Paeds · haematology-oncology-and-transfusion
Transfusion reactions and massive transfusion
Also known as Acute transfusion reaction · Transfusion-associated circulatory overload · TACO · Transfusion-related acute lung injury · TRALI · Acute haemolytic transfusion reaction · Massive transfusion protocol
Fellowship guide to transfusion reactions and massive transfusion in children. Covers the recognition and stepwise management of the acute transfusion reactions a paediatric trainee meets on the ward and in the emergency department, from the common febrile and allergic reactions through to the life-threatening acute haemolytic reaction of an ABO mismatch, the circulatory overload of TACO and the non-cardiogenic pulmonary oedema of TRALI. Explains the mechanisms of intravascular complement-mediated haemolysis, donor anti-leucocyte antibody-driven capillary leak and hydrostatic volume overload, the bedside rule of stopping the transfusion at the first sign of a reaction, and the investigation that distinguishes them. Sets out the paediatric massive transfusion protocol with its balanced ratio of red cells, plasma and platelets, the early use of tranexamic acid in trauma, and the citrate, temperature and electrolyte hazards of rapid transfusion. Built on the paediatric epidemiology of Stone, the child-versus-adult meta-analysis of Wang, the haemolytic reaction review of Panch, the Lancet transfusion-reaction series of Delaney, the TACO and TRALI reviews of Semple, Bosboom, Tung and Yu, the paediatric massive-transfusion work of Neff and Evangelista, the SHOT haemovigilance analysis of Bolton-Maggs and the leucoreduction and premedication review of Duran.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A transfusion reaction is any unwanted response that follows the giving of a blood product, and it ranges from a fleeting fever or itch that settles on its own to a catastrophe that kills within the hour. The child who reacts may be a baby in intensive care, an oncology patient on the ward, or a trauma victim bleeding to death in the emergency department, and the trainee who meets the reaction must act fast and act in the right order. The single most important rule, taught and repeated at every level, is to stop the transfusion at the first sign of trouble and keep the intravenous line open, because the first minutes decide whether a mild reaction stays mild. [4][11]
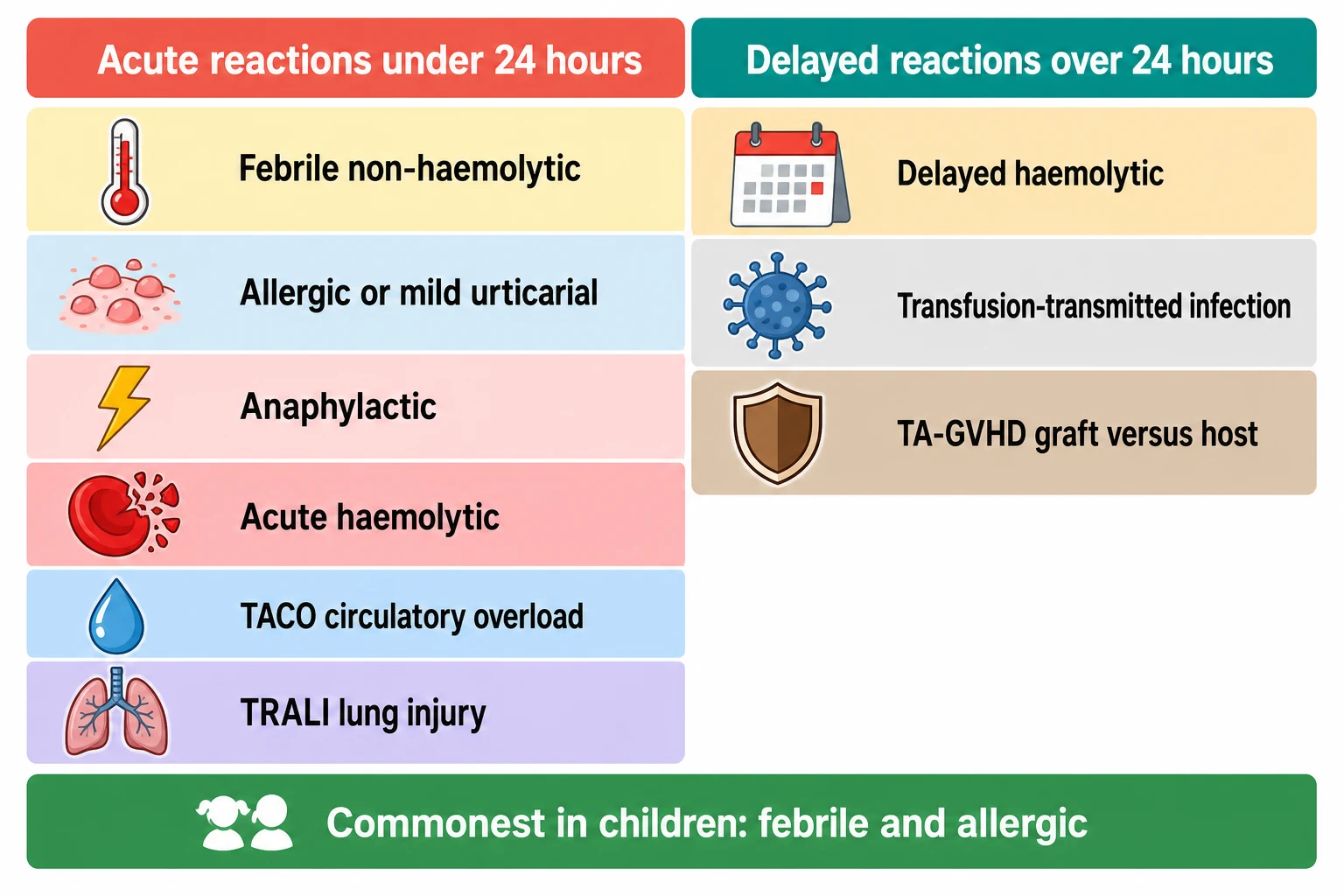
The reactions sort themselves by how soon they appear after the transfusion begins, and the timing is the first clue the trainee uses at the bedside. The acute reactions appear within twenty-four hours, and they are the ones that demand an immediate response, while the delayed reactions appear days to weeks later and are met with investigation rather than resuscitation. Within the acute group, the febrile and the allergic reactions are by far the commonest in children. The severe ones, the acute haemolytic reaction, TACO and TRALI, are the ones that carry the morbidity and the mortality, and the ones the examination tests in depth. [1][2]
Massive transfusion stands beside the reactions as the other half of the topic, and it is the protocol the trainee activates when a child is bleeding faster than the body can replace. The aim is to deliver red cells, plasma and platelets in a balanced ratio that prevents the lethal triad of acidosis, hypothermia and coagulopathy, and to do it fast enough to keep the child alive. The two ideas meet in the child who is being massively transfused, because the rapid delivery of large volumes brings its own hazards of citrate toxicity, hypothermia and electrolyte disturbance, and because a reaction during a massive transfusion is the hardest of all to recognise. [9][10]
Classification
A transfusion reaction is first classified as acute or delayed by whether it appears within or after twenty-four hours of the transfusion, and this single split directs the urgency of the response. The acute reactions demand an immediate bedside decision because they unfold within minutes to hours, while the delayed reactions are investigated after the event. Within the acute group the reactions are further sorted by mechanism, and the mechanisms separate the mild from the severe and point to the treatment. [4]
The acute reactions include the febrile non-haemolytic reaction, the allergic reaction that ranges from mild urticaria to anaphylaxis, the acute haemolytic reaction, the circulatory overload of TACO and the lung injury of TRALI, together with the rare septic reaction from a bacterially contaminated unit. The febrile and allergic reactions are the commonest in children, and they are usually mild, while the haemolytic, the overload and the lung injury are the severe ones that carry the risk to life. The delayed reactions include the delayed haemolytic reaction from an anamnestic antibody response, the transfusion-transmitted infection and the transfusion-associated graft-versus-host disease, each appearing days to weeks after the transfusion. [1][11]
The practical point for the bedside and for the examination is that the common reactions in children are the mild ones, while the severe reactions are the ones that test the trainee. A child who reacts during a transfusion is far more likely to have a fever or a rash than a haemolytic crisis, but the discipline of the response is the same, because the mild reaction cannot be told from the severe one in the first minutes without investigation. The classification therefore serves the rule that every reaction is stopped, assessed and investigated, and only then labelled and managed. [4][11]
Epidemiology & Risk Factors
Transfusion reactions are common in children, and the paediatric epidemiology has been clarified by the 2026 analysis of Stone and colleagues, which showed that the reaction rate in transfused children is higher than in adults, driven largely by the common febrile and allergic reactions. The child-versus-adult meta-analysis of Wang and colleagues confirmed the same pattern, finding that allergic and febrile reactions occur more often in the young, while the rarer and more severe reactions such as TRALI are less frequent but carry a higher mortality. The message for the trainee is that a child who is transfused is more likely than an adult to react, and that the reaction is most often mild. [1][2]
The risk of a reaction rises with the type of product and the underlying condition of the child, and these are the risk factors the trainee weighs before a transfusion begins. Platelets, because they are stored at room temperature and carry plasma, carry a higher rate of febrile and allergic reactions than red cells, and they are the commonest source of bacterial contamination and of TRALI. The child who has been transfused many times, such as the oncology patient or the child with sickle cell disease, builds antibodies against donor leucocytes and red cell antigens, which raises the risk of febrile and haemolytic reactions. The very young, the child with heart or kidney failure, and the child given blood rapidly or in large volume carry the risk of TACO. [1][12]
The preventable root cause of the most dangerous reaction, the acute haemolytic reaction, is the clerical error that gives the wrong unit of blood to the wrong patient, and this is the finding that runs through every haemovigilance report. The Serious Hazards of Transfusion scheme of the United Kingdom, reviewed by Bolton-Maggs on its twentieth anniversary, showed that the largest single category of preventable harm was the error in patient or unit identification, and the same finding holds in every system that reports. The trainee who checks the unit, the wristband and the paperwork at the bedside, and who insists that two people do it, is the trainee who prevents the haemolytic reaction that the clerical error causes. [11][3]
Pathophysiology
Each of the severe acute reactions follows a distinct mechanism, and the mechanisms explain the features and point to the treatment. The acute haemolytic reaction begins with the binding of a preformed antibody to the transfused red cells, almost always an immunoglobulin M antibody against the A or the B antigen in an ABO mismatch. The antibody activates the complement cascade on the surface of the red cell, the cell is destroyed within the blood vessel, and the free haemoglobin and the complement fragments drive the fever, the hypotension, the renal injury and the disseminated intravascular coagulation that define the reaction. [3][4]
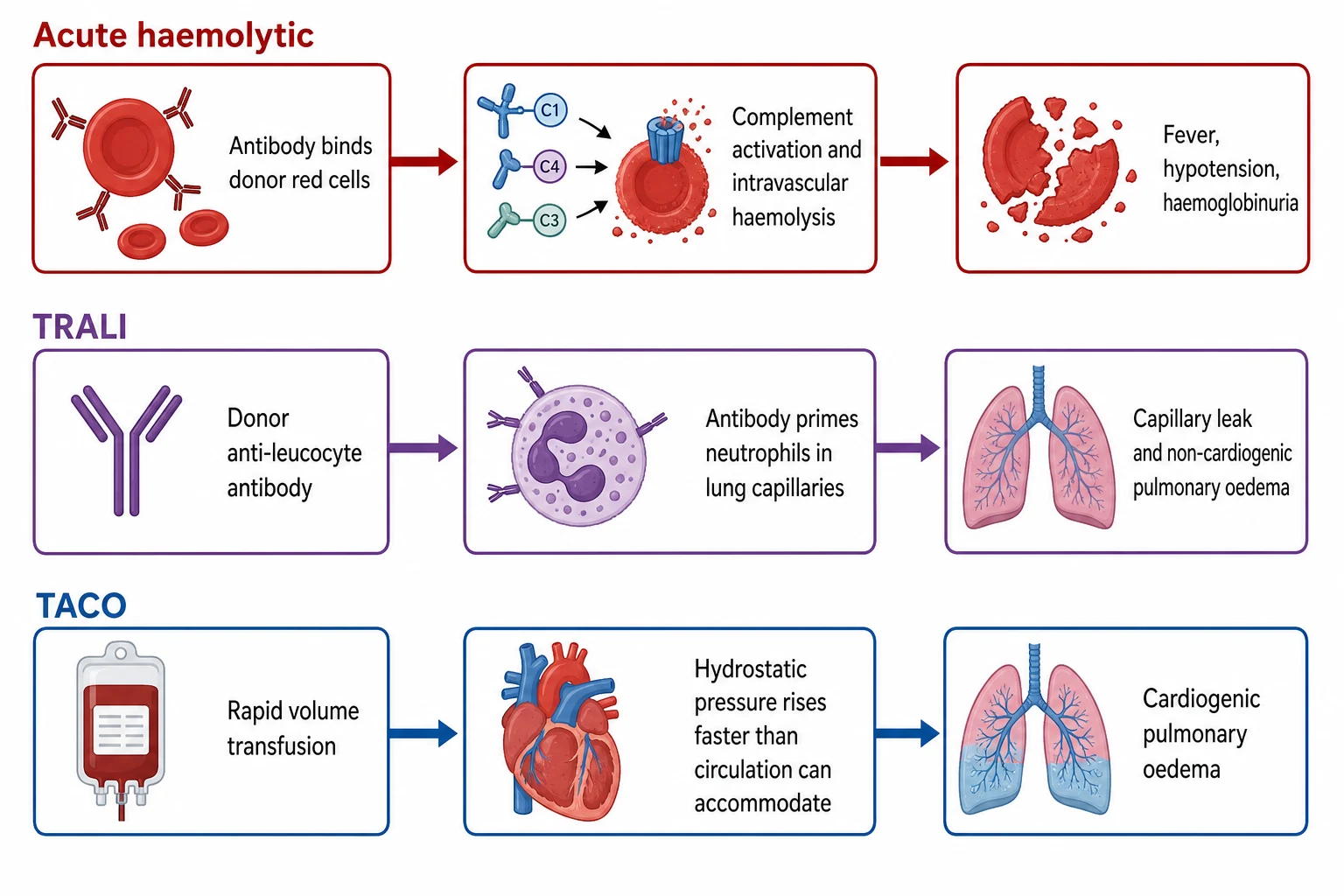
TRALI follows a different path that ends in the lung rather than in the blood vessel, and the donor rather than the recipient is usually the source of the antibody. The donor plasma carries an antibody against the human leucocyte antigen or the human neutrophil antigen of the recipient, and the antibody meets the neutrophils that are normally sequestered in the pulmonary capillaries. The antibody activates the neutrophils, the neutrophils release their enzymes, and the capillary endothelium leaks so that protein-rich fluid floods the alveoli. The result is a non-cardiogenic pulmonary oedema that looks like acute respiratory distress syndrome, and because the left atrial pressure is normal the child is not fluid overloaded. [6][7]
TACO is the simplest of the three in mechanism but no less dangerous, and it is the failure of the circulation to handle the volume rather than an immune event. The transfusion delivers fluid faster than the heart can accommodate, the hydrostatic pressure in the pulmonary capillaries rises, and the fluid is pushed into the alveoli as cardiogenic pulmonary oedema. The child who is small, or who has a heart or a kidney that cannot handle the load, is the child who overloads, and the rapid or the large transfusion is the trigger. The contrast with TRALI is the whole of the diagnosis, because TACO is a volume problem with a raised left atrial pressure and TRALI is a lung problem with a normal one. [5][8]
Clinical Presentation
The child who reacts during a transfusion shows the reaction in the first minutes to hours, and the features are the clues the trainee reads at the bedside. The mild reactions declare themselves with a fever, a chill or a rash, and the child is otherwise well, while the severe reactions declare themselves with breathlessness, a fall in blood pressure or dark urine, and the child is unwell. The discipline of transfusing only a child who is being observed, and of checking the temperature, the pulse and the blood pressure at the start and through the transfusion, is the discipline that catches the reaction early. [4][11]
The acute haemolytic reaction appears within minutes of the start of the transfusion, and the features flow from the destruction of the red cells within the blood vessel. The child develops a fever, shaking rigors and a sense of dread, with pain in the flank or the back as the free haemoglobin damages the kidney, a fall in blood pressure as the complement fragments drive vasodilation, and dark urine as the haemoglobin spills into the urine. The bleeding that follows signals the disseminated intravascular coagulation, and the child under anaesthesia may show only unexplained bleeding, a fall in blood pressure and dark urine, which is why the anaesthetised child is watched with particular care. [3]
TACO and TRALI share the presentation of breathlessness during or within six hours of a transfusion, and the trainee must separate them at the bedside because their treatments differ. The child with TACO is breathless with a raised jugular venous pressure, a high blood pressure and crackles, because the circulation is overloaded. The child with TRALI is breathless with bilateral infiltrates but a normal or low blood pressure and no overload, because the lung is injured and the circulation is not. The volume history is the key question, because the child given blood rapidly or in large volume, or the child with a heart or kidney problem, points to TACO, while the child given a plasma-rich product points to TRALI. [5][8]
[5] [7]The allergic reaction ranges from a mild urticarial rash to a full anaphylaxis, and the trainee treats the severity rather than the label. The mild reaction shows an itch and a few wheals, and it settles when the transfusion is slowed and an antihistamine is given. The severe reaction shows bronchospasm, angioedema and a fall in blood pressure, and it demands the transfusion be stopped and intramuscular adrenaline given at once. The child with selective IgA deficiency who has formed anti-IgA antibodies is the classic cause of anaphylaxis to blood products, and the reaction is severe and rapid, which is why any child who has had a severe reaction to a plasma-containing product is investigated for IgA deficiency. [4][12]
Differential Diagnosis
The fever that appears during a transfusion has a short list of causes, and the trainee must separate the benign from the dangerous before the child is labelled. The commonest cause is the febrile non-haemolytic reaction, which is a fever with or without rigors from cytokines in the stored product or from antibodies against donor leucocytes, and it is benign once the dangerous causes are excluded. The dangerous causes that the fever alone cannot exclude are the acute haemolytic reaction, the septic reaction from a contaminated unit and the underlying infection that the transfusion has coincided with, and each must be sought before the fever is dismissed as benign. [4][11]
Acute haemolytic
minutes, ABO mismatch
- Clerical error giving wrong unit to wrong patient
- Immunoglobulin M and complement, intravascular haemolysis
- Fever, rigors, flank pain, hypotension, haemoglobinuria
- Stop transfusion, fluids for urine output and renal perfusion
TACO
within 6 hours, volume overload
- Small child or cardiac or renal disease, rapid or large volume
- Hydrostatic pressure and cardiogenic pulmonary oedema
- Breathlessness, raised venous pressure, hypertension, crackles
- Stop or slow transfusion, oxygen, diuretic such as furosemide
TRALI
within 6 hours, donor antibody
- Donor anti-leucocyte antibody, plasma-rich product
- Neutrophil activation in lung capillaries, capillary leak
- Breathlessness, hypoxaemia, bilateral infiltrates, no overload
- Stop transfusion, oxygen, respiratory support, no diuretic
Febrile non-haemolytic
during or shortly after
- Cytokines in stored product or anti-leucocyte antibody
- Fever with or without rigors, child otherwise well
- Exclude haemolytic and septic before labelling benign
- Slow or pause, paracetamol, observe, restart cautiously
The breathless child after a transfusion is the harder distinction, and it turns on the volume state and the blood pressure, as the bedside findings above set out. The septic reaction from a contaminated unit, most often a platelet unit stored at room temperature, presents with a high fever, rigors and a profound fall in blood pressure during the transfusion, and it is managed as septic shock with the transfusion stopped, blood cultures taken and broad-spectrum antibiotics begun. The trainee who holds the possibilities of haemolysis, overload, lung injury and sepsis in mind, and who stops and investigates before labelling, is the trainee who avoids the error of treating a dangerous reaction as a benign one. [4][11]
Clinical & Bedside Assessment
The assessment of a suspected transfusion reaction begins at the bedside with the stop-the-transfusion rule, and the steps that follow are the same for every reaction. The transfusion is stopped at the first sign and the intravenous line is kept open with normal saline, the airway, the breathing and the circulation are checked, and the child is examined for the features that separate the mild from the severe. The unit and the giving set are set aside, the blood bank is called, and the paperwork and the wristband are checked against the unit, because the error that caused the reaction is found here. [4]
The examination looks for the signs of each of the severe reactions, because the treatment follows the sign. The temperature, the pulse and the blood pressure are taken, because the fever with a falling blood pressure points to haemolysis or sepsis. The chest is auscultated for the crackles and the breathlessness of TACO or TRALI, and the neck is looked at for the jugular venous pressure that separates the overloaded child from the one with a lung injury. The urine is checked for the dark colour of haemoglobinuria, and the skin is checked for the urticaria of an allergic reaction or the bleeding of a coagulopathy. [3][8]
The bedside response to a suspected acute transfusion reaction
Stop the transfusion at once and keep the intravenous line open with normal saline
Check the airway, the breathing and the circulation, and give oxygen if the child is breathless or hypoxaemic
Check the identity of the child, the wristband and the unit label against the paperwork at the bedside
Examine for fever, hypotension, breathlessness, crackles, raised venous pressure, rash and dark urine
Take blood for full blood count, group and antibody screen, coagulation, direct antiglobulin test, urea and electrolytes, and send the unit and fresh samples to the blood bank
Classify the reaction and treat it, report it through the haemovigilance system, and plan future transfusions accordingly
The teaching of the nurses and the families is the clinical act that prevents the next reaction, and the trainee builds the culture of safety around the transfusion. The nurses are taught to stay with the child for the first fifteen minutes of every transfusion, because that is when the severe reactions appear, and to take and record the observations at the start and through the transfusion. The family is taught to call for help at the first sign of a fever, a chill, a rash or breathlessness, because the child who is watched is the child who is saved. The reporting of every reaction through the haemovigilance system is the act that turns one child's reaction into the system change that prevents the next. [11][12]
Investigations
The investigation of a transfusion reaction confirms the type and excludes the dangerous mimics, and the samples are taken at the moment the transfusion is stopped. The blood is sent for a full blood count, a group and antibody screen, a coagulation screen, a direct antiglobulin test, and urea and electrolytes, and the urine is dipped for haemoglobin. The unit, the giving set and the fresh blood samples are returned to the blood bank with a report, because the blood bank performs the checks that confirm or exclude the haemolytic reaction. [3][4]
The direct antiglobulin test is the key investigation of the acute haemolytic reaction, and it confirms that antibody or complement has coated the transfused red cells. A positive direct antiglobulin test, together with a fall in haemoglobin, a rise in lactate dehydrogenase, a rise in bilirubin and a fall in haptoglobin, confirms the intravascular haemolysis, and the repeat of the group and antibody screen identifies the antibody and the mismatch. The blood bank repeats the crossmatch on the unit and the samples, and it cultures the unit if a septic reaction is suspected, because the contaminated unit is a source of sepsis that must be identified. [3]
The reporting of a transfusion reaction through the national haemovigilance system is the practice that turns one event into system learning, and the trainee names the local system. The Serious Hazards of Transfusion scheme in the United Kingdom, the National Healthcare Safety Network haemovigilance module in the United States, and the Transfusion Transmitted Injuries Surveillance System in Canada each collect, analyse and feed back the reactions to drive prevention. Australia and Aotearoa New Zealand report through their own blood safety frameworks. The fellow reports every reaction, because the under-reported reaction is the reaction that recurs. [11]
The investigation of TACO and TRALI is largely clinical, because the distinction is made at the bedside from the volume history and the examination, supported by the chest radiograph and the blood gases. The chest radiograph shows bilateral infiltrates in both, but the TACO child has a large heart and fluid in the fissures and the TRALI child has a normal heart size, and the brain natriuretic peptide may help, with a higher value supporting the overload of TACO. The echocardiogram, where available, confirms the impaired or the normal cardiac function, and it settles the distinction in the difficult case. The donor of the implicated unit is tested for anti-leucocyte antibodies if TRALI is confirmed, and the donor is deferred to prevent the next case. [8][7]
Management — Resuscitation
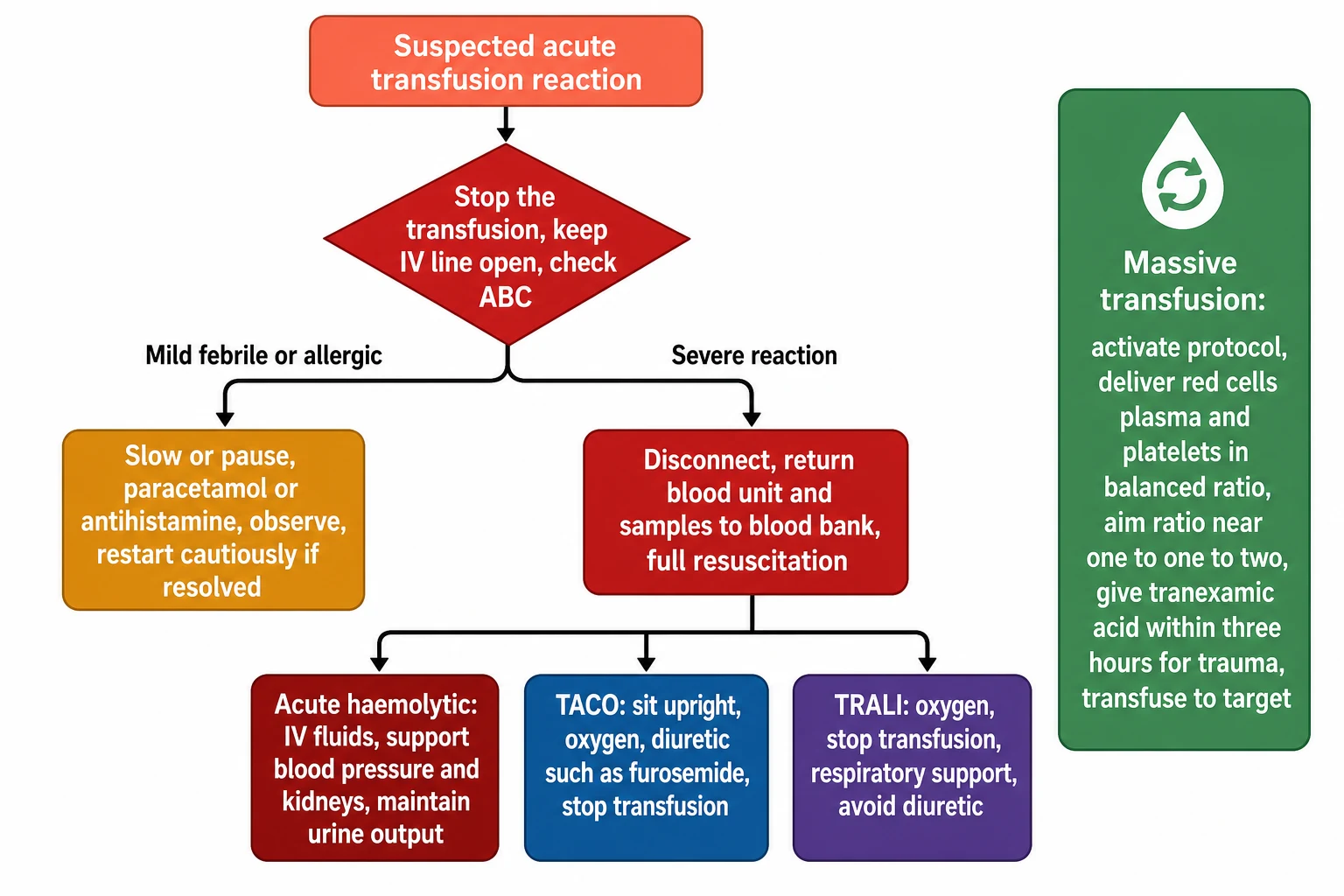
The resuscitation of the acute transfusion reaction follows the stop-the-transfusion rule and then the airway, breathing and circulation, and the trainee runs the steps in the same order for every reaction. The transfusion is stopped and the line is kept open, oxygen is given to the breathless or hypoxaemic child, and the circulation is supported with fluid or inotropes if the blood pressure has fallen. The unit and the fresh samples are sent to the blood bank, and the reaction is reported, while the child is monitored in a setting that matches the severity. [4]
The acute haemolytic reaction is the one that demands the most aggressive resuscitation, because the intravascular haemolysis drives the shock, the renal failure and the disseminated intravascular coagulation. The transfusion is stopped at once, generous intravenous fluids are given to maintain the urine output and the renal perfusion, and the blood pressure is supported with fluids and vasopressors as needed. The coagulopathy is treated with blood components as guided by the coagulation tests, and the child is observed in a high-dependency or intensive care setting, because the renal failure and the bleeding may unfold over the hours that follow. [3][4]
[3] [4]TACO is treated by removing the cause and removing the fluid, and the response is rapid when it is recognised early. The transfusion is slowed or stopped, the child is sat upright and given oxygen, and a loop diuretic such as furosemide is given to remove the excess fluid and lower the hydrostatic pressure. The child who is severely overloaded or who does not respond to the diuretic may need non-invasive ventilation, and the rare child with refractory pulmonary oedema may need continuous positive airway pressure or intubation. The blood pressure and the oxygen are monitored, and the response confirms the diagnosis, because the child with TACO improves with the diuretic while the child with TRALI does not. [8][5]
TRALI is treated by stopping the transfusion and supporting the lung, and the distinction from TACO matters because the diuretic that helps the overloaded child harms the child with the lung injury. The transfusion is stopped, oxygen is given, and the child who remains hypoxaemic is supported with non-invasive or invasive ventilation as the severity demands. A diuretic is avoided, because the TRALI child is not fluid overloaded and the diuretic lowers the preload and the blood pressure in a child who is often already hypotensive. The lung injury is self-limiting in most children who survive the acute episode, and the recovery over days to weeks is the usual course with good supportive care. [7][6]
Management — Definitive & Stepwise
The definitive management of the mild reactions is conservative, and the trainee applies the principles after the dangerous causes are excluded. The febrile non-haemolytic reaction is managed by slowing or pausing the transfusion, giving an antipyretic such as paracetamol, and observing the child, with the transfusion restarted cautiously only if the reaction has fully settled and the dangerous causes are excluded. The mild allergic reaction is managed by slowing the transfusion and giving an antihistamine, with the transfusion restarted cautiously if the urticaria settles. The severe allergic reaction or anaphylaxis is managed by stopping the transfusion and giving intramuscular adrenaline, with fluids, oxygen and the full anaphylaxis pathway as the severity demands. [4][12]
Management of the common acute transfusion reactions
Dose
Febrile non-haemolytic: slow or pause the transfusion, give paracetamol 15 mg per kg orally or rectally, observe and restart cautiously if settled. Mild allergic: slow the transfusion and give an antihistamine. Anaphylaxis: stop the transfusion and give intramuscular adrenaline 10 micrograms per kg, repeated as needed, with the full anaphylaxis pathway. TACO: stop or slow the transfusion, oxygen, and a loop diuretic such as furosemide 1 mg per kg.
The prevention of the reactions is the management that runs ahead of the transfusion, and the trainee builds the measures into every transfusion prescription. Leucodepletion of all cellular components, now universal in most high-income systems, lowers the rate of febrile reactions and the transmission of cytomegalovirus. Premedication with paracetamol and an antihistamine is no longer routine for every transfusion, because the evidence shows it has little effect on the reaction rate, but it is reserved for the child who has reacted before. The slow start to every transfusion, with close observation for the first fifteen minutes, is the measure that catches the severe reaction early, and the correct identification of the child and the unit at the bedside is the measure that prevents the ABO mismatch. [12][11]
[4] [9]The massive transfusion protocol is the definitive management of the shocked bleeding child, and its principles are the balanced delivery of components, the early use of tranexamic acid in trauma and the prevention of the citrate, the temperature and the electrolyte hazards. The protocol is activated the moment a child is recognised to be bleeding faster than the body can replace, defined practically as the replacement of one blood volume in twenty-four hours or the ongoing haemorrhage with shock. Red cells, fresh frozen plasma and platelets are delivered in packs in a balanced ratio that approaches one unit of red cells to one unit of plasma to one pool of platelets, so that the coagulopathy of dilution is prevented as the bleeding is controlled. [9][10]
Specific Subtypes & Scenarios
The child on the oncology ward is the one who meets transfusion reactions most often, because the repeated transfusions of red cells and platelets through the treatment of leukaemia and solid tumours raise the lifetime exposure. The oncology child is the one who develops the febrile reaction from the cytokines in the platelet pool and the antibodies against the donor leucocytes, and the one who may become alloimmunised against the red cell antigens. The trainee who transfuses the oncology child uses leucodepleted components, matches the red cell antigens in the child who has formed antibodies, and watches for the reaction that the repeated exposure makes more likely. [12][2]
The child with sickle cell disease is the other chronic transfusion patient, and the prevention of alloimmunisation is the central concern. The sickle cell child forms antibodies against the donor red cell antigens because the donor pool differs in antigen profile, and the antibodies make future crossmatching hard and cause the delayed haemolytic reaction. The prevention is the extended phenotypic matching of the red cells for the major antigens before the first transfusion, and the minimisation of unnecessary transfusion. The trainee who transfuses the sickle cell child also watches for the hyperhaemolysis, the rare and dangerous syndrome in which the child's own red cells are destroyed alongside the transfused ones. [4]
The course of a severe acute transfusion reaction
The neonate is the child for whom the transfusion hazards are most specific, and the trainee who transfuses the smallest patients follows the neonatal rules. The rapid transfusion of citrated components lowers the ionised calcium as the citrate binds it faster than the immature liver can metabolise it, so the neonate given rapid or large transfusion is monitored for hypocalcaemia and given calcium replacement if it falls. The stored red cell unit, especially if irradiated or old, carries a high potassium load that causes the hyperkalaemia and the arrhythmia in the neonate given a large volume rapidly, so the freshest or the washed unit is chosen for the large transfusion. The slow, the warmed and the aliquoted transfusion is the neonatal standard, and the volume is calculated to the gram. [9][8]
Complications & Pitfalls
The first pitfall is the failure to stop the transfusion at the first sign, and it is the pitfall that turns a treatable reaction into a fatal one. The temptation to slow the transfusion rather than stop it, or to treat the fever and push on, is the error that allows the haemolytic reaction to continue and the renal failure and the shock to deepen. The trainee who builds the stop-the-transfusion rule into the culture, who teaches the nurses to call at the first sign, and who never dismisses a fever during a transfusion as benign until it is investigated, is the trainee who prevents this death. [4][11]
The second pitfall is the confusion of TACO with TRALI, and it is the pitfall that leads to the wrong treatment. The diuretic that removes the fluid of TACO and relieves the overloaded child is the diuretic that lowers the preload and the blood pressure of the TRALI child and worsens the hypotension. The trainee who assesses the volume state, the blood pressure and the jugular venous pressure, and who treats the overload with a diuretic and the lung injury with respiratory support, is the trainee who avoids this error. The chest radiograph and the echocardiogram settle the difficult case, but the bedside assessment is the first and the decisive step. [8][7]
[5] [8]The third pitfall is the failure to prevent the citrate, the temperature and the electrolyte hazards of the massive transfusion, and it is the pitfall that turns a life-saving protocol into a source of new harm. The rapid transfusion of citrated components causes the hypocalcaemia that depresses the myocardium and prolongs the bleeding, the cold blood causes the hypothermia that impairs the coagulation and the platelet function, and the stored unit causes the hyperkalaemia that threatens the arrhythmia. The trainee who warms the blood, who checks the ionised calcium and replaces it, and who monitors the potassium during the massive transfusion, is the trainee who prevents these harms. [9][10]
The fourth pitfall is the failure to report the reaction through the haemovigilance system, and it is the pitfall that lets the preventable reaction recur. The reaction that is not reported is the reaction whose root cause is not found, and the donor whose antibody caused the TRALI is not deferred, and the clerical error whose flaw in the process caused the ABO mismatch is not fixed. The trainee who reports every reaction, who cooperates with the blood bank and the haemovigilance team, and who closes the loop on the root cause, is the trainee who turns one child's reaction into the change that protects the next. [11]
Prognosis & Disposition
The prognosis of a transfusion reaction depends on its type and on the speed of the recognition, and the mild reactions carry an excellent prognosis while the severe ones carry a mortality that the early response can reduce. The febrile and the allergic reactions settle with the conservative measures and leave no harm, while the acute haemolytic reaction carries a mortality that has fallen with the improvements in identification and the early resuscitation, but that remains a cause of death in the systems where the clerical error persists. TRALI carries the highest mortality among the severe acute reactions, but the mitigation strategies of donor deferral and male-donor plasma have lowered its incidence and its toll. [1][6]
The disposition of the child depends on the severity of the reaction, and the trainee matches the setting to the need. The child with a mild reaction that has settled is observed and managed conservatively. The child with an acute haemolytic reaction or a severe TACO or TRALI is managed in a high-dependency or intensive care setting for the monitoring and the support that the shock, the renal failure or the respiratory failure demand. The child who has had a reaction is investigated to define the cause, and the future transfusions are planned around it, with the special components and the matching that prevent the recurrence. [4][8]
The long-term follow-up of the child who has reacted is the plan that prevents the next reaction, and it is built into the transfusion record. The child who has formed an antibody is flagged so that the future transfusions are matched, the child who has had TRALI is not transfused with the implicated donor again, and the child with IgA deficiency is given washed or IgA-deficient components. The trainee who records the reaction, who communicates it to the primary team and the family, and who builds the prevention into every future transfusion, is the trainee who keeps the child safe across the years of transfusion. [11][4]
Special Populations
The child who is transfusion-dependent, such as the oncology patient, the child with sickle cell disease or the child with thalassaemia, is the special population that meets the transfusion reaction most often, and the prevention is built into the transfusion programme. The extended phenotypic matching, the leucodepletion, the slow start and the close observation are the measures that lower the reaction rate in the chronically transfused child, and the flagging of the antibodies and the previous reactions is the measure that prevents the recurrence. The trainee who runs the transfusion programme for the chronic patient builds the safety measures into every unit, and reviews the reactions at the transfusion committee. [12][4]
The neonate and the infant are the special population for whom the transfusion hazards are most specific, and the volume, the rate and the product are calculated to the gram and to the minute. The neonatal transfusion uses small aliquots, the freshest units, the warming and the slow rate to avoid the hyperkalaemia, the hypothermia and the hypocalcaemia that the immature physiology cannot buffer. The child in heart or kidney failure, and the child who is small for age, is the special population at risk of TACO, and the transfusion is given slowly, in the smallest effective volume, with the diuretic and the monitoring that the overload demands. [9][8]
STOPPED
The child in the rural or the remote setting, far from the blood bank and the intensive care, is the special population for whom the transfusion is planned with the greatest caution. The blood is given only when the need is clear, and the first fifteen minutes are watched with the same care. The emergency response and the retrieval are planned before the transfusion begins, because the child who reacts far from the centre needs the retrieval team and the plan that the distance demands. The trainee who works in the remote setting values the local network, the shared protocols and the telehealth link to the transfusion specialist, because the child who is connected to the centre through it is the child who is kept safe. [10]
Evidence, Guidelines & Regional Differences
The evidence base for the transfusion reactions has been transformed by the paediatric epidemiology that the earlier, adult-dominated reports lacked. The 2026 analysis of Stone and colleagues, drawn from a large multicentre paediatric dataset, defined the reaction rates and the types in children and confirmed that the febrile and the allergic reactions dominate the paediatric picture. The meta-analysis of Wang and colleagues placed the child beside the adult and showed that the reaction rate is higher in the young, a finding that underpins the vigilance that the paediatric transfusion demands. [1][2]
The mechanism and the management of the severe reactions are set out in the reviews that the trainee reads for the topic. The New England Journal of Medicine review of Panch and colleagues distilled the haemolytic reaction, and the Lancet series article of Delaney and colleagues set the whole field of transfusion reactions in context. The TACO and the TRALI reviews of Semple, Bosboom, Tung and Yu traced the mechanisms from the donor antibody to the capillary leak and from the volume overload to the pulmonary oedema, and they are the references the trainee cites for the bedside distinction and the management. [3][5]
Epidemiology of pediatric transfusion reactions - Stone 2026
Key finding
In a large multicentre paediatric cohort, transfusion reactions were more frequent in children than in adults, with the febrile and allergic reactions accounting for the majority and the severe reactions remaining rare but consequential.
Transfusion reactions in children and adults - Wang 2022
Key finding
A systematic review and meta-analysis comparing children and adults found a higher rate of allergic and febrile reactions in children, while severe reactions such as TRALI were rarer but carried a higher mortality.
Massive transfusion in pediatric patients - Neff 2021
Key finding
The review set out the principles of the paediatric massive transfusion protocol, with the balanced delivery of red cells, plasma and platelets, the early use of tranexamic acid in trauma and the prevention of the citrate, temperature and electrolyte hazards.
The guidelines that translate the evidence into practice differ by region, and the trainee names the one being followed. The British Society for Haematology and the Association for the Advancement of Blood and Biotherapies set the standards for the transfusion and the reaction management. The Royal Children's Hospital in Melbourne sets the local protocol that the Australian and New Zealand trainee follows, and the Serious Hazards of Transfusion scheme sets the haemovigilance standard that the United Kingdom and its mirror regions apply. The chief controversy is the role of routine premedication before transfusion, where the evidence shows little benefit in the unselected child and the practice is reserved for the child who has reacted before. [11][12]
Exam Pearls
The single most testable fact is the stop-the-transfusion rule, and the trainee who holds it carries the whole of the topic. The first response to any suspected acute transfusion reaction is to stop the transfusion, keep the intravenous line open, check the airway, the breathing and the circulation, verify the identity of the child and the unit, and return the unit and the fresh samples to the blood bank. The discipline is the same for the mild fever and the haemolytic crisis, because the mild reaction cannot be told from the severe one in the first minutes, and the trainee who stops and investigates before labelling is the trainee who passes the examination and keeps the child safe. [4][11]
The second most testable set is the TACO versus TRALI distinction, and it is asked as a pair because the treatments differ. TACO is the circulatory overload of the child given blood rapidly or in large volume, with a raised jugular venous pressure, hypertension and crackles, treated by stopping the transfusion, oxygen and a diuretic. TRALI is the non-cardiogenic pulmonary oedema of the donor antibody, with hypoxaemia, bilateral infiltrates and no overload, treated by stopping the transfusion and respiratory support and no diuretic. The trainee who separates them at the bedside from the volume state and the blood pressure has the heart of the topic. [5][8]
[3] [5]The third high-yield set is the massive transfusion protocol, and it turns on the balanced ratio and the early tranexamic acid. The shocked bleeding child needs the protocol activated with red cells, plasma and platelets in a balanced ratio that approaches one to one to one, so that the dilutional coagulopathy is prevented as the bleeding is controlled. Tranexamic acid is given early in trauma, and the citrate, the temperature and the electrolyte hazards are prevented by warming the blood and checking the ionised calcium. The trainee who holds the rule, the distinction and the protocol carries the management of the topic, and the bedside discipline of the stop-the-transfusion rule holds it together. [9][10]
References
- [1]Stone EF, Chacreton D, Jimenez A, et al Epidemiology of pediatric transfusion reactions JAMA Netw Open, 2026.PMID 42043816
- [2]Wang Y, Sun W, Wang X, et al Comparison of transfusion reactions in children and adults: a systematic review and meta-analysis. Pediatr Blood Cancer, 2022.PMID 35758531
- [3]Panch SR, Montemayor-Garcia C, Klein HG Hemolytic transfusion reactions. N Engl J Med, 2019.PMID 31291517
- [4]Delaney M, Wendel S, Bercovitz RS, et al Transfusion reactions: prevention, diagnosis, and treatment. Lancet, 2016.PMID 27083327
- [5]Semple JW, Rebetz J, Kapur R Transfusion-associated circulatory overload and transfusion-related acute lung injury. Blood, 2019.PMID 30808638
- [6]Tung JP, Chiaretti S, Dean MM, et al Transfusion-related acute lung injury (TRALI): potential pathways of development, strategies for prevention and treatment, and future research directions. Blood Rev, 2022.PMID 35065815
- [7]Yu Y, Lian Z Update on transfusion-related acute lung injury: an overview of its pathogenesis and management. Front Immunol, 2023.PMID 37251400
- [8]Bosboom JJ, Klanderman RB, Migdady Y, et al Transfusion-associated circulatory overload: a clinical perspective. Transfus Med Rev, 2019.PMID 30853167
- [9]Neff LP, Beckwith MA, Russell RT, et al Massive transfusion in pediatric patients. Clin Lab Med, 2021.PMID 33494884
- [10]Evangelista ME, Gaffley M, Neff LP Massive transfusion protocols for pediatric patients: current perspectives. J Blood Med, 2020.PMID 32547282
- [11]Bolton-Maggs PHB Serious hazards of transfusion - conference report: celebration of 20 years of UK haemovigilance. Transfus Med, 2017.PMID 29282809
- [12]Duran J, Siddique S, Cleary M Effects of leukoreduction and premedication with acetaminophen and diphenhydramine in minimizing febrile nonhemolytic transfusion reactions and allergic transfusion reactions during and after blood product administration: a literature review with recommendations for practice. J Pediatr Oncol Nurs, 2014.PMID 24794886