Paeds · haematology-oncology-and-transfusion
Megaloblastic and macrocytic anaemia
Also known as Megaloblastic anaemia · Vitamin B12 deficiency · Cobalamin deficiency · Folate deficiency · Macrocytic anaemia · Pernicious anaemia
Fellowship guide to megaloblastic and macrocytic anaemia in children. Covers the distinction between macrocytosis as a mean corpuscular volume above the age-specific range and megaloblastic anaemia as the impaired-DNA-synthesis subset with hypersegmented neutrophils and macro-ovalocytes, the folate and methionine remethylation cycle in which methionine synthase needs B12 and thymidylate synthase needs folate, the infant of the vegan or deficient mother with developmental regression, the methylmalonic acid and homocysteine metabolite pair that separates B12 from folate deficiency, the cardinal rule never to give folic acid alone, the hydroxocobalamin intramuscular replacement schedule of the British Society for Haematology, and the inherited causes of transcobalamin II deficiency and Imerslund-Graesbeck syndrome.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A pale, irritable infant who has stopped smiling, whose blood film shows red cells larger than they should be and a neutrophil with too many lobes, carries a single missing vitamin that is quietly stalling the division of every fast-growing cell in the body. Megaloblastic anaemia is the anaemia of impaired DNA synthesis, in which a deficiency of vitamin B12 or folate slows nuclear maturation so that the cell enlarges but cannot divide, and the marrow fills with oversized, asynchronous precursors while the blood carries oversized oval red cells and hypersegmented neutrophils. It is one of the most rewarding diagnoses in paediatrics because, caught early, it is fully reversible, and missed, it leaves a child with permanent neurological injury. [1][2]
The vocabulary matters because the two words are not synonyms. Macrocytosis is a size, a mean corpuscular volume above the age-specific reference range, and it has many causes that have nothing to do with DNA synthesis. Megaloblastic anaemia is the specific subset of macrocytosis born of impaired DNA synthesis, and it carries its own morphology of macro-ovalocytes and hypersegmented neutrophils. The clinician who sees a high mean corpuscular volume therefore asks two questions in sequence, which nutrient is missing if it is megaloblastic, and what else could enlarge the red cell if it is not. [7]
Three ideas make this topic central to the paediatric exam. The first is recognition of the infant of the vegan or deficient mother, because the breastfeeding infant is wholly dependent on maternal stores and can deplete a marginal supply within months, presenting with developmental regression that is reversible if caught. The second is the metabolite logic, because methylmalonic acid and homocysteine separate B12 from folate deficiency when the vitamin levels are borderline. The third is the cardinal safety rule, that folic acid must never be given alone until B12 is excluded, because it can precipitate subacute combined degeneration of the spinal cord. The British Society for Haematology guideline of Devalia and colleagues sets the diagnostic and treatment standard. [3][1]
Classification
The first classification the clinician makes is between the megaloblastic and the non-megaloblastic causes of a large red cell, and it rests on the blood film rather than the size alone. The megaloblastic macrocytes are oval, and they are accompanied by the hypersegmented neutrophil with five or more lobes, the morphological signature of stalled DNA synthesis. The non-megaloblastic macrocytes are round, the neutrophil lobe count is normal, and they reflect something other than impaired division, a high reticulocyte count, a liver, a thyroid, or a diseased marrow. [7]
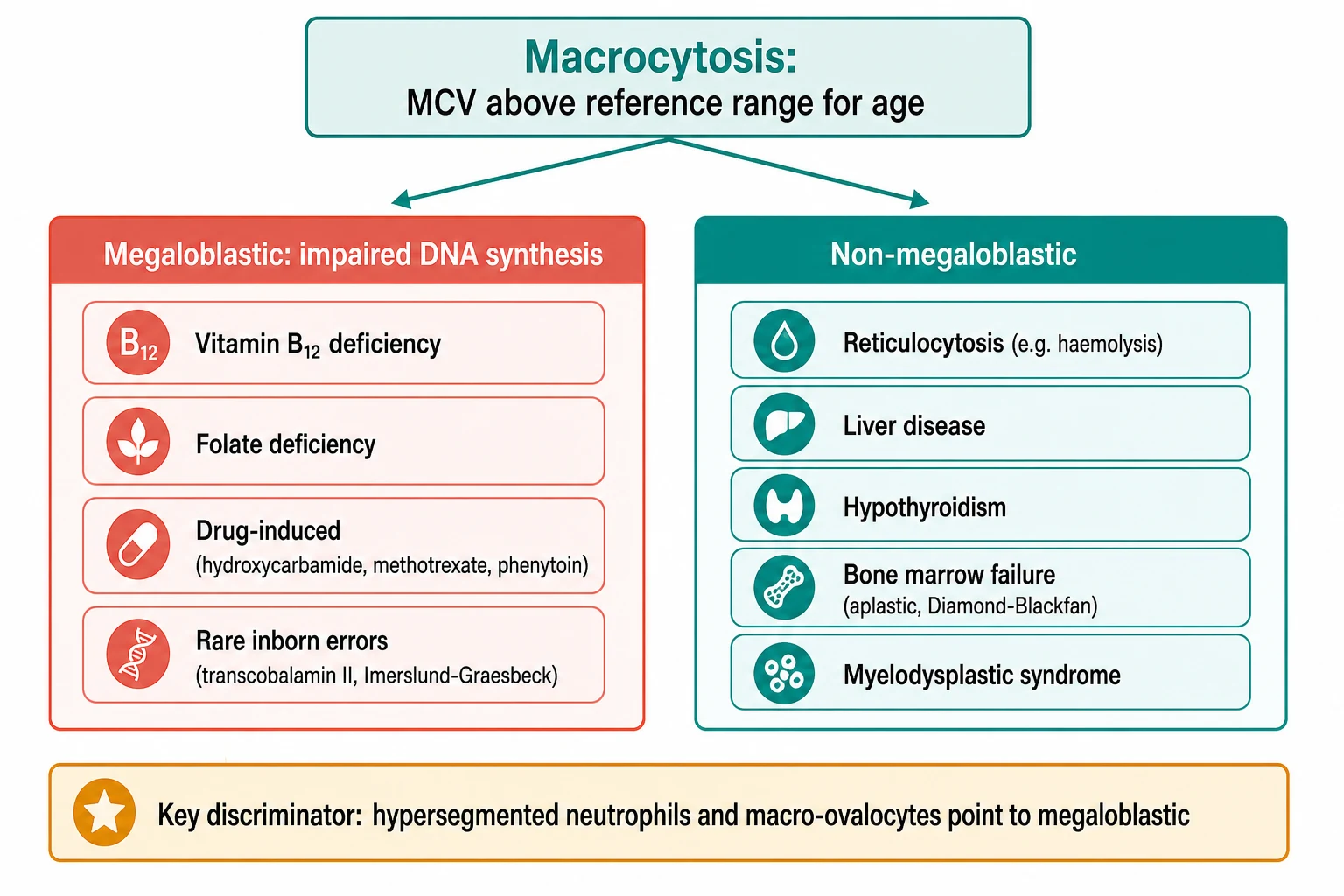
Among the megaloblastic causes, the dominant pair is vitamin B12 and folate deficiency, and they are split again by the metabolites and by the neurological examination. The drug-induced megaloblastosis of hydroxycarbamide in sickle cell disease, of methotrexate and trimethoprim that antagonise folate, and of phenytoin is the common iatrogenic form seen in paediatric haematology. The rare inborn errors, transcobalamin II deficiency, Imerslund-Graesbeck syndrome, congenital intrinsic factor deficiency, and hereditary orotic aciduria, complete the megaloblastic list. The non-megaloblastic list is led by the reticulocytosis of haemolysis or bleeding, followed by liver disease, hypothyroidism, alcohol, and the bone marrow failure and myelodysplastic syndromes. [1]
Epidemiology & Risk Factors
Megaloblastic anaemia is uncommon in well-nourished populations, but it remains a significant problem wherever nutrition is marginal and in specific paediatric risk groups. The single strongest infant risk factor is exclusive breastfeeding by a strict vegan or a subclinically B12-deficient mother, because human milk reflects maternal stores and the rapidly growing infant exhausts a marginal supply within months, as the Italian case of Guez and colleagues showed in a supplemented mother whose infant nonetheless became profoundly deficient. Goat milk feeding is the classic cause of folate deficiency, because goat milk is folate-poor, and a boiled-milk or restricted diet does the same in the older infant. [8][4]
The other risk factors gather around malabsorption, increased demand, and drugs. Malabsorption from coeliac disease or inflammatory bowel disease, and the rare autoimmune pernicious anaemia that is seen in children with other autoimmune conditions or after gastric surgery, impair B12 and folate uptake. Increased demand from chronic haemolysis such as sickle cell disease, from prematurity with its low stores and high turnover, and from exfoliative skin disease consumes folate faster than the diet supplies it. Drug exposure to the folate antagonists, methotrexate, trimethoprim, and phenytoin, and the antiretroviral and chemotherapeutic agents, produces a secondary megaloblastosis that the clinician recognises rather than chasing a new deficiency. [4]
Pathophysiology
The mechanism of megaloblastic anaemia is the failure of DNA synthesis, and the two vitamins sit at adjacent steps of the same folate cycle. Folate enters the cycle as 5-methyltetrahydrofolate, and it donates its methyl group to homocysteine in a reaction catalysed by methionine synthase, which uses vitamin B12 as its cofactor. The methyl transfer regenerates tetrahydrofolate and produces methionine, and the tetrahydrofolate then feeds the thymidylate synthase reaction that makes thymidine, the DNA base that the dividing cell cannot do without. [5]
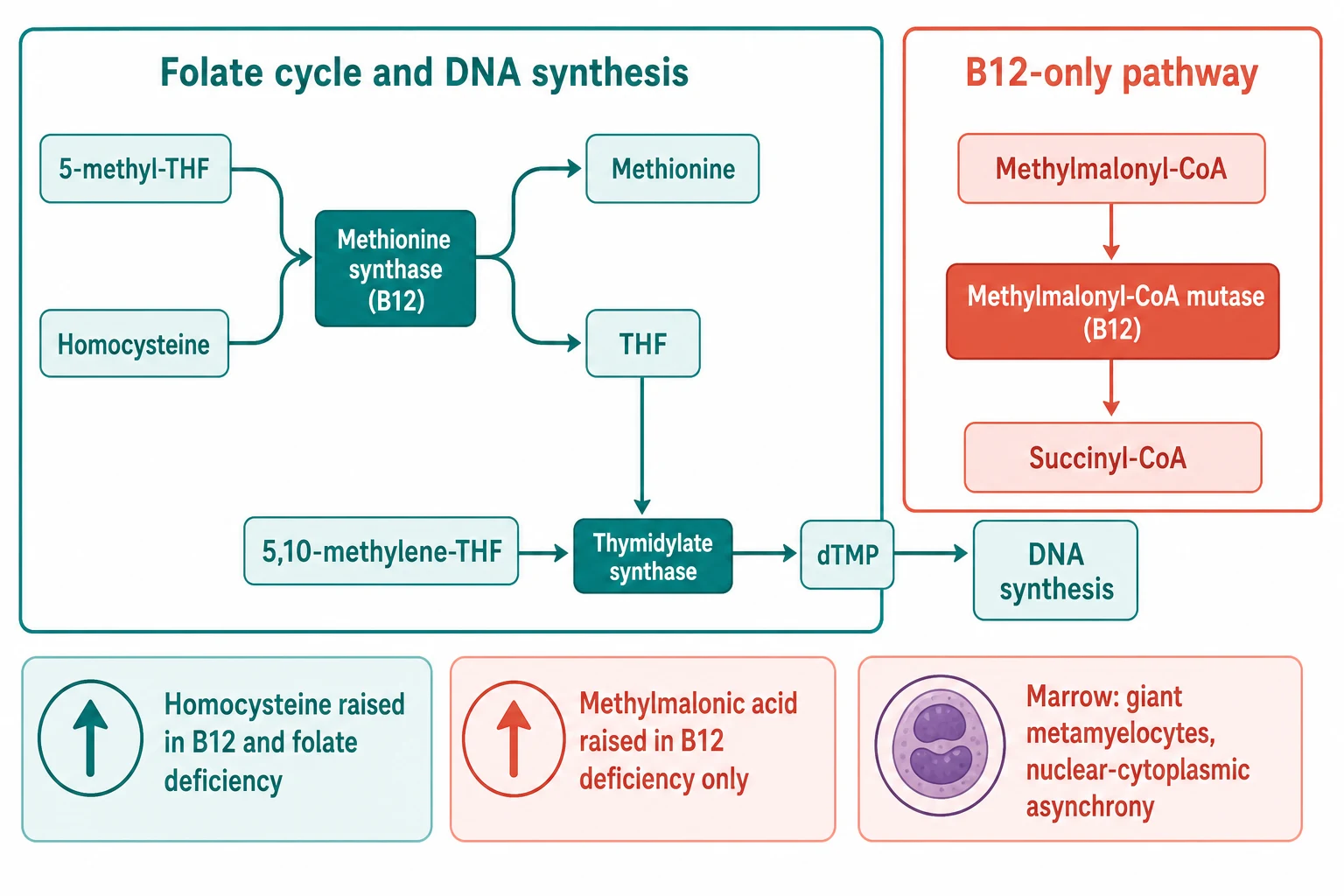
When either vitamin is lacking, thymidine synthesis falters, DNA replication slows, and the nucleus matures more slowly than the cytoplasm. The cell keeps growing but it cannot divide, so the red cell becomes a large oval macrocyte and the neutrophil acquires extra lobes, while the marrow fills with the giant metamyelocyte and the megaloblastic erythroblast whose nucleus lags behind its cytoplasm. This nuclear-cytoplasmic asynchrony is the histological face of impaired DNA synthesis, and it explains why a single missing vitamin enlarges every fast-growing cell line and can present as a pancytopenia. [1]
The methylmalonic acid and homocysteine logic follows directly from the shared and the separate steps. Vitamin B12 is also the cofactor for methylmalonyl-CoA mutase, the enzyme that converts methylmalonyl-CoA to succinyl-CoA, so a lack of B12 raises methylmalonic acid while a lack of folate does not. Homocysteine, by contrast, is the substrate of the shared methionine synthase step, so it rises in both deficiencies. This is why the metabolite pair separates the two deficiencies when the serum vitamin levels are borderline, a problem the clinician meets often because the serum B12 assay is confounded by pregnancy and liver disease. [6][5]
Clinical Presentation
The infant with B12 deficiency rarely presents with anaemia that anyone has measured first. The parents bring a baby between four and twelve months who has gone pale, who has become irritable or apathetic, who feeds poorly and has stopped gaining weight, and who has lost skills he once had, the smile, the reach, the roll, the babble. The developmental regression is the sign that points away from a simple nutritional anaemia and toward the nervous system, and it is often joined by a tremor or a choreiform movement disorder, by hypotonia, and sometimes by seizures. This is the presentation that Jain and Chalouhi described, and it is the one that rewards the clinician who measures a B12 before it becomes permanent. [9][10]
The temporal course of infantile vitamin B12 deficiency
The older child more often presents with the anaemia itself, with fatigue, pallor, and the mild scleral icterus of ineffective erythropoiesis, in which the marrow makes red cells that die before they reach the blood and release a little bilirubin on the way. When the deficiency has gone on long enough, the nervous system declares itself with the signs of subacute combined degeneration of the cord, loss of vibration and joint position sense from the posterior columns, weakness and extensor plantar responses from the corticospinal tracts, and ataxia from the spinocerebellar pathways, often with a peripheral neuropathy. The folate-deficient child carries the same haematological picture, but the nervous system is spared, and that bedside distinction is the one the examiner rewards. [1][2]
Differential Diagnosis
The child with a raised mean corpuscular volume has macrocytosis, and the blood film is the first fork. The film that shows oval macrocytes and a hypersegmented neutrophil points to the megaloblastic causes, B12 deficiency, folate deficiency, and the drug-induced and inherited forms. The film that shows round macrocytes and a normal neutrophil points to the non-megaloblastic causes, and the clinician then asks whether the marrow is turning over too fast or too slowly. A high reticulocyte count from haemolysis or recent bleeding, liver disease with its altered lipid membrane, hypothyroidism, and the bone marrow failure of aplastic anaemia and Diamond-Blackfan anaemia and the myelodysplastic syndromes, all enlarge the red cell without impairing DNA synthesis. [7]
Vitamin B12 deficiency
neurological signs
- Breastfed infant of vegan or deficient mother, pernicious anaemia, ileal disease
- Macro-ovalocytes, hypersegmented neutrophils, pancytopenia
- Methylmalonic acid raised, homocysteine raised
- Neurological regression, subacute combined degeneration, treat with parenteral hydroxocobalamin
Folate deficiency
no neurological signs
- Goat milk diet, malabsorption, increased demand, drugs such as methotrexate
- Same megaloblastic blood film as B12 deficiency
- Methylmalonic acid normal, homocysteine raised
- No neurological signs, treat with oral folic acid 5 mg once daily
Non-megaloblastic macrocytosis
round macrocytes
- Reticulocytosis from haemolysis or bleeding, liver disease, hypothyroidism
- Round macrocytes, normal neutrophil lobe count
- Normal metabolites and normal vitamin levels
- Treat the underlying cause, not the vitamin
The can't-miss mimic is the haemolytic anaemia in crisis, in which the flood of young reticulocytes, which are larger than mature red cells, raises the mean corpuscular volume and can fool the clinician who does not look at the film or the reticulocyte count. The cold agglutinin and the hyperglycaemic sample cause a spurious macrocytosis that vanishes on the repeat, and the myelodysplastic syndrome in the older child carries a dysplastic film rather than the clean hypersegmentation of the megaloblast. Among the megaloblastic causes themselves, B12 and folate deficiency are separated by the methylmalonic acid and homocysteine pair and by the neurological examination, which favours B12, and the inherited transport defects are considered when the deficiency is severe, early, and unexplained by diet or malabsorption. [1][11]
Clinical & Bedside Assessment
The assessment opens with the diet, because the cause is most often in it. The examiner asks what the child eats and, for the breastfed infant, what the mother eats, whether the family is vegan, whether the infant was given goat milk or a boiled-milk formula, and whether the pregnancy was supplemented. The history then gathers the malabsorption clues, the chronic diarrhoea or poor weight gain of coeliac disease, the autoimmune conditions in the family, and any gastric or ileal surgery, and the drug list for the folate antagonists. The developmental history documents the regression, skill by skill and month by month, because the loss of acquired milestones is the sign that lifts the infant out of the ordinary anaemia. [9]
The examination looks for the pallor and the mild scleral icterus of ineffective erythropoiesis, the growth and the weight, and then the nervous system. The tone, the power, the deep tendon reflexes, and the plantar responses are tested, and the posterior columns are examined with a tuning fork for vibration and with joint position sense at the toe, seeking the subacute combined degeneration that is the danger of B12 deficiency. The developmental screen records the milestones the infant has lost, and the abdomen is examined for the splenomegaly that sometimes accompanies severe megaloblastic haemopoiesis. The heart is examined for a flow murmur or the gallop of a decompensated severe anaemia. [10]
The bedside assessment of the macrocytic child
Take the diet and the maternal diet, asking about veganism, goat milk, supplementation, and the pregnancy
Seek the malabsorption, autoimmune, surgical, and drug clues, and map the developmental regression skill by skill
Examine for pallor, scleral icterus, growth, and the flow murmur or gallop of severe anaemia
Test tone, power, reflexes, and plantar responses, then vibration and joint position sense for the posterior columns
Run the developmental screen, plot the growth, and examine the abdomen for splenomegaly
Order the full blood count, the blood film, and the B12, folate, methylmalonic acid, and homocysteine in the same venepuncture
Investigations
The full blood count shows a macrocytic anaemia with a mean corpuscular volume above the age-specific reference range, and in the more severe case a pancytopenia with anaemia, thrombocytopenia, and neutropenia, because the impaired DNA synthesis stalls every fast-growing cell line. The lactate dehydrogenase is raised and the indirect bilirubin is mildly raised from ineffective erythropoiesis, while the haptoglobin is normal, which excludes haemolysis and quietly settles the most important mimic. The blood film is the single most informative first test, and it shows the oval macrocytes, the anisocytosis and poikilocytosis, and the hypersegmented neutrophil with five or more lobes that is the morphological hallmark of megaloblastic haemopoiesis. [1]
Hydroxocobalamin for vitamin B12 deficiency (British Society for Haematology)
Dose
1000 micrograms intramuscularly on alternate days for up to three weeks, or until no further improvement, then 1000 micrograms every two to three months for maintenance; lifelong for permanent causes
Folic acid for folate deficiency
Dose
5 mg once daily by mouth for four months, or lifelong if the cause persists
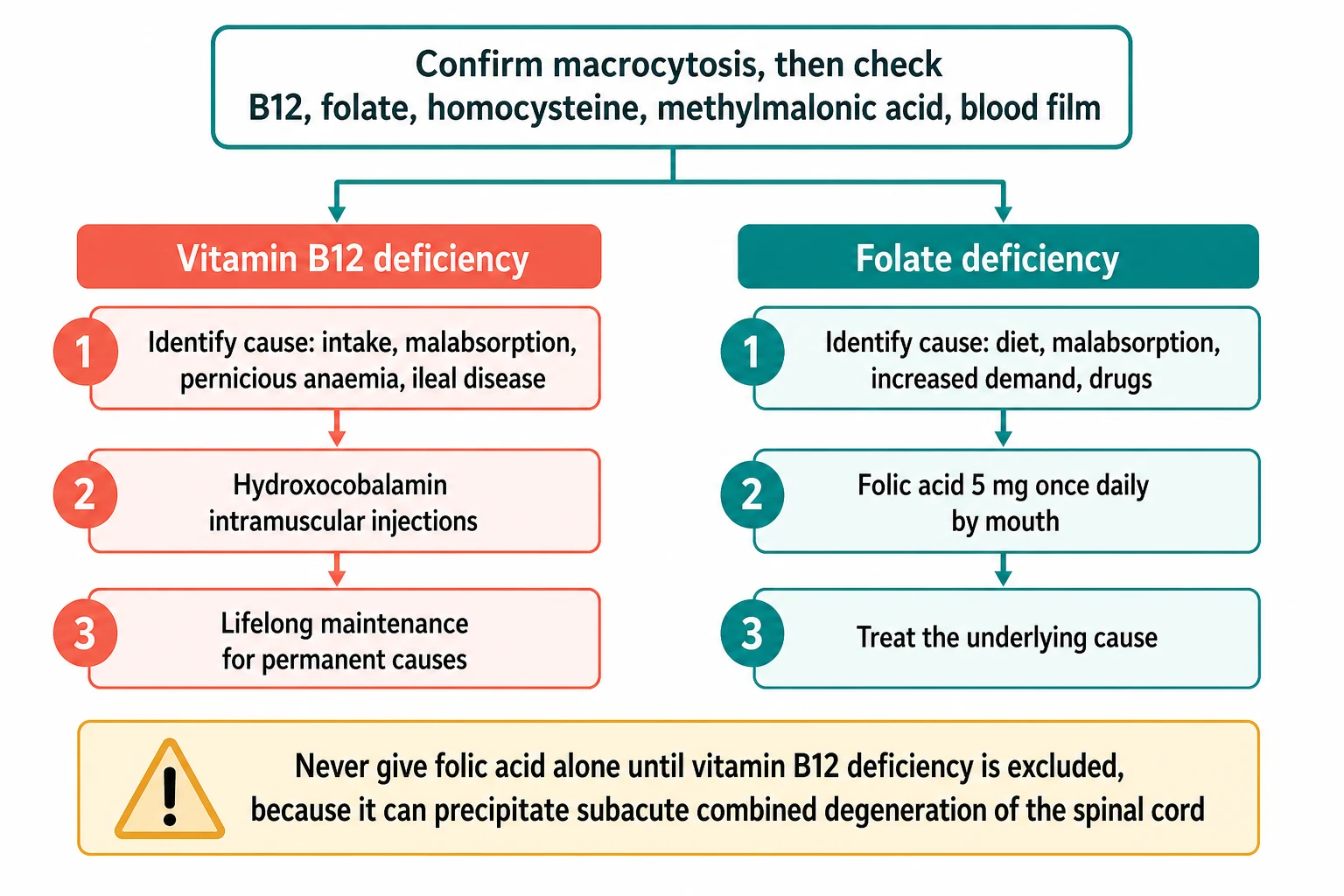
The serum B12 and the serum and red cell folate are measured together, with the red cell folate reflecting the chronic folate status better than the serum, which fluctuates with recent intake. The metabolites refine the diagnosis when the vitamin levels are borderline or the assay is confounded, with methylmalonic acid raised only in B12 deficiency and homocysteine raised in both deficiencies. A bone marrow aspirate, showing the giant metamyelocytes and the megaloblastic erythroblasts with their nuclear-cytoplasmic asynchrony, is reserved for the atypical or pancytopenic case in which the peripheral picture is not diagnostic. The cause is then sought with the anti-intrinsic factor and anti-parietal cell antibodies for pernicious anaemia and the anti-tissue transglutaminase immunoglobulin A for coeliac disease, and the inherited causes are considered when the deficiency is early, severe, and unexplained. [3][5]
Management — Resuscitation
Megaloblastic anaemia is rarely an immediate resuscitation, but the severely anaemic child can present with high-output cardiac failure, and the transfusion of packed red cells is then given cautiously and slowly, or as a partial exchange in the smallest infant. The hypercellular but ineffective marrow can respond to replacement with a dangerous shift in potassium and fluid, so the rate is measured. The transfusion threshold is restrictive and the rate is measured, and the aim is to lift the haemoglobin only enough to relieve the strain on the heart while the vitamin replacement does the definitive work. [2]
Two safety rules govern every step of the treatment, and the examiner tests both. The first is that folic acid must never be given alone until B12 deficiency is excluded, because folate can drive the B12-dependent neurological injury and precipitate or worsen the subacute combined degeneration of the cord. The second is that severe deficiency carries a risk of hypokalaemia in the first days of replacement, as the marrow resumes effective haemopoiesis and the new cells take up potassium, so the serum potassium is monitored and supplemented. Any combined iron deficiency is treated with elemental iron at 3 to 6 mg per kg per day once the vitamin replacement is under way, because the two deficiencies often coexist and the iron demand rises as the marrow recovers. [1]
[3]Management — Definitive & Stepwise
The definitive treatment is the replacement of the deficient vitamin and the correction of its cause, and the agent, the route, and the schedule matter. For vitamin B12 deficiency the agent of choice is hydroxocobalamin by intramuscular injection, which is retained longer than cyanocobalamin and is preferred by the British Society for Haematology guideline. The schedule for deficiency with neurological involvement is hydroxocobalamin 1000 micrograms intramuscularly on alternate days for up to three weeks, or until no further improvement is seen, followed by maintenance of 1000 micrograms every two to three months. Permanent causes such as pernicious anaemia, ileal disease, and the inherited malabsorption syndromes require lifelong maintenance, while a purely dietary deficiency in an older child may be managed with a shorter induction and oral replacement once the stores are repleted. [3]
[3]For folate deficiency the treatment is folic acid 5 mg once daily by mouth for four months, or lifelong if the cause persists, and the underlying malabsorption or increased demand is addressed at the same time. Prophylactic folic acid is given in pregnancy at 400 micrograms daily for the general population and at 5 mg daily for the high-risk pregnancy, and as a low daily dose in chronic haemolysis such as sickle cell disease to keep pace with the turnover. The population-level intervention is the mandatory fortification of flour with folic acid, adopted in Australia, the United States, and Canada, which has reduced the neural tube defect rate. The infant of the vegan or deficient mother is treated with parenteral B12, the mother is treated and advised to supplement, and the breastfeeding is supported with the replacement rather than curtailed. [3][4]
British Society for Haematology guideline, Devalia et al, Br J Haematol 2014
Key finding
The guideline recommends the measurement of methylmalonic acid and homocysteine when the vitamin levels are borderline, the use of hydroxocobalamin over cyanocobalamin for replacement, and the longer induction of 1000 micrograms on alternate days for up to three weeks for deficiency with neurological involvement, followed by maintenance every two to three months, with lifelong treatment for permanent causes and oral replacement reserved for selected maintenance settings.
Specific Subtypes & Scenarios
The breastfed infant of a vegan or subclinically deficient mother is the scenario at the heart of the paediatric topic, and it is the one the examiner returns to. The infant is wholly dependent on maternal stores, and a marginal supply is exhausted within months, so the presentation is a pale, irritable, regressing baby between four and twelve months. The management pairs the infant replacement with maternal treatment and dietary supplementation, and the breastfeeding is continued with the replacement rather than stopped, because the human milk remains the best feed once the B12 is restored. [8][4]
Imerslund-Graesbeck syndrome is the rare autosomal recessive cause of selective vitamin B(12) malabsorption with proteinuria, born of mutations in cubilin or amnionless, the proteins that handle the intrinsic factor and B12 complex in the ileum. It presents in early childhood with megaloblastic anaemia and a persistent low-grade proteinuria that is the diagnostic clue, and it is treated with lifelong parenteral B12, which corrects the anaemia though the proteinuria persists. Transcobalamin II deficiency is the autosomal recessive transport defect in which the serum B12 is normal, because it is carried on transcobalamin I, but the cellular delivery fails, producing failure to thrive, pancytopenia, and neurological signs. These demand high-dose parenteral B12 to saturate the missing carrier, as the Turkish series of Ünal and colleagues described. [12][11]
The drug-induced megaloblastosis of hydroxycarbamide in sickle cell disease is the commonest iatrogenic form in paediatric haematology, and it is recognised from the drug history rather than chased as a new deficiency, because the macrocytosis is the expected effect of the ribonucleotide reductase inhibition and it requires no vitamin replacement. Congenital folate malabsorption and hereditary orotic aciduria are rarer still, and the adolescent with an eating disorder or a strict vegan diet is the older-child scenario in which the deficiency is nutritional and reversible with replacement and dietary counselling. Autoimmune pernicious anaemia is uncommon in children but occurs with other autoimmune disease and after gastric surgery, and it demands lifelong parenteral B12. [1][4]
Complications & Pitfalls
The gravest complication is the neurological injury of untreated B12 deficiency, which is reversible only if it is caught early and which progresses to permanent cognitive and motor impairment and subacute combined degeneration if it is missed. The paediatric series make this plain, that the more severe and the more prolonged the neurological deficit at presentation, the less complete the recovery, so the developmental regression of the infant is an emergency for the vitamin level and the replacement. The iatrogenic counterpart is the precipitation or the acceleration of the cord injury when folic acid is given alone, which remains the single most testable pitfall of the topic. [9][10]
The early treatment period carries the risk of hypokalaemia as the marrow resumes effective haemopoiesis and the new cells take up potassium, and the severely anaemic child given a rapid transfusion may suffer circulatory overload. The diagnostic pitfall is the borderline serum B12, which can mislead when the assay is confounded by pregnancy or liver disease, and the metabolite pair resolves it. Combined iron deficiency may unmask or persist after the vitamin replacement, because the iron demand rises as the marrow recovers, and the reticulocytosis that follows correct treatment is the expected evidence of response rather than a sign of haemolysis. The cognitive pitfall is to mistake the round macrocyte and the normal neutrophil of a non-megaloblastic cause for the megaloblastic picture, which the blood film settles. [1][6]
Prognosis & Disposition
The prognosis of megaloblastic anaemia from nutritional deficiency is excellent when the deficiency is recognised and replaced before the permanent neurological injury, with the haematological picture correcting within weeks and the neurological signs improving over months. The proviso is the one the examiner wants, that the more severe and the more prolonged the neurological deficit at presentation, the less complete the recovery, so an infant who presents with a dense developmental regression and a movement disorder may recover the blood count fully and the development only partially. The inherited and the autoimmune causes demand lifelong replacement, and their prognosis is the prognosis of the disease once the vitamin is kept replete. [9][2]
The disposition is to a paediatrician with an interest in haematology for the diagnostic workup and the replacement course, to dietetics for the nutritional rehabilitation of the vegan family or the restricted diet, and to a neurodevelopmental service for the follow-up of the infant with regression. The milestones must be re-taught as the nervous system recovers. The family receives genetic counselling where the cause is inherited, and the child with an underlying disease such as coeliac disease is followed for the management of that disease. The safety net is the serum potassium and the developmental review in the early weeks, and the population at large is protected by the mandatory folate fortification and the periconceptional supplementation. [3][4]
Special Populations
The infant of a vegan or subclinically B12-deficient mother is the population at the heart of the topic, because the breastfeeding infant is wholly dependent on maternal stores. The maternal B12 status is therefore part of antenatal and breastfeeding care, and the vegan mother is advised to supplement with a B12 preparation throughout the pregnancy and the lactation, because the marginal supply is the supply the infant inherits. The pregnant adolescent and woman receive prophylactic folic acid at 400 micrograms daily, or at 5 mg daily for those at high risk of a neural tube defect, because the neural tube closes in the first weeks before many pregnancies are recognised. [4][8]
The child with chronic haemolysis such as sickle cell disease or thalassaemia receives a low prophylactic daily dose of folic acid to keep pace with the increased turnover, because the folate demand outruns the ordinary diet. The Aboriginal and Torres Strait Islander child and the child from a remote or disadvantaged setting may meet the nutritional deficiency later and with less access to the diagnostic tests. The retrieval, the telehealth link to the paediatric centre, and the culturally safe dietary and family counselling are part of the care, and the nutritional rehabilitation is delivered with respect for the family's circumstances. The migrant and refugee family may carry a dietary pattern or an undiagnosed malabsorption that brings the deficiency to the clinic, and the workup is the same. [1]
Evidence, Guidelines & Regional Differences
The evidence base is anchored by the British Society for Haematology guideline of Devalia and colleagues from 2014, which sets the diagnostic and treatment standard for the cobalamin and folate disorders. The guideline recommends the methylmalonic acid and homocysteine testing for the borderline case, the hydroxocobalamin over the cyanocobalamin for the replacement, the longer induction of 1000 micrograms on alternate days for up to three weeks for the deficiency with neurological involvement, and the lifelong maintenance for the permanent causes. The authoritative reviews of Green and of Stabler set the pathophysiology and the clinical spectrum, and the paediatric series of Jain, Chalouhi, and Guez define the infantile and the childhood neurological presentation and its response to the treatment. [3][1][2]
The controversy turns on two questions. The first is the relative role of the oral and the parenteral B12, which the guideline reserves for the selected maintenance setting, because the oral absorption of a large dose is variable and the intramuscular route is reliable. The second is the population strategy of the mandatory folate fortification, which is adopted in Australia, the United States, and Canada and debated in the United Kingdom and elsewhere. It has reduced the neural tube defect rate at the cost of a possible drift in the folate status of the un-supplemented elderly that is less relevant to paediatrics. The inherited causes are rare enough that the evidence is the case series, and the management is the lifelong replacement that the guidelines extrapolate from the nutritional disease. [3][4]
Exam Pearls
Macrocytosis is a mean corpuscular volume above the age-specific reference range, and megaloblastic anaemia is the subset with the impaired DNA synthesis, the oval macrocyte, and the hypersegmented neutrophil. Methylmalonic acid rises only in B12 deficiency and homocysteine rises in both, and the neurological signs point to B12. The cardinal rule is that folic acid is never given alone until B12 is excluded, because it can precipitate the subacute combined degeneration of the cord. The high-yield stems are the breastfed infant of the vegan mother, the goat milk for folate, and the hydroxycarbamide for the iatrogenic form. [7][1]
[3] [2]The dose of hydroxocobalamin and the schedule are the numbers the examiner wants, 1000 micrograms intramuscularly on alternate days for the induction and every two to three months for the maintenance, with the lifelong treatment for the permanent causes. The folic acid dose is 5 mg once daily by mouth for four months, and the prophylactic pregnancy dose is 400 micrograms daily, or 5 mg daily for the high-risk pregnancy. The two inherited causes to name are the Imerslund-Graesbeck syndrome with its proteinuria and the transcobalamin II deficiency with its normal serum B12, and the two trials to name are the guideline of Devalia and the authoritative review of Green. [3][12]
References
- [1]Green R, Allen LH, Bjørke-Monsen AL, Brito A Vitamin B(12) deficiency. Nat Rev Dis Primers, 2017.PMID 28660890
- [2]Stabler SP Clinical practice. Vitamin B12 deficiency. N Engl J Med, 2013.PMID 23301732
- [3]Devalia V, Hamilton MS, Molloy AM Guidelines for the diagnosis and treatment of cobalamin and folate disorders. Br J Haematol, 2014.PMID 24942828
- [4]Allen LH Causes of vitamin B12 and folate deficiency. Food Nutr Bull, 2008.PMID 18709879
- [5]Froese DS, Fowler B, Baumgartner MR Vitamin B12, folate, and the methionine remethylation cycle-biochemistry, pathways, and regulation. J Inherit Metab Dis, 2019.PMID 30693532
- [6]Ueland PM, Monsen AL Hyperhomocysteinemia and B-vitamin deficiencies in infants and children. Clin Chem Lab Med, 2003.PMID 14656020
- [7]Kaferle J, Strzoda CE Evaluation of macrocytosis. Am Fam Physician, 2009.PMID 19202968
- [8]Guez S, Chiarelli G, Menni F, Salera S Severe vitamin B12 deficiency in an exclusively breastfed 5-month-old Italian infant born to a mother receiving multivitamin supplementation during pregnancy. BMC Pediatr, 2012.PMID 22726312
- [9]Jain R, Singh A, Mittal M, Talukdar B Vitamin B12 deficiency in children: a treatable cause of neurodevelopmental delay. J Child Neurol, 2015.PMID 24453156
- [10]Chalouhi C, Faesch S, Anthoine-Milhomme MC, Fulla Y Neurological consequences of vitamin B12 deficiency and its treatment. Pediatr Emerg Care, 2008.PMID 18708898
- [11]Ünal S, Karahan F, Arıkoğlu T, Akar A Different Presentations of Patients with Transcobalamin II Deficiency: A Single-Center Experience from Turkey. Turk J Haematol, 2019.PMID 30185401
- [12]Gräsbeck R Imerslund-Gräsbeck syndrome (selective vitamin B(12) malabsorption with proteinuria). Orphanet J Rare Dis, 2006.PMID 16722557