Paeds · infectious-diseases
Antimicrobial pharmacology, selection, dosing and stewardship in children
Also known as Paediatric antimicrobial stewardship · Antibiotic dosing in children · Antimicrobial selection in children · Paediatric antimicrobial pharmacology · WHO AWaRe in children
A fellowship approach to antimicrobial pharmacology, selection, dosing and stewardship in children covering developmental pharmacokinetics, pharmacodynamic killing patterns, empiric and targeted drug selection, weight-based and age-adjusted dosing, therapeutic drug monitoring, the stewardship cycle of de-escalation, IV-to-oral stepdown and duration review, and the WHO AWaRe framework.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A six-month-old with meningitis who needs the right dose of a third-generation cephalosporin to penetrate the CSF, a toddler on an aminoglycoside whose interval is set to match her renal maturity, and a teenager on broad empiric cover whose antibiotics are narrowed the moment an organism returns — these are the faces of antimicrobial stewardship at the bedside. Stewardship is not restriction for its own sake. It is the organised, evidence-driven effort to ensure that every child receives the antimicrobial most likely to work, at a dose that achieves it, for just long enough, and no longer. [1] [8]
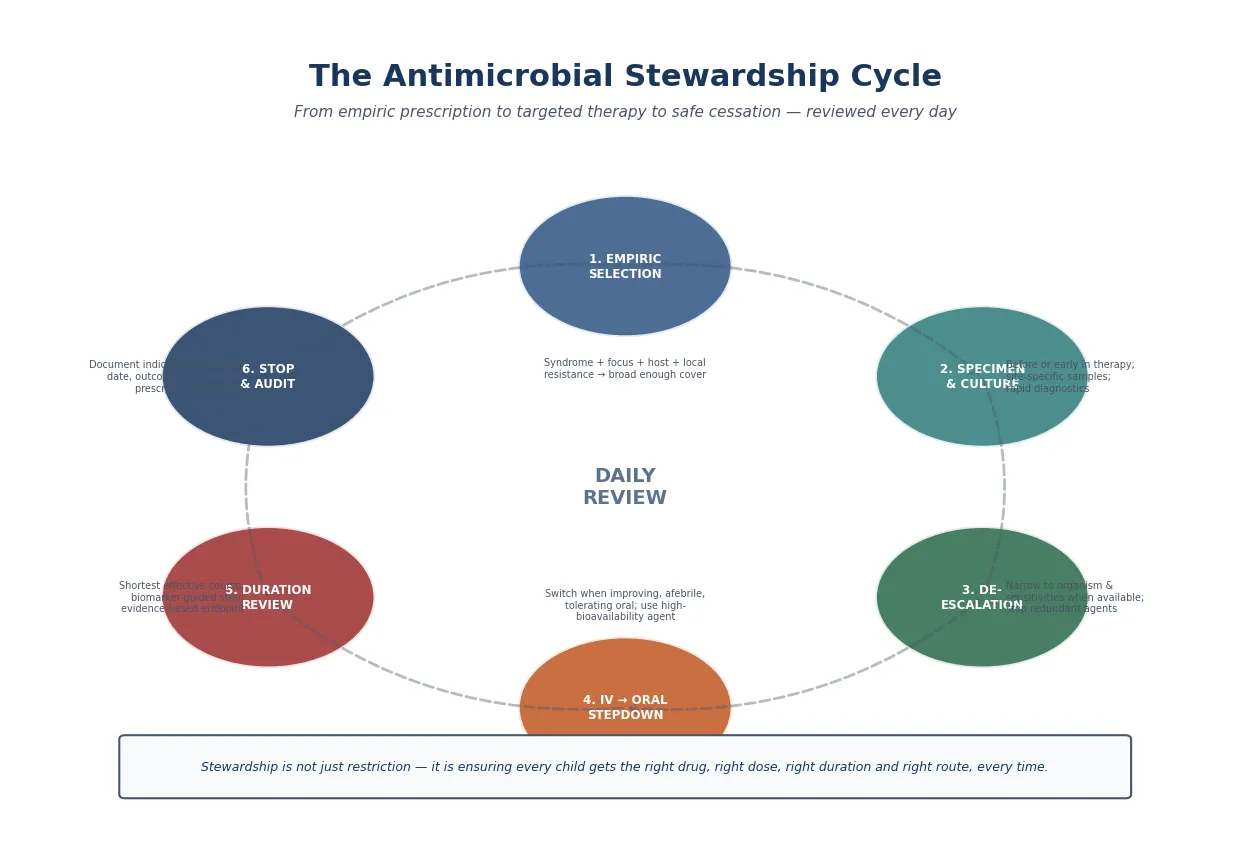
The four decisions at the heart of every antimicrobial prescription are the right drug (empiric then targeted, chosen by spectrum, tissue penetration, host factors, and local antibiogram), the right dose (weight-based, age-adjusted for developmental pharmacokinetics, with therapeutic drug monitoring where required), the right duration (the shortest course supported by evidence, with biomarker or clinical endpoints), and the right route (intravenous for severe illness, with early oral switch when the child improves). A fifth cross-cutting element — the stewardship cycle of daily review, audit, and feedback — binds the four together. [1] [2] [8]
From first prescription to safe cessation
1 · Select empirically
Cover the likely organism and focus narrowly, guided by host risk, immunisation status, and local resistance data. Use WHO Access antibiotics first-line where possible.
2 · Dose correctly
Calculate weight-based mg/kg, adjust for age and PK maturation, account for renal and hepatic function, and plan therapeutic drug monitoring where indicated.
3 · Specimen and review
Obtain cultures before or early in therapy. At 48–72 hours, review: is infection confirmed? Can the drug be narrowed? Is the child improving?
4 · De-escalate and switch
Narrow to the organism and sensitivities. Switch from IV to oral when the child is improving, afebrile, and tolerating oral. Use a high-bioavailability agent for stepdown.
5 · Set duration and stop
Prescribe the shortest evidence-based duration. Use a biomarker (CRP, procalcitonin) or clinical endpoint. Document the indication, start, stop, and outcome.
Classification
Antibiotics can be classified in three useful ways, and a candidate should hold all three simultaneously: by their pharmacodynamic killing pattern (which dictates the dosing strategy), by their spectrum and stewardship priority (the WHO AWaRe system), and by whether they are bactericidal or bacteriostatic (relevant in endocarditis, meningitis, and neutropenia). [2] [5]
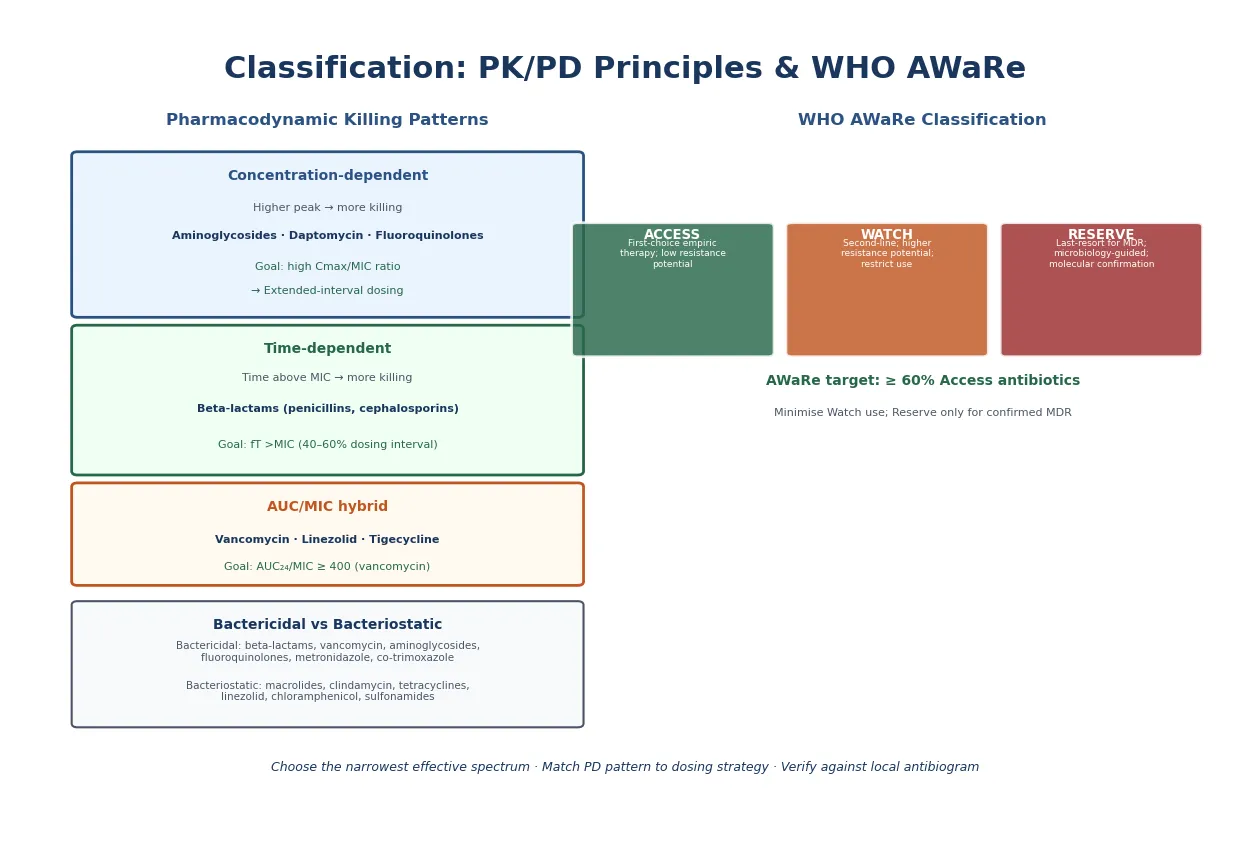
The pharmacodynamic pattern tells you how to dose. Concentration-dependent agents — aminoglycosides, daptomycin, fluoroquinolones — kill best when the peak concentration is high relative to the minimum inhibitory concentration (MIC), so they are given as large, infrequent doses to maximise the peak-to-MIC ratio while exploiting the post-antibiotic effect. Time-dependent agents — beta-lactams — kill best when the drug concentration stays above the MIC for a proportion of the dosing interval, so dosing is scheduled to keep levels above the MIC. AUC/MIC agents — vancomycin and linezolid — target the total drug exposure over 24 hours relative to the MIC. [3] [5] [6]
The WHO AWaRe system guides which drug to choose first. The Access group are first-choice empiric agents with a narrow spectrum and low resistance potential — amoxicillin, amoxicillin-clavulanate, ampicillin, gentamicin, and first-generation cephalosporins. The Watch group have higher resistance potential and should be restricted to specific indications — ciprofloxacin, azithromycin, vancomycin, and clindamycin. The Reserve group are last-resort agents for multidrug-resistant infections — colistin, linezolid, and newer beta-lactam combinations. A national or institutional target of at least 60 per cent Access antibiotic use is a common stewardship benchmark. [2] [8]
| Killing pattern | Representative agents | Dosing goal | Dosing consequence |
|---|---|---|---|
| Concentration-dependent | Aminoglycosides, daptomycin, fluoroquinolones | Maximise Cmax/MIC | High once-daily dose; extended interval |
| Time-dependent | Beta-lactams (penicillins, cephalosporins, carbapenems) | Time above MIC (40–60% interval) | Frequent dosing or continuous infusion |
| AUC/MIC | Vancomycin, linezolid, tigecycline | AUC₂₄/MIC ≥ 400 (vancomycin) | Area-under-curve-guided dosing and monitoring |
| Bactericidal vs bacteriostatic | Bactericidal: beta-lactams, vanco, aminoglycosides; bacteriostatic: macrolides, clindamycin, linezolid | Use bactericidal in endocarditis, meningitis, neutropenia | Not a dosing change but a selection principle |
Epidemiology & Risk Factors
Antimicrobial resistance is a growing threat to children worldwide, and the scale of the problem shapes every prescribing decision. Across low- and middle-income settings, a high proportion of childhood bloodstream infections are now caused by resistant organisms, and resistance limits the empiric choices available at the moment a sick child presents. Children in sub-Saharan Africa, South Asia, and the Pacific bear a disproportionate burden, but resistance is rising everywhere — including in high-income countries where broad-spectrum use in hospitals drives selection pressure. [9] [8]
Several factors place a child at particular risk of both receiving unnecessary antibiotics and of being infected by a resistant organism. Hospital exposure — especially to intensive care, surgical wards, and long inpatient stays — selects for healthcare-associated pathogens such as extended-spectrum beta-lactamase-producing Enterobacterales and methicillin-resistant Staphylococcus aureus. Immunocompromise from chemotherapy, transplant, or primary immunodeficiency broadens the empiric differential and often mandates broader initial cover. Prior antibiotic exposure within the preceding 90 days is one of the strongest predictors of a resistant organism. [9] [13]
Community-acquired
Previously well child
- Likely organisms from local epidemiology
- Narrow empiric Access-group cover often sufficient
- Lower baseline resistance risk
- Short course, early oral switch common
Healthcare-associated
Recent admission or device
- Resistant organisms more likely
- Prior antibiotic exposure shapes resistance
- Broader empiric cover may be needed
- De-escalate aggressively when cultures return
Immunocompromised
Neutropenia, transplant, CI
- Broad empiric cover from the outset
- Atypical and resistant organisms on differential
- Early infectious diseases input
- Therapeutic drug monitoring essential
Neonate
PK and resistance differ
- Age-adjusted dosing essential
- Maternal and perinatal organisms predominate
- Higher mortality from undertreatment
- Stewardship programs now evidence-supported
The driver of resistance at the population level is total antibiotic consumption, and children are among the highest consumers per head of population. Every unnecessary prescription — a viral upper respiratory infection given antibiotics, a course extended past its evidence-based endpoint, a broad-spectrum agent where a narrow one would do — contributes to selection pressure. Stewardship directly counters this by reducing unnecessary, overly broad, and overly long courses while preserving access to effective therapy for children who genuinely need it. [1] [9] [13]
Pathophysiology
Children are not small adults when it comes to handling drugs. Four pharmacokinetic processes — absorption, distribution, metabolism, and elimination — each change with age, and these developmental changes explain why the same mg/kg dose can be subtherapeutic in a two-year-old but toxic in a neonate. Understanding these shifts is the foundation of paediatric dosing. [15] [16]
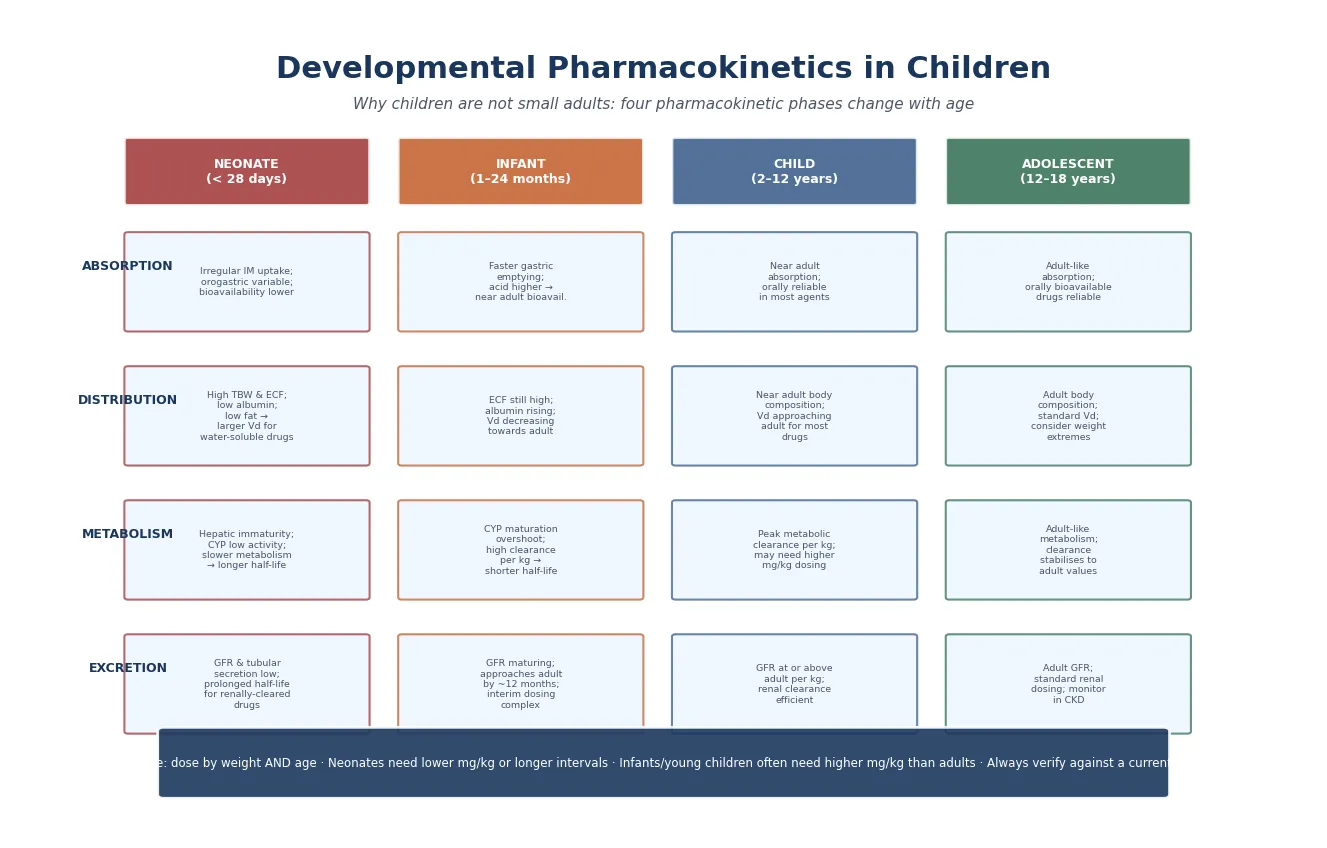
Absorption is variable in the neonate: intramuscular uptake is erratic, and oral bioavailability of some drugs is reduced by lower gastric acidity and irregular gastric emptying. By infancy, oral absorption approaches adult patterns for most agents, making oral therapy reliable for the improving child. Distribution changes with body composition: neonates have a high total body water and extracellular fluid volume relative to weight, which enlarges the volume of distribution for water-soluble drugs such as aminoglycosides and beta-lactams, meaning the same mg/kg dose produces a lower serum concentration. Albumin is lower in the neonate, altering the free fraction of highly protein-bound drugs. [15] [16]
Metabolism follows a biphasic maturation curve. At birth, hepatic enzyme systems — particularly the cytochrome P450 family — are immature, so metabolism is slow and half-lives are prolonged. During infancy and early childhood, enzyme activity per kilogram overshoots adult values, producing faster clearance and shorter half-lives; many children in this age group need higher mg/kg doses or shorter intervals than adults to achieve the same exposure. Elimination mirrors this pattern: glomerular filtration rate is low at birth, approaches adult values by roughly 8–12 months of age, and exceeds adult per-kg values during childhood before settling. [15] [16]
Clinical Presentation
The clinical presentation in antimicrobial stewardship is not a symptom complex but a prescribing decision: a child with a suspected infection needs an antimicrobial chosen, dosed, and reviewed. The clinical question at the bedside is whether antibiotics are needed at all, and if so, which drug, at what dose, by which route, and for how long. A viral upper respiratory infection with a red throat does not need antibiotics; a febrile neonate does. [1] [13]
Several bedside cues flag an antimicrobial decision worth scrutinising. A child started on broad empiric therapy who is improving at 72 hours should be reviewed for de-escalation. A child on intravenous therapy who is now afebrile, eating, and clinically improved is a candidate for oral switch. A child whose cultures are negative and whose inflammatory markers are falling may not need the full empiric course. Each of these moments is a stewardship intervention point. [1] [8]
The documented indication is the single most important stewardship safeguard. Before any antimicrobial is prescribed, the prescriber should state the suspected infection, the likely organism, the planned duration, and the review point. This forces a clinical reasoning step that prevents the reflexive continuation of therapy that drives resistance and harm. Every prescription without a clear indication is a red flag. [1] [13]
Differential Diagnosis
The differential in this context is the set of questions that separate an appropriate antimicrobial prescription from an inappropriate one. The clinician asks: is this infection bacterial, viral, or neither? Viral upper respiratory infections, viral exanthems, and self-limiting gastroenteritis are the conditions most commonly inappropriately treated with antibiotics in children. [1] [13]
When bacterial infection is plausible, the clinician narrows the question: what is the likely organism, and what is the focus? A community-acquired pneumonia in a vaccinated child points toward Streptococcus pneumoniae; a urinary tract infection in an infant suggests Escherichia coli; cellulitis suggests Streptococcus pyogenes or Staphylococcus aureus. The empiric drug should cover the likely organism with the narrowest effective spectrum. [2] [8]
The penicillin allergy label is a differential that demands active management rather than passive acceptance. Up to 10 per cent of children carry a reported penicillin allergy, but fewer than 5 per cent have a true IgE-mediated allergy when formally tested. Uncritical acceptance of the label drives the use of broader, more toxic alternatives — vancomycin, clindamycin, fluoroquinolones — which increase resistance, Clostridioides difficile risk, and cost. Structured allergy assessment, including risk-stratified oral challenge, can safely delabel the majority of children. [10] [11]
Clinical & Bedside Assessment
Bedside assessment of an antimicrobial prescription means examining the decision, not the child alone. The clinician asks five questions of every antimicrobial: Is there a clear indication? Is the drug the narrowest effective choice? Is the dose correct for this child's weight and age? Is the route appropriate? Is there a documented duration and review date? A prescription that cannot answer all five needs revision. [1] [13]
Weight-based dosing is the first step in getting the dose right, but weight alone is insufficient. The prescriber must also account for age (neonatal versus child dosing), renal function (reduce or extend interval for renally-cleared drugs when GFR is low), hepatic function, and body composition (use ideal or adjusted weight for obese children where relevant). A dose written without confirming the child's weight at the time of prescribing is a common source of error. [15] [16]
| Drug | Why monitor | Target | Key caution |
|---|---|---|---|
| Vancomycin | AUC₂₄/MIC ≥ 400 for serious MRSA; narrow therapeutic window | AUC-guided; or trough in some protocols | Nephrotoxicity; augmented clearance in PICU |
| Aminoglycosides (gentamicin, tobramycin, amikacin) | Concentration-dependent; narrow window; oto- and nephrotoxicity | High peak; low or undetectable trough | Extended-interval dosing; individualised in neonates |
| Beta-lactams (selected) | Severe infection, augmented clearance, PK/PD target attainment | Free drug above MIC for 40–60% of interval | May need continuous infusion in critical illness |
Penicillin allergy assessment is a stewardship act that happens at the bedside. Ask about the original reaction, the timing, the time since the last exposure, and whether the child has tolerated other beta-lactams. A low-risk history (rash without features of IgE-mediated allergy, remote reaction, or a family history only) makes direct oral challenge appropriate in many settings, and the PALACE trial showed this is safe for the majority of low-risk patients. Delabeling restores first-line beta-lactam access and narrows future empiric therapy. [10] [11]
Investigations
Investigations in antimicrobial stewardship serve two purposes: to confirm whether infection is present, and to identify the organism so therapy can be narrowed. Microbiology before or early in therapy is the cornerstone. Draw blood cultures, obtain urine (by catheter or clean catch, not bag), collect cerebrospinal fluid when safe and indicated, and swab or aspirate focal collections. The specimens taken at the start of therapy determine whether de-escalation will be possible 48 hours later. [1] [8]
Rapid diagnostics have transformed the pace of de-escalation. Molecular panels on CSF, blood, and respiratory samples can identify an organism and key resistance genes within hours, allowing earlier narrowing than conventional culture. Blood cultures remain essential because they provide the organism for full susceptibility testing and because molecular panels detect only the resistance genes they are designed for. A culture-negative, clinically well child with falling inflammatory markers may not need continued empiric therapy. [1] [8]
START — a stewardship check before every prescription
Inflammatory and infection biomarkers support stewardship decisions but do not replace clinical judgement. C-reactive protein trends help track response and support the decision to stop. Procalcitonin has been studied for guiding antibiotic initiation and discontinuation in acute respiratory tract infections, and a Cochrane review found that procalcitonin-guided protocols reduced antibiotic exposure without increasing adverse outcomes in that context — though results should be applied to children with caution and alongside clinical assessment, not as a standalone rule. [14]
Management — Resuscitation
In the acutely septic child, the first antimicrobial decision is timing, not choice: give a broad-spectrum, weight-based antibiotic within one hour of recognising sepsis. The Surviving Sepsis Campaign 2026 children's guideline reinforces empiric antimicrobial therapy within the first hour for septic shock or sepsis-associated organ dysfunction. De-escalation, not the initial breadth, is what the stewardship program addresses later. [17] [1]
The empiric regimen is chosen by the syndrome, focus, host risk, and local resistance patterns. For a previously well child with community-acquired sepsis, a third-generation cephalosporin is a common first-line agent, with vancomycin added when resistant organisms or central nervous system involvement are suspected. For a neonate, a beta-lactam plus an aminoglycoside guided by neonatal sepsis protocols is standard. For an immunocompromised child, broad anti-pseudomonal cover is essential from the outset. [17] [8]
Empiric dosing principles (verify against current local formulary)
Therapeutic drug monitoring is essential for vancomycin and aminoglycosides from the first dose in serious infections. Vancomycin monitoring has shifted toward area-under-the-curve targeting (AUC₂₄/MIC of 400 or more for serious MRSA infection) rather than trough-only strategies, because AUC monitoring better predicts efficacy while reducing nephrotoxicity. Critically ill children — especially those in PICU — often have augmented renal clearance, which can produce unexpectedly low vancomycin levels on standard dosing and demand higher or more frequent administration. [3] [12]
Aminoglycoside dosing illustrates how pharmacodynamic principles shape practice. Because aminoglycosides are concentration-dependent with a significant post-antibiotic effect, extended-interval (once-daily) dosing maximises the peak concentration, minimises accumulation, and appears to reduce nephrotoxicity. Meta-analyses in both neonates and older children have confirmed that extended-interval dosing is as effective as traditional multiple-daily dosing with no increase in toxicity, though neonatal dosing intervals are individualised by gestational and postnatal age. [4] [5] [6]
Management — Definitive & Stepwise
Definitive antimicrobial therapy means converting a broad empiric choice into targeted treatment as the organism and clinical response become clear. De-escalation — narrowing from the empiric regimen to the narrowest effective agent once sensitivities are known — is the central stewardship move in this phase. The evidence is consistent: de-escalation does not worsen outcomes and reduces resistance selection, adverse effects, and cost. [1] [8]
The IV-to-oral switch is one of the highest-value stewardship interventions. A child who is improving, afebrile for 24–48 hours, tolerating oral intake, and has an oral agent with good bioavailability available can safely switch from intravenous to oral therapy. Beta-lactams such as amoxicillin, amoxicillin-clavulanate, cefalexin, clindamycin, fluoroquinolones, co-trimoxazole, metronidazole, and linezolid have oral bioavailability approaching their intravenous equivalents, making oral stepdown a pharmacologically sound decision. This switch reduces line complications, shortens hospital stay, and returns the child to normal activity sooner. [1] [8]
Duration is the stewardship decision that has changed most in recent years. Across a range of common paediatric infections — community-acquired pneumonia, urinary tract infection, intra-abdominal infection, and skin and soft tissue infection — shorter courses have proven as effective as longer ones. The principle is to prescribe the shortest evidence-based duration, set a clear stop date at the time of prescribing, and review the child at that point. Biomarker-guided discontinuation, particularly with procalcitonin in respiratory infection, can further shorten therapy when integrated into a protocol. [1] [14]
Specific Subtypes & Scenarios
The neonate is the population where developmental pharmacokinetics matters most and where stewardship programs are now evidence-supported. A 2024 meta-analysis of antimicrobial stewardship programs in neonates found that stewardship interventions reduced antibiotic use without increasing adverse outcomes. Neonatal dosing demands age-adjusted intervals for aminoglycosides and beta-lactams because GFR and hepatic enzyme activity are immature; using older-child or adult dosing intervals in a neonate risks accumulation and toxicity. The empiric regimen covers organisms shaped by maternal and perinatal risk — Group B Streptococcus, E. coli, and Listeria monocytogenes in early-onset sepsis, and coagulase-negative staphylococci in late-onset device-associated sepsis. [7] [8] [15]
The immunocompromised child — neutropenic from chemotherapy, post-transplant, or carrying a primary immunodeficiency — needs empiric broad-spectrum cover that includes Pseudomonas aeruginosa, and the regimen is broadened by the clinical context. De-escalation in this population requires coordination with the oncology, transplant, or immunology team, because the differential includes atypical and resistant organisms. Therapeutic drug monitoring for vancomycin and aminoglycosides is essential because augmented clearance and shifting renal function are common. [9] [12]
The stewardship timeline for a sick child
The child with cystic fibrosis or chronic suppressive antibiotic needs represents a specialised stewardship challenge. These children need repeated courses of targeted antipseudomonal therapy, and their regimens are shaped by their individual sputum microbiology, prior antibiotic exposure, and lung function trajectory. Stewardship here is individualised — not a restriction of necessary therapy, but a structured approach to getting the right drug, at the right dose, for the right duration in a child whose microbiology is well characterised. [9] [13]
Complications & Pitfalls
The complications of antimicrobial therapy extend beyond the individual child's adverse drug reaction. At the patient level, antibiotics cause gastrointestinal upset, allergic reactions, C. difficile infection, nephrotoxicity (vancomycin, aminoglycosides), hepatotoxicity, and QT prolongation (macrolides, fluoroquinolones). At the population level, unnecessary and overly broad use drives antimicrobial resistance, lengthening hospital stays and narrowing future treatment options. [1] [9]
Three common pitfalls undermine stewardship at the bedside. Prescribing without a documented indication is the foundational failure — a prescription started reflexively, without a clear clinical reason or planned endpoint, tends to be continued indefinitely out of inertia. Failing to de-escalate when cultures return keeps children on broader-than-necessary therapy, driving resistance and adverse effects. Overlong durations, driven by habit or a desire for certainty, expose children to harm without clinical benefit when evidence supports a shorter course. [1] [13]
Select
- Narrowest effective empiric spectrum
- WHO Access first, Watch second-line
- Guided by focus, host, local resistance
- Penicillin allergy: assess and delabel
Dose
- Weight-based mg/kg
- Age-adjusted for developmental PK
- TDM for vancomycin (AUC) and aminoglycosides
- Renal/hepatic adjustment
Review
- Documented indication and duration
- De-escalate at 48–72 h
- IV-to-oral switch when improving
- Shortest evidence-based course
PK/PD
- Concentration-dependent → once daily (aminoglycosides)
- Time-dependent → keep above MIC (beta-lactams)
- AUC/MIC → vancomycin target
- Bactericidal for endocarditis, meningitis, neutropenia
Pitfalls
- No documented indication
- Empiric breadth becomes maintenance
- Wrong dose for age/weight
- Overlong course
“Right drug (Access-first, de-escalate) → right dose (weight- and age-based, TDM where needed) → right duration (shortest evidence-based) → right route (early oral switch) → daily review, audit, feedback.”
A communication pitfall is the unreviewed prescription at the transition of care. A child transferred from the emergency department to the ward, or from a referring hospital to a tertiary centre, may carry an empiric regimen that no one has revisited. Structured medication reconciliation at every handover — with explicit review of indication, culture results, and the plan to de-escalate, switch, or stop — prevents the silent continuation of unnecessary therapy. [1] [8]
Prognosis & Disposition
The prognosis of an antimicrobial decision depends on whether the right drug reaches the right site at the right concentration for the right duration. A child who receives timely, appropriate, weight-based empiric therapy for a serious bacterial infection, followed by de-escalation to a targeted oral agent and an evidence-based total duration, has the best chance of cure with the least collateral harm. Stewardship directly improves this outcome by ensuring that appropriate therapy is neither delayed nor needlessly prolonged. [1] [8]
Disposition decisions are intertwined with the route. A child who has been switched to oral therapy, is clinically improving, and has reliable follow-up can complete treatment at home — shortening hospital stay, reducing line-associated complications, and returning the child to normal activity. The child who remains unwell, cannot tolerate oral intake, or has a deep-seated infection requiring prolonged intravenous therapy may need continued inpatient or outpatient parenteral management. [1] [8]
The long-term prognosis of effective stewardship extends beyond the individual child. By preserving the efficacy of existing antimicrobials, stewardship protects future patients — including the child in front of you if they return with another infection. Resistance is cumulative and intergenerational; every unnecessary prescription today narrows the options for a sick child tomorrow. [9] [13]
Special Populations
The neonate requires age-adjusted dosing as a core safety measure, not an optional refinement. GFR is low at birth and rises through infancy; hepatic enzyme activity is immature in the first weeks of life. Standard mg/kg doses given at standard intervals designed for older children will accumulate and cause toxicity. Neonatal stewardship programs, supported by the 2024 meta-analysis evidence, focus on reducing unnecessary exposure — particularly for suspected-but-unconfirmed early-onset sepsis — while preserving prompt appropriate treatment. The neonatal empiric regimen is chosen from the maternal and perinatal risk profile and adjusted for gestational and postnatal age. [7] [15]
The immunocompromised child needs empiric broad-spectrum cover at first presentation, because the differential includes resistant and atypical organisms. Stewardship in this population is not about narrowing the initial regimen, which must be broad, but about daily review, de-escalation as cultures return, and therapeutic drug monitoring. The oncology, transplant, or immunology team shapes the empiric regimen and the de-escalation plan. The child with febrile neutropenia is a paradigm: broad empiric cover from the outset, with early oral stepdown for low-risk children and de-escalation guided by the culture results. [9] [13]
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne Antibiotic guidelines and Therapeutic Guidelines (eTG) Antibiotic are the primary empiric prescribing references, supported by the Australian Commission on Safety and Quality in Health Care antimicrobial stewardship clinical care standard. The annual AURA surveillance report tracks resistance and prescribing patterns. State and territory formularies and antimicrobial restriction policies vary and must be checked against the current local source. [1] [2]
Global and low-resource settings: the WHO AWaRe framework and the WHO Model List of Essential Medicines for Children are the primary tools for standardising empiric selection, especially where local antibiograms are unavailable. Antimicrobial resistance among children in low-resource settings is a major driver of mortality, and stewardship — including reducing unnecessary use, standardising empiric therapy, and ensuring access to effective Access-group antibiotics — is a global health priority. The Global Action Plan on AMR frames stewardship within a One Health approach. [2] [9]
Evidence, Guidelines & Regional Differences
The evidence base for antimicrobial stewardship in children has matured significantly. The IDSA/SHEA guidelines established the framework for hospital stewardship programs — prospective audit with feedback, formulary restrictions, and education — and these elements translate directly to paediatric practice. A growing body of evidence supports shorter courses across common paediatric infections, and meta-analyses have confirmed the safety and efficacy of extended-interval aminoglycoside dosing and neonatal stewardship programs. [1] [4] [7]
The pharmacodynamic dosing principles that underpin modern dosing strategies — concentration-dependent, time-dependent, and AUC/MIC — have shifted vancomycin monitoring from trough-only to AUC-guided strategies, supported by the 2020 consensus guideline from ASHP, IDSA, PIDS, and SIDP. Critically ill children with augmented renal clearance present a particular challenge: standard vancomycin doses may produce subtherapeutic levels, and population pharmacokinetic models are informing individualised dosing. [3] [12]
The procalcitonin evidence is nuanced. The Cochrane review of procalcitonin-guided antibiotic initiation and discontinuation in acute respiratory tract infections found reduced antibiotic exposure without increased adverse outcomes, but this evidence is strongest in adult populations and must be applied to children with clinical judgement. Biomarkers support — but do not replace — the clinician's assessment of whether a child is improving. [14]
Board and assessment distinctions
RACP current PREP curriculum candidates in 2026 must apply safe prescribing and antimicrobial stewardship within acute and general paediatric learning objectives, while first-year trainees from 2027 encounter stewardship under quality and safety goals. RCPCH Progress+ embeds safe prescribing and patient safety as core outcomes. The ABP General Pediatrics Content Outline covers infectious diseases and pharmacology as distinct domains, while ACGME milestones include antimicrobial stewardship as a systems-based practice. [1] [13]
| Board or format | What the candidate must demonstrate |
|---|---|
| RACP DWE | Interpret a vignette and choose the correct empiric drug, dose, or stewardship action |
| RACP DCE long case | Integrate host risk, focus, local resistance, dosing, and a full stewardship plan for a complex child |
| MRCPCH clinical | Explain the stewardship decision to a family and demonstrate safe prescribing reasoning |
| ABP | Apply pharmacology and infectious-disease domains to select, dose, and review an antimicrobial |
| RCPSC structured oral | Defend an empiric-to-targeted antimicrobial plan across age groups and settings |
Exam Pearls
Viva: why do we dose aminoglycosides once daily in children?
Aminoglycosides are concentration-dependent killers: the higher the peak relative to the MIC, the more effective the kill. They also exhibit a post-antibiotic effect, meaning bacterial suppression continues after the drug level falls below the MIC. Once-daily dosing maximises the peak, exploits the post-antibiotic effect, and minimises renal accumulation. Meta-analyses in neonates and older children confirm that extended-interval dosing is as effective as traditional dosing with no increase in nephro- or ototoxicity, though neonatal intervals are individualised by gestational and postnatal age. [4] [5] [6]
Structured oral: the child with a penicillin allergy label
Do not accept the label uncritically. Take a structured allergy history: what was the reaction, when did it occur, how was it managed, and has the child tolerated other beta-lactams? A low-risk history (non-IgE rash, remote reaction, family history only) supports risk-stratified oral challenge — the PALACE trial showed this is safe in the majority. Delabeling restores first-line beta-lactam access, narrows empiric therapy, reduces resistance, and lowers cost. If the history suggests true IgE-mediated allergy, use an alternative agent and arrange formal allergy referral. [10] [11]
References
- [1]Barlam, Tamar F; Cosgrove, Sara E; Abbo, Lilian M Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 2016.PMID 27080992
- [2]Moja, Lorenzo; Zanichelli, Valeria; Mertz, Didier WHO's essential medicines and AWaRe: recommendations on first- and second-choice antibiotics for empiric treatment of clinical infections. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases, 2024.PMID 38342438
- [3]Rybak, Michael J; Le, Jennifer; Lodise, Thomas P Therapeutic Monitoring of Vancomycin for Serious Methicillin-resistant Staphylococcus aureus Infections: A Revised Consensus Guideline and Review. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 2020.PMID 32658968
- [4]Nestaas, Erik; Bangstad, Hans-Jacob; Sandvik, Leiv Aminoglycoside extended interval dosing in neonates is safe and effective: a meta-analysis. Archives of disease in childhood Fetal and neonatal edition, 2005.PMID 15857879
- [5]Contopoulos-Ioannidis, Despina G; Giotis, Nikolaos D; Baliatsa, Dimitra V Extended-interval aminoglycoside administration for children: a meta-analysis. Pediatrics, 2004.PMID 15231982
- [6]Jenh, Anna M; Tamma, Pranita D; Milstone, Aaron M Extended-interval aminoglycoside dosing in pediatrics. The Pediatric infectious disease journal, 2011.PMID 21407038
- [7]Mascarenhas, Darren; Ho, Mona S P; Ting, John Antimicrobial Stewardship Programs in Neonates: A Meta-Analysis. Pediatrics, 2024.PMID 38766702
- [8]Bielicki, Julia; Lundin, Rebecca; Patel, Sanjay Antimicrobial stewardship for neonates and children: a global approach. The Pediatric infectious disease journal, 2015.PMID 25584443
- [9]Williams, Philip C M; Isaacs, David; Berkley, James A Antimicrobial resistance among children in sub-Saharan Africa. The Lancet infectious diseases, 2018.PMID 29033034
- [10]Vyles, David; Antoon, James W; Norton, Allison Children with reported penicillin allergy: Public health impact and safety of delabeling. Annals of allergy, asthma & immunology : official publication of the American College of Allergy, Asthma, & Immunology, 2020.PMID 32224207
- [11]Copaescu, Ana M; Vogrin, Senjuti; James, Frances Efficacy of a Clinical Decision Rule to Enable Direct Oral Challenge in Patients With Low-Risk Penicillin Allergy: The PALACE Randomized Clinical Trial. JAMA internal medicine, 2023.PMID 37459086
- [12]He, Chen-Yu; Ye, Pei-Pei; Liu, Bo Population Pharmacokinetics and Dosing Optimization of Vancomycin in Infants, Children, and Adolescents with Augmented Renal Clearance. Antimicrobial agents and chemotherapy, 2021.PMID 34339268
- [13]Hersh, Adam L; Beekmann, Susan E; Polgreen, Philip M Antimicrobial stewardship programs in pediatrics. Infection control and hospital epidemiology, 2009.PMID 19852666
- [14]Schuetz, Philipp; Wirz, Yannick; Sager, Roland Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Evidence-based child health : a Cochrane review journal, 2017.PMID 29025194
- [15]Pineda, Lina C; Watt, Kelly M New antibiotic dosing in infants. Clinics in perinatology, 2015.PMID 25678003
- [16]Zhao, Wei; Leroux, Sebastien; Jacqz-Aigrain, Evelyne Dosage individualization in children: integration of pharmacometrics in clinical practice. World journal of pediatrics : WJP, 2014.PMID 25124969
- [17]Weiss, Scott L; Peters, Mark J; Oczkowski, Stephen J W Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2026.PMID 41869844