Paeds · infectious-diseases
Animal bites, arthropod bites and zoonoses
Also known as Dog and cat bites · Mammalian bite wounds · Cat scratch disease · Rabies and Australian bat lyssavirus · Tick-borne disease and Lyme disease · Scabies · Snakebite and envenomation · Brucellosis, Q fever and leptospirosis
Fellowship guide to animal and arthropod bites and zoonoses in children: the exposure history that drives risk stratification, dog and cat bite microbiology with Pasteurella and Capnocytophagus, the irreplaceable role of wound irrigation and the hand-bite rule, rabies and Australian bat lyssavirus post-exposure prophylaxis with immunoglobulin and vaccine, cat scratch disease and Bartonella, tick-borne Lyme and rickettsial disease, scabies, snakebite pressure-immobilisation and antivenom, and the systemic zoonoses leptospirosis, Q fever and brucellosis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
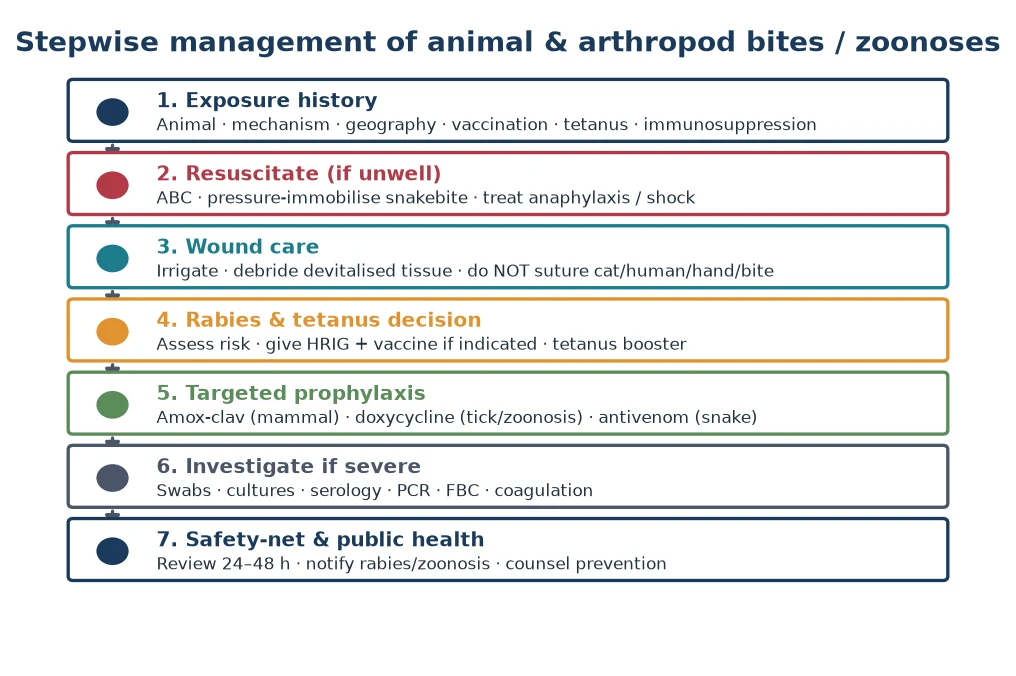
A child who has been bitten by an animal or insect, or who has a fever after contact with animals, sits at a busy crossroads of wound care, microbiology, toxinology, and public health. The unified skill the examiner wants is the ability to extract a precise exposure history and then convert it into three simultaneous decisions: how to clean and dress the wound, whether to give antimicrobial prophylaxis, and whether the encounter carries a rabies or tetanus risk. Most bites are minor and heal with irrigation alone, but a small minority hide deep structure injury, necrotising infection, or a fatal neurotropic virus, and recognising that minority is the whole game. [12]
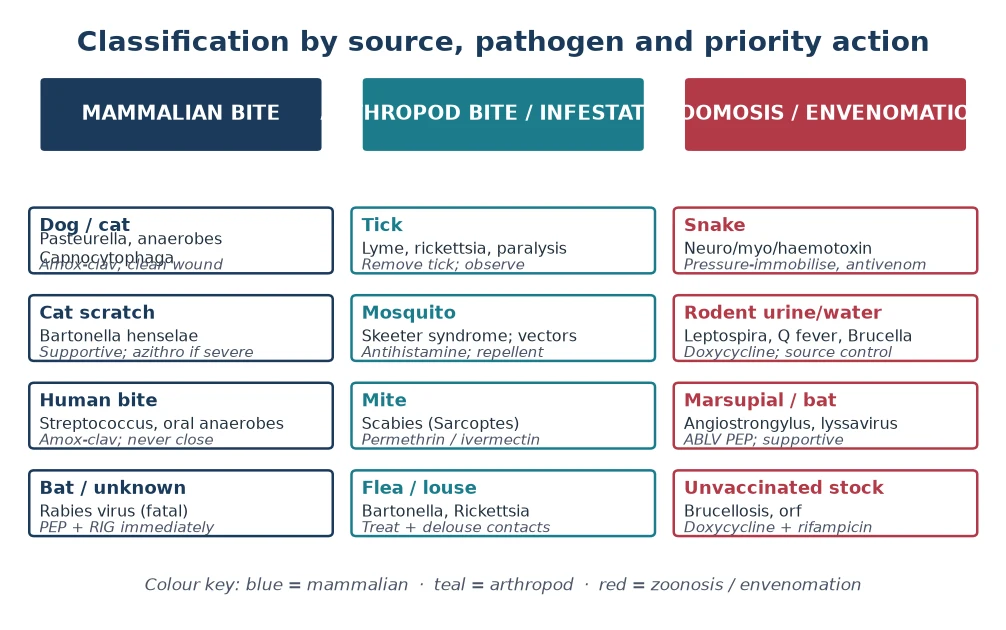
The clinical terrain spans three families of problem that share only the mechanism of animal contact. Mammalian bites inject oral flora such as Pasteurella, anaerobes, and Capnocytophagus into tissue and cause cellulitis, abscess, or sepsis. Arthropod bites and infestations range from immediate hypersensitivity reactions through vector-borne infections such as Lyme disease and rickettsial illness to the intense pruritus of scabies. Zoonoses and envenomation, including snakebite, rabies, leptospirosis, Q fever, and brucellosis, produce systemic disease whose link to the animal encounter may not be obvious unless the history is taken. [1]
The single most load-bearing principle is that the exposure history, far more than any investigation, determines management. Knowing the species, the mechanism, the geography, the child's immune and vaccination status, and the time elapsed turns a generic bite into a specific risk profile and dictates every downstream decision from antibiotic choice to pressure-immobilisation to rabies prophylaxis. [12]
Classification
Clinically, the first split is by the source of the exposure, because source predicts both the microbiology and the priority action. A mammalian bite from a dog, cat, or human demands wound care and prophylaxis against oral flora and a rabies assessment. An arthropod bite or infestation, from a tick, mosquito, mite, flea, or louse, raises the question of vector-borne disease or hypersensitivity. A zoonosis or envenomation, including snakebite, lyssavirus, leptospirosis, Q fever, and brucellosis, is a systemic illness in which the animal link is the diagnostic key. [12]
The second split is by severity and depth, which decides disposition and whether primary closure is safe. A superficial bite with no structural involvement can be managed in the community with review. A bite involving the hand, a joint, a tendon, or bone is high-risk for deep infection and permanent functional loss and must never be primarily closed. A bite in an unvaccinated, immunocompromised, or asplenic child, or one with signs of systemic toxicity, crosses into the urgent or emergency category. [1]
Epidemiology & Risk Factors
Dog and cat bites together account for the great majority of animal bite presentations in children, with dogs most often biting the face and hands of young children and cats producing deep puncture wounds of the hand in older children. Infected mammalian bites are polymicrobial, mixing aerobic and anaerobic oral organisms, and Pasteurella species are recovered from roughly half of infected dog and cat wounds, which explains why agents that cover this fastidious organism are preferred. [1]
Risk factors for a poor outcome cluster around three axes: the depth and location of the wound, the child's host defences, and the delay to care. Hand bites, puncture wounds, and bites crossing joints or tendon sheaths are the wounds most likely to develop deep infection, osteomyelitis, or permanent stiffness. Immunocompromised, asplenic, and chronically ill children, and those on biologic therapy, are vulnerable to overwhelming sepsis even from minor wounds. Delayed presentation, particularly beyond twenty-four hours, sharply raises the infection rate and is the single most modifiable risk. [2]
Arthropod-borne and zoonotic illness is unevenly distributed and tightly geography-bound. Lyme disease is common in endemic areas of North America and Europe but is not acquired locally in Australia, where the controversy over locally acquired Lyme-like illness is resolved by pursuing treatable differential diagnoses. Leptospirosis follows freshwater and rodent exposure, Q fever tracks livestock and parturient animals, and brucellosis reflects unpasteurised dairy or animal-handling exposure. Snakebite disproportionately affects rural children in the tropics and is a major neglected tropical disease. [6]
Pathophysiology
A mammalian bite damages tissue mechanically and simultaneously inoculates the rich oral flora of the animal into devitalised tissue. Dogs generate crush and laceration injuries with high-pressure teeth that drive bacteria deep, while cats produce narrow deep puncture wounds that seal over and trap infection. The inoculum is polymicrobial: Pasteurella multiplies rapidly to produce early cellulitis within twelve to twenty-four hours, alongside streptococci, staphylococci, fusobacteria, and anaerobes, and Capnocytophagus canimorsus rarely causes overwhelming sepsis in asplenic or immunocompromised hosts. [1]
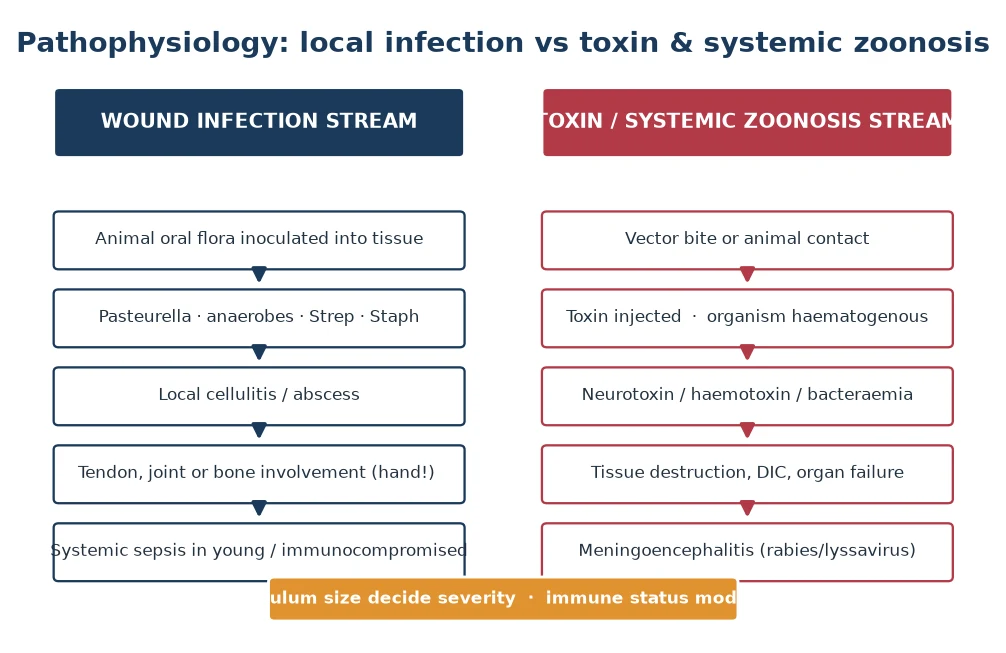
The arthropod and zoonotic stream follows a different biology. Vectors inject organisms or toxins that act systemically rather than locally. A tick attaches and transmits Borrelia, Rickettsia, or a neurotoxin that causes ascending flaccid paralysis; a mosquito injects salivary antigens that trigger immunoglobulin-E mediated papular urticaria or skeeter syndrome; a scabies mite burrows and lays eggs, provoking a delayed type-four hypersensitivity itch. Snake venoms are injected subcutaneously and spread lymphatically, with elapids causing presynaptic or postsynaptic neurotoxicity and coagulopathy. [6]
Host and inoculum factors together determine whether a bite stays local or becomes systemic. A small inoculum in an immunocompetent child with prompt irrigation often resolves, whereas a large inoculum, a deep puncture, or an impaired host converts local cellulitis into lymphangitis, bacteraemia, septic arthritis, osteomyelitis, or necrotising soft tissue infection. Understanding this escalation pathway is what allows the clinician to set the right threshold for review and admission. [12]
Clinical Presentation
Most mammalian bites present with a visible wound, pain, and surrounding erythema, and the task is to judge whether the findings represent normal early inflammation, established infection, or something more dangerous. A bite seen within hours that is clean and minimally tender is at low risk, whereas a bite presenting after twenty-four hours with spreading erythema, warmth, swelling, purulent discharge, or regional lymphadenopathy is infected and needs active treatment. [12]
The features that escalate a bite from routine to dangerous are the ones that signal deep structure involvement or systemic toxicity. Pain on passive movement of a finger, reduced range of motion, or tenderness along a tendon sheath points to tenosynovitis or septic arthritis of the hand. Numbness or weakness suggests nerve injury, crepitus or skin blistering suggests necrotising infection, and fever, tachycardia, or hypotension signals bacteraemia or sepsis. A child who looks unwell after any bite warrants immediate senior review. [1]
Arthropod and zoonotic presentations are more protean and depend entirely on the agent. Tick-borne Lyme disease classically begins with an expanding erythema migrans rash at the bite site days to weeks later, often with low-grade fever, arthralgia, and malaise, while tick paralysis causes an ascending symmetrical weakness over hours to days that can mimic Guillain-Barre syndrome until the tick is found. Scabies presents with intense nocturnal pruritus and burrows in the finger webs, wrists, and axillae. Systemic zoonoses cause undifferentiated prolonged fever with hepatosplenomegaly, arthralgia, or aseptic meningitis, and the animal link is often missed unless asked. [6]
Severity features to seek at the bedside
Deep puncture or wound crossing a joint, tendon, or bone
Hand location with pain on passive movement or reduced range
Spreading erythema, lymphangitis, or regional lymphadenopathy
Purulent discharge, crepitus, or skin blistering suggesting necrotising infection
Fever, tachycardia, hypotension, or a child who looks unwell
Neurological signs after tick attachment or snakebite: ascending weakness
Bleeding, bruising, or coagulopathy after snakebite
Prolonged fever with hepatosplenomegaly suggesting systemic zoonosis
Differential Diagnosis
For an infected bite wound the differential revolves around how deep the infection has gone and whether it is necrotising. Superficial cellulitis sits beside abscess, which needs drainage, and both must be distinguished from necrotising soft tissue infection, which spreads rapidly with severe pain out of proportion to the examination, systemic toxicity, and sometimes crepitus or blistering. Septic arthritis and osteomyelitis are the deep complications to exclude in any hand or joint bite, and Capnocytophagus bacteraemia enters the differential in an asplenic or immunocompromised child with sepsis after a dog bite. [1]
For a febrile child with an arthropod or animal exposure, the differential is broad and depends on the geography. An expanding rash after a tick bite in an endemic area is erythema migrans and Lyme disease, whereas a similar rash in an Australian returned traveller points to alternative diagnoses because locally acquired Lyme is not endemic. A child with fever and ascending weakness after tick attachment has tick paralysis until the tick is removed, and a child with neurotoxic ptosis, ophthalmoplegia, and coagulopathy after a snakebite has envenomation requiring antivenom. [6]
The systemic zoonoses share an undifferentiated febrile prodrome and are separated by their exposure signature. Leptospirosis follows freshwater or rodent exposure and may progress to jaundice, renal failure, and bleeding. Q fever follows livestock or parturient animal exposure and causes atypical pneumonia, hepatitis, or endocarditis. Brucellosis follows unpasteurised dairy or animal handling and causes undulant fever, arthralgia, and hepatosplenomegaly. Each is confirmed by paired serology, and the exposure history is the diagnostic lever. [8]
Clinical & Bedside Assessment
Begin with the paediatric assessment triangle and a sick-or-well judgement, because the envenomated or septic child can decompensate quickly. Record temperature, heart rate, respiratory rate, blood pressure, capillary refill, and oxygen saturation, and examine for the systemic features that demand resuscitation: shock, respiratory distress, and altered conscious level. A child with neurotoxic snake envenomation can lose airway protection within hours, so a sick child after a bite or sting needs early senior and retrieval involvement. [11]
The wound examination is the centrepiece and determines everything downstream. Note the location, depth, and mechanism, and probe for involvement of tendon, joint capsule, bone, nerve, or vessel. Measure and mark the margin of any erythema so spread can be tracked objectively over hours. Examine for purulent discharge, foreign body such as a tooth fragment, and regional lymphadenopathy, and document neurovascular and tendon function distal to the wound before any intervention. [12]
The exposure history is the second centrepiece and frames the rabies, tetanus, and zoonosis decisions. Ask precisely which animal was involved, whether it was provoked, whether it is available for observation, the geographic location, any water, livestock, rodent, or bat exposure, the time elapsed since the bite, and the child's tetanus and rabies vaccination status. In Australia, any bat contact is treated as Australian bat lyssavirus exposure until cleared by public health, regardless of how trivial the scratch appears. [5]
Investigations
Most uncomplicated mammalian bites need no investigation, and management is driven by the history and examination. A wound swab is only useful if the wound is already clinically infected and purulent, in which case it guides therapy for a deep or treatment-failing infection. Blood cultures, full blood count, C-reactive protein, and electrolytes are reserved for the child with systemic toxicity, suspected deep infection, or sepsis, and imaging is indicated when bone, joint, or a retained foreign body such as a tooth is suspected. [12]
For arthropod and zoonotic presentations, the investigations are tailored to the suspected agent. Lyme disease is diagnosed clinically when erythema migrans is present in an endemic area, with serology reserved for later or atypical presentations interpreted by the two-tier framework. Tick paralysis is a clinical diagnosis reversed by tick removal. Scabies is confirmed by identifying burrows or mites on skin scraping. The systemic zoonoses rely on paired serology with a rising titre, and polymerase chain reaction is increasingly used for leptospirosis and Q fever. [6]
Snakebite demands a defined investigation panel because envenomation can be occult. A coagulation profile, full blood count, creatine kinase, urea, creatinine, and a venom detection kit from the bite site swab or urine guide whether antivenom is needed. A child with a normal conscious level, no coagulopathy, and no local effects after observation is likely not envenomed, but deterioration can be delayed, so a period of structured observation with serial testing is standard. [11]
Management — Resuscitation
Resuscitation is reserved for the bite or sting that has produced systemic compromise, and the priorities follow the familiar airway, breathing, circulation sequence. The child with neurotoxic snake envenomation may need airway protection and ventilation as the first priority, and any child in shock from sepsis or haemotoxic envenomation needs intravenous or intraosseous access and careful fluid resuscitation while definitive therapy is prepared. Anaphylaxis after an insect sting is treated with intramuscular adrenaline without delay. [11]
Resuscitation sequence for the severe bite or sting
Assess airway, breathing, circulation and give high-flow oxygen
Secure intravenous or intraosseous access in the shocked or envenomated child
Control catastrophic external bleeding with direct pressure
Keep a snakebite limb immobilised with a pressure-immobilisation bandage in place
Give intramuscular adrenaline for insect-sting anaphylaxis
Draw bloods, coagulation, group and hold, and venom detection kit for snakebite
Summon senior, toxicology, and retrieval support early
The defining first-aid manoeuvre for snakebite in Australia is the pressure-immobilisation bandage, applied over the bite and the whole limb to slow lymphatic venom transport while the child is kept still. The bandage should be firm enough to obstruct lymphatic but not arterial flow, the limb splinted, and the child transported without walking. The common error of washing, incising, or applying a tourniquet must be avoided, because these measures cause harm and do not help. [11]
For the septic child after an infected bite, resuscitation follows paediatric sepsis principles with fluid boluses, early broad-spectrum intravenous antibiotics covering Pasteurella and anaerobes, and source control through drainage of any abscess. The rare child with necrotising soft tissue infection needs aggressive fluid resuscitation, broad-spectrum antibiotics, and urgent surgical debridement in theatre, and this is one diagnosis that must never be watched overnight. [1]
Management — Definitive & Stepwise
Definitive management of the uncomplicated bite rests on three pillars: meticulous wound care, targeted antibiotic prophylaxis, and the rabies and tetanus decision. Copious high-pressure irrigation with normal saline is the single most effective intervention to reduce infection, and devitalised tissue is debrided. Puncture wounds are left open, and most bite wounds are managed by delayed primary closure or secondary intention, because primary closure traps infection, with the rare exception of a clean facial laceration in a child who presents early. [12]
Antibiotic prophylaxis is given for all cat bites, all hand bites, all bites with deep puncture or crush, and any bite in an immunocompromised, asplenic, or chronically ill child, because these are the wounds most likely to become infected. The agent of choice is amoxicillin-clavulanate, which covers Pasteurella, anaerobes, and Capnocytophagus in a single drug; a penicillin-allergic child is managed with doxycycline plus metronidazole or specialist guidance, and a metronidazole and clindamycin combination covers anaerobes. [2]
Amoxicillin-clavulanate
Dose
Children over 2 months: amoxicillin component 22.5 mg/kg orally twice daily for 5 days
When to give antibiotic prophylaxis after a bite
The rabies and tetanus decision is made for every bite and is the highest-stakes part of the encounter. For a child with a possible rabies or lyssavirus exposure, post-exposure prophylaxis is started urgently and consists of thorough wound washing, rabies immunoglobulin infiltrated into and around the wound, and a course of rabies vaccine on days zero, three, seven, and fourteen. Immunoglobulin is given on the first visit only and is critical for a previously unvaccinated child, and the regimen is never delayed while waiting for public health confirmation in a high-risk exposure such as a bat scratch. [5]
Rabies post-exposure prophylaxis: immunoglobulin plus vaccine
Population: Children with possible rabies or Australian bat lyssavirus exposure
Key finding
Prompt wound washing combined with rabies immunoglobulin and a full vaccine course virtually eliminates rabies after a recognised exposure, whereas once symptoms develop the disease is almost universally fatal, which is why every suspected exposure is treated as an emergency.
Tetanus prophylaxis follows the child's vaccination status and the wound characteristics, with a booster and immunoglobulin considered for contaminated or devitalised wounds in a child whose immunisation is incomplete or uncertain. Cat scratch disease is usually self-limiting and treated supportively, with azithromycin reserved for severe or disseminated disease, and scabies is treated with permethrin cream or oral ivermectin with simultaneous treatment of close contacts and bedding. [3]
Specific Subtypes & Scenarios
The dog bite is the most common mammalian bite in children and often involves the face in toddlers and the hand in older children. Management centres on irrigation, debridement of devitalised tissue, amoxicillin-clavulanate prophylaxis for hand and deep wounds, and a rabies and tetanus assessment, with clean facial lacerations managed by a clinician skilled in repair because cosmetic outcome matters in children. The child is reviewed at twenty-four to forty-eight hours to confirm healing and catch early infection. [1]
The cat bite is the bite most likely to become infected, because the long narrow teeth of a cat produce a deep puncture that seals over and seeds Pasteurella into tendon sheaths and joints, especially in the hand. Every cat bite receives prophylactic amoxicillin-clavulanate, the wound is irrigated but not closed, and a hand bite is examined for septic arthritis and tenosynovitis, with surgical exploration if these are suspected. [1]
Cat scratch disease follows a cat scratch or lick and is caused by Bartonella henselae. A papule appears at the inoculation site within days, followed one to two weeks later by tender regional lymphadenopathy that may suppurate, and most cases resolve without antibiotics over weeks to months. Azithromycin is used for severe, prolonged, or disseminated disease, and suppuration may need needle aspiration, with an atypical presentation such as fever of unknown origin, neuroretinitis, or encephalopathy triggering the diagnosis through serology. [3]
Tick-borne disease and scabies cover the common arthropod presentations. Lyme disease in an endemic area is treated with oral amoxicillin or doxycycline guided by the 2020 guideline framework, with erythema migrans treated clinically without serology. Tick paralysis is reversed by finding and removing the embedded tick and watching for recovery, and scabies is treated with permethrin or ivermectin and contact tracing. The systemic zoonoses, leptospirosis, Q fever, and brucellosis, are treated with doxycycline or combination regimens guided by severity, and a returned traveller with undifferentiated fever needs these in the differential alongside malaria. [6]
Snakebite is the archetype of envenomation and is managed with pressure-immobilisation first aid, a period of structured observation, coagulation and venom detection testing, and specific antivenom guided by the venom detection kit or the recognised snake species. Antivenom is given for clinical or laboratory evidence of envenomation, with premedication and resuscitation facilities available because of the risk of reaction, and children receive a full adult dose because the venom load, not the child's weight, determines severity. [11]
Complications & Pitfalls
The complications of mammalian bites range from local cellulitis and abscess through deep structure infection to life-threatening sepsis. Septic arthritis and osteomyelitis of the hand are the complications that cause permanent functional loss, and necrotising soft tissue infection is the one that kills if missed. Capnocytophagus canimorsus bacteraemia causes overwhelming sepsis, particularly in asplenic or immunocompromised children, and is the reason a sick child after a dog bite needs broad cover and senior review. [1]
The complications of the systemic bites and zoonoses are specific to each agent. Lyme disease can progress to arthritis, carditis, and neuroborreliosis if untreated, and tick paralysis can progress to respiratory failure until the tick is removed. Snakebite envenomation causes coagulopathy, renal failure, rhabdomyolysis, and respiratory paralysis, and antivenom itself carries a risk of immediate or serum-sickness reaction. The systemic zoonoses can cause endocarditis, meningitis, or chronic relapsing illness if the exposure link is missed and treatment is delayed. [6]
The common pitfalls are the ones examiners test relentlessly. Closing a hand bite primarily and trapping infection, failing to give prophylaxis for a cat bite, omitting a rabies and tetanus assessment, sending a hand bite home without checking tendon sheath signs, and anchoring on a febrile returned traveller to malaria while missing a treatable zoonosis are the recurring errors. Each is avoided by a disciplined, checklist-driven approach to every bite. [12]
Prognosis & Disposition
The prognosis of an uncomplicated bite that is irrigated early and given appropriate prophylaxis is excellent, with most wounds healing without sequelae. The wounds with a guarded prognosis are the deep hand bites and those with established septic arthritis or osteomyelitis, where permanent stiffness is a real risk, and the bites complicated by necrotising infection or Capnocytophagus sepsis, which carry mortality. Early wound care and the right prophylaxis decision are what convert a potentially serious bite into a routine one. [2]
Disposition follows severity and reliability of follow-up. A child with systemic toxicity, a deep hand infection, suspected necrotising infection, or an unreliable family is admitted, while the rest are discharged with written safety-netting advice, prophylaxis where indicated, and a planned review at twenty-four to forty-eight hours. The child receiving rabies post-exposure prophylaxis leaves with a documented vaccine schedule and a clear plan for the remaining doses, and snakebite cases are observed until envenomation is excluded. [12]
For the systemic zoonoses, prognosis depends on early recognition and targeted therapy. Leptospirosis and Q fever generally respond well to doxycycline, brucellosis requires prolonged combination therapy to prevent relapse, and untreated disease can cause chronic endocarditis or meningitis. Every child treated for a zoonosis needs structured follow-up to confirm clinical and serological resolution and to catch late complications. [8]
Special Populations
Immunocompromised, asplenic, and biologic-treated children are uniquely vulnerable after a bite, because the same inoculum that causes a minor cellulitis in a healthy child can produce overwhelming sepsis here. Capnocytophagus canimorsus is the classic pathogen in the asplenic host, and these children receive prophylaxis for any mammalian bite, are reviewed early, and are admitted at the first sign of systemic illness. The threshold for intravenous antibiotics and admission is deliberately low. [1]
Indigenous and rural children carry a higher burden of bites and zoonoses through outdoor exposure, dog populations, and proximity to livestock and wildlife, and may face barriers to early care that increase the infection rate. Returned travellers, migrant, and refugee children may have had exposures in rabies-endemic countries that were not managed with prophylaxis, and a careful history of animal contact during travel is part of every febrile returned-traveller assessment. [5]
The child in out-of-home care and any child whose immunisation status is uncertain needs the tetanus decision made explicitly and documented, because incomplete tetanus cover converts a contaminated bite into a higher-risk wound. In all these groups the principles are unchanged but the thresholds for prophylaxis, admission, and follow-up are lower, reflecting the greater consequences of a missed infection or an unrecognised exposure. [12]
Evidence, Guidelines & Regional Differences
The evidence base for mammalian bite management rests on the bacteriology of infected dog and cat wounds, which established the polymicrobial nature of the inoculum and the dominance of Pasteurella, and on a meta-analysis of prophylactic antibiotics for dog bites that defined who benefits. These underpin the modern preference for amoxicillin-clavulanate as single-agent prophylaxis and for selective prophylaxis guided by bite source, depth, location, and host. [1]
Rabies and Australian bat lyssavirus policy is driven by the absolute lethality of the disease once symptomatic and the near-complete protection offered by prompt prophylaxis, which is why national guidelines treat every suspected exposure as an emergency. Lyme disease management follows the 2020 Infectious Diseases Society of America guideline, which emphasises clinical diagnosis of erythema migrans and first-line oral antibiotics, and is explicit that chronic Lyme and prolonged antibiotic courses are not supported. [6]
Two regional differences shape practice in Australia and New Zealand. Australian bat lyssavirus is treated identically to rabies, so any bat exposure triggers the full prophylaxis regimen, and locally acquired Lyme disease is not endemic, which means the emphasis in a returned traveller with an expanding rash is on the alternative travel-related diagnoses. Snakebite management is built around pressure-immobilisation first aid and a defined panel of specific antivenoms, and the systemic zoonoses are notifiable diseases that link clinical care to public health. [5]
Exam Pearls
C.R.O.W.S. — when to give bite antibiotic prophylaxis
References
- [1]Talan DA, Citron DM, Abrahamian FM, Moran GJ, Goldstein EJ Bacteriologic analysis of infected dog and cat bites. Emergency Medicine Animal Bite Infection Study Group. N Engl J Med, 1999.PMID 9887159
- [2]Cummings P Antibiotics to prevent infection in patients with dog bite wounds: a meta-analysis of randomized trials. Ann Emerg Med, 1994.PMID 8135429
- [3]Florin TA, Zaoutis TE, Zaoutis LB Beyond cat scratch disease: widening spectrum of Bartonella henselae infection. Pediatrics, 2008.PMID 18443019
- [4]Jackson AC Rabies. Can J Neurol Sci, 2000.PMID 11097515
- [5]Lewis T, Baack K, Greenberg MR Rabies post-exposure prophylaxis in the emergency department. Am J Emerg Med, 2024.PMID 38330834
- [6]Lantos PM, Rumbaugh J, Bockenstedt LK, Falck-Ytter Y, Aguero-Rosenfeld ME, Auwaerter PG, et al Clinical Practice Guidelines by the Infectious Diseases Society of America, American Academy of Neurology, and American College of Rheumatology: 2020 Guidelines for the Prevention, Diagnosis, and Treatment of Lyme Disease. Neurology, 2021.PMID 33257476
- [7]Thomas C, Coates SJ, Engelman D, Chosidow O, Chang AY Ectoparasites: Scabies. J Am Acad Dermatol, 2020.PMID 31310840
- [8]España PP, Uranga A, Aramburu A, Arrieta I, Salcedo I, Mínguez I, et al Q Fever (Coxiella Burnetii). Semin Respir Crit Care Med, 2020.PMID 32629489
- [9]Tullu MS, Karande S Leptospirosis in children: a review for family physicians. Indian J Med Sci, 2009.PMID 19770531
- [10]Tanir G, Tufekci SB, Tuygun N Presentation, complications, and treatment outcome of brucellosis in Turkish children. Pediatr Int, 2009.PMID 19371290
- [11]Iliyasu G, Dajel TB, Abdulkarim A, Tiamiyu AB, Dayyabu F, Salisu IM, et al Comparison of snakebite in children and adults in Nigeria. Toxicon, 2023.PMID 37062344
- [12]Aloi M, Coley T, Kandil T, Damask A, Shah MI Mammalian bite wounds in children: evidence-based management in the emergency department. Pediatr Emerg Med Pract, 2023.PMID 37646652