Paeds · infectious-diseases
Cellulitis, abscess and necrotising soft-tissue infection
Also known as Skin and soft-tissue infection · Cellulitis · Cutaneous abscess · Necrotising fasciitis · Necrotising soft-tissue infection · Gas gangrene
Fellowship guide to paediatric cellulitis, cutaneous abscess, and necrotising soft-tissue infection: distinguishing non-purulent from purulent and necrotising disease, age- and MRSA-aware antibiotic selection, incision and drainage as definitive therapy for abscess, and the time-critical recognition and surgical management of necrotising fasciitis including the LRINEC score, empiric broad-spectrum cover, and prognosis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Skin and soft-tissue infections span a spectrum from mild, self-limiting cellulitis to rapidly fatal necrotising fasciitis, and the clinician's central task is to place each child correctly along that spectrum. The 2014 Infectious Diseases Society of America guidelines frame this as three categories that drive every management decision: non-purulent infection such as cellulitis and erysipelas, purulent infection such as a cutaneous abscess, and necrotising infection that is a surgical emergency. Two organisms, Staphylococcus aureus and Streptococcus pyogenes, cause the great majority of paediatric cases, but their behaviour and the treatment they demand differ sharply across the categories. [1]
Cellulitis is a non-purulent, spreading infection of the dermis and subcutaneous tissue that responds to antibiotics, while a cutaneous abscess is a localised collection of pus within the skin that is cured by incision and drainage and often needs no antibiotic at all. Necrotising soft-tissue infection is fundamentally different: it destroys tissue along fascial planes, thromboses the blood supply to the overlying skin, and cannot be controlled by antibiotics alone because drug cannot reach dead, avascular tissue. The mortality of necrotising infection in children, though lower than in adults, remains substantial, and survival depends on how quickly the surgeon reaches the operating theatre. [2]
The cardinal principle is that the dividing line between a child who needs oral antibiotics and one who needs emergency surgery is a clinical judgement, not a single test. Severe pain out of proportion to the visible skin changes, systemic toxicity, and rapid progression are the features that should trigger escalation long before the laboratory results return. Every clinician assessing a child with a skin infection must actively ask whether this could be necrotising disease, because that question, asked early, is the one that saves limbs and lives. [3]
Classification
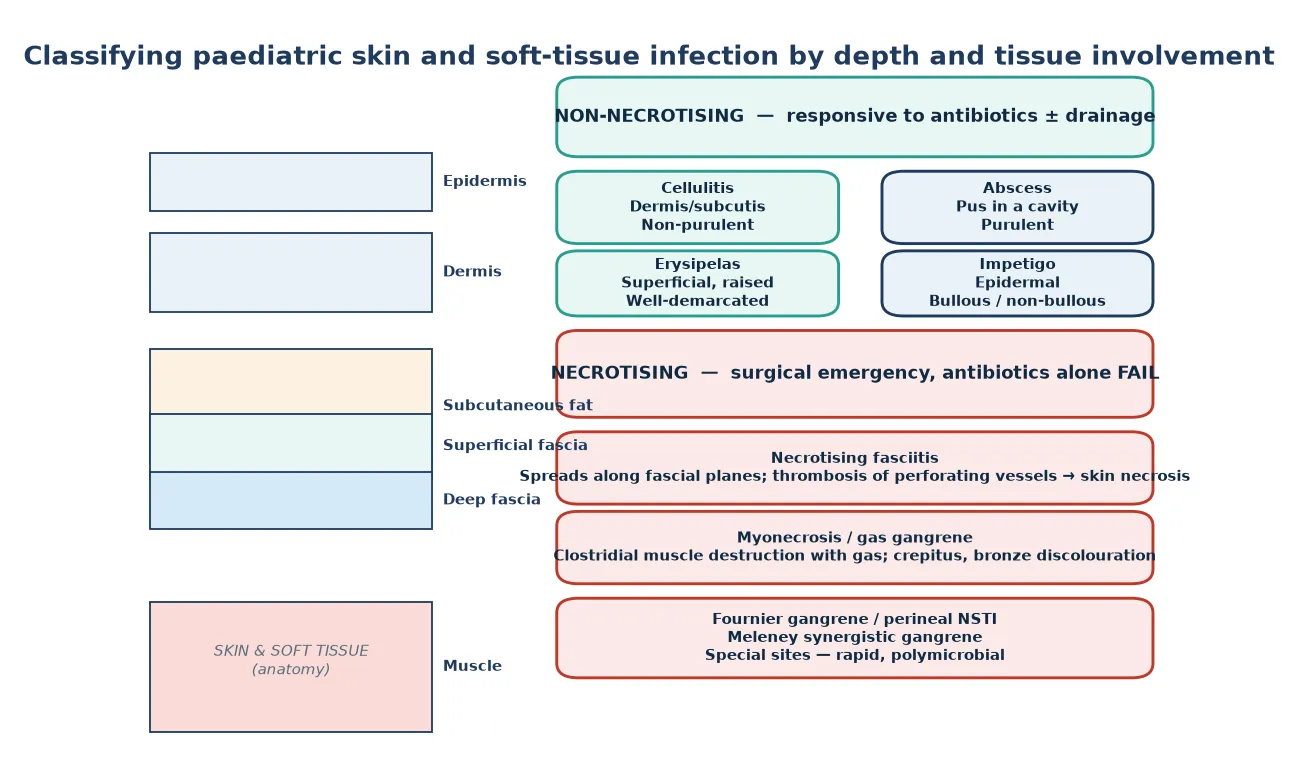
The classification used at the bedside separates infection by two axes: the presence or absence of pus, and whether the infection is necrotising. Non-purulent infection includes cellulitis, which involves the deep dermis and subcutaneous fat, and erysipelas, which is a more superficial, raised, sharply demarcated form affecting the upper dermis. Purulent infection is the cutaneous abscess, a walled-off collection of pus that may be surrounded by a rim of cellulitis. Necrotising infection involves the fascia and deeper tissues and includes necrotising fasciitis, myonecrosis or gas gangrene, and special-site forms such as Fournier gangrene of the perineum. [1]
[1]Depth of tissue involvement refines the picture further. Impetigo is a superficial epidermal infection, bullous or non-bullous, that is usually managed with topical or oral agents and sits outside the cellulitis-abscess-necrotising triad. Periorbital or preseptal cellulitis involves the eyelid and superficial tissues anterior to the orbital septum, whereas orbital cellulitis lies posterior to the septum and threatens vision and intracranial spread, so the distinction drives imaging and admission decisions. Knowing where the infection sits anatomically determines both the likely organism and the urgency. [8]
Epidemiology & Risk Factors
Skin and soft-tissue infections are among the most common reasons children present to emergency departments and are admitted to hospital, and their epidemiology has been reshaped by the rise of community-associated methicillin-resistant Staphylococcus aureus. In centres where MRSA is prevalent, it now accounts for a large proportion of purulent infections and abscesses in children, whereas cellulitis and erysipelas remain predominantly streptococcal. The prominence of MRSA has shifted empiric antibiotic choice toward agents such as clindamycin and trimethoprim-sulfamethoxazole for purulent disease. [6]
Necrotising fasciitis is uncommon in children but carries a disproportionate burden of mortality and long-term morbidity. Group A Streptococcus is the most frequent cause of monomicrobial necrotising fasciitis in previously well children, while polymicrobial infections involving anaerobes and Gram-negative organisms are seen after surgery, in immunocompromised hosts, and in special sites such as the perineum. Case fatality in paediatric necrotising infection is reported in the range of 5 to 20 per cent and rises steeply when surgical debridement is delayed. [3]
The dominant risk factors for severe or necrotising disease are young age, immunocompromise, diabetes, malnutrition, obesity, and breaks in the skin from trauma, insect bites, surgery, or varicella lesions. A preceding blunt injury or muscle strain is often the portal of entry for Vibrio species in coastal settings and for Aeromonas after freshwater exposure. In Indigenous and remote communities across Australia and New Zealand, higher rates of skin infection, recurrent impetigo and abscess, scabies, later presentation, and greater distance from surgical services all amplify both risk and severity. [12]
Pathophysiology
Most skin and soft-tissue pathogens enter through a break in the skin, whether a surgical wound, an insect bite, a varicella lesion, or unrecognised minor trauma, and then spread through the tissue planes they are equipped to invade. Streptococcus pyogenes spreads rapidly through the dermis and subcutaneous tissue using hyaluronidase and streptokinase, producing the spreading erythema of cellulitis and, when it reaches the fascia, the destructive invasion of necrotising fasciitis. Staphylococcus aureus tends to form a walled-off abscess through its coagulase activity, localising pus within the skin. [2]
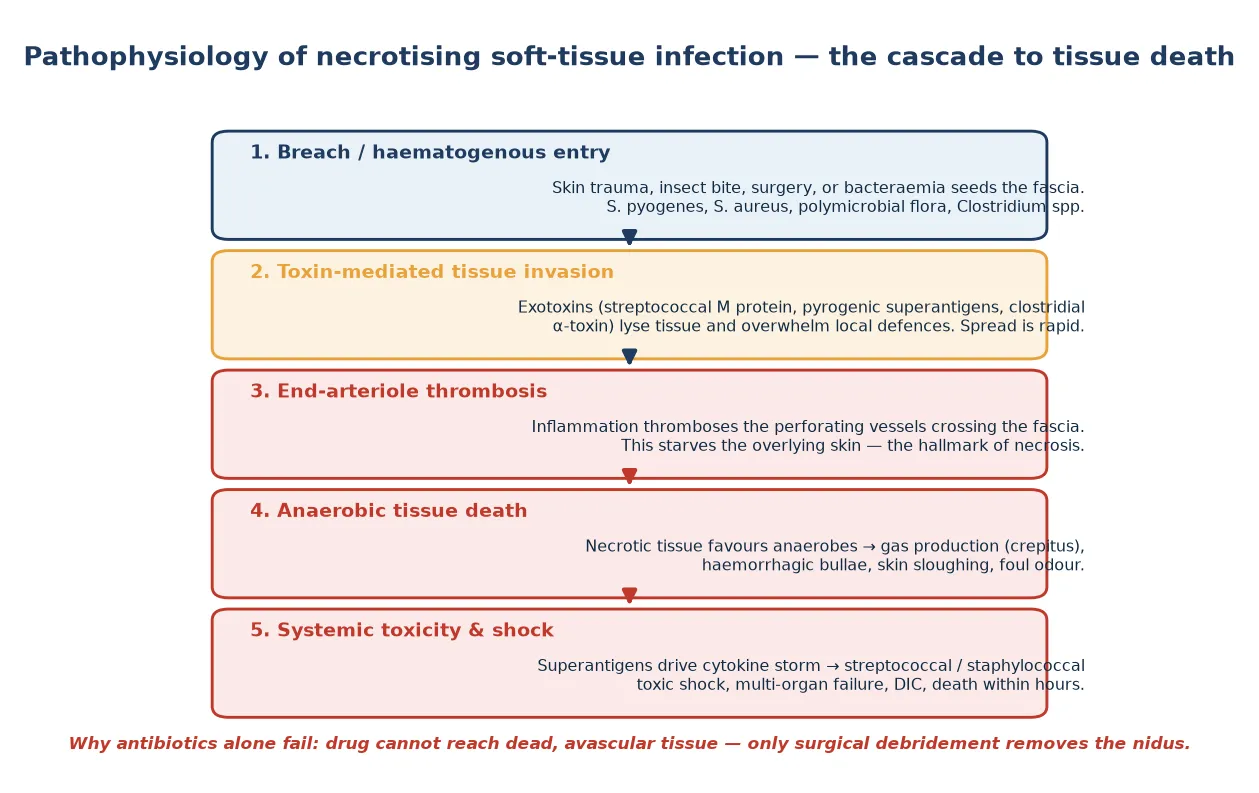
The defining event in necrotising infection is thrombosis of the small perforating blood vessels that cross the fascia to supply the overlying skin. As inflammation intensifies within the fascial plane, these end-arterioles thrombose, starving the skin and subcutaneous tissue of blood. This is why the skin initially looks deceptively normal while the child is in agony, and why haemorrhagic bullae, skin necrosis, and numbness appear only once the blood supply is lost. It is also why antibiotics fail: no blood flow means no drug delivery to the infected tissue. [4]
Toxins drive both the tissue destruction and the systemic illness. Streptococcal pyrogenic exotoxins and staphylococcal superantigens bypass normal antigen presentation and trigger a massive cytokine release, producing streptococcal or staphylococcal toxic shock syndrome with hypotension, multi-organ failure, and disseminated intravascular coagulation. Clostridial alpha-toxin, in gas gangrene, lyses tissue and produces gas within muscle, giving the crepitus and bronze discolouration that are late but classic signs. [2]
Clinical Presentation
Cellulitis presents with spreading erythema, warmth, swelling, and tenderness of the skin, most often on a limb or the face, with poorly demarcated margins that the clinician should mark with a pen to track progression over hours. The child is usually febrile and irritable but not toxic, and there is no fluctuance or pus. Erysipelas is the more superficial variant with a sharply raised, clearly demarcated border, classically on the face or lower limb. [6]
A cutaneous abscess presents as a tender, fluctuant, erythematous swelling, often with a visible pustule or point, and frequently in the axilla, groin, buttock, or neck where Staphylococcus aureus colonises the skin. The surrounding skin may show a rim of cellulitis, and the child may have a low-grade fever. The diagnosis is clinical, and bedside ultrasound can confirm a fluid collection when examination is uncertain, particularly in the chubby subcutaneous tissue of young children. [9]
Necrotising fasciitis presents with the triad of severe pain out of proportion to the visible findings, systemic toxicity, and rapidly progressive skin changes. Early on the skin may look like simple cellulitis, but the pain is extreme, the child is profoundly unwell, and the area is tense, woody, or indurated. As tissue death advances, the skin develops haemorrhagic bullae, numbness from nerve infarction, crepitus from gas, and finally dusky or necrotic patches. The disproportion between the child's agony and the skin's appearance is the single most important clue. [3]
Presenting features of necrotising infection by stage
Severe pain that is disproportionate to the visible skin erythema
Tachycardia, fever, irritability, and a toxic, unwell child
Tense, woody, or indurated swelling that spreads over hours
Numbness, skin beyond pain, or haemorrhagic bullae
Crepitus or dusky, necrotic skin indicating advanced tissue death
Shock, multi-organ failure, and disseminated intravascular coagulation
Periorbital cellulitis presents with eyelid swelling, erythema, and warmth without proptosis, pain on eye movement, or visual change, and the child is usually systemically well. Orbital cellulitis, by contrast, presents with the same eyelid signs plus proptosis, painful or limited eye movement, reduced visual acuity, and fever, and signals extension posterior to the orbital septum with risk of abscess, optic nerve compromise, and intracranial spread. These red flags, not the appearance of the eyelid alone, are what separate a child safe for oral therapy from one needing imaging, intravenous antibiotics, and an otolaryngology or ophthalmology review. [8]
Differential Diagnosis
The differential diagnosis for a red, swollen, painful area of skin in a child is broad, and several non-infectious causes must be excluded before committing to a diagnosis of cellulitis. The most important mimic is a deep venous thrombosis or thrombophlebitis, which can cause unilateral limb swelling and erythema, though this is uncommon in children outside the context of central lines or prothrombotic states. Contact dermatitis, insect bites, and acute allergic reactions produce erythema and swelling but are usually itchy rather than painful and lack systemic features. [9]
Orthopaedic and rheumatological conditions enter the differential when the presentation centres on a limb. Septic arthritis and osteomyelitis cause pain, fever, and reluctance to use the limb, and may coexist with overlying soft-tissue swelling. Transient synovitis of the hip, juvenile idiopathic arthritis, and a haemarthrosis in haemophilia all mimic a swollen, tender limb, so careful joint examination and, when needed, imaging distinguish a joint problem from a skin infection. [9]
Other mimics of necrotising infection include severe erythema multiforme or Stevens-Johnson syndrome, calciphylaxis in renal disease, and haemorrhagic panniculitis. In the neonate, omphalitis around the umbilical stump and breast abscess are important special-site presentations, while in the immunocompromised child, mould infections such as mucormycosis can produce necrotising lesions that require a different antifungal approach. Maintaining a broad differential prevents the tunnel vision that delays diagnosis of the surgical emergency. [2]
Clinical & Bedside Assessment
Begin every assessment with an overall judgement of how sick the child is, using the paediatric assessment triangle of appearance, work of breathing, and circulation. A child who is toxic, tachycardic, hypotensive, or peripherally shut down needs immediate resuscitation and a senior surgical review regardless of how the skin looks, because these are the children harbouring necrotising disease or toxic shock. Measure temperature, heart rate, respiratory rate, blood pressure, capillary refill, and oxygen saturation, and weigh the child for drug dosing. [3]
Examine the skin lesion itself with the child fully exposed, looking for erythema, swelling, warmth, fluctuance, and any break in the skin that marks the portal of entry. Mark the margin of erythema with a skin marker and record the time, because spread beyond that margin over the next hours is a powerful sign of progression toward necrotising infection. Gently palpate for crepitus, which is a late but specific sign of gas-forming organisms, and look for haemorrhagic bullae, skin necrosis, and numbness, each of which signals advanced tissue death. [4]
Assess for the features that separate necrotising from non-necrotising disease. The bedside clue that should trigger alarm is pain that is severe and disproportionate to the visible erythema, often with a child who screams when the area is lightly touched but whose skin looks deceptively mild. Compare this against a simple cellulitis, where the pain is proportionate to the redness and the child is mildly unwell rather than toxic. Bedside ultrasound can help by showing a fluid collection for drainage, or the fascial fluid and gas of necrotising infection, though a normal ultrasound never excludes necrotising disease. [2]
Investigations
Investigations serve two purposes in skin infection: confirming the severity of non-necrotising disease, and supporting, never replacing, the clinical decision to operate on suspected necrotising infection. For a child with mild cellulitis or a simple abscess, no blood tests or imaging are needed, and the diagnosis and treatment are clinical. For a child who is systemically unwell, send a full blood count, C-reactive protein, electrolytes, creatinine, and blood cultures before the first antibiotic dose. [9]
For suspected necrotising infection, the laboratory panel is both diagnostic and prognostic. Send blood cultures, a full blood count, C-reactive protein, creatinine, creatine kinase, sodium, glucose, coagulation studies, and a blood gas with lactate. A high lactate, a markedly raised C-reactive protein, hyponatraemia, acute kidney injury, and a rising creatine kinase each support the diagnosis and quantify the severity. The LRINEC score combines six of these values to estimate the probability of necrotising fasciitis, but it must never be used to exclude the diagnosis, because a low score in a child with disproportionate pain and toxicity is still a surgical emergency. [5]
Imaging has a limited and specific role. A plain radiograph may show soft-tissue gas in clostridial myonecrosis, and computed tomography can define the extent of deep infection and identify gas along fascial planes, but neither should delay surgery in a child with convincing clinical features. For periorbital and orbital cellulitis, contrast-enhanced computed tomography of the orbits is the modality of choice to distinguish preseptal from postseptal disease and to detect a subperiosteal or orbital abscess. A wound swab or pus from incision and drainage should be sent for Gram stain and culture to guide later antibiotic narrowing, particularly to detect MRSA. [7]
Management — Resuscitation
A child with severe skin infection and signs of shock or toxic shock needs immediate resuscitation using an airway, breathing, circulation approach. Secure the airway and give high-flow oxygen for hypoxia, respiratory distress, or a falling conscious level. Establish intravenous or intraosseous access rapidly and do not spend more than a few minutes hunting for a peripheral line before going to the intraosseous route in a shocked child. [3]
Give a 10 mL per kilogram bolus of isotonic crystalloid, 0.9 per cent sodium chloride or balanced crystalloid, for hypotension or poor perfusion, and reassess after each bolus. Repeat boluses titrated to perfusion and blood pressure may be required in septic or toxic shock, while watching for hepatomegaly and a rising oxygen requirement as signs of volume overload. In toxic shock, aggressive fluid resuscitation and early vasopressor support are essential because the cytokine storm causes profound vasodilation and capillary leak. [4]
Draw blood cultures, a full blood count, C-reactive protein, electrolytes, creatinine, coagulation, and lactate on cannulation, and give the first dose of broad-spectrum antibiotics immediately after. For suspected necrotising infection, alert the surgeon and the anaesthetist at the same time as resuscitation begins, because the resuscitation and the surgical preparation must proceed in parallel rather than in sequence. [2]
Resuscitation sequence for severe or necrotising skin infection
Assess airway, breathing, circulation and give high-flow oxygen
Establish intravenous or intraosseous access within minutes
Draw bloods and cultures, give first antibiotic dose immediately
Fluid bolus 10 mL/kg isotonic crystalloid for shock, reassess after each
Alert surgeon, anaesthetist, and PICU in parallel with resuscitation
Prepare for urgent surgical exploration and debridement
The single most important early intervention in necrotising infection is calling the surgeon. Antibiotics reduce the bacterial load and toxin production, fluids restore perfusion, but only debridement removes the dead tissue that sustains the infection, so the surgical alert belongs at the front of the management sequence rather than after stabilisation is complete. [4]
Management — Definitive & Stepwise
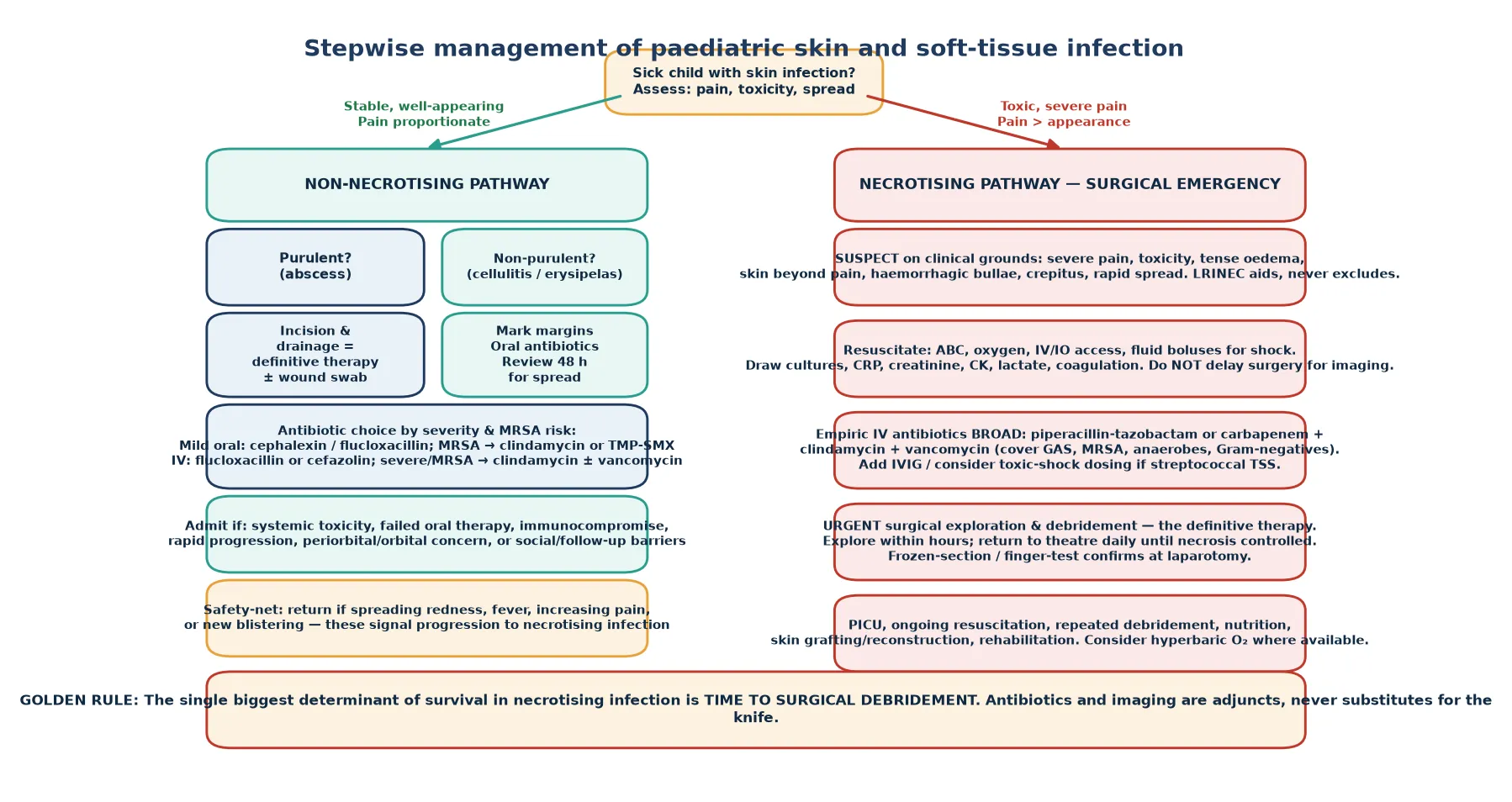
For a mild, non-purulent cellulitis in a well child, oral antibiotics directed at streptococci and staphylococci are sufficient. The first-line oral agent is cephalexin or flucloxacillin, with clindamycin or trimethoprim-sulfamethoxazole added when MRSA is suspected or prevalent locally. Mark the margins, give a clear safety-net, and review at 48 hours for response, because failure to improve signals either the wrong organism, an undrained abscess, or progression to necrotising disease. [1]
For a cutaneous abscess, incision and drainage is the definitive therapy and should be performed wherever the child is assessed. After adequate analgesia, often with topical or local anaesthetic and nitrous oxide or ketamine for larger lesions, make an adequate incision over the point of maximal fluctuance, break loculations, express the pus, and send a sample for culture. Adjunctive antibiotics are needed when there is extensive surrounding cellulitis, systemic illness, immunocompromise, or a facial or hand location, but a simple, well-drained abscess in a well child often needs no antibiotic at all. [9]
Cephalexin (oral, first-line cellulitis)
Dose
25 mg/kg (max 500 mg) orally every 6 hours for 5 days
For moderate or severe non-necrotising infection requiring admission, intravenous flucloxacillin or cefazolin is the mainstay, with clindamycin added for suspected MRSA or toxin-mediated disease. For severe or necrotising infection, the empiric regimen must be broad, covering group A Streptococcus, methicillin-sensitive and resistant Staphylococcus aureus, anaerobes, and Gram-negatives. A common combination is piperacillin-tazobactam or a carbapenem plus clindamycin plus vancomycin, with clindamycin included to suppress toxin production in streptococcal and staphylococcal toxic shock. [10]
Empiric antibiotic logic by disease category
Urgent surgical exploration and debridement is the definitive therapy for necrotising infection, and it must not wait for imaging or a full laboratory panel. At operation, the surgeon confirms the diagnosis with the finger test or frozen section, opens the involved fascial planes, and excises all necrotic tissue back to healthy, bleeding muscle and fascia. Repeat planned returns to theatre every 24 to 48 hours continue until no further necrosis is found, because the infection can outpace a single debridement. Reconstruction with skin grafting or flaps follows once the infection is controlled. [3]
Specific Subtypes & Scenarios
Periorbital cellulitis is usually managed with oral or intravenous antibiotics directed at sinus pathogens and is typically streptococcal or staphylococcal in origin. The critical decision is recognising orbital cellulitis, which presents with proptosis, painful eye movement, reduced vision, and systemic toxicity, and which demands contrast-enhanced computed tomography, intravenous antibiotics, and urgent otolaryngology and ophthalmology review. A subperiosteal or orbital abscess may require surgical drainage, and the threshold to image is low whenever a child with eyelid swelling shows any of these orbital signs. [7]
Group A streptococcal necrotising fasciitis in a previously well child is the archetype of the surgical emergency, often following varicella, a minor injury, or a muscle strain. It progresses from pain to shock within hours, is accompanied by a high risk of streptococcal toxic shock syndrome, and demands resuscitation, clindamycin-containing broad-spectrum antibiotics, and immediate surgical debridement. Intravenous immunoglobulin is often added for streptococcal toxic shock to neutralise circulating toxin, though the evidence base is limited. [2]
Clostridial myonecrosis, or gas gangrene, follows contaminated wounds and produces rapidly progressive muscle destruction with gas in the tissues, crepitus, and a bronze or dusky discolouration. It demands urgent surgical debridement of all affected muscle alongside high-dose penicillin and clindamycin. Hyperbaric oxygen has been used as an adjunct, but the evidence is insufficient to recommend it universally, and it must never delay surgery, so its role is confined to centres with chambers where it can be delivered safely after debridement. [11]
Neonatal and special-site infections deserve particular vigilance. Omphalitis around the umbilical stump can progress rapidly to necrotising fasciitis of the abdominal wall in a neonate, and a breast abscess in infancy can cause bacteraemia and scarring. In the immunocompromised child, both the range of pathogens and the threshold for surgical exploration are broader, with mould infections and Gram-negative sepsis joining the usual suspects, so infectious diseases and surgical input are essential early. [12]
[12]Complications & Pitfalls
The complications of skin infection range from local to systemic and are determined by the depth of infection and the speed of treatment. Cellulitis can cause local abscess formation, lymphangitis, and recurrent episodes that damage lymphatics. Abscesses can rupture, scar, or seed bacteraemia. Necrotising infection causes limb loss, extensive scarring, renal failure from rhabdomyolysis, and death, while toxic shock adds multi-organ failure and disseminated intravascular coagulation. [2]
Post-streptococcal complications are a particular concern in children. Cellulitis and skin sores caused by group A Streptococcus can trigger acute post-streptococcal glomerulonephritis, and recurrent streptococcal skin infection is a risk factor for acute rheumatic fever in high-risk populations, so identifying and treating streptococcal skin disease carries importance beyond the acute episode. In regions with high rates of rheumatic fever, skin health is part of preventive paediatrics. [12]
The major clinical pitfalls are giving antibiotics without draining an abscess, treating a toxic child as simple cellulitis, delaying surgery while awaiting imaging or a normalising LRINEC score, under-dosing antibiotics, and failing to provide a clear safety-net for return. Each of these errors is common, each is examinable, and each is preventable by a structured approach that asks, at every reassessment, whether this could be necrotising disease. [4]
Prognosis & Disposition
The two determinants of outcome in skin infection are the depth of infection and the speed of definitive treatment. A child with simple cellulitis or a drained abscess who responds within 48 hours has an excellent prognosis and can complete therapy at home. The child with necrotising infection fares according to how quickly debridement occurs, with mortality and limb loss rising steeply for each hour of delay toward the operating theatre. [3]
After necrotising infection and toxic shock, survivors face prolonged recovery that includes repeated operations, skin grafting, rehabilitation, and psychological support. Renal recovery from rhabdomyolysis and acute kidney injury is usually complete, but limb function depends on the extent of muscle and nerve removed at debridement. Structured follow-up with surgical, rehabilitation, and psychological services is essential, because the visible scar is often only part of the burden. [2]
Disposition depends on the severity and the response. A well child with mild cellulitis or a successfully drained abscess goes home with oral or no antibiotics and a clear safety-net. A child with systemic toxicity, rapid progression, periorbital signs, immunocompromise, or failed oral therapy is admitted for intravenous antibiotics and observation. A child with necrotising infection goes to theatre, then to the paediatric intensive care unit, then to the ward for a prolonged reconstruction and rehabilitation phase. [9]
Special Populations
Immunocompromised children, including those on chemotherapy, after transplantation, with primary immunodeficiency, or on immunosuppressive biologics, are susceptible to a broader range of pathogens including resistant Gram-negatives, moulds, and opportunistic fungi. They may present with less inflammation and more rapid progression, the threshold for surgical exploration is lower, and empiric regimens must be broadened with early infectious diseases input. A necrotising lesion in a neutropenic child is a mould infection until proven otherwise. [2]
Neonates are a special group because their immature skin and immune defences allow rapid spread of infection. Omphalitis and breast abscess can progress to necrotising fasciitis within hours, and the threshold for surgical assessment is correspondingly low. The neonate with a spreading skin infection needs intravenous antibiotics covering group B Streptococcus and Staphylococcus aureus, close observation, and a surgical review at the first sign of induration or toxicity. [12]
In Indigenous and remote communities across Australia and New Zealand, higher rates of skin infection, recurrent abscess, scabies, and post-streptococcal disease interact with later presentation and greater distance from surgical services to worsen outcomes. Culturally safe, family-centred care with interpreter access, healthy skin education, and reliable aeromedical retrieval pathways is essential. In migrant and refugee families, language barriers, overcrowded housing, and unfamiliarity with the health system shape both risk and presentation, so a clear safety-net in the family's language is part of safe care. [12]
[12]Evidence, Guidelines & Regional Differences
The 2014 Infectious Diseases Society of America guidelines remain the foundational framework for the diagnosis and management of skin and soft-tissue infection, organising care around the non-purulent, purulent, and necrotising categories. These guidelines converge with the more recent necrotising infection literature on the primacy of early surgical debridement, the use of clindamycin to suppress toxin production, and the addition of vancomycin for MRSA cover in severe disease. [1]
The LRINEC score was developed to distinguish necrotising fasciitis from other soft-tissue infections using six routine laboratory values, and it has been widely adopted despite concerns about its sensitivity. The central teaching point is that the score raises the probability of necrotising infection when it is high but never lowers it enough to exclude the diagnosis when the clinical picture is convincing, so a low score in a toxic child with disproportionate pain remains a surgical emergency. [5]
[3]Controversies persist around the routine use of intravenous immunoglobulin for streptococcal toxic shock, the role of hyperbaric oxygen as an adjunct to surgery, the duration of antibiotics after debridement, and the optimal threshold for imaging in periorbital cellulitis. The Cochrane review of hyperbaric oxygen for necrotising fasciitis found insufficient evidence to recommend it universally, so it is reserved for centres with chambers and never delays surgery. Rising antimicrobial resistance in staphylococci and the variable regional prevalence of MRSA keep empiric antibiotic choice a live, locally calibrated decision. [11]
Exam Pearls
PAIN OUT red flags for necrotising infection
References
- [1]Stevens DL Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America. Clin Infect Dis, 2014.PMID 24947530
- [2]Hua C Necrotising soft-tissue infections. Lancet Infect Dis, 2023.PMID 36252579
- [3]McDermott J Necrotizing Soft Tissue Infections: A Review. JAMA Surg, 2024.PMID 39259555
- [4]Anaya DA Necrotizing soft-tissue infection: diagnosis and management. Clin Infect Dis, 2007.PMID 17278065
- [5]Wong CH The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med, 2004.PMID 15241098
- [6]Glennon CM Cellulitis in Pediatric Patients: Recognition and Management in the Era of Evolving Resistance. Am J Clin Dermatol, 2025.PMID 40259138
- [7]Wong SJ Management of pediatric orbital cellulitis: A systematic review. Int J Pediatr Otorhinolaryngol, 2018.PMID 29859573
- [8]Williams KJ Paediatric orbital and periorbital infections. Curr Opin Ophthalmol, 2019.PMID 31261188
- [9]Sanders JE Evidence-based management of skin and soft-tissue infections in pediatric patients in the emergency department. Pediatr Emerg Med Pract, 2015.PMID 25682652
- [10]Vayalumkal JV Children hospitalized with skin and soft tissue infections: a guide to antibacterial selection and treatment. Paediatr Drugs, 2006.PMID 16608371
- [11]Levett D Adjunctive hyperbaric oxygen for necrotizing fasciitis. Cochrane Database Syst Rev, 2015.PMID 25879088
- [12]Yueh CM Etiology, clinical features, management, and outcomes of skin and soft tissue infections in hospitalized children: A 10-year review. J Microbiol Immunol Infect, 2022.PMID 35283045