Paeds · infectious-diseases
Bacteraemia and occult bloodstream infection
Also known as Bloodstream infection · Occult bacteraemia · Positive blood culture · Invasive bacterial infection · Fever without source · Serious bacterial infection
An age-, appearance- and immunity-aware fellowship approach to bacteraemia and occult bloodstream infection in children: how viable bacteria in the blood present from the febrile young infant through the older child, how to risk-stratify and investigate, how to resuscitate the septic child, when to give empiric antibiotics, and how conjugate vaccines have reshaped the whole question.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a 14-month-old brought in with two days of fever to 39.5 °C. She is alert, smiling, drinks from her cup, has a clear chest, no rash and no obvious focus. In the pre-pneumococcal-vaccine era, between roughly three and nine of every hundred children just like her had bacteria circulating in their bloodstream, and the worry was that pneumococcus might settle in her meninges before anyone realised. Today that number is a fraction of one per cent. The child has not changed; the population risk has. That shift is the single most important idea on this topic. [1] [9]
Bacteraemia is the presence of viable bacteria in the bloodstream, confirmed when a blood culture grows a pathogen. The word describes a laboratory and physiological fact, not a syndrome. A febrile child with bacteraemia may be in septic shock, may have an obvious pneumonia, or may look completely well — the same finding spans the whole spectrum of severity. [1] [12]
Occult bacteraemia is the historical name for the child at the well end of that spectrum: fever without an apparent focus in a child who does not look toxic, where bacteraemia is found only because a blood culture was drawn. It was a clinical problem worth chasing in the 1990s because occult pneumococcal bacteraemia carried a real risk of meningitis if the child was sent home untreated. With pneumococcal and Haemophilus influenzae type b conjugate vaccines, the prevalence fell so far that the question reframed: clinicians now ask whether the febrile child is at risk of a serious or invasive bacterial infection, and use validated pathways to decide who needs investigation and empiric treatment. [1] [3] [9]
Why the modern numbers reframe the question
Classification
Sort a bloodstream finding along three independent axes. First, separate a true pathogen from a contaminant: a single bottle growing coagulase-negative staphylococci, diphtheroids or bacillus in a well child is usually skin flora introduced at sampling, whereas growth of Streptococcus pneumoniae, Neisseria meningitidis, Staphylococcus aureus, Escherichia coli, group B streptococcus or Salmonella is a pathogen until proven otherwise. Second, separate apparent from occult by how the child looks. Third, separate transient bacteraemia (a brief seed after a mucosal breach, usually cleared) from continuous or persistent bacteraemia (an undrained deep focus, endovascular source or device infection that keeps seeding and demands source control). [1] [10]
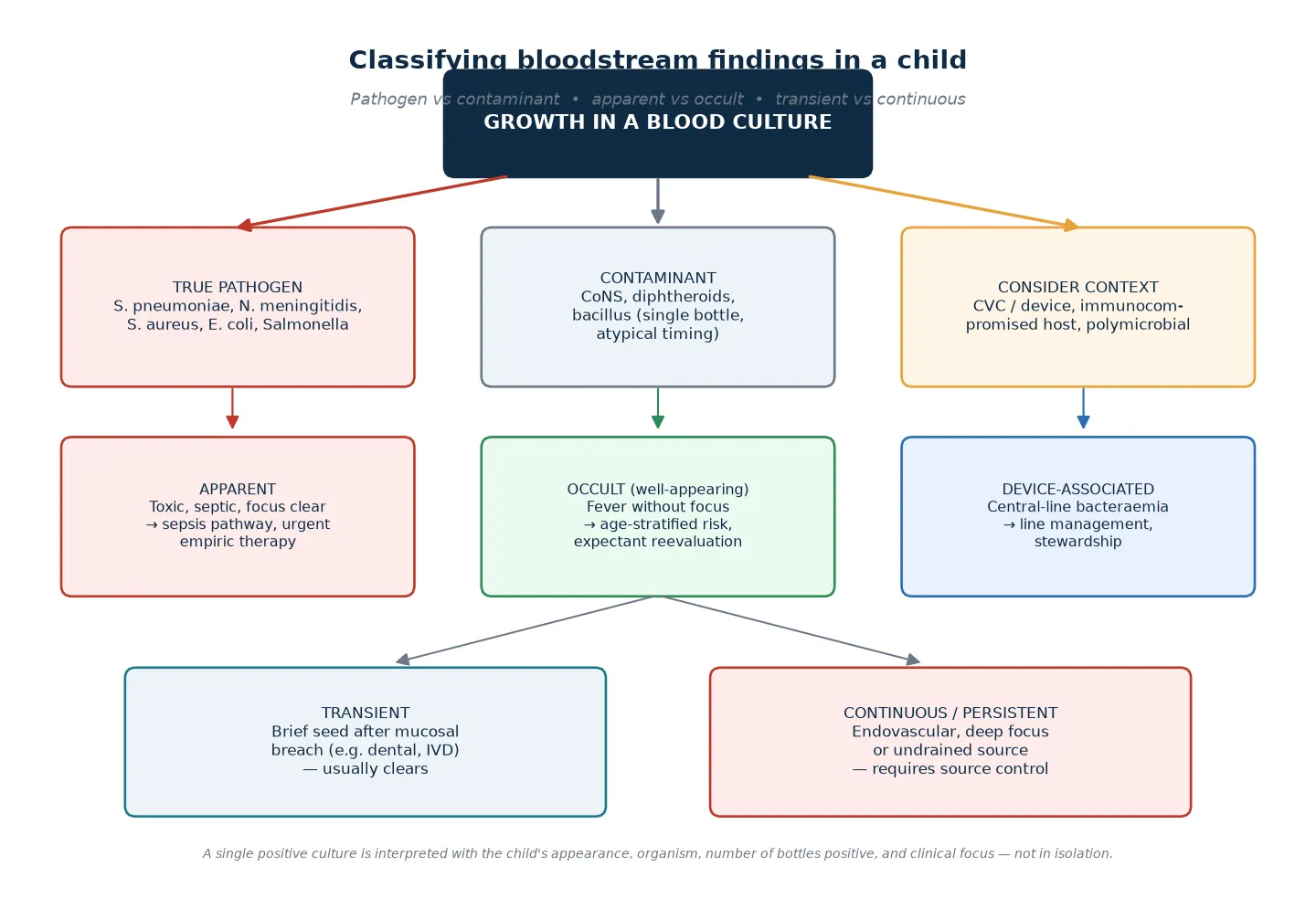
A device-associated bloodstream infection sits in its own category. A child with a central venous catheter, whether for oncology, intestinal failure or complex chronic disease, can develop a true line infection with an organism that would be a contaminant in anyone else. Coagulase-negative staphylococci growing in two bottles of a febrile neutropenic child with a line is a central-line-associated bloodstream infection until the line and the child are assessed together. [10]
True pathogen
Act on it
- S. pneumoniae, N. meningitidis, S. aureus, E. coli, GBS, Salmonella
- Usually recovered from appropriately collected cultures
- Drives empiric and directed therapy, source control and follow-up
- Polymicrobial or unusual organisms raise the question of a deep focus, device or immunocompromise
Contaminant
Question it
- Coagulase-negative staphylococci, diphtheroids, bacillus, Micrococcus
- Often a single bottle, delayed growth, atypical timing
- Reassess the child; repeat only if clinical concern persists
- Over-treating contaminants causes line loss, resistance and harm
Device-associated
Assess line and host together
- Central venous catheter, ventricular shunt, peritoneal dialysis
- Organism interpreted in the host context
- May require line salvage, lock therapy or removal
- Stewardship and infection-prevention bundle apply
Epidemiology & Risk Factors
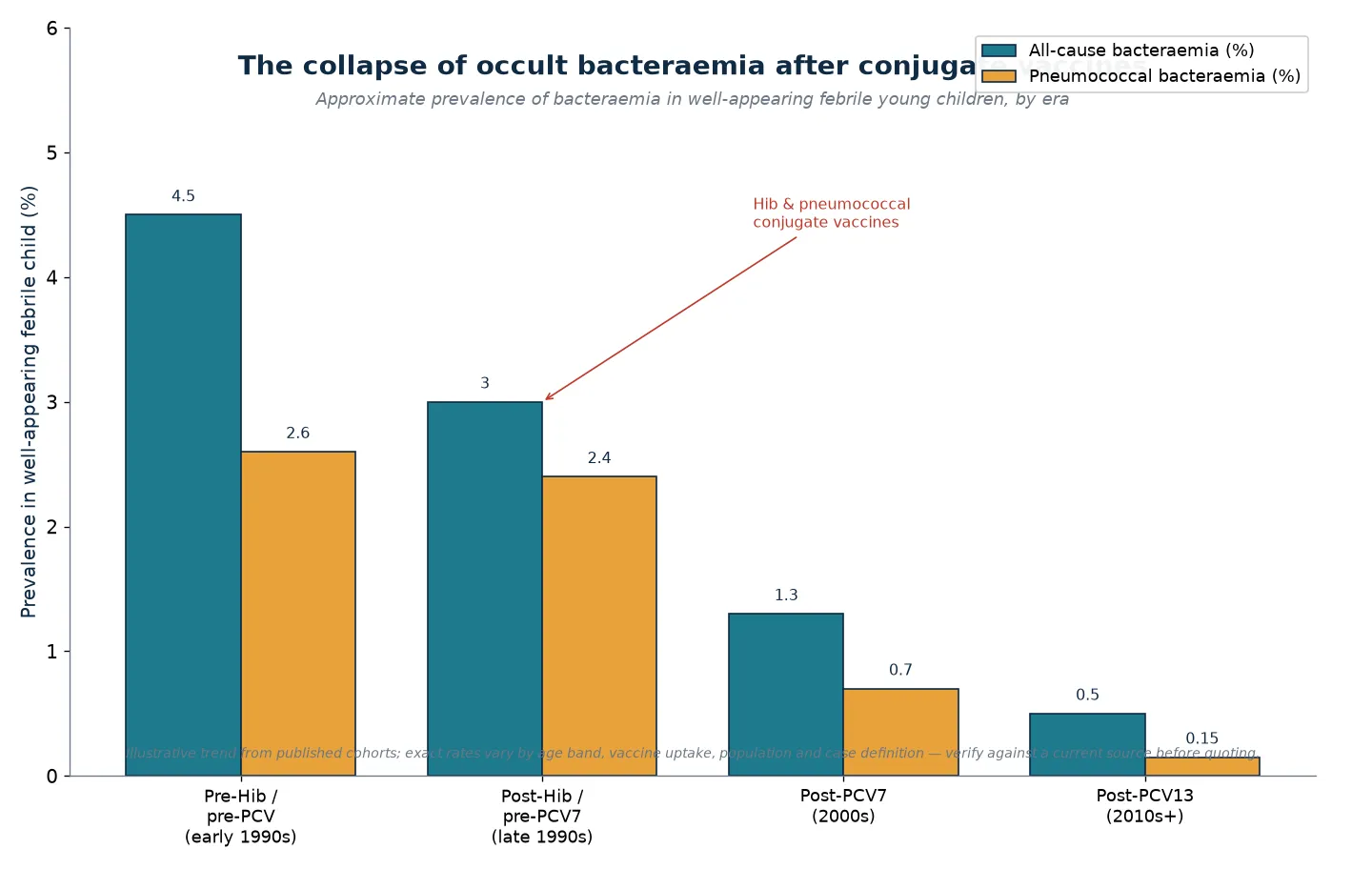
The epidemiology of paediatric bacteraemia cannot be stated as one number because it has been transformed by immunisation. Before conjugate vaccines, occult bacteraemia in well-appearing febrile young children was common enough to justify routine blood cultures and expectant antibiotics, and Streptococcus pneumoniae and Haemophilus influenzae type b dominated. After sequential introduction of Hib, then seven-valent and thirteen-valent pneumococcal conjugate vaccines, the prevalence of occult bacteraemia in vaccinated populations fell below one per cent, and pneumococcal meningitis fell with it. [1] [9]
What did not disappear is the age-related risk of the febrile young infant. Neonates and infants in the first two to three months of life carry a substantially higher risk of invasive bacterial infection than older children, driven by immature neutrophil and complement function and by organisms such as group B streptococcus and E. coli. This is why every modern febrile-infant pathway anchors on age, and why the highest-yield clinical question on this topic is usually about a baby under two months old rather than a toddler. [2] [3]
Child factors
- Young age, especially the febrile neonate and infant under 60 days
- Incomplete or no immunisation against pneumococcus, Hib or meningococcus
- Fever without focus and high fever above 39 °C in the young child
- Functional or anatomical asplenia, including sickle cell disease
- Congenital or acquired immunodeficiency, neutropenia, malignancy
Device and exposure factors
- Indwelling central venous catheter, ventricular shunt or peritoneal dialysis
- Recent surgery, invasive procedure or healthcare exposure
- Close contact with meningococcal or invasive bacterial disease
- Outbreak or seasonal surge of respiratory virus or invasive bacterial disease
- Travel to a region with higher prevalence of vaccine-preventable disease
System and social factors
- Vaccine access barriers, late or incomplete immunisation
- Rural or remote location with delayed access to definitive care
- Language, health-literacy and follow-up barriers that impair safety-netting
- Household crowding and socioeconomic disadvantage
- Reliable caregiver concern that the child is not their usual self
A febrile infant with a documented viral infection is not automatically protected from bacterial coinfection. A large Pediatric Emergency Care Applied Research Network cohort showed that febrile infants sixty days and younger with documented viral infections still carry a measurable risk of serious and invasive bacterial coinfection, highest with influenza and lower but not zero with respiratory syncytial virus. A positive viral test therefore lowers, but does not eliminate, the need to consider invasive bacterial infection. [4]
Pathophysiology
Bacteraemia begins when bacteria cross a mucosal or skin barrier into the bloodstream. Most seeds are transient and cleared by reticuloendothelial and neutrophil defences within minutes; the child never becomes unwell and the episode is never detected. Disease happens when the inoculum is large, the organism is virulent, or the host cannot clear it, so that bacteria persist, multiply or settle in a distant sterile site. [1] [12]
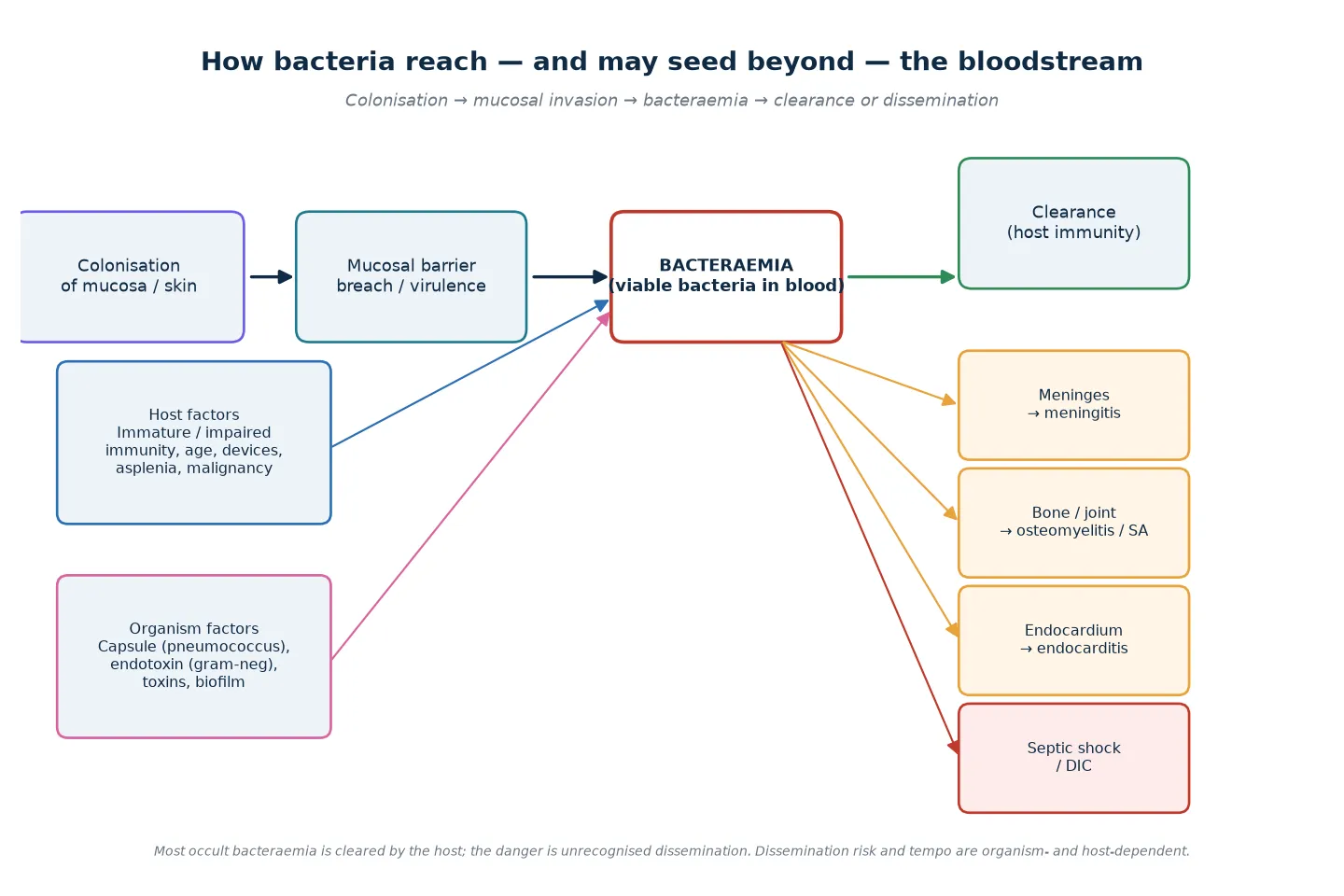
Encapsulation is the key virulence theme. Streptococcus pneumoniae, Haemophilus influenzae type b and Neisseria meningitidis resist phagocytosis unless they are first opsonised by antibody and complement. Infants rely on transplacentally acquired antibody that wanes through the first months of life, and children without a functional spleen cannot clear encapsulated organisms once they enter the blood. This is why conjugate vaccines — which convert a T-independent response into a memory response in infants — changed the epidemiology so dramatically, and why asplenic and hyposplenic children remain vulnerable despite vaccination. [9] [12]
Host immunity matures with age, and this is the physiological basis for age-stratified pathways. Neonates and young infants have quantitative and qualitative neutrophil immaturity, reduced bone-marrow reserve, and an alternative complement pathway that is less efficient, so a small bacterial seed can overwhelm them. They may also mount a blunted inflammatory response, producing the afebrile or hypothermic septic neonate — the absence of fever never excludes invasive infection in this age group. [2] [12]
The downstream harm of bacteraemia depends on where bacteria settle and how the host responds. Streptococcus pneumoniae that breaches the blood–brain barrier causes pneumococcal meningitis; Staphylococcus aureus seeds bone, joint and endocardium; Neisseria meningitidis drives rapid meningococcaemia with purpura, adrenal haemorrhage and shock; gram-negative endotoxin produces the vasodilatory, warm-then-cold distributive shock of sepsis. Recognising dissemination is the clinical task; understanding the mechanism tells you why some organisms demand empirical coverage before culture results return. [1] [12]
Clinical Presentation
The presentation of bacteraemia spans two extremes joined by every shade in between. At one end is the toxic, septic child: ill-looking, tachycardic, with cool or mottled peripheries, prolonged capillary refill, altered interaction and often a high — or, in the neonate, low — temperature. This child is in trouble now and the blood culture is almost an afterthought to resuscitation. At the other end is the well-appearing febrile child with no focus, the classic occult-bacteraemia presentation, where the only clue to possible bloodstream infection is the decision to draw a culture. [1] [12]
The neonate and young infant deserves its own sentence because the usual cues fail. Fever may be absent; instead the baby is hypothermic, irritable, lethargic, feeding poorly, grunting, or has apnoea, a bulging or full fontanelle, or just a caregiver report that the child is not right. Temperature instability and feeding difficulty are as significant as fever in this age group, and a hypothermic, hypotonic neonate is septic until the work-up says otherwise. [2] [3]
A petechial or purpuric rash in a febrile child is meningococcaemia until proven otherwise and bypasses all the careful risk-stratification below: this child needs immediate antibiotics and resuscitation. A rapidly evolving rash with shock, altered consciousness or a rising ferritin-like picture must be treated as time-critical invasive bacterial disease while the work-up proceeds. [1] [12]
| Life stage | Presentation clues that matter | Assessment adaptation |
|---|---|---|
| Neonate and infant under 60 days | Hypothermia, poor feeding, irritability, apnoea, grunting, bulging fontanelle; fever may be absent | Treat as higher pre-test risk; use age-stratified febrile infant pathway; do not be reassured by a normal temperature |
| Older infant and toddler | Fever without focus, reduced play and intake, altered interaction; toxic appearance is the key discriminator | Assess appearance carefully; reserve blood culture and inflammatory markers for higher-risk children |
| School-age child | Focal pain, rash, rigors, unwell appearance; the focus is more often identifiable | Examine for focus; culture guided by appearance and the suspected source |
| Adolescent | Rigors, petechiae, meningism, collapse; consider meningococcal risk and confidential history | Include substance use, sexual health and mental state; do not apply adult thresholds uncritically |
| Immunocompromised or line-bearing child | May be afebrile or febrile with blunted signs; fever in neutropenia is an emergency | Assess the line and the host; empirical broad-spectrum therapy early; do not wait for toxicity |
The Yale Observation Scale was the formal tool built to grade how a febrile child looks, scoring quality of cry, reaction to parents, state variation, colour and hydration. Its core insight survives in modern practice even as the score itself has been overtaken: an abnormal appearance — whatever scale or gestalt you use — substantially raises the probability of serious and invasive bacterial infection, while a well-appearing child lowers but never abolishes it. The appearance assessment is the single most powerful bedside variable on this topic, and it should be stated explicitly in the notes, not buried in "looks well". [1]
Differential Diagnosis
When you encounter possible bacteraemia, the differential operates on two levels: the differential of the fever itself, and the differential of a positive culture once it returns. Fever without a focus is most often viral, but the task is to separate the viral majority from the bacterial minority, and within that minority to find the children with an invasive rather than a contained infection. [1] [3]
Viral infection (the commonest)
- Upper respiratory infection, bronchiolitis, influenza, gastroenteritis, exanthems
- Usually well-appearing with a compatible syndrome
- A documented virus lowers but does not abolish bacterial coinfection risk
- Reassess; do not anchor on the virus if the child is unwell
Focal serious bacterial infection
- Urinary tract infection and pyelonephritis — the commonest SBI in febrile infants
- Pneumonia, empyema
- Meningitis, brain abscess
- Osteomyelitis, septic arthritis, cellulitis, abscess, enteritis
Invasive bacterial infection
- Bacteraemia with or without a focus
- Meningococcaemia with petechiae, purpura and shock
- Pneumococcal or meningococcal meningitis
- Sepsis progressing to septic shock and multi-organ failure
Non-infectious mimics
- Leukaemia and other malignancy with fever and cytopenias
- Kawasaki disease, autoimmune inflammation
- Drug fever, factitious fever, heat illness
- Haemophagocytic lymphohistiocytosis and macrophage activation
Contaminant or sampling artefact
- Coagulase-negative staphylococci in a single bottle
- Organism, timing and host context decide pathogen versus contaminant
- Repeat only if clinical concern persists; avoid reflex line removal
- Document the interpretation so downstream teams do not over-treat
Build the differential in order of immediate threat. Ask first what could kill the child now: meningococcaemia, sepsis, meningitis, a deep abscess. Then ask what is most likely given age, exposure and season: a viral syndrome, a urinary tract infection, a pneumonia. Then ask what is reversible and what would be most harmful to miss. A rigoring febrile child with a petechial rash is meningococcaemia and gets antibiotics before the differential is finished; a well-appearing toddler with coryza is viral until something changes that view. [1] [12]
Clinical & Bedside Assessment
Begin with the doorway impression. Is the child interactive and consolable, with normal colour and tone, or is there something that makes you want to step closer? Say it out loud and write it down: "alert, smiling, pink, normal tone, drinks well" or "withdrawn, mottled, tachypnoeic, grunting, reduced interaction". This appearance judgement is the most important single observation because it determines whether the child moves down a resuscitation pathway or a risk-stratification pathway. [1] [3]
Vital signs and the focused examination
Measure temperature, heart rate, respiratory rate, capillary refill, oxygen saturation and blood pressure, and interpret each against age-appropriate ranges and the child's personal baseline. Then hunt for a focus: ears and throat, chest (work of breathing, air entry, crackles, wheeze), abdomen (tenderness, organomegaly), skin (rash, cellulitis, petechiae, purpura), joints and limbs (swelling, warmth, refusal to bear weight), and central nervous system (fontanelle, tone, meningism, conscious level). Meningeal signs are unreliable in infants under one year; a bulging fontanelle, irritability or altered interaction may be the only clue to meningitis in this group. [1] [2]
Bedside assessment of the febrile child at possible risk of bacteraemia
Doorway appearance
Decide toxic versus well-appearing and state it. A toxic child enters the resuscitation pathway immediately.
Age-adjusted observations
Temperature, heart rate, respiratory rate, capillary refill, oxygen saturation and blood pressure against age-appropriate ranges.
Focused focus search
Ears, throat, chest, abdomen, skin, joints and central nervous system. A found focus changes the differential and the work-up.
Bedpoint tests
Capillary or clean-catch urine where indicated; point-of-care glucose in any unwell or altered child.
Risk synthesis
Combine age, appearance, focus, comorbidity and observations into a single risk estimate that drives the investigation plan.
Take the history in parallel, prioritising onset, tempo, maximum temperature, intake, urine output, behaviour, rash, rigors, focal pain, immunisation status, exposures and contacts. Ask specifically about immunisation against pneumococcus, Hib and meningococcus, about any indwelling device, about sickle cell or asplenia, and about a family or household contact with invasive bacterial disease. In an unwell child, do not let history-taking delay resuscitation. [1] [3]
Investigations
The guiding principle is that a test must change a decision. In the toxic child, investigations run alongside resuscitation and the first blood culture is drawn as access is established; in the well-appearing older child, most tests are unnecessary and the question is whether the child is low-risk enough to avoid a culture entirely. [1] [3]
Blood culture: the test that defines the diagnosis
Blood culture is the reference standard for bacteraemia, and its single most important modifiable attribute is volume. Yield rises with the volume of blood cultured, and under-filling is the commonest reason a true bacteraemia is missed; pediatric programmes that increased the inoculum volume saw higher detection of true pathogens. Draw the culture before antibiotics whenever it is safe to do so, because even a single dose of an effective antibiotic can sterilise a culture — but never delay antibiotics in a septic child to obtain one. [6] [10] [13]
Always in the unwell or young infant
- Blood culture before antibiotics where safe
- Urine (catheter or suprapubic) for microscopy and culture
- Blood gas, lactate and glucose in the shocked or altered child
- Full blood count, CRP and, where available, procalcitonin
Conditional and question-driven
- Lumbar puncture when meningitis is plausible and the child is stable
- Chest radiograph only if respiratory signs or persistent tachypnoea
- Electrolytes, renal and hepatic indices, coagulation in the unwell child
- Rapid viral testing to reframe but not exclude bacterial coinfection
Avoid in the low-risk child
- Routine blood cultures in well-appearing vaccinated older children
- Panels of inflammatory markers that will not change disposition
- Imaging or lumbar puncture when the child is unstable
- Repeated cultures for an obvious contaminant without clinical change
Inflammatory markers and the prediction rules
No single blood number confirms or excludes bacteraemia in isolation, but the markers are powerful when combined into validated prediction tools. A systematic review and meta-analysis found procalcitonin to be the most accurate individual inflammatory marker for invasive and serious bacterial infection in young febrile infants, ahead of C-reactive protein and white-cell count, though neither is perfect. The absolute neutrophil count, C-reactive protein and procalcitonin are the variables that modern prediction rules draw on. [11]
The PECARN febrile infant prediction rule combines urinalysis, absolute neutrophil count and procalcitonin to identify infants sixty days and younger at very low risk of serious bacterial infection, so that a proportion can be safely managed with observation rather than empiric lumbar puncture, antibiotics and admission. The American Academy of Pediatrics guideline operationalises a similar age-banded approach for well-appearing infants eight to sixty days old. Both tools are decision aids that sit beneath clinical judgement: a worried clinician or caregiver overrides a "low-risk" label. [2] [3]
CULTURE
Lumbar puncture: when, and what antibiotics do to it
Lumbar puncture is indicated when meningitis is plausible and the child is stable enough for the procedure. Antibiotics sterilise the cerebrospinal fluid within hours: classic data showed that after parenteral antibiotic pretreatment, CSF cultures become sterile within hours and are usually negative well before 24 hours. The practical consequence is that a negative CSF culture in a child who received pre-hospital or pre-LP antibiotics does not exclude bacterial meningitis — interpret the cell count, biochemistry and the clinical course, and treat on probability. Perform a delayed lumbar puncture once the child is stable if the initial study could not be done. [6]
Management — Resuscitation
A toxic or shocked child with suspected bacteraemia is a sepsis resuscitation first and an infectious-disease question second. The Surviving Sepsis Campaign international guidelines for children set the standard bundle: recognise and escalate early, establish airway and breathing support as needed, obtain vascular access (intravenous or intraosseous) and draw cultures, give empirical broad-spectrum antibiotics within the first hour, and use judicious fluid boluses with vasoactive support for refractory shock. [12]
Give oxygen to any child with hypoxia or respiratory compromise, and support ventilation when breathing is ineffective. Establish access and draw the blood culture, urine and bloods, then start empirical antibiotics within the first hour in suspected septic shock — the antibiotics must not wait for the work-up to finish. The first hour bundle of the Surviving Sepsis Campaign links early antibiotics to outcome, and the principle holds for the child with apparent bacteraemia who is deteriorating. [12]
Use fluid in aliquots, not as a target. The Surviving Sepsis Campaign recommends an initial bolus of 10 to 20 mL/kg of isotonic crystalloid, with reassessment after each aliquot and escalation to vasoactive support if shock persists or signs of fluid overload appear. A bolus volume is a ceiling to be reassessed against, never a goal to be reached: stop for hepatomegaly, rising respiratory distress, new crackles or a failing circulation, and call for critical-care and retrieval help early. [12]
The first hour in suspected sepsis or apparent bacteraemia
Recognise and call for help
State toxicity and shock; activate the local sepsis response and name a team leader.
Airway and breathing
Oxygen for hypoxia or compromise; escalate to ventilatory support if breathing is ineffective.
Access and cultures
Intravenous or intraosseous access; draw blood culture, urine and bloods before antibiotics if it does not delay them.
Empiric antibiotics
Broad-spectrum, weight-based, within the first hour; do not wait for culture results in septic shock.
Judicious fluids and vasoactives
10 to 20 mL/kg crystalloid aliquots with reassessment; vasoactive support for refractory shock; stop for overload.
Source control and reassess
Remove or drain the source; reassess appearance, perfusion and trend continuously.
Management — Definitive & Stepwise
Once the child is stable, the stepwise plan is driven by age, appearance and the likely organism. The aim is to treat genuine invasive bacterial infection aggressively, to avoid exposing low-risk children to unnecessary investigation and antibiotics, and to build a follow-up structure that catches the child whose culture turns positive after discharge. [1] [3]
The febrile young infant: follow the validated pathway
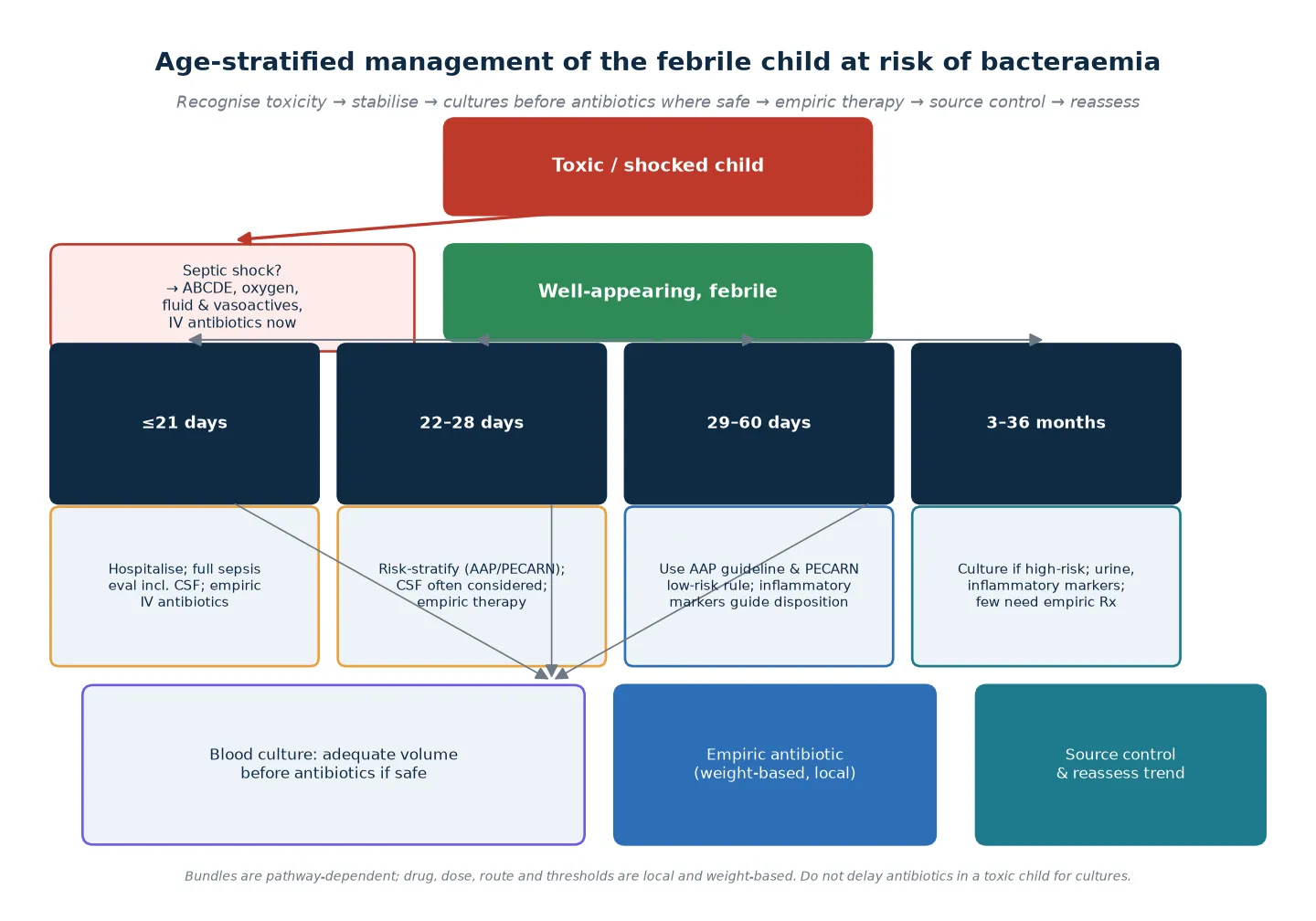
For the well-appearing febrile infant in the first two months of life, the American Academy of Pediatrics guideline and the PECARN prediction rule structure the decision. Infants eight to twenty-one days old with fever are managed as high-risk: full sepsis evaluation including cerebrospinal fluid, admission and empirical intravenous antibiotics. Infants twenty-two to twenty-eight days old are risk-stratified using inflammatory markers and urinalysis, with lumbar puncture often performed and empirical therapy usual. Infants twenty-nine to sixty days old can be managed with the PECARN low-risk rule, where a combination of normal urinalysis, absolute neutrophil count and procalcitonin allows a proportion to be observed without lumbar puncture or empirical antibiotics. [2] [3]
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne fever-without-source guideline structures investigation of the febrile child in the Victorian system and is widely referenced across Australasia. Local fever and sepsis pathways differ between services and between Australia and Aotearoa New Zealand, so verify the active local rule rather than importing a single threshold. NICE NG143 is an England-and-Wales traffic-light tool, not an ANZ standard. [1] [2]
Empiric antibiotic selection
Empiric therapy is chosen for the likely organism, the age and the focus, and given in weight-based doses from the local paediatric drug chart — this page names agents but does not publish a universal dose. For the young infant, a third-generation cephalosporin such as cefotaxime or ceftriaxone (typically 50 mg/kg per dose in the local weight-based regimen) covers the common neonatal and infant pathogens; ampicillin is added in the first weeks of life for listeria. For the older child with suspected occult or apparent bacteraemia, ceftriaxone is the usual single agent, with vancomycin added when meningitis, methicillin-resistant staphylococci or severe sepsis raise the stakes. [3] [12]
[3] [12]The well-appearing older child and the modern role of expectant antibiotics
In the well-appearing vaccinated child over three months with fever without focus, the residual rate of occult bacteraemia is now so low that routine blood cultures and empirical ceftriaxone — the standard expectant-observation practice of the 1990s — are no longer justified for most children. Investigate the higher-risk child: those with high fever, an abnormal appearance, an identified focus, abnormal inflammatory markers or a vulnerable host. For those sent home, a clear safety-net and reliable follow-up of the culture result are the safeguards that replaced routine antibiotics. [1] [3]
Source control, de-escalation and follow-up
Find and remove the source. Drain an abscess, wash out a septic joint, manage a central line, and reconsider the diagnosis if a child fails to improve. When the organism and sensitivities return, narrow therapy to the narrowest effective agent — antimicrobial stewardship is part of managing bacteraemia, not an add-on. Arrange follow-up of every blood culture result at 24 hours, give the family a specific safety-net for what change brings them back, and ensure pending results have a named owner before the child leaves your care. [1] [10]
Specific Subtypes & Scenarios
The recognition loop is constant, but the organism, the host and the setting change what you look for and how aggressively you act. Each scenario below keeps resuscitation first, then asks what is specific to that child. [1] [3]
Febrile infant ≤60 days
- Higher pre-test risk of invasive bacterial infection
- Driven by E. coli, group B streptococcus and, historically, Listeria
- Manage with the AAP guideline and PECARN low-risk rule
- Do not be reassured by a well appearance or a normal temperature
Meningococcaemia
- Fever with petechial or purpuric rash, rapid progression
- Time-critical: antibiotics and resuscitation before completing the differential
- Consider shock, adrenal haemorrhage and meningitis together
- Notify public health; arrange chemoprophylaxis for close contacts
Occult pneumococcal bacteraemia
- Now rare in vaccinated populations
- When it occurs, usually in under-vaccinated or immunocompromised children
- Historically carried a risk of meningitis if untreated
- Reevaluate; admit and treat if the child deteriorates or fails to improve
Salmonella bacteraemia
- Higher risk in infants under three months and in sickle cell disease
- Consider focal complications: osteomyelitis, meningitis, endovascular
- Non-typhoidal Salmonella in young infants often treated empirically
- Enteric fever is a separate pathway with its own regional guidance
Central-line bloodstream infection
- Oncology, intestinal failure, complex chronic disease
- Coagulase-negative staphylococci can be a true pathogen
- Assess line and host together; line salvage, lock or removal
- Stewardship and a bundled prevention strategy apply
Fever in the neutropenic or immunocompromised child
- Fever in neutropenia is an emergency — broad-spectrum cover immediately
- Signs may be blunted; do not wait for toxicity
- Add anti-pseudomonal cover per the local oncology protocol
- Involve the oncology or immunology team early
Asplenic and hyposplenic children
- Encapsulated organisms: pneumococcus, meningococcus, Hib, salmonella
- Fulminant sepsis can develop within hours
- Ensure vaccination and standby emergency antibiotics per personal plan
- Sickle cell disease adds Salmonella osteomyelitis risk
Rural, remote or under-vaccinated
- Higher prevalence of vaccine-preventable invasive disease
- Delayed access to definitive care lowers the threshold to treat
- Plan retrieval and a delay contingency early
- Confirm immunisation status and treat gaps as additional risk
Complications & Pitfalls
Most harm on this topic comes from one of two errors: treating a toxic child too slowly, or over-investigating and over-treating a low-risk child while a contaminant is pursued as a pathogen. Both errors are preventable by sticking to appearance, age and validated rules. [1] [3]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Treating a contaminant as a pathogen | Unnecessary antibiotics, line removal, admission and resistance | Read the organism, number of bottles and host context; repeat only if concern persists |
| Under-filled blood culture | A true bacteraemia is missed and the child is falsely reassured | Draw an adequate volume for age and weight; audit volumes locally |
| Antibiotics before culture without documentation | Negative cultures mislead downstream teams | Record antibiotic timing; interpret cultures in light of pretreatment |
| Delaying antibiotics in septic shock for the work-up | The first hour of sepsis matters for survival | Draw cultures as access is established, but give antibiotics within the hour |
| Over-investigating low-risk older children | Pain, false positives, cost and antimicrobial exposure | Reserve cultures for higher-risk children; use a clear safety-net |
| Trusting a well appearance in a young infant | Invasive infection is missed in the highest-risk age group | Apply age-stratified pathways regardless of how well the baby looks |
| Failing to follow up a pending culture | A positive culture after discharge is acted on late | Name an owner for every pending result before the child leaves |
| Ignoring caregiver concern | The change from baseline is lost and deterioration is missed | Treat caregiver-reported change as clinical information and reassess |
Look actively for harm from treatment once the child is stable: fluid overload, drug reactions, line complications, repeated painful sampling and the psychological impact of an unnecessary admission. The fact that the child did not arrest does not prove an intervention was harmless, and a positive culture that later proves to be a contaminant should prompt a stewardship conversation, not quiet continuation. [1] [10]
Prognosis & Disposition
Disposition follows appearance, age, the likely organism, the trend and the family's ability to act on a safety-net — never a single number. The toxic or septic child is admitted for ongoing resuscitation and critical care; the febrile young infant is managed on the validated pathway; the well-appearing older child at low risk can be discharged with a clear safety-net and reliable follow-up of the culture result. [1] [3]
In the pre-vaccine era, reevaluation studies of children with occult pneumococcal bacteraemia found that a proportion had developed a focal complication such as meningitis by the time they returned, which is what made the entity worth chasing. Those risks have fallen with conjugate vaccines, but the principle endures: a child discharged with a pending culture must have a structure that catches deterioration, and a positive result must reach a named clinician. [7] [8]
Admit to critical care
- Toxic or shocked, or with a rapidly progressive rash
- Need for ventilation, vasoactives or monitoring beyond ward capability
- Meningococcaemia, septic shock or suspected meningitis
- Retrieval activated before local support is exhausted
Admit to ward or observation
- Young infant managed on the febrile-infant pathway
- Pending culture in a child who cannot be safely observed at home
- Empirical antibiotics running and trend not yet reassuring
- Awaiting inflammatory markers, CSF or imaging
Discharge only when defensible
- Sustained improvement or stable low-risk presentation
- No high-harm diagnostic concern and a viable safety-net
- Named owner for every pending result
- Caregiver concern addressed and understanding checked
A defensible safety-net names what change to watch for, how urgently to act, and exactly where or how to get help. "Return if worried" is not enough. Confirm understanding with teach-back, document the plan, and connect the child to primary care or the medical home so that the pending culture and any follow-up have a clear handover. [1] [3]
Special Populations
The standard of vigilance is the same; what changes is the pre-test probability and the threshold to treat. In each group below, fever is a higher-stakes signal than in a fully vaccinated, previously well child of the same age. [1] [9]
| Population | Why the risk is higher | Adaptation in care |
|---|---|---|
| Immunocompromised, neutropenic or post-transplant | Blunted inflammatory signs; rapid progression; broader organism range | Empirical broad-spectrum cover immediately; involve the specialist team early |
| Central venous catheter or device | Line infection with skin-flora organisms; biofilm | Assess line and host together; line salvage, lock or removal per protocol |
| Asplenia or sickle cell disease | Encapsulated organisms; fulminant sepsis | Personal emergency plan with standby antibiotics; confirm vaccination |
| Neonate and young infant | Immature immunity; blunted, afebrile presentation | Age-stratified pathway regardless of how well the baby looks |
| Indigenous, remote or under-vaccinated | Higher vaccine-preventable disease prevalence; access barriers | Lower threshold to treat; plan retrieval early; verify immunisation |
| Migrant, refugee or newly arrived | Possibly incomplete vaccination and exposure history | Treat immunisation gaps as additional risk; use interpreter services |
Use a professional interpreter for any family with limited English proficiency during a clinical or safety-net conversation; communication access is a safety measure, not a courtesy. For Indigenous children and families, work with the local Aboriginal and Torres Strait Islander or Māori health service and recognise that delayed presentation and disproportionate invasive-disease burden reflect access and structural factors that the clinician can act on. [1]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The transformation of this topic by conjugate vaccines is among the best-evidenced changes in modern paediatrics. Successive pneumococcal conjugate vaccine programmes produced large, sustained falls in vaccine-serotype invasive pneumococcal disease in young children, both directly and through indirect (herd) protection, which is why the clinical question moved from "chase occult bacteraemia" to "risk-stratify the febrile child". [9]
PECARN febrile infant prediction rule
JAMA Pediatrics
Prospective cohort derivation of a prediction rule in febrile infants 60 days and younger across the Pediatric Emergency Care Applied Research Network
Key finding
A combination of urinalysis, absolute neutrophil count and procalcitonin identified infants at very low risk of serious bacterial infection.
Practice change
A proportion of well-appearing young infants can be safely observed without lumbar puncture or empirical antibiotics, under clinical judgement.
Surviving Sepsis Campaign — Children 2026
Pediatric Critical Care Medicine
International consensus guidelines for paediatric sepsis and septic shock
Key finding
A first-hour bundle of recognition, access, cultures, antibiotics within the hour, judicious fluids and vasoactive support for refractory shock.
Practice change
Empiric antibiotics within the first hour and aliquot-based fluid resuscitation with early vasoactive support for septic shock.
Inflammatory markers are imperfect. A systematic review and meta-analysis confirmed that procalcitonin outperforms C-reactive protein and white-cell count for invasive and serious bacterial infection in young febrile infants, but no single marker is sensitive or specific enough to rule bacteraemia in or out alone; they work as part of validated rules, not as stand-alone tests. A documented viral infection lowers but does not abolish the coinfection risk. Where evidence is thin — the exact procalcitonin threshold, the role of cerebrospinal fluid analysis in every older young infant, the place of expectant antibiotics in the modern era — say so and defer to the active local pathway. [4] [11]
Jurisdictional implementation
Global and low-resource settings: vaccine uptake, serotype distribution and access to culture and antibiotics vary widely, so the prevalence of occult and apparent bacteraemia is higher where conjugate vaccine coverage is incomplete. WHO Integrated Management of Childhood Illness (IMCI) and local fever-and-sepsis pathways structure assessment in low-resource settings; do not transplant a high-resource rule uncritically into a setting where the population risk and available rescue differ. [9] [12]
Controversies and open questions
Three debates recur. First, the optimal procalcitonin threshold for defining low risk in young infants is still refined by ongoing meta-analyses. Second, whether cerebrospinal fluid analysis is needed in every febrile young infant, or only in a risk-stratified subset, is now answered by validated rules for the well-appearing 29-to-60-day-old but remains case-by-case for the 22-to-28-day-old. Third, the place of expectant empirical ceftriaxone in well-appearing older children has all but disappeared with the fall in occult bacteraemia, replaced by selective investigation and reliable follow-up. In each case, the named guideline is the operative standard and the local pathway is the deliverable. [1] [2] [3] [11]
Exam Pearls
Reframe
- Conjugate vaccines collapsed the old occult-bacteraemia problem
- The modern question is risk of invasive bacterial infection, not chasing a culture
- Young infants still carry the risk — age is the master variable
Assessment
- Appearance is the single most powerful bedside variable
- Hunt for a focus: ears to skin to joints
- Read age × appearance × focus × comorbidity as one risk estimate
Investigation
- Blood culture volume is the key determinant of yield
- Procalcitonin is the best single inflammatory marker but imperfect
- Use PECARN and AAP rules, not a single threshold
- Antibiotics sterilise CSF within hours — interpret post-treatment cultures accordingly
Management
- Resuscitate the toxic child first; antibiotics within the hour in septic shock
- Empiric agent by age and focus: ceftriaxone, plus ampicillin in neonates, plus vancomycin if meningitis or MRSA
- Source control and stewardship narrow therapy
- Adequate blood volume before antibiotics when safe to wait
Safety
- Name an owner for every pending culture before discharge
- A contaminant is not a pathogen — state organism, bottles and host
- Give a specific safety-net, not 'return if worried'
- Check understanding with teach-back
Boundaries
- No universal dose on this page — local and weight-based
- A well appearance does not close the question under two months
- A negative culture after antibiotics does not exclude meningitis
- A documented virus does not exclude bacterial coinfection
“Appearance + age + focus → resuscitate if toxic, else risk-stratify → adequate-volume culture before antibiotics if safe → weight-based empiric therapy → source control and stewardship → 24-hour follow-up with a named owner and a specific safety-net.”
Viva: a well-appearing 14-month-old with fever to 39.5 °C and no focus
Start by stating that the post-conjugate-vaccine prevalence of occult bacteraemia in such a child is now well below one per cent, so routine blood culture and empirical ceftriaxone are not justified for most well-appearing vaccinated children. Assess appearance explicitly, examine for a focus, check a urine if the fever is unexplained or the child is under 24 months, and reserve blood culture and inflammatory markers for higher-risk features: a high or prolonged fever, an abnormal appearance, an identified focus, a vulnerable host or incomplete immunisation. Send the child home with a specific safety-net — what change brings them back and how urgently — and name a clinician who owns the result of any pending test. [1] [3] [9]
Viva: a febrile 25-day-old who looks well
Do not be reassured by the appearance. A febrile infant at 25 days is managed on the validated pathway: this age band sits between the always-investigate under-21-day group and the PECARN-eligible 29-to-60-day group, and is usually risk-stratified with inflammatory markers and urinalysis, with lumbar puncture often performed and empirical intravenous antibiotics commonly given. State that appearance is a weaker discriminator in young infants, and that the goal is to identify invasive bacterial infection early in the age group where it is most likely and most easily missed. [2] [3]
SAQ: a positive blood culture 24 hours after discharge
Call the family, recall the child, and reassess appearance and focus. Reinterpret the organism against the host: a true pathogen such as pneumococcus, meningococcus or E. coli demands urgent assessment, repeat cultures if indicated, empirical or directed therapy and admission; a single-bottle coagulase-negative staphylococcus in a now-well child is more likely a contaminant and warrants clinical reassessment rather than reflex treatment. State that a pending result must always have a named owner so that this call happens within a safe interval, and that the safety-net you gave at discharge is what makes a positive culture actionable rather than dangerous. [1] [6] [10]
References
- [1]Gomez B Bacteremia in previously healthy children in emergency departments: clinical and microbiological characteristics and outcome European journal of clinical microbiology & infectious diseases, 2015.PMID 25252630
- [2]Kuppermann N A Clinical Prediction Rule to Identify Febrile Infants 60 Days and Younger at Low Risk for Serious Bacterial Infections JAMA pediatrics, 2019.PMID 30776077
- [3]Pantell RH Evaluation and Management of Well-Appearing Febrile Infants 8 to 60 Days Old Pediatrics, 2021.PMID 34281996
- [4]Mahajan P Risk of Bacterial Coinfections in Febrile Infants 60 Days Old and Younger with Documented Viral Infections The Journal of pediatrics, 2018.PMID 30195552
- [5]Mahajan P Association of RNA Biosignatures With Bacterial Infections in Febrile Infants Aged 60 Days or Younger JAMA, 2016.PMID 27552618
- [6]Kanegaye JT Lumbar puncture in pediatric bacterial meningitis: defining the time interval for recovery of cerebrospinal fluid pathogens after parenteral antibiotic pretreatment Pediatrics, 2001.PMID 11694698
- [7]Bachur R Reevaluation of outpatients with Streptococcus pneumoniae bacteremia Pediatrics, 2000.PMID 10699100
- [8]Korones DN Occult pneumococcal bacteremia: what happens to the child who appears well at reevaluation? The Pediatric infectious disease journal, 1994.PMID 8072821
- [9]Ben-Shimol S Dynamics of invasive pneumococcal disease in infants younger than 2 years old following PCV7/13 implementation using two infant and a booster dose schedule: evidence for indirect protection of young infants, Israel, 2004 to 2019 Euro surveillance, 2023.PMID 37347413
- [10]Gaur AH Optimizing blood culture practices in pediatric immunocompromised patients: evaluation of media types and blood culture volume The Pediatric infectious disease journal, 2003.PMID 12799512
- [11]Norman-Bruce H Diagnostic test accuracy of procalcitonin and C-reactive protein for predicting invasive and serious bacterial infections in young febrile infants: a systematic review and meta-analysis The Lancet Child & adolescent health, 2024.PMID 38499017
- [12]Weiss SL Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026 Pediatric critical care medicine, 2026.PMID 41869844
- [13]Whelan SO Pediatric blood cultures - turning up the volume: a before and after intervention study European journal of pediatrics, 2024.PMID 38656384