearls
The high-yield facts for the exam are the ones that change a decision at the bedside. Acute lymphoblastic leukaemia is the commonest childhood cancer with a peak at two to five years, and the standard risk is the age of one to under ten years with a white cell count under fifty times ten to the nine per litre. A pale, bruising, febrile child with the circulating blasts has the leukaemia until proven otherwise, and the first priority is the resuscitation of the unstable elements before the diagnosis is pursued. [1]
Tumour lysis syndrome is prevented before the chemotherapy with the hyperhydration, the rasburicase for the high-risk child, and the four-to-six-hourly biochemistry, and the rasburicase is contraindicated in the glucose-6-phosphate dehydrogenase deficiency. Febrile neutropenia gets the antipseudomonal beta-lactam within one hour after the blood cultures. A white cell count over one hundred times ten to the nine per litre risks the leukostasis and needs the urgent cytoreduction. The acute promyelocytic leukaemia needs the all-trans retinoic acid on suspicion, because of the disseminated intravascular coagulation. [3][7]
The final pearls are the ones that catch the candidate who has learned the headline and forgotten the corner. The bone marrow aspirate is taken from the posterior iliac crest in the child, never the sternum. The platelet transfusion threshold is higher in the bleeding or the pre-procedure child than in the stable child. The mediastinal mass is never sedated before the airway is secured. The first sign of a relapse in the boy may be a testicular mass. The message for the exam is that the corners are where the marks are won, and the reasoning that holds the resuscitation before the diagnosis, the risk stratification at the centre, and the family at the heart is what carries the topic. [7][9]
References
- [1]Hunger SP, Mullighan CG Acute Lymphoblastic Leukemia in Children N Engl J Med, 2015.PMID 26465987
- [2]Rubnitz JE, Kaspers GJL How I treat pediatric acute myeloid leukemia Blood, 2021.PMID 34115839
- [3]Howard SC, Avagyan A, Workeneh B Tumour lysis syndrome Nat Rev Dis Primers, 2024.PMID 39174582
- [4]Perissinotti AJ, Bishop MR, Bubalo J Expert consensus guidelines for the prophylaxis and management of tumor lysis syndrome in the United States: Results of a modified Delphi panel Cancer Treat Rev, 2023.PMID 37579533
- [5]Cooper SL, Brown PA Treatment of pediatric acute lymphoblastic leukemia Pediatr Clin North Am, 2015.PMID 25435112
- [6]Verma A, Lupo PJ, Shah NN Management of Down Syndrome-Associated Leukemias: A Review JAMA Oncol, 2023.PMID 37440251
- [7]Prusakowski MK, Cannone D Pediatric Oncologic Emergencies Hematol Oncol Clin North Am, 2017.PMID 29078932
- [8]Sas V, Blag C, Zaharie G Transient leukemia of Down syndrome Crit Rev Clin Lab Sci, 2019.PMID 31043105
- [9]Fragkandrea I, Nixon JA, Panagopoulou P Signs and symptoms of childhood cancer: a guide for early recognition Am Fam Physician, 2013.PMID 23939697
- [10]Bhojwani D, Pui CH Relapsed childhood acute lymphoblastic leukaemia Lancet Oncol, 2013.PMID 23639321