Paeds · haematology-oncology-and-transfusion
Tumour lysis syndrome and oncologic emergencies
Also known as Tumour lysis syndrome · Oncologic emergencies · Cairo-Bishop syndrome · Superior vena cava syndrome · Spinal cord compression · Hyperleukocytosis · Febrile neutropenia
Fellowship guide to tumour lysis syndrome and the paediatric oncologic emergencies. Covers the Cairo-Bishop classification of laboratory and clinical tumour lysis syndrome with its thresholds for urate, potassium, phosphate and calcium, the pathophysiology of the metabolic cascade from tumour breakdown to acute kidney injury and arrhythmia, the prevention with hyperhydration and rasburicase with the glucose-six-phosphate-dehydrogenase contraindication, the management of the hyperkalaemia and the acute kidney injury, and the structural and haematological emergencies of febrile neutropenia, hyperleukocytosis and leukostasis, superior vena cava obstruction from an anterior mediastinal mass, and malignant spinal cord compression.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child with a large, fast-growing tumour sits on the edge of a metabolic cliff. The moment chemotherapy or steroids begin to kill the tumour cells, those cells spill their contents into the blood faster than the kidneys can clear them, and within hours the potassium can stop the heart and the phosphate and urate can shut the kidneys down. This is tumour lysis syndrome, and it is one of the few complications of cancer treatment that can kill a child in the first day of therapy. The whole point of recognising it is to stand on the cliff edge first: to anticipate it before the first dose of chemotherapy, to flush the kidneys hard, and to dissolve the urate with rasburicase, so that the child never falls over. [1]
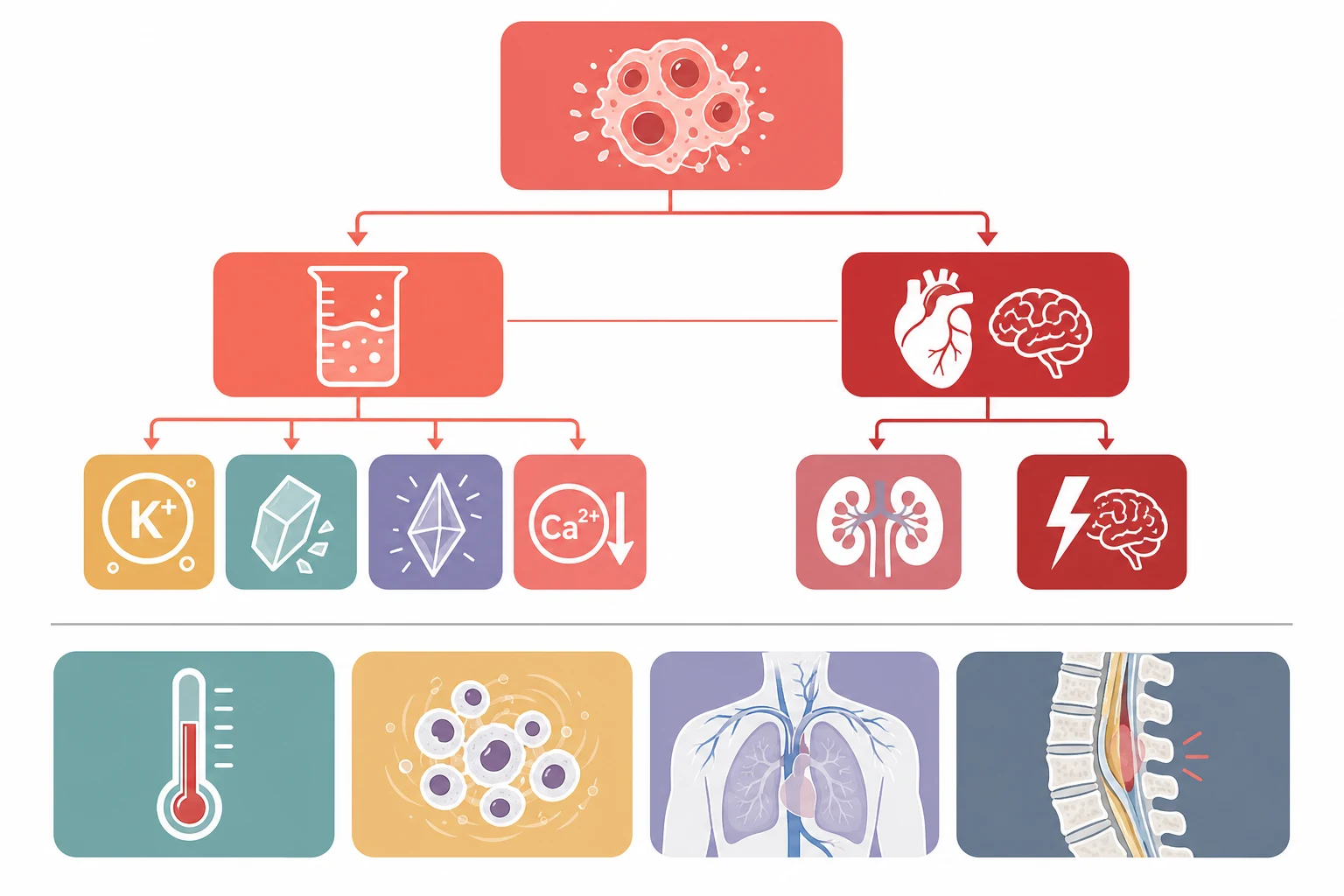
Tumour lysis syndrome is the name for the cluster of metabolic derangements that follow the rapid breakdown of a bulky tumour. The dying cells release their intracellular potassium, phosphate and nucleic acids, and the nucleic acids are turned into urate. When the release outstrips the renal excretion, the potassium rises, the phosphate rises, the urate rises, and the calcium falls, and the child develops an acute kidney injury, a cardiac arrhythmia, or a seizure. The classification that every candidate must carry is the Cairo-Bishop definition, which separates the laboratory tumour lysis syndrome, a pattern on the blood test, from the clinical tumour lysis syndrome, the same pattern plus an organ that fails. [2]
This topic holds tumour lysis at its centre because it is the model oncologic emergency: the danger is inside the child, it is predictable, and it is preventable. Around it sit the other paediatric oncologic emergencies that share the same logic of anticipation and speed. Fever in the neutropenic child is a bacterial emergency that kills within hours, so the antibiotic is given within one hour of arrival. A white cell count over one hundred times ten to the nine per litre makes the blood too thick to flow through the brain and the lungs, so the cells are lowered before the blood is transfused. An anterior mediastinal mass can collapse the airway the moment sedation removes the tone that holds it open, so the airway is secured before any procedure. A tumour pressing on the spinal cord can paralyse a child within a day, so the steroid and the scan are given without delay. Each of these is a decision that changes an outcome, which is why they sit together in the fellowship examination. [5][6]
Classification
Begin with the tumour burden, because the risk of tumour lysis is set long before the chemotherapy begins. A large, fast-growing tumour with a high cell turnover and a high white cell count carries the most risk, because there is more cell mass to break down. The highest-risk tumours in childhood are the Burkitt and the lymphoblastic lymphomas, the T-cell acute lymphoblastic leukaemia with a high white cell count, the acute myeloid leukaemia, and the bulky advanced-stage solid tumours. The risk is refined by the tumour sensitivity, the lactate dehydrogenase as a marker of the tumour burden, the pre-existing renal function, and the hydration status, and the 2010 Cairo risk stratification sorts the child into the low, the intermediate and the high risk to decide the intensity of the prophylaxis. [3]
The Cairo-Bishop definition from 2004 is the framework the examination rewards, and it turns the bedside recognition into an objective set of numbers. The laboratory tumour lysis syndrome is present when two or more of four biochemical derangements appear within the window of three days before to seven days after the start of the cytotoxic therapy, and each derangement is met either by an absolute threshold or by a twenty-five percent change from the baseline. The thresholds are a urate over four hundred and seventy-six micromoles per litre, a potassium over six millimoles per litre, a phosphate over two point one millimoles per litre in the child, and a corrected calcium under one point seven five millimoles per litre. The clinical tumour lysis syndrome adds an organ effect to the laboratory derangement, and it is present when the laboratory criteria are met alongside an acute kidney injury, a cardiac arrhythmia or a sudden death, or a seizure. [2]
The phosphate threshold is age-adjusted, and the candidate who remembers this avoids a common error. Children have a higher normal phosphate than adults because of their active bone growth, so the threshold that defines the hyperphosphataemia of tumour lysis is set higher in the child, at two point one millimoles per litre, than in the adult, at one point four five millimoles per litre. The calcium derangement is the mirror of the phosphate rise, because the phosphate binds the calcium and drives it down, and the symptomatic hypocalcaemia is what produces the tetany, the cramps and the seizure. The lesson is that the four numbers move together, and the child who meets two of them in the treatment window has the laboratory tumour lysis syndrome whether or not they feel unwell. [1]
Epidemiology & Risk Factors
The tumours that threaten a child with tumour lysis are the ones with the highest cell turnover and the largest burden, and the candidate should hold the short list. The Burkitt lymphoma is the classic high-risk tumour, with its extraordinarily rapid doubling time of around twenty-four hours and its large abdominal or jaw mass, and it is the tumour for which the aggressive prophylaxis was first developed. The lymphoblastic lymphoma, the T-cell acute lymphoblastic leukaemia with a white cell count over one hundred times ten to the nine per litre, the acute myeloid leukaemia, and the high-burden advanced-stage solid tumours round out the high-risk group. The standard-risk B-cell precursor leukaemia of the young child is usually low risk. [3]
The host features raise the risk further, and they are worth a mark at the viva. A pre-existing renal impairment, an oliguria, a dehydration, and an acidic urine all reduce the clearance of the urate and the phosphate and so raise the risk of the clinical syndrome. A high lactate dehydrogenase reflects the large tumour burden and the high turnover, and it is a useful marker of the risk alongside the white cell count and the tumour size. The combination of a high-risk tumour, a high lactate dehydrogenase, and an impaired renal function is the profile that demands the rasburicase and the intensive monitoring before the first dose of chemotherapy. [3]
The timing of the tumour lysis is narrow and predictable, which is why the prevention works. The peak of the metabolic derangement falls in the first twenty-four to seventy-two hours after the start of the cytotoxic therapy, although a spontaneous tumour lysis can occur before any treatment in the very high-burden disease. The Cairo-Bishop window of three days before to seven days after the therapy captures the great majority of the events, and the intensive biochemical monitoring is concentrated in this window. The message for the exam is that the danger is in the first few days, and the vigilance is matched to it. [1]
Pathophysiology
The pathophysiology of tumour lysis is the pathophysiology of a cell dying fast, and it is worth walking through because it explains every feature. A tumour cell is rich in potassium, in phosphate, and in the nucleic acids that carry its genetic material. When the chemotherapy kills the cell rapidly, all of this intracellular contents is dumped into the bloodstream at once. The potassium rises, the phosphate rises, and the nucleic acids are broken down into purines and then into uric acid. The normal kidney can clear a modest rise, but a bulky tumour releases more than the kidney can handle, and the four derangements follow. [1]
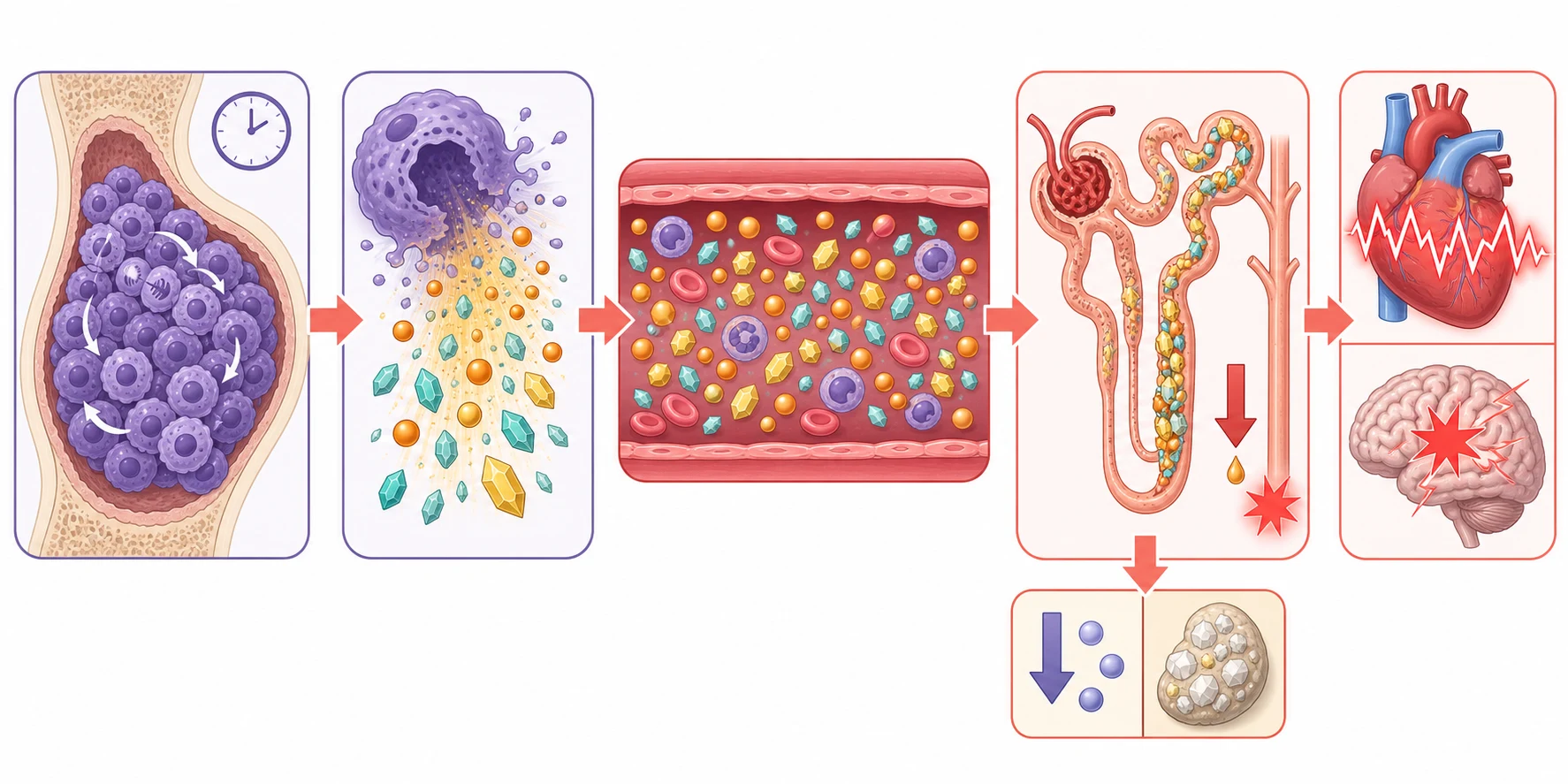
The urate is the kidney's enemy, and the story of the urate is the story of the acute kidney injury. The uric acid is poorly soluble, and at the high concentrations of the tumour lysis it precipitates in the acidic environment of the renal tubule and blocks the flow of the filtrate. The phosphate adds a second kidney injury, because it binds the calcium to form the calcium-phosphate crystals that deposit in the renal tubules and the collecting system, a process called the nephrocalcinosis. The kidney injury is worsened by the prerenal component of the dehydration that often accompanies the presentation, and the cycle is vicious, because the failing kidney clears the urate and the phosphate even less well, and the levels climb further. [1]
The potassium and the calcium are the heart's and the brain's enemies, and they are what kill the child. The hyperkalaemia raises the resting potential of the cardiac myocyte and produces the characteristic ECG changes of the peaked T waves, the widened QRS, and finally the arrhythmia and the arrest. The hypocalcaemia, driven by the phosphate binding, lowers the threshold for the neuromuscular excitability and produces the perioral tingling, the tetany, the carpopedal spasm, the Chvostek and the Trousseau signs, and ultimately the seizure. The calcium must be checked before it is corrected, however, because the correction in the high-phosphate state drives more calcium-phosphate deposition and worsens the kidney injury. [1][2]
Clinical Presentation
The child with the clinical tumour lysis syndrome is a sick child, and the symptoms map directly onto the four derangements. The hyperkalaemia declares itself through the cardiac symptoms of the palpitations, the chest pain, and the syncope, and through the ECG changes that may precede the symptoms. The hypocalcaemia declares itself through the neuromuscular symptoms of the muscle cramps, the tetany, the carpopedal spasm, and the seizure. The acute kidney injury declares itself through the oliguria, the fluid overload, and the hypertension, and the child may be encephalopathic from the uraemia. The tempo is hours, not days, and a child who was stable in the morning can arrest by the evening. [5]
The laboratory tumour lysis syndrome is often silent, and this is the trap. A child on the high-risk protocol can run a rising potassium and a rising phosphate that the four-to-six-hourly biochemistry alone detects, long before any symptom appears. This is the reason for the intensive monitoring, because the silent biochemical rise is the window in which the intervention prevents the clinical syndrome. The child who is monitored only on the symptoms will be monitored too late, and the message is that the numbers are watched, not the child. [1]
The other oncologic emergencies declare themselves through their own signatures, and the candidate must hold each one. The febrile neutropenia declares itself as a fever in the child with a neutrophil count under zero point five times ten to the nine per litre, and it may have no focus, because the neutropenic child mounts no pus and no localising sign. The hyperleukocytosis declares itself through the leukostasis, with the neurological signs of the confusion, the seizure and the stroke, and the respiratory signs of the hypoxia and the diffuse pulmonary infiltrate. The superior vena cava obstruction declares itself through the facial and the upper-limb swelling, the raised jugular venous pressure, and the dyspnoea that worsens on lying flat. The cord compression declares itself through the back pain, the leg weakness, and the change in the bowel and the bladder function. [5][6]
Differential Diagnosis
The differential of a rising potassium in the child with cancer is short, but each entry changes the management. The haemolysed sample is the commonest mimic, and a single high potassium in a well child with a normal ECG is rechecked on a free-flowing sample before any treatment. The true hyperkalaemia of the tumour lysis sits alongside the phosphate and the urate rises, and the four move together, which is the discriminator from the isolated hyperkalaemia of the renal failure or the drug effect. The acute kidney injury of the tumour lysis is distinguished from the prerenal injury of the dehydration, the sepsis, and the nephrotoxic drugs by the pattern and the course. [1]
The differential of the anterior mediastinal mass and the superior vena cava syndrome must be run at the bedside, because the mimic can change the airway plan. A pericardial tamponade can produce the raised venous pressure and the dyspnoea, and it is excluded by the bedside echocardiogram. A severe asthma or a foreign body can produce the respiratory distress, and the wheeze and the history point to them. The anterior mediastinal mass declares itself on the chest imaging, but the candidate must remember that the imaging is done in a child who is kept upright and never sedated for the scan if the airway is threatened. [5]
The back pain in the child with cancer is the differential that decides the speed of the imaging. A simple mechanical back pain, a muscle strain, or a vertebral collapse from the steroid osteoporosis are common, but the malignant cord compression is the diagnosis that cannot be missed, because the window to preserve the ambulation is measured in hours. Any child with cancer who develops a back pain with a neurological symptom, a weakness, a sensory change, or a bowel or bladder dysfunction, is assumed to have a cord compression until the magnetic resonance imaging proves otherwise. [7]
Clinical & Bedside Assessment
The bedside assessment of the child with a suspected oncologic emergency is a search for the immediately dangerous elements, and it begins with the airway, the breathing and the circulation. The child with the anterior mediastinal mass is assessed for the stridor, the orthopnoea, the facial swelling, and the raised venous pressure, and the position is kept upright. The child with the tumour lysis is assessed for the fluid status, the urine output, and the signs of the hyperkalaemia and the hypocalcaemia, and the ECG is obtained early for the peaked T waves. The child with the cord compression is assessed for the back tenderness, the motor power, the sensory level, and the anal tone and the sacral sensation. [5]
The focused examination takes only a few minutes, and each finding carries a decision. The heart is auscultated and the ECG is read for the arrhythmia of the hyperkalaemia. The abdomen is palpated for the tumour mass of the Burkitt lymphoma and the bladder of the urinary retention of the cord compression. The chest is examined for the mediastinal mass and the effusion. The nervous system is examined for the cranial nerves and the motor and the sensory levels, and the limbs for the power, the tone, and the reflexes. The skin is inspected for the pallor, the bruising, and the petechiae of the marrow failure. [5]
The focused assessment of the child with a suspected oncologic emergency
Assess the airway and the breathing first, with the child kept upright, looking for the stridor, the orthopnoea, the facial swelling and the raised jugular venous pressure of the mediastinal mass
Assess the circulation and the fluid status, the heart rate, the blood pressure, the perfusion, and the urine output, and obtain the early ECG for the peaked T waves of the hyperkalaemia
Examine the abdomen for the tumour mass and the bladder retention, and the chest for the mediastinal mass and the effusion
Perform the focused neurological examination for the motor power, the sensory level, the reflexes, and the anal tone and the sacral sensation of the cord compression
Inspect the skin for the pallor, the bruising and the petechiae of the marrow failure
Plan the urgent blood tests and the biochemistry, secure the venous access, and make the decision on the stability for any procedure
The decision on the stability for the diagnostic procedures is the decision that catches the unwary, and it rests on the principle that the unstable child is resuscitated before the definitive investigation. A child with a threatened airway from a mediastinal mass has the tissue diagnosis made by the least-invasive route, not by the sedated biopsy. A child with the tumour lysis has the electrolytes corrected and the kidney supported before the definitive cancer therapy is escalated. A child with the cord compression has the steroid started and the imaging arranged before the elaborate workup. The lesson is that the emergency is treated first, and the diagnosis is confirmed in parallel. [6]
Investigations
The investigation of the suspected tumour lysis is built around the frequent biochemistry, and the frequency is the point. The first-line panel includes the potassium, the phosphate, the calcium, the creatinine, the urate, the lactate dehydrogenase, the electrolytes, the full blood count, and the ECG. In the high-risk child the biochemistry is repeated every four to six hours for the first twenty-four to forty-eight hours, and the urine output is measured hourly. The reason for the frequency is that the silent biochemical rise is the window for the prevention, and a four-hour gap can miss the rise that precedes the arrest. [1][4]
The ECG is the single most useful bedside test in the hyperkalaemia, and the candidate must know its progression. The early changes are the peaked, the narrowed, and the tented T waves, followed by the widening of the QRS, the prolongation of the PR interval, the loss of the P wave, and finally the sine wave and the ventricular fibrillation or the asystole. The ECG change is the trigger for the immediate calcium gluconate to stabilise the cardiac membrane, even before the confirmatory biochemistry returns, because the arrhythmia of the severe hyperkalaemia can be fatal within minutes. [5]
The imaging is tailored to the structural emergencies, and it is urgent. The child with the suspected cord compression has the urgent whole-spine magnetic resonance imaging, because the plain films and the computed tomography miss the soft-tissue cord compression, and the window to preserve the ambulation is short. The child with the mediastinal mass has the chest imaging, but the candidate must remember that the computed tomography or the magnetic resonance imaging with the contrast defines the mass and the airway compromise, and the least-invasive tissue diagnosis is preferred over the sedated biopsy. [7]
Management — Resuscitation
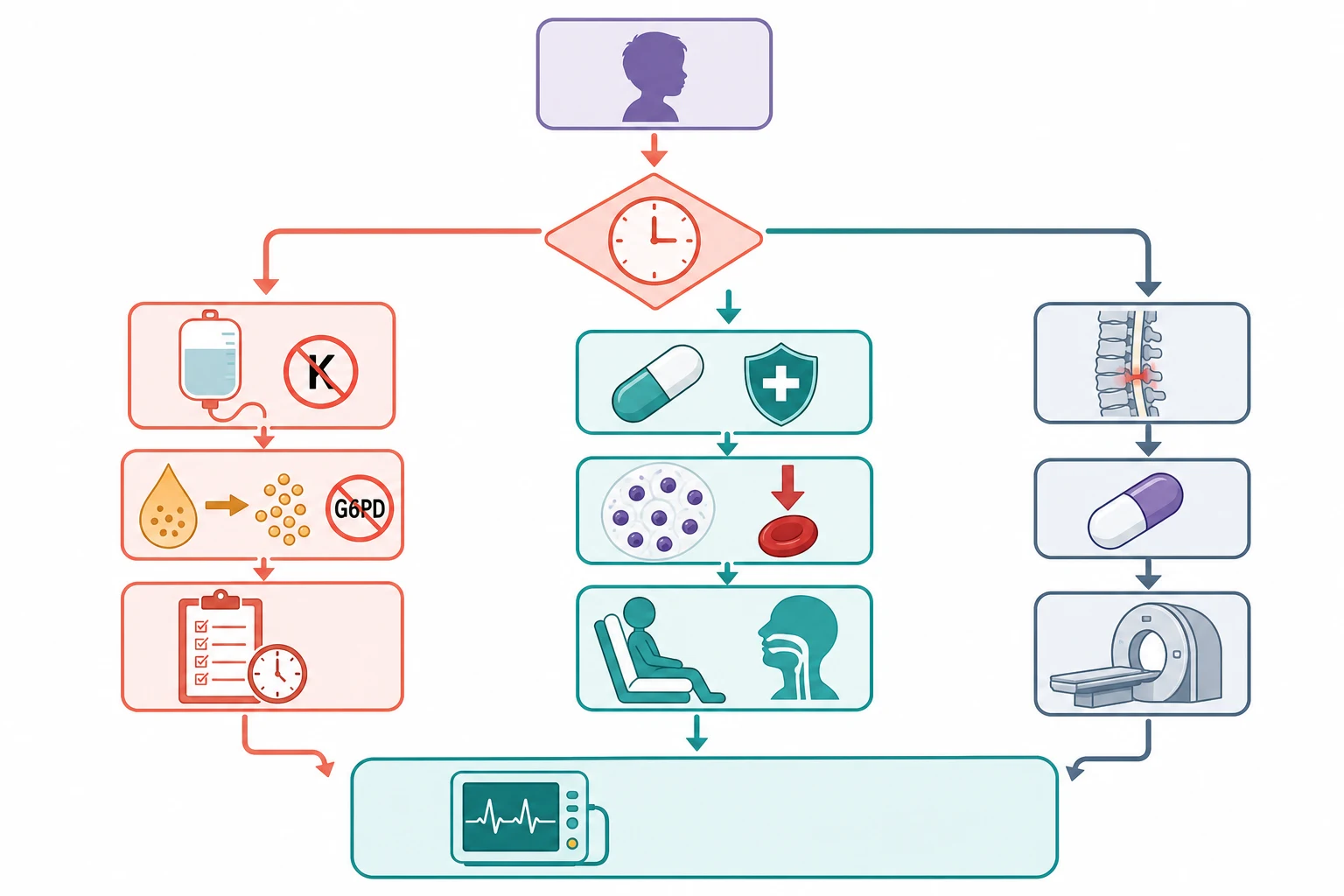
The resuscitation of the child with the tumour lysis rests on the prevention, and the prevention begins before the first dose of the chemotherapy. The foundation is the hyperhydration with an isotonic fluid that contains no potassium, run at two to three litres per square metre per day to maintain a urine output above two millilitres per kilogram per hour. The high urine flow flushes the urate and the phosphate through the tubules before they can precipitate, and it is the single most effective preventive measure. The fluid is potassium-free because the addition of the potassium to a child already hyperkalaemic would be dangerous, and the urine output is maintained with the careful fluid balance and the furosemide only if the volume is overloaded. [1][4]
The rasburicase is the drug that changed the tumour lysis management, and the candidate must know it precisely. Rasburicase is a recombinant urate oxidase that converts the existing uric acid into the soluble allantoin, and it lowers the urate within hours, far faster than the allopurinol, which only blocks the new urate formation. The dose for the high-risk child is zero point one five to zero point two milligrams per kilogram, given as a single dose or daily for up to five days, and it is given before the first dose of the chemotherapy. The allopurinol, at ten milligrams per kilogram per day in the divided doses, is reserved for the low and the intermediate risk child, and for the child in whom the rasburicase is contraindicated. [1][4]
Tumour lysis prophylaxis for the high-risk child
Dose
Hyperhydration with an isotonic potassium-free fluid at two to three litres per square metre per day to keep the urine output above two millilitres per kilogram per hour, with rasburicase at zero point one five to zero point two milligrams per kilogram as a single dose or daily for up to five days, or allopurinol at ten milligrams per kilogram per day in the divided doses for the low or the intermediate risk child
The hyperkalaemia is the immediate killer, and its management is staged by the severity and the ECG changes. The calcium gluconate at zero point five millilitres per kilogram of the ten percent solution, given slowly intravenously, stabilises the cardiac membrane within minutes, and it is given the moment the ECG shows the severe changes, before anything else. The insulin and the glucose, the salbutamol, and the sodium bicarbonate shift the potassium into the cell over the next minutes to hours. The refractory hyperkalaemia, the oliguria, the volume overload, and the symptomatic uraemia are the indications for the renal replacement therapy, which removes the potassium, the phosphate, and the fluid directly. [5]
Management — Definitive & Stepwise
The definitive management of the tumour lysis is the stepwise escalation that matches the severity, and it runs from the prophylaxis through the electrolyte correction to the renal replacement. The prophylaxis by the risk group is the first step, and it is settled by the Cairo risk stratification. The low-risk child receives the hydration and the allopurinol, the intermediate-risk child receives the hydration and the allopurinol with the rasburicase held in reserve, and the high-risk child receives the hydration and the rasburicase from the outset. The four-to-six-hourly biochemistry is the surveillance that triggers the escalation, and the renal replacement therapy is the ceiling of the supportive care. [3][4]
[1] [5]The hyperleukocytosis is managed by the hydration and the cytoreduction, and the principle of avoiding the early red-cell transfusion is the high-yield fact. A white cell count over one hundred times ten to the nine per litre makes the blood too viscous for the microcirculation, and the transfusion of the red cells raises the viscosity further and worsens the leukostasis. The hydration is the first step, the hydroxyurea lowers the count over the hours to days, and the leukapheresis is reserved for the severe leukostasis with the neurological or the respiratory compromise, where the cells are removed directly. The red-cell transfusion, if it is needed for the symptomatic anaemia, is given slowly and only after the cytoreduction has begun. [8]
The febrile neutropenia is managed empirically with the antipseudomonal beta-lactam within one hour of the presentation, after the blood cultures are drawn. The monotherapy with the cefepime, the ceftazidime, the piperacillin-tazobactam, or the meropenem is the standard, and the aminoglycoside and the glycopeptide are added for the haemodynamically unstable child or when a resistant organism is suspected. The child is monitored closely for the first twenty-four hours, and the source is sought with the cultures and the imaging. The principle is that the fever in the neutropenic child is a bacterial emergency until proven otherwise, and the antibiotic is never withheld for the workup. [10]
Febrile neutropenia empiric cover
Dose
An antipseudomonal beta-lactam such as the cefepime, the ceftazidime, the piperacillin-tazobactam or the meropenem as the monotherapy, with the aminoglycoside and the glycopeptide added for the unstable child or the suspected resistant organism
Specific Subtypes & Scenarios
The Burkitt lymphoma and the very high-risk tumour
The Burkitt lymphoma is the tumour that taught the world the tumour lysis prevention, and it holds a special place in the topic. Its extraordinarily rapid growth, with a doubling time of around twenty-four hours, and its large mass, produce the highest cell turnover of any childhood tumour, and the start of its chemotherapy releases a torrent of intracellular contents. The prophylaxis is escalated accordingly, with the aggressive hyperhydration, the rasburicase from the outset, the allopurinol, and the intensive four-to-six-hourly biochemistry, and the team is prepared for the renal replacement therapy from the first day. The lesson is that the Burkitt lymphoma is managed by a team that expects the tumour lysis and that has the supportive care ready. [3]
The mediastinal mass and the superior vena cava syndrome
The child with the anterior mediastinal mass and the superior vena cava obstruction is the scenario that turns every procedure into an airway emergency, and the management is built on the airway-first principle. The child is kept upright, the supplemental oxygen is given, and the sedation is avoided until the airway is secured in a controlled setting, because the loss of the muscular tone can collapse the trachea against the tumour within seconds. The tissue diagnosis is made by the least-invasive route, the peripheral flow cytometry, the effusion cytology, the bone marrow, or the superficial node under the local anaesthetic, before any sedated biopsy. The steroids or the emergency radiotherapy are given first if the obstruction is critical, accepting that they may obscure the diagnosis, because the airway is the priority. [5][11]
The spinal cord compression
The malignant spinal cord compression is the scenario where the speed of the steroid and the decompression decides whether the child walks again, and the candidate must hold the timeline. The child with the back pain, the leg weakness, and the bowel or the bladder dysfunction is assumed to have the cord compression until the magnetic resonance imaging proves otherwise, and the intravenous dexamethasone is started early to reduce the cord oedema. The urgent whole-spine magnetic resonance imaging defines the level and the cause, and the definitive management is the emergency radiotherapy, the surgical decompression, or the chemotherapy, depending on the tumour type and the response. The ambulation at the presentation is the strongest predictor of the ambulation at the outcome, which is why the window of twenty-four to forty-eight hours is so heavily weighted. [7]
SPINE
The glucose-six-phosphate-dehydrogenase child
The child with the glucose-six-phosphate-dehydrogenase deficiency is the scenario that traps the candidate who gives the rasburicase without the check, and the management is built on the screening. The deficiency is commonest in the African, the Mediterranean, the Middle Eastern, and the South and the East Asian populations, and the screen is performed before the rasburicase in the at-risk child. Where the status is unknown or the deficiency is present, the allopurinol is used, with the hydration and the monitoring, and the rasburicase is reserved for the crisis under the specialist guidance. The rasburicase-induced haemolysis or the methaemoglobinaemia is recognised by the sudden anaemia, the jaundice, and the cyanosis that does not respond to the oxygen, and it is treated with the supportive care, the exchange transfusion, and the methylene blue where appropriate. [9]
Complications & Pitfalls
The complications of the tumour lysis itself are the complications of the four derangements, and they are the reasons the syndrome is feared. The cardiac arrest from the hyperkalaemia is the commonest cause of the death, and it may be the first sign in the unmonitored child. The acute kidney injury ranges from the transient oliguria to the irreversible failure, and the calcium-phosphate deposition can leave a permanent nephropathy. The seizure from the hypocalcaemia or the uraemia and the neurological injury from the leukostasis complete the acute harm. The message is that the untreated tumour lysis is a multi-organ failure, and the prevention is the only reliable management. [1]
The complications of the management are the costs of the drugs and the fluids that save the child. The rasburicase causes the haemolysis and the methaemoglobinaemia in the glucose-six-phosphate-dehydrogenase deficiency, and the allopurinol causes the rash and the rare hypersensitivity. The hyperhydration causes the circulatory overload, especially in the child with the renal impairment, and the over-correction of the calcium in the high-phosphate state drives the calcium-phosphate deposition and worsens the kidney injury. The principle of correcting only the symptomatic hypocalcaemia, and never the asymptomatic biochemical low calcium, is the rule that prevents this iatrogenic harm. [9][1]
The pitfall of the early red-cell transfusion in the hyperleukocytosis is worth a separate mention, because it is a recurring error. A child with a leukaemia and a white cell count over one hundred is often also anaemic, and the temptation to transfuse the red cells is strong, but the transfusion raises the viscosity and worsens the leukostasis. The red cells, if they are needed, are given slowly and only after the cytoreduction has begun, and the hydration is the first step. The lesson is that the hyperleukocytosis is managed by the lowering of the white cells, not by the raising of the red cells. [8]
Prognosis & Disposition
The prognosis of the tumour lysis syndrome is decided by whether it was anticipated. A tumour lysis that is prevented by the risk-stratified prophylaxis carries a near-normal outlook for the metabolic emergency, and the child proceeds to the definitive cancer therapy. A tumour lysis that declares and is treated late carries a significant mortality from the cardiac arrest and the renal failure, and the survivors may be left with the chronic kidney disease. The lesson is that the prognosis is set by the anticipation, and the anticipation is set by the risk stratification at the start of the therapy. [1]
The disposition of the child with the oncologic emergency is the specialist paediatric oncology centre, with the paediatric intensive care and the renal replacement therapy available. The high-risk child is admitted for the prophylaxis and the intensive monitoring from the first day of the chemotherapy, and the child with the clinical tumour lysis is managed in the intensive care. The child with the febrile neutropenia is admitted for the intravenous antibiotics and the monitoring, and the child with the cord compression is admitted for the urgent imaging and the steroid or the decompression. The safety-net is the family taught to return at once with the fever or the new symptom. [5]
The prognosis of the cord compression is decided by the speed of the intervention, and the candidate must carry the numbers. The ambulation at the presentation is the strongest predictor of the ambulation at the outcome, and the child who is ambulant at the presentation and treated within twenty-four to forty-eight hours has the best chance of walking again. The child who is paraplegic at the presentation has a much poorer outlook, which is why the early steroid and the imaging are so heavily weighted. The long-term outcome also depends on the tumour type and the response, and the survivors are followed for the late effects of the radiotherapy and the surgery. [7]
In Australia and Aotearoa New Zealand, the child with the oncologic emergency is managed in a tertiary paediatric oncology centre, with the paediatric retrieval services transferring the unstable child from the regional or the rural hospital. The family is supported by the paediatric oncology group, the social work, and the educational liaison, and the long-term survivor is followed in the late-effects clinic. The regional differences are chiefly in the distance and the retrieval time, which is why the early recognition and the stabilisation in the referring hospital, and the communication with the specialist centre before the transfer, are so heavily weighted in the exam.
[5][6]Special Populations
The neonate and the infant with the high-burden leukaemia hold a special position in the topic, because the fluid and the electrolyte management is more delicate. The infant has a smaller circulating volume and a less mature renal function, and the hyperhydration must be run with the careful monitoring of the fluid balance and the weight. The glucose and the electrolyte stability are harder to maintain, and the rasburicase is dosed by the weight. The lesson is that the infant tumour lysis is managed with the same principles and a finer attention to the detail. [1]
The glucose-six-phosphate-dehydrogenase population is the special population that decides the drug choice, and the screening is built into the high-risk protocol. The deficiency is commonest in the African, the Mediterranean, the Middle Eastern, and the South and the East Asian populations, and the screen is offered to the at-risk child before the rasburicase. Where the deficiency is present, the allopurinol is used, with the hydration and the monitoring, and the family is counselled on the rationale and on the avoidance of the other oxidant triggers. [9]
The socioeconomic disadvantage, the remoteness, and the migrant or the refugee status shape the access to the specialist centre and the prevention of the oncologic emergencies, and they are the reason the early recognition in the regional hospital is so heavily emphasised. A child far from the specialist centre may first present to a clinician who sees few such cases, and the recognition of the emergency and the early communication with the specialist centre are the bridge to the retrieval and the definitive care. The adherence to the monitoring and the follow-up is itself a function of the social support. [6]
The adolescent with the high-risk tumour is counselled and supported through the oncologic emergency and the transition into the definitive therapy, with the attention to the reproductive and the fertility counselling before the gonadotoxic therapy, the psychological burden of the diagnosis, and the transition to the adult service. The young person is offered the fertility preservation before the therapy, and the survivorship plan is begun from the day of the diagnosis. [5]
Evidence, Guidelines & Regional Differences
The landmark evidence that underpins the modern tumour lysis management is the Cairo-Bishop classification of 2004 and the 2010 risk-stratification recommendation, and together they turned the bedside recognition into an objective set of criteria and a risk-stratified prophylaxis. The classification gave the field a common language for the laboratory and the clinical syndrome, and the risk stratification matched the intensity of the prophylaxis to the risk, so that the rasburicase was reserved for the high-risk child and the allopurinol for the low. The contemporary consensus guidelines, including the 2023 United States expert panel, have refined the prophylaxis and the monitoring, and the principle of the anticipation has held. [2][3][4]
The risk stratification and the prophylaxis for the tumour lysis are broadly consistent across Australia, Aotearoa New Zealand, the United Kingdom, the United States and Canada, with the hyperhydration and the rasburicase for the high-risk child and the allopurinol for the low. The exact rasburicase dose, the single-dose versus the multi-day course, and the frequency of the biochemistry differ in the detail by the protocol and the centre, and the glucose-six-phosphate-dehydrogenase screening is more uniform in the regions with the higher prevalence. The fellow should know the local protocol and the regional oncology group guidance.
[1][4]The controversies in the field are the live ones, and the fellow holds them as open questions. The optimal rasburicase dose and the single-dose versus the multi-day course are debated, with the trend toward the lower and the single dose driven by the cost and the safety. The place of the leukapheresis in the hyperleukocytosis is contested, because the evidence for the benefit over the hydration and the hydroxyurea is mixed, and the complication rate of the procedure is real. The decompression versus the radiotherapy for the paediatric cord compression depends on the tumour type, the radiosensitivity, and the spinal stability, and the evidence is maturing. [3][7][8]
Exam Pearls
The high-yield facts for the exam are the ones that change a decision at the bedside. The Cairo-Bishop laboratory tumour lysis syndrome is two or more of the urate over four hundred and seventy-six micromoles per litre, the potassium over six millimoles per litre, the phosphate over two point one millimoles per litre in the child, and the corrected calcium under one point seven five millimoles per litre, within three days before to seven days after the cytotoxic therapy, and the clinical form adds the acute kidney injury, the arrhythmia, or the seizure. The high-risk child gets the hyperhydration with the isotonic potassium-free fluid and the rasburicase at zero point one five to zero point two milligrams per kilogram before the first dose, with the four-to-six-hourly biochemistry. [1][2]
The other oncologic emergencies carry their own high-yield facts. The febrile neutropenia gets the antipseudomonal beta-lactam within one hour after the blood cultures. The hyperleukocytosis over one hundred times ten to the nine per litre is managed by the hydration and the cytoreduction without the early red-cell transfusion. The anterior mediastinal mass with the stridor or the superior vena cava obstruction is an anaesthetic catastrophe, and no sedation is given before the airway is secured. The cord compression is managed by the urgent imaging and the high-dose dexamethasone within twenty-four to forty-eight hours to preserve the ambulation. The rasburicase is contraindicated in the glucose-six-phosphate-dehydrogenase deficiency. [5][7]
The final pearls are the ones that catch the candidate who has learned the headline and forgotten the corner. The calcium is corrected only if the hypocalcaemia is symptomatic, because the correction in the high-phosphate state worsens the deposition. The calcium gluconate for the hyperkalaemia is given the moment the ECG changes appear, before the confirmatory biochemistry. The red-cell transfusion in the hyperleukocytosis is withheld first and given slowly after the cytoreduction. The least-invasive tissue diagnosis is preferred for the mediastinal mass. The back pain with the weakness is the cord compression until the magnetic resonance imaging proves otherwise. The candidate who holds these corners has the reasoning that carries the topic. [1][5]
References
- [1]Howard SC, Avagyan A, Workeneh B, Pui CH Tumour lysis syndrome Nat Rev Dis Primers, 2024.PMID 39174582
- [2]Cairo MS, Bishop M Tumour lysis syndrome: new therapeutic strategies and classification Br J Haematol, 2004.PMID 15384972
- [3]Cairo MS, Coiffier B, Reiter A, Pui CH Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases Br J Haematol, 2010.PMID 20331465
- [4]Perissinotti AJ, Bishop MR, Bubalo J Expert consensus guidelines for the prophylaxis and management of tumor lysis syndrome in the United States: Results of a modified Delphi panel Cancer Treat Rev, 2023.PMID 37579533
- [5]Prusakowski MK, Cannone D Pediatric Oncologic Emergencies Hematol Oncol Clin North Am, 2017.PMID 29078932
- [6]Briggs JE, Rabin M Oncologic Emergencies Pediatr Rev, 2026.PMID 42219190
- [7]Quraishi NA, Palliyil N, Hassanin MA Malignant spinal cord compression in the paediatric population-a systematic review, meta-analysis. Eur Spine J, 2023.PMID 37338630
- [8]Lowe EJ, Pui CH, Hancock ML, Geiger TL, Bakke AC, Fletcher BD, Sandlund JT Early complications in children with acute lymphoblastic leukemia presenting with hyperleukocytosis Pediatr Blood Cancer, 2005.PMID 15547931
- [9]Hammami MB, Qasim A, Thakur R, Soubra R, Al-Shash S Rasburicase-induced hemolytic anemia and methemoglobinemia: a systematic review of current reports Ann Hematol, 2024.PMID 37468669
- [10]Lehrnbecher T, Robinson PD, Ammann RA, et al Guideline for the Management of Fever and Neutropenia in Pediatric Patients With Cancer and Hematopoietic Cell Transplantation Recipients: 2023 Update. J Clin Oncol, 2023.PMID 36689694
- [11]Leung KKY, Hon KL, Hui WF, Li AM, Cheung HM Therapeutics for paediatric oncological emergencies Drugs Context, 2021.PMID 34234831