Paeds · infectious-diseases
Common viral exanthems, including roseola and erythema infectiosum
Also known as Roseola infantum · Exanthem subitum · Sixth disease · Human herpesvirus 6 infection · Erythema infectiosum · Fifth disease · Slapped cheek disease · Parvovirus B19 infection
Fellowship topic on the common benign viral exanthems of childhood, with roseola infantum (human herpesvirus 6 and 7) and erythema infectiosum (parvovirus B19) as the flagship entities. Covers the fever-versus-rash timing that anchors the diagnosis, the host-dependent parvovirus B19 disease spectrum (transient aplastic crisis in haemolytic anaemia, fetal hydrops in pregnancy, pure red cell aplasia in immunodeficiency), the rash differential that separates a self-limiting exanthem from meningococcal disease, Kawasaki disease and staphylococcal scalded skin, the selective use of serology and PCR, supportive management of the well child, urgent pathways for the high-risk contact, and the public-health layer of exclusion and counselling.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The numbered exanthems — a scaffold, not a list to recite
Overview & Definition
Picture an eighteen-month-old brought to the emergency department after three days of fever that has hovered around 39.5 °C. The parents are frightened by the height of the temperature, yet the child is reaching for toys and smiling between spikes, the observations are normal for age, and there is no focus on examination. You send them home with safety-net advice. That evening the fever breaks, and the next morning the mother phones in a panic: the child is covered in a rash. That sequence — high fever in a well child, then a rash appearing as the fever resolves — is roseola, and recognising it spares the child and family an avalanche of unnecessary tests and antibiotics. [6] [7]
Now picture a different child, a six-year-old sent home from school because of "slapped cheeks". She is afebrile and playing, her cheeks are an angry red that fades at the nose and mouth, and over the next two days a faint lacelike rash appears on her arms and the backs of her thighs. Her mother, twenty weeks pregnant, asks if it is dangerous. That is erythema infectiosum, and the question that matters is not about the child — she will be fine — but about her pregnant mother, because parvovirus B19 can cross the placenta and stop the fetal bone marrow making red cells. [1] [3]
A viral exanthem is a rash produced by a systemic viral infection, either by the virus damaging skin cells directly or, more often, by the immune response to the virus. The common viral exanthems of childhood are mostly benign, self-limiting illnesses that a clinician recognises from the morphology and the story, treats supportively, and uses as a chance to find and protect the vulnerable contact. This page owns the two flagship benign exanthems that do not have their own dedicated leaves — roseola (HHV-6 and HHV-7) and erythema infectiosum (parvovirus B19) — together with the reasoning that separates them from their dangerous mimics. Measles, rubella, varicella, hand-foot-and-mouth disease, Kawasaki disease and staphylococcal scalded skin syndrome each have their own pages; this one teaches you how to point a febrile rash towards the benign answer and, just as importantly, when to point it away. [1] [8]
Classification
Classify a childhood exanthem the way you actually use it at the bedside — by the fever-to-rash timing, by the organism, and by the danger the eruption signals — because each lens moves the thinking forward. The timing lens is the fastest and the most powerful. Some illnesses run fever first and produce the rash only as the fever settles, which is the roseola pattern. Others bring the rash out with the fever, as measles, rubella, varicella and hand-foot-and-mouth disease do. And a few declare the rash as the fever fades but in a recognisable sequence, as fifth disease does with its slapped cheek followed days later by the lacelike body rash. Get the timing right and you have narrowed the differential before you have touched the child. [2] [5]
The organism lens then names the cause and tells you what else to worry about. Roseola is HHV-6 and occasionally HHV-7; fifth disease is parvovirus B19. The non-polio enteroviruses produce a host of summer rashes, Epstein-Barr virus and adenovirus produce nonspecific morbilliform eruptions, and the vaccine-preventable and vesicular illnesses — measles, rubella, varicella — have their own dedicated pages because their prevention, complications and public-health weight set them apart. Placing the organism tells you the natural history, the incubation, and the complications to expect. [1] [9]
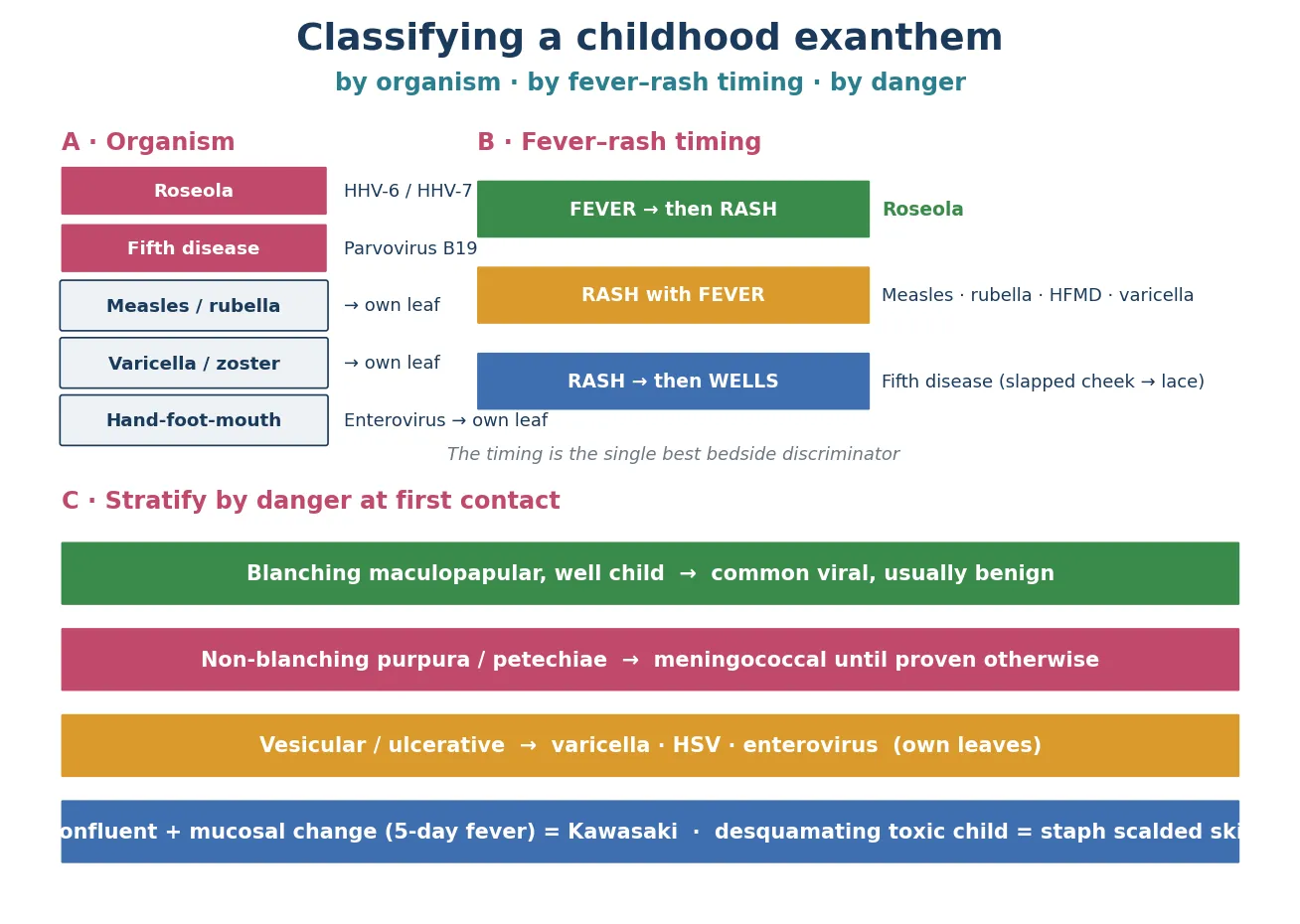
The danger lens is the one that protects the child, because a benign pattern can coexist with a fatal one. A blanching maculopapular rash in a well child points to a common viral exanthem. A non-blanching purpuric or petechial rash in a febrile child points to meningococcal disease until you prove otherwise, no matter what virus is circulating in the school. A vesicular or ulcerative eruption points to varicella, herpes simplex or enterovirus. And a confluent rash with mucosal change after five days of fever points to Kawasaki disease. Holding all three lenses at once — timing, organism, danger — is what lets you reassure with confidence on the benign pattern while staying alert to the mimic that would change everything. [1]
Epidemiology & Risk Factors
Human herpesvirus 6 is one of the most universal infections of early childhood. By two years of age almost every child has acquired it, most in the second six months of life as maternal antibody wanes, which is why roseola peaks in infants between six and twenty-four months old. HHV-6B causes almost all primary roseola; the virus spreads through saliva and respiratory secretions, so siblings, childcare and the endless mouthing of objects in infancy drive transmission. The population-based Seattle study found that HHV-6 was the most common single cause of febrile illness bringing infants to medical attention in the first two years, and that the fever was characteristically high and sustained. [7] [6]
Human herpesvirus 7 is a close relative that causes a minority of roseola cases, usually in slightly older children and often after HHV-6 has already been acquired. HHV-7 was identified later, and the comparison studies showed that primary HHV-7 infection can produce the same fever-then-rash picture but tends to be milder and later; the two viruses coexist in childhood populations and share the property of lifelong latency after primary infection. Knowing that HHV-7 exists matters for the exam because it explains why a child can appear to get roseola twice, and why the clinical label "roseola" does not always mean HHV-6. [9] [10]
Parvovirus B19 has a different epidemiology because it circulates in outbreaks. It spreads in winter and spring, mainly among primary-school children, with secondary attack rates of around fifty percent in households and classrooms. Roughly half of adults are immune by mid-adulthood, having acquired it in childhood, which means the other half remain susceptible — and the susceptible pregnant woman is where the morbidity and mortality of this virus live. The infectivity is highest in the days before the rash appears, which is the cruellest feature of fifth disease: by the time the slapped cheek is visible and the family seeks help, the child is no longer contagious, but the exposures that matter happened silently a week earlier. [1] [2]
The risk factors for severe disease are not about catching the virus but about the host who catches it. Parvovirus B19 is dangerous in three hosts. The fetus of a non-immune mother is at risk of hydrops because the virus halts fetal red-cell production during a period of massive erythropoiesis. The child with a chronic haemolytic anaemia — sickle cell disease, thalassaemia, hereditary spherocytosis, pyruvate kinase deficiency — is at risk of a transient aplastic crisis because the short red-cell lifespan cannot tolerate even a brief arrest in production. And the child with impaired immunity — HIV, transplantation, chemotherapy, primary immunodeficiency — is at risk of persistent pure red cell aplasia because the antibody response that would normally clear the virus never arrives. The same virus that causes a trivial cheek rash in one child causes fetal death or aplastic crisis in another, and that is the single most important idea in this topic. [1] [4]
For roseola, the principal risk is the height and duration of the fever, which is why HHV-6 is a leading cause of febrile seizures in infants. The seizure is driven by the fever, not by direct brain infection in the typical case, and the prognosis matches that of simple febrile seizures elsewhere — but the clinician still has to distinguish a benign HHV-6 seizure from meningitis or encephalitis, and HHV-6 is increasingly recognised as a rare cause of meningoencephalitis in its own right. [6] [8]
Pathophysiology
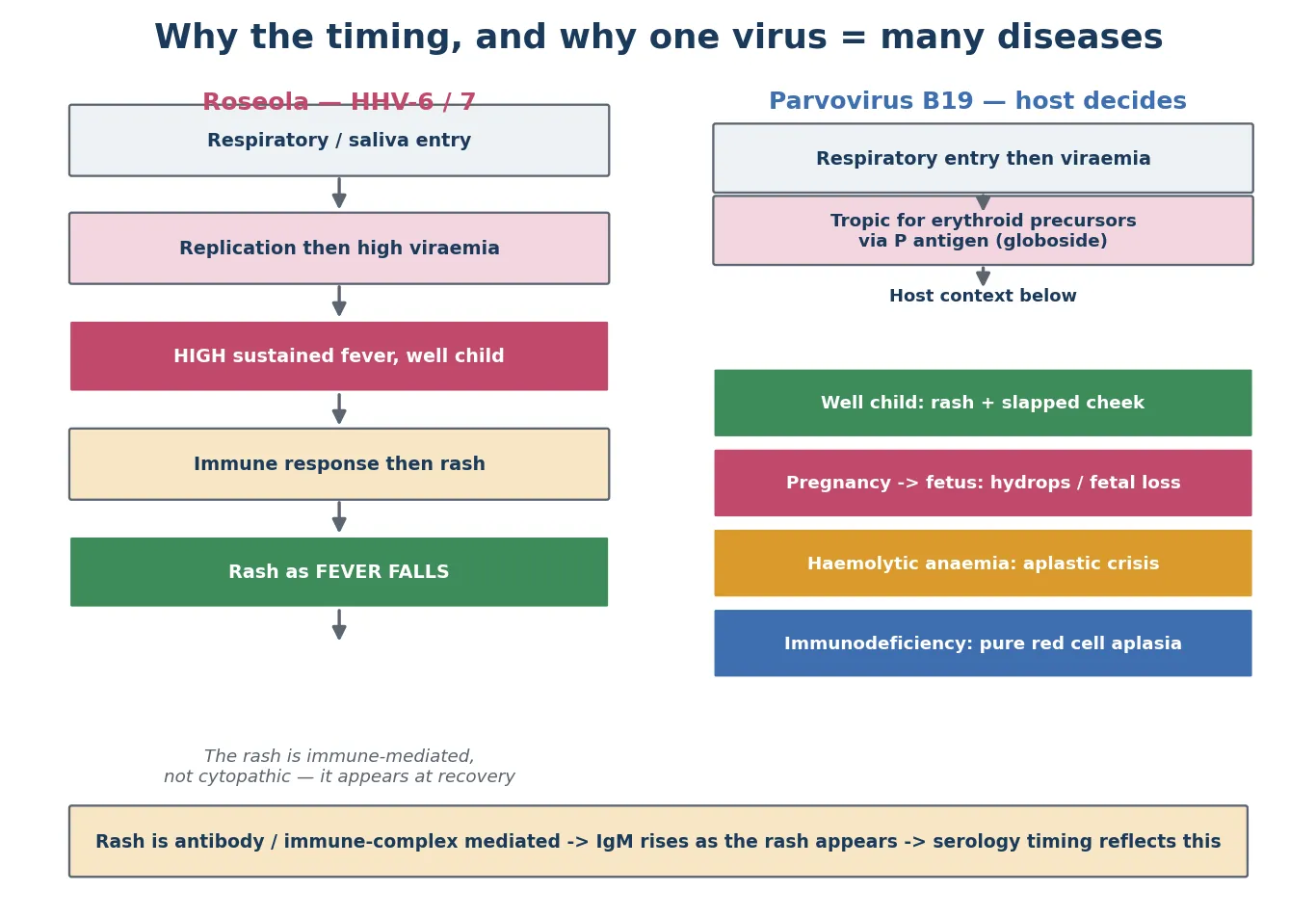
Why does roseola cause days of high fever and then a rash, when measles causes the rash while the fever is at its peak? The answer is in the biology of human herpesvirus 6, and it is worth understanding because it explains the timing that makes the diagnosis. The virus enters through the respiratory tract and spreads to regional lymph nodes, where it replicates in T-lymphocytes and monocytes. A high viraemia follows, and the viraemia is what drives the sustained fever — the child is hot because the virus is circulating in large amounts. The rash does not appear during the viraemia because it is not caused by virus damaging skin cells directly. It appears days later, as the immune response clears the virus, which is why it coincides with the fall in fever. The rash is an immune-mediated exanthem announcing recovery, not a sign of worsening. [5] [6]
That single insight — the roseola rash is immune-mediated and appears at recovery — reframes the frightened phone call from a parent whose child has just developed a rash as the fever breaks. Far from deteriorating, the child is recovering, and the rash is the immune system's signature on that recovery. It also explains why the child looks surprisingly well despite the height of the fever: the fever reflects viraemia, not tissue destruction, and the host is coping. [7] [8]
Parvovirus B19 works through a different and more dangerous mechanism that turns on its choice of cell. The virus uses the P blood group antigen, globoside, as its receptor, and globoside is abundant on erythroid progenitor cells in the bone marrow. Once inside, the virus halts red-cell production by killing the precursors. In a child with normal haemopoiesis and a normal red-cell lifespan of around one hundred and twenty days, this brief arrest is invisible — a few reticulocytes fail to be made, and the body's reserve easily covers it. The rash and the joint pains are not direct viral damage; they are immune-complex mediated, which is why they coincide with the appearance of antibody and why IgM rises as the rash appears. [1] [2]
Now follow parvovirus B19 into its dangerous hosts and the consequences fall out of the receptor biology. In a child with chronic haemolytic anaemia, the red-cell lifespan is short — perhaps fifteen to twenty days in sickle cell disease — so red-cell production is running at a furious baseline rate just to keep up. When parvovirus halts that production even briefly, the haemoglobin falls off a cliff, because there is no reserve and the surviving cells are being consumed at the usual high rate. That is the transient aplastic crisis: a precipitous, symptomatic anaemia with reticulocytes near zero, often the first manifestation of parvovirus in a child whose haemoglobinopathy was previously stable. [1]
In the fetus, the same receptor biology is catastrophic for a different reason. The fetal marrow is producing red cells at a tremendous rate to support rapid growth, the fetal red-cell lifespan is short, and the immature heart cannot compensate easily for a sudden fall in oxygen carriage. When parvovirus crosses the placenta and infects the fetal marrow, the fetus develops severe anaemia, then high-output cardiac failure, then hydrops — fluid accumulation in at least two compartments — and may die. The window for intervention is narrow, but a fetus with hydrops from parvovirus can be rescued by intrauterine transfusion, which is why recognising the maternal exposure matters so much. [3] [1]
And in the immunocompromised host, the virus cannot be cleared because the antibody response that would end the viraemia never develops. The result is persistent infection of the marrow and chronic pure red cell aplasia — an anaemia that does not resolve and that transfusion alone will not cure, because the virus keeps suppressing the precursors. Recognition that this is a treatable cause of chronic anaemia in AIDS and other immunodeficiencies was a landmark, because giving intravenous immunoglobulin supplies the antibodies the host cannot make and clears the infection. [4]
Clinical Presentation
The classic roseola story is so consistent that the diagnosis is often obvious in the telling. An infant between six and twenty-four months old runs a high fever, typically 39 to 40 °C, for three to five days. The striking feature is the mismatch between the height of the temperature and the appearance of the child, who remains alert, playful and interested in feeds between the fever spikes — what clinicians call a "happy well-looking febrile infant". There is no focus on examination: no otitis, no coryza pointing to a respiratory cause, no localising sign. Then the fever defervesces, and over the next few hours to a day a rash appears. [6] [7]
The roseola rash is discrete, rose-pink, blanching and maculopapular. It begins on the trunk and neck and spreads to the face and limbs, and it fades within hours to two days without scaling or pigment change. Because it appears as the fever falls, the family often interprets the rash as a sign of deterioration and presents at exactly the moment the illness is resolving. Recognising the pattern — high fever ending as the rash begins — lets you reassure and avoid unnecessary investigation, and it is the contrast with the rash-with-fever illnesses that makes the pattern so diagnostic. Less commonly, HHV-6 primary infection presents without the rash, as an undifferentiated febrile illness, or with cervical and occipital lymphadenopathy, mild eyelid oedema, or a bulging fontanelle. [6] [8]
[6] [5]Erythema infectiosum tells a different story, and its two-phase rash is its signature. A school-age child may have a brief prodrome of low-grade fever, headache and mild coryza. Then the cheeks flush an intense, fiery red — the "slapped cheek" appearance — classically sparing the nasal bridge and the skin around the mouth, so the child has a pale circumoral ring framing the red cheeks. One to four days later, a pink maculopapular rash appears on the trunk, arms, buttocks and the extensor surfaces of the thighs and rapidly takes on a characteristic lacelike or reticulate pattern as the central portions clear. [1] [2]
The lacelike rash of fifth disease has a behaviour the family needs to know about, because it causes needless anxiety and repeat visits. It fluctuates. Heat, sunlight, exercise, emotion and bathing can bring it back or intensify it days or weeks after it first seemed to resolve, and these recurrences are not signs of new infection or treatment failure — they are a post-infectious immune phenomenon. The rash may flicker on and off for weeks, and the child is well throughout. Knowing this lets you reassure with precision rather than hedging. [1]
Parvovirus B19 also produces a symmetric small-joint arthropathy that is common in adolescents and adults, especially females, and uncommon in young children. It affects the hands, wrists, knees and ankles, can mimic juvenile idiopathic arthritis in its acute phase, and usually resolves within weeks, though in adults it can persist for months. A teenager with acute symmetric small-joint pain and a recent fifth-disease exposure has parvovirus arthropathy until shown otherwise, and the reassurance is that it is self-limiting in children. [1]
The atypical and severe presentations are the ones that test the clinician. An infant with HHV-6 can present with a febrile seizure, and rarely with meningoencephalitis, hepatitis or a picture mimicking the Kawasaki pattern. A child with sickle cell disease and parvovirus B19 presents not with a rash but with acute pallor, fatigue, breathlessness and a haemoglobin far below baseline — the aplastic crisis. The rare papular-purpuric gloves-and-socks syndrome presents with painful pruritic papules and purpura on the hands and feet. And the fetus presents, weeks after the maternal exposure, with hydrops on an ultrasound — a presentation the obstetric team will attribute to parvovirus only if someone thought to test the mother. [3] [8]
Differential Diagnosis
The differential for a febrile infant whose fever precedes a rash is short, and roseola sits at its head. Measles is the chief alternative, but measles does not look like roseola in the febrile phase: the measles child has coryza, cough and conjunctivitis — the three C's — and Koplik spots on the buccal mucosa, and the rash descends from the hairline as the fever is rising, not falling. Rubella causes a milder fever with postauricular and suboccipital lymphadenopathy and a pink rash that spreads quickly. The enteroviruses produce a bewildering variety of summer rashes, often with pharyngitis or a hand-and-foot component. Get the timing and the prodrome right and these separate cleanly. [2] [5]
The differential for a red-cheeked child is broader. Erythema infectiosum is the prototype, but a slapped cheek can be sunburn, or cellulitis, or the sandpaper rash of scarlet fever accompanied by a strawberry tongue and a fever. Systemic lupus erythematosus causes a malar rash, but it spares the nasolabial folds and comes with systemic disease in an adolescent, not an acute self-limiting illness in a primary-school child. The distribution matters: fifth disease spares the perioral skin and favours the extensor surfaces with its lacelike pattern, which is hard to mimic. [1]
[1] [2]The dangerous mimics are the ones this whole topic exists to protect against, because each is treatable if caught and lethal if missed. A febrile child with a non-blanching purpuric or petechial rash has meningococcal disease until proven otherwise, full stop — the existence of a fifth-disease epidemic in the school changes nothing. A child with five or more days of fever plus conjunctivitis, red cracked lips, a strawberry tongue, a polymorphous rash and extremity changes has Kawasaki disease, and the price of mistaking it for a benign viral exanthem is a coronary artery aneurysm. A toxic, irritable child with tender skin and superficial peeling may have staphylococcal scalded skin syndrome. And a child on a new drug with a rash, fever, facial oedema, lymphadenopathy and internal organ involvement has a drug reaction with eosinophilia and systemic symptoms, which can be fatal. [1]
The lesser-known pattern rashes deserve a mention because they appear in differential questions. Gianotti-Crosti syndrome is an acral papular eruption on the cheeks, buttocks and extensor limbs of young children, classically following hepatitis B in older descriptions but more often linked to Epstein-Barr virus today, and it runs a self-limiting course. Unilateral laterothoracic exanthem begins around the axilla and spreads centrifugally on one side before becoming bilateral, again self-limiting. These pattern rashes are benign but worth naming because they complete the picture of the common viral exanthems. [1] [8]
For the pregnant contact, the differential is not about the child's rash but about the mother's immune status, and the only way to resolve it is serology. A pregnant woman exposed to fifth disease is either immune — prior infection, IgG positive, no risk — or susceptible, IgG negative, at risk of primary infection and its fetal consequences. That single distinction, made on a blood test, determines whether she gets reassurance or a fetal-medicine referral, which is why asking about pregnancy contacts is part of every fifth-disease encounter. [3]
Clinical & Bedside Assessment
The assessment begins with a focused history built around the fever-rash relationship, because that relationship usually makes the diagnosis. Ask how many days of fever preceded the rash, and pin down whether the rash appeared while the fever was climbing or as it was falling. Ask what the child looked like during the fever — a happy, playful infant despite 39.5 °C points strongly to roseola, while a toxic, irritable child points away from it. Ask about the morphology and distribution: discrete blanching trunk papules, slapped cheeks with perioral sparing, a lacelike reticulate eruption, or something that does not blanch. [6] [1]
The host context is the part of the history that changes everything, so ask for it explicitly. Is anyone in the household pregnant? Does the child have sickle cell disease, thalassaemia or any other chronic anaemia? Is the child immunocompromised — chemotherapy, transplant, HIV, primary immunodeficiency, or on immunosuppressive drugs? These three questions, asked every time, are what convert a routine reassurance into a life-saving referral. The child with fifth disease who is sent home without anyone asking about a pregnant mother is the child whose fetal sibling develops hydrops three weeks later. [3] [1]
Examine for the red flags that exclude a benign viral exanthem, and document that you looked. Does the rash blanch? Press a clear glass or a finger against a lesion and look through the skin — a blanching maculopapular rash fits the common viral pattern, but a non-blanching purpuric rash in a febrile child is meningococcal disease until proven otherwise. Is the child's conscious state normal? Meningism, a bulging fontanelle, or a drowsy irritable child demand a sepsis and meningitis workup rather than reassurance. Are there mucocutaneous features of Kawasaki disease — non-purulent conjunctivitis, red cracked lips, a strawberry tongue, extremity changes? And is there pallor, breathlessness or signs of high-output cardiac failure that suggest aplastic crisis in an at-risk child? [1]
Document the morphology and distribution precisely, because for these exanthems the pattern is the diagnosis. "Slapped cheek with perioral sparing followed by a lacelike reticulate rash on the extensor surfaces" is fifth disease. "Three to five days of high fever in a well infant, then discrete blanching trunk maculopapules as the fever fell" is roseola. Vague descriptions like "a viral rash" or "some spots" do not help you or the next clinician, and they leave no record that you distinguished the benign pattern from its dangerous mimics. The quality of the documented description is, for these illnesses, the quality of the diagnosis. [2]
Capture the public-health essentials before the family leaves. Who else is in the household, and is any of them pregnant? Where does the child go to school or childcare, and are there other cases? When did the rash start, and when was the child last well enough to attend? Fifth disease is most contagious before the rash appears, so a child currently showing the rash has already exposed their contacts — the tracing question is about the preceding week, not the day of presentation. These details drive the counselling and the contact follow-up that close the encounter properly. [1]
Investigations
Recognise that roseola and erythema infectiosum are clinical diagnoses in the typical well child, and that ordering panels of tests on an obvious benign exanthem is a failure of reasoning, not thoroughness. A well-looking infant whose high fever has just resolved as a typical rash appeared needs no blood tests — the diagnosis is the story. A school-age child with classic slapped cheeks and a lacelike rash needs no swabs or serology to confirm fifth disease for their own sake. The temptation to investigate "to be sure" usually reflects discomfort with clinical diagnosis, and it exposes the child to needles and the family to anxiety without changing management. [6] [1]
Parvovirus B19 serology is reserved for the situations where the answer changes management, and the most important of these is the pregnant contact. IgM indicates recent or acute infection and appears as the rash appears, persisting for two to three months, so a positive IgM in an exposed pregnant woman means recent infection and triggers fetal surveillance. IgG indicates past infection and immunity, so a positive IgG with negative IgM in an exposed woman means she is protected and the fetus is safe. This single pair of results, read correctly, is the fulcrum of the pregnancy pathway. [3] [1]
Parvovirus B19 PCR, which detects viral DNA, has a different role. It is the test of choice in the immunocompromised host, who may not mount a detectable antibody response and in whom persistent viraemia rather than serology defines the disease. PCR is also used to confirm fetal infection by testing amniotic fluid or fetal blood, and to diagnose the aplastic crisis when the clinical picture is atypical. In the well child with classic fifth disease, PCR adds nothing that the clinical pattern has not already given you. [4] [2]
Check a full blood count and reticulocyte count whenever parvovirus B19 meets a haemoglobinopathy. The transient aplastic crisis shows a precipitous haemoglobin fall — often far below the child's baseline — with reticulocytes near zero, because the marrow has stopped producing red cells. The haemoglobin can drop low enough to cause high-output cardiac failure, and the reticulocytopenia is the laboratory fingerprint that distinguishes aplastic crisis from a haemolytic crisis, in which reticulocytes would be high. In any child with chronic haemolytic anaemia and a sudden drop in haemoglobin, parvovirus B19 is the presumed cause until proven otherwise. [1]
In the febrile, unwell infant or child where a dangerous mimic cannot be excluded, investigate for sepsis and meningitis — the benign diagnosis is made only after the dangerous one is ruled out. A non-blanching rash, meningism, a toxic appearance, or an infant under a month with fever demands blood cultures, a full blood count, inflammatory markers, and a lumbar puncture where appropriate, with empirical antibiotics. The point of this topic is not to make clinicians cavalier about febrile rashes; it is to make them confident about the benign ones once the dangerous ones have been excluded. [1] [8]
Management — Resuscitation
Resuscitation is about the hosts in whom a benign exanthem is a warning of a medical emergency, and there are four of them. The first is the non-immune pregnant woman exposed to parvovirus B19, whose fetus is at risk of hydrops and death. The second is the child in transient aplastic crisis, whose haemoglobin has fallen off a cliff. The third is the immunocompromised child with persistent parvovirus anaemia, who cannot clear the virus alone. The fourth is any febrile child with a non-blanching rash or meningism, in whom the working diagnosis is sepsis or meningitis, not a viral exanthem. Each reframes the encounter from reassurance to action. [3] [4]
Manage parvovirus B19 transient aplastic crisis as the haematological emergency it is. Take blood urgently for a full blood count and reticulocytes, cross-match, and transfuse red cells for severe symptomatic anaemia, because the precipitous haemoglobin fall can be life-threatening in a child whose baseline is already low. Involve the haemato-oncology team early, watch for the complications of severe anaemia and transfusion, and remember that the child will recover marrow function as the virus clears — the crisis is transient, and most children do not need long-term support once they have been tided over. [1]
Refer the parvovirus B19-exposed non-immune pregnant woman urgently rather than reassuring her. The pathway is serology to confirm susceptibility, then serial fetal ultrasound for ten to twelve weeks after the infection looking for signs of hydrops — ascites, pleural or pericardial effusions, skin oedema, polyhydramnios — and referral to fetal medicine for intrauterine transfusion if hydrops develops. The stakes are a live fetus that can be saved by a transfusion versus a stillbirth that no one saw coming, and the difference is whether the exposure was recognised and the mother was referred. [3]
Treat HHV-6 febrile seizures the way you treat any simple febrile seizure: protect the airway, position the child, and give antipyretics. Most seizures self-terminate within minutes, and the child recovers promptly. Escalate for a complex seizure — prolonged, focal, or recurring within twenty-four hours — a prolonged postictal state, or any sign of meningoencephalitis, which demands a septic workup, an electroencephalogram and neuroimaging. The family needs reassurance that a simple HHV-6 febrile seizure is benign, and clear safety-net advice about what would bring them back. [6] [8]
For the well child, supportive care is the treatment: paracetamol for comfort and to bring the fever into a range the child can tolerate, fluids to maintain hydration, and reassurance. There is no antiviral for HHV-6 or HHV-7 in routine use, and none is needed, because the illness resolves on its own. The safety-net is the part of supportive care that closes the loop: tell the family exactly what would bring them back — a non-blanching rash, a fever that does not resolve, drowsiness, breathing difficulty, or any concern that a pregnant household contact has been exposed. [7] [1]
Management — Definitive & Stepwise
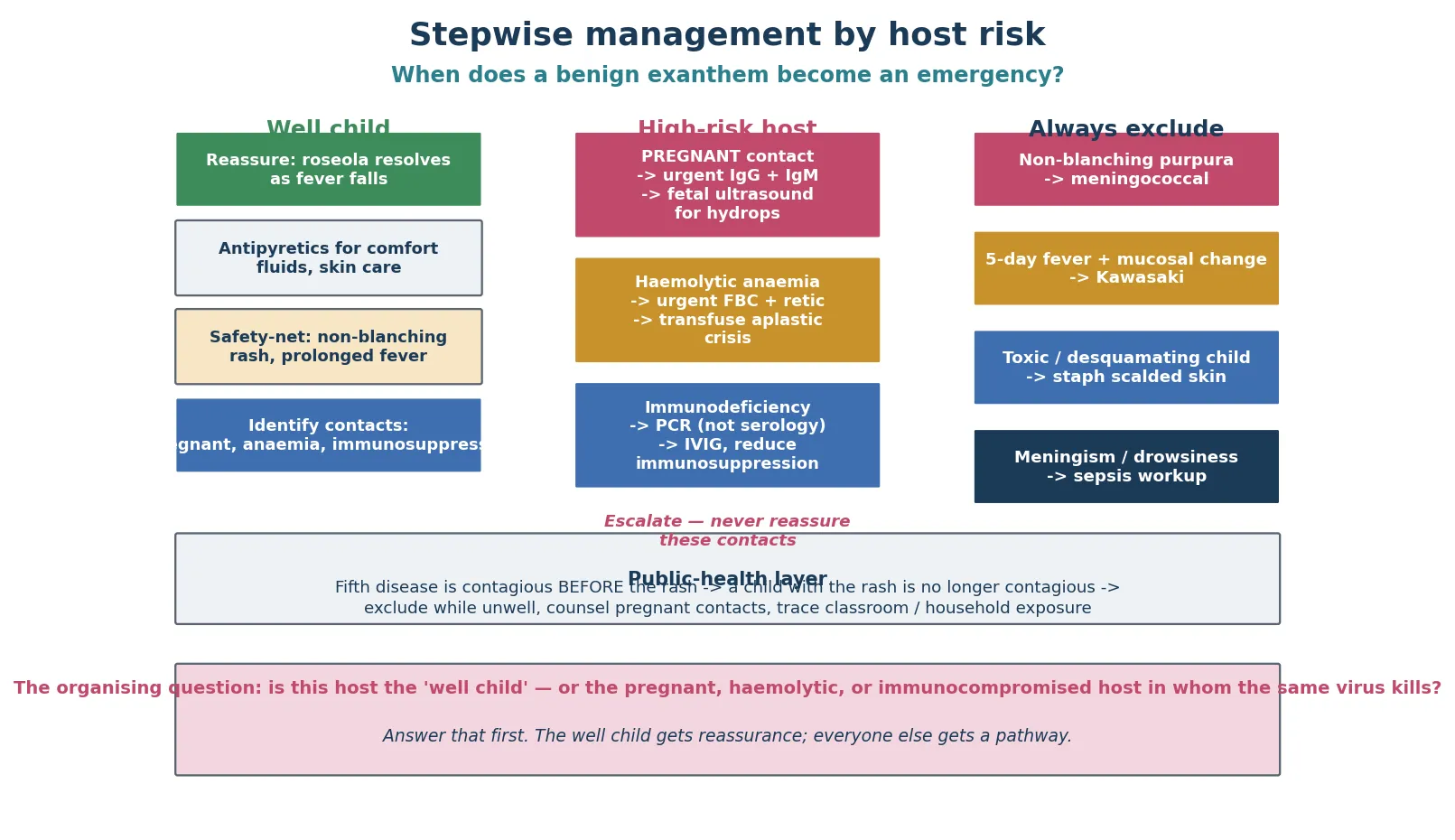
Definitive management runs as a stepwise pathway matched to the host, because the same virus needs completely different management in different people. For the well child, the answer is reassurance and supportive care. For the non-immune pregnant contact, the answer is urgent serology and fetal-medicine referral. For the child with aplastic crisis, the answer is transfusion and haematology. For the immunocompromised host with persistent parvovirus, the answer is intravenous immunoglobulin and reduction of immunosuppression. Holding the host in mind at the first contact is what keeps each of these pathways on track. [1]
The stepwise exanthem pathway
Ask the host questions first: any pregnancy in the household? Any chronic haemolytic anaemia? Any immunodeficiency? These three questions reframe a routine rash encounter.
Decide the danger at the bedside: does the rash blanch? Is the child's conscious state normal? Are there mucocutaneous features of Kawasaki disease? Non-blanching purpura or a toxic child triggers a sepsis workup, not reassurance.
Match the pattern: fever-then-rash in a well infant is roseola; slapped cheek with a lacelike body rash is fifth disease. The well child needs no tests.
Manage the well child with reassurance, antipyretics, fluids and a safety-net; for fifth disease, advise the family that the rash may fluctuate for weeks and is not a sign of ongoing infection.
Refer the high-risk contacts: pregnant contact for serology and fetal surveillance; haemolytic anaemia for full blood count, reticulocytes and transfusion; immunocompromised host for PCR and intravenous immunoglobulin.
Run the public-health layer: exclude the unwell child from school per local guidance, counsel pregnant contacts, and trace classroom and household exposures — remembering fifth disease is contagious before, not after, the rash.
For the well child with roseola, the management message is reassurance grounded in the mechanism. Explain that the high fever was the virus circulating, that the child looked well because the illness was not destroying tissue, and that the rash appears now because the fever has gone and the immune system is clearing the virus — so the rash is a sign of recovery, not of deterioration. Antipyretics given for comfort, fluids to maintain hydration, and a clear safety-net complete the care. The defervescence is the resolution, and the family can be told that confidently. [6] [7]
For the well child with erythema infectiosum, the management has an extra layer of counselling because of the contacts. Reassure about the benign course and the fluctuating rash. Ask explicitly about pregnancy in the household and advise the family to inform any pregnant contacts to seek advice. Explain the paradox that defines fifth disease: the child is contagious before the rash and no longer contagious once the rash appears, so a child with the visible rash does not need to be excluded on grounds of infectivity, though schools and local guidance vary on exclusion while the child is systemically unwell. [1]
For parvovirus B19 in pregnancy, follow the fetal-medicine pathway precisely. Confirm maternal immune status with IgG and IgM. If the mother is immune, reassure her — the fetus is protected. If she is non-immune and seroconverts, arrange serial fetal ultrasound for ten to twelve weeks after the infection to detect hydrops, and refer to fetal medicine for consideration of intrauterine transfusion when hydrops develops. The outcome with timely transfusion can be excellent, which is the most important thing to convey to an anxious mother: this is a problem that can be detected and treated. [3]
For the immunocompromised host with persistent parvovirus B19 pure red cell aplasia, the treatment is intravenous immunoglobulin, which supplies the neutralising antibodies the host cannot make, combined with reduction of immunosuppression where feasible. The diagnosis rests on PCR showing persistent viraemia rather than serology, and the response is often dramatic as the donor antibody clears the marrow infection. This is one of the great treatable causes of chronic anaemia in immunodeficiency, and missing it condemns the child to ongoing transfusion dependence. [4]
Specific Subtypes & Scenarios
A well infant with three days of high fever, then a trunk rash as the fever resolves. This is classic roseola, and the encounter is a masterclass in confident clinical diagnosis. Examine to exclude a focus and to confirm the child is well, document the fever-then-rash pattern, reassure the family that the rash is the recovery phase, and give a safety-net. No tests, no antibiotics, no follow-up unless the family has concerns. The temptation to investigate "to be sure" should be resisted — the diagnosis is the story. [6] [7]
A school-age child with red cheeks and a lacelike rash. This is classic erythema infectiosum. Confirm the perioral sparing and the reticulate extensor pattern, reassure, and — the non-negotiable step — ask about pregnancy in the household and advise on school guidance. Explain that the rash may come and go for weeks with heat and bathing, that this is expected, and that the child is no longer contagious now the rash is visible. The visit is mostly counselling, done well. [1] [2]
A child with sickle cell disease and sudden pallor. This is parvovirus B19 transient aplastic crisis until proven otherwise, and it is a haematological emergency. The child may not have a rash at all — the aplastic crisis often occurs without the classic exanthem — and presents instead with acute anaemia: pallor, fatigue, breathlessness, sometimes high-output cardiac failure. Check the haemoglobin and reticulocytes urgently, cross-match, transfuse for severe symptomatic anaemia, and involve haemato-oncology. The reticulocytopenia is the fingerprint. [1]
A non-immune pregnant woman exposed to a child with fifth disease. This is the scenario where early action saves a fetus. Take a careful exposure history and confirm the timing, send IgG and IgM, and refer the seronegative or seroconverting woman to fetal medicine for serial ultrasound surveillance over the next ten to twelve weeks. If hydrops develops, intrauterine transfusion is the intervention that can rescue the fetus. The whole pathway hangs on one thing: someone thought to ask whether the woman was pregnant. [3]
An immunocompromised child with persistent anaemia. This is parvovirus B19 pure red cell aplasia, a treatable cause of chronic anaemia in immunodeficiency that is missed when serology alone is relied on, because the host cannot make the antibody. Diagnose with PCR showing persistent viraemia, treat with intravenous immunoglobulin, and reduce immunosuppression where possible. The response confirms the diagnosis and relieves the transfusion dependence. [4]
An infant with HHV-6 and a febrile seizure. Manage the seizure and the fever as for any simple febrile seizure, and consider a sepsis and meningitis workup in the unwell or atypical infant, the child with a complex seizure, or any child with meningism or a prolonged postictal state. Reassure the family about the generally excellent prognosis of simple febrile seizures, and give a clear safety-net. The seizure is driven by the height of the fever, and the HHV-6 illness will resolve as the viraemia clears. [6] [8]
Complications & Pitfalls
The parvovirus B19 complications are best remembered by the host they strike, because the same virus produces completely different complications in different people. In a child with chronic haemolytic anaemia, parvovirus causes a transient aplastic crisis — a sudden, dangerous arrest of red-cell production that can precipitate heart failure. In a non-immune pregnant woman, it causes fetal infection that can progress to hydrops and intrauterine death. In an immunocompromised host, it causes persistent pure red cell aplasia. In a well child it causes a rash and sometimes an arthropathy, and in the rare papular-purpuric gloves-and-socks syndrome it causes painful purpuric lesions on the hands and feet. The complication follows the host. [1] [4]
The HHV-6 complications are fewer but real. Because the fever is high and sustained, HHV-6 is a leading cause of febrile seizures in infants, and the clinician has to distinguish a simple seizure from meningitis or encephalitis. HHV-6 is a rare but recognised cause of meningoencephalitis and hepatitis, and it has been implicated in bone-marrow suppression and in mimicking drug reaction with eosinophilia and systemic symptoms. Most of these are rare; the febrile seizure is common, and it is the one the exam will test. [6] [8]
The first pitfall is reassuring a non-immune pregnant contact without serology and referral. Fetal hydrops from parvovirus is a preventable loss if surveillance catches it and intrauterine transfusion is delivered in time, and the only thing standing between recognition and loss is whether someone asked the pregnancy question and acted on it. Every fifth-disease encounter should include a documented question about household pregnancy, and any positive answer should trigger the pathway. [3]
The second pitfall is missing Kawasaki disease behind a febrile viral exanthem. Kawasaki disease is treated within ten days of fever onset to prevent coronary artery aneurysms, and it presents with fever plus mucocutaneous features that can be dismissed early on as a viral illness. A child with five or more days of fever and any of conjunctivitis, red cracked lips, a strawberry tongue, a polymorphous rash, or extremity changes needs Kawasaki assessment, inflammatory markers and an echocardiogram — not reassurance that "it's just a virus". The cost of the error is a coronary aneurysm in a child. [1]
The third pitfall is missing meningococcal disease behind a viral exanthem during a school outbreak. When fifth disease or roseola is going around, the temptation to attribute any febrile rash to "the virus going round" is strong, and it is exactly when meningococcal disease is missed. A febrile child with a non-blanching rash has meningococcal disease until proven otherwise, regardless of what else is circulating. The glass test is not a courtesy — it is the test that separates the lethal diagnosis from the benign one. [1]
The fourth pitfall is attributing prolonged parvovirus rash recurrence to ongoing infection or treatment failure. The fluctuating rash of fifth disease is a post-infectious immune phenomenon, provoked by heat, sunlight and exercise, and it is not contagious and does not need treatment. Families frightened by a rash that keeps coming back need a confident explanation that this is expected and benign, not a repeated course of reassurance that hedges. [1]
Prognosis & Disposition
Roseola resolves completely within days of defervescence, with the rash fading in hours to two days and the child returning to normal immediately. The long-term consequence of HHV-6 and HHV-7 infection is lifelong latent infection, integrated into the host genome in a minority of people and reactivating rarely and usually silently. The prognosis in the well child is excellent, and the disposition is home with a safety-net. The febrile seizures associated with HHV-6 carry the prognosis of simple febrile seizures generally — benign in the short and long term. [7] [9]
Erythema infectiosum in the well child is benign and self-limiting, with the rash fluctuating for weeks and the child remaining well throughout. The prognosis is determined entirely by the host: in the well child it is trivial; in pregnancy it can be devastating to the fetus; in haemolytic anaemia it can be life-threatening; in immunodeficiency it can be chronic and debilitating. Disposition follows the host — home for the well child, urgent referral for the pregnant contact, admission for the aplastic crisis, specialist management for the immunocompromised host. [1]
The parvovirus B19 arthropathy in children is usually brief and resolves without chronic sequelae, in contrast to adults in whom it can persist for months. A child with acute symmetric small-joint pain after fifth disease can be reassured that it will settle, and juvenile idiopathic arthritis is not triggered by a single parvovirus episode. This matters because the arthropathy is frightening to families who fear a chronic rheumatological disease, and the reassurance is specific and correct. [1]
Discharge planning for the well child is straightforward but must close the loop. Identify and counsel any high-risk contacts before the family leaves — pregnancy, chronic anaemia, immunodeficiency — because the encounter is incomplete if a pregnant mother goes home unprotected. Complete the exclusion period per local guidance while the child is unwell, and give a clear safety-net for the features that demand return: a non-blanching rash, prolonged fever, drowsiness, breathing difficulty, pallor, or a pregnant contact who needs assessment. Reinforce that the recovered child with fifth disease is no longer contagious. [1] [8]
The overarching prognosis message is that these are benign illnesses in the right host, and the clinician's job is to confirm that the host is the right one. Once the dangerous mimics are excluded and the high-risk contacts are protected, the well child can be reassured confidently, and that confidence — grounded in the pattern and the mechanism — is itself therapeutic for a frightened family. [2]
Special Populations
Pregnant women exposed to parvovirus B19 are the highest-stakes special population in this topic, because the consequence of inaction is fetal death. Determine immune status urgently with IgG and IgM. An immune woman can be reassured. A non-immune woman who seroconverts needs serial fetal ultrasound for ten to twelve weeks to detect hydrops and referral to fetal medicine for intrauterine transfusion if it develops. The message to carry is that a fetus with parvovirus hydrops can be saved — but only if the exposure was recognised and the pathway was activated. [3] [1]
Children with chronic haemolytic anaemia — sickle cell disease, thalassaemia, hereditary spherocytosis, pyruvate kinase deficiency — are at risk of parvovirus B19 transient aplastic crisis. Any febrile illness with acute pallor, fatigue, breathlessness or a falling haemoglobin in such a child warrants an urgent full blood count and reticulocyte count and transfusion for severe anaemia. The aplastic crisis may be the first presentation of parvovirus in a child whose haemoglobinopathy was previously stable, and the reticulocytopenia is the diagnostic fingerprint. [1]
Immunocompromised children — HIV and AIDS, solid-organ and stem-cell transplant, chemotherapy, primary immunodeficiency — are at risk of persistent parvovirus B19 pure red cell aplasia because they cannot mount the antibody response that clears the virus. Diagnose with PCR showing persistent viraemia rather than serology, and treat with intravenous immunoglobulin and reduction of immunosuppression. This is one of the great treatable causes of chronic anaemia in immunodeficiency, and recognising it transforms a transfusion-dependent child into one who clears the virus. [4]
Infants under two are the principal population for roseola, and the high fever frequently prompts a sepsis evaluation in the young infant. The clinician has to balance the well-looking febrile infant rule — that a well appearance does not exclude serious infection in the very young — against the recognition that HHV-6 is the commonest cause of fever in this age group and that the pattern is characteristic. In the infant under three months, or any unwell infant, the default remains a septic workup; in the older well infant with the classic pattern, confident clinical diagnosis is appropriate with a safety-net. [6] [7]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children, and refugee, asylum-seeking and migrant families deserve equitable access to diagnosis, maternal parvovirus surveillance in pregnancy, and haemoglobinopathy screening that identifies the haemolytic-anaemia risk before a crisis occurs. Sickle cell disease and thalassaemia are over-represented in some of these populations, which raises both the chance of an aplastic crisis and the importance of recognising it. Use interpreters, provide culturally safe care, and ensure that disadvantage never delays recognition of the dangerous host or the activation of the pregnancy pathway. [1]
Evidence, Guidelines & Regional Differences
The discovery that human herpesvirus 6 causes roseola was a landmark of modern paediatric infectious disease, reported by Yamanishi and colleagues in 1988. They isolated the virus from the blood of children with exanthem subitum and showed that antibody rose as the illness resolved, anchoring a clinical syndrome that had been recognised for decades to its organism. That paper is the foundation of everything that follows on roseola, and it is worth citing because it is the moment roseola stopped being a pattern and became a disease with a cause. [5]
The natural history of primary HHV-6 infection was defined by Hall and colleagues in their 1994 prospective study, which documented the complications and the reactivation of HHV-6 in children and established the high fever, the febrile-seizure burden, and the characteristic course. Zerr and colleagues then provided the population-based epidemiology in their 2005 New England Journal paper, showing that HHV-6 is acquired by almost all children by age two and that it is the commonest cause of febrile illness bringing infants to medical attention. Together these papers define roseola as a clinical and epidemiological entity. [6] [7]
The parvovirus B19 literature is anchored by two definitive reviews. Young and Brown's 2004 New England Journal review lays out the biology, the clinical disease and the host-dependent complications in the form the exam expects, and Heegaard and Brown's 2002 Clinical Microbiology Reviews article provides the microbiological depth. For the pregnancy pathway, Enders and colleagues' 2010 study of the risk of fetal hydrops and non-hydropic late intrauterine fetal death after gestational parvovirus B19 infection defines the fetal risk that the pathway is built to detect and treat. [1] [2]
For the immunocompromised host, Frickhofen and colleagues' 1990 paper established persistent parvovirus B19 infection as a treatable cause of chronic anaemia in AIDS, which generalised to other immunodeficiencies and underpins the use of intravenous immunoglobulin today. The HHV-7 literature — Hall and colleagues' 2006 paper and Caserta and colleagues' 1998 comparison of HHV-7 and HHV-6 — completes the picture of the roseoloviruses and explains why a child can appear to get roseola twice. [4] [9] [10]
The controversies in this topic are practical and recurring. Whether school exclusion for erythema infectiosum has any value is contested, because the child is contagious before the rash and no longer contagious once it appears — many guidelines therefore exclude only while the child is systemically unwell, rather than for a fixed period after the rash. The role of intrauterine transfusion at the extremes of gestation and hydrops severity continues to be refined, and fetal-medicine judgement drives the decision. The diagnostic value of HHV-6 PCR in central nervous system disease is complicated by chromosomally integrated HHV-6, which produces high viral loads in blood without active infection. And the global equity of access to maternal parvovirus surveillance and intrauterine transfusion remains a real gap, with fetal loss from parvovirus still common where surveillance is unavailable. [3] [8]
Exam Pearls
- Roseola (sixth disease) is HHV-6 and sometimes HHV-7: high fever for three to five days in a well-looking infant, then a rash as the fever falls. Fever-then-rash is the key, and it is the opposite of measles. [5] [6]
- Erythema infectiosum (fifth disease) is parvovirus B19: slapped cheeks with perioral sparing, then a lacelike reticulate trunk and limb rash that fluctuates for weeks with heat and sunlight. [1]
- Parvovirus B19 is tropic for erythroid precursors via the P antigen (globoside) — the host decides the disease: well child (rash), haemolytic anaemia (aplastic crisis), fetus (hydrops), immunodeficiency (pure red cell aplasia). [1]
- Fifth disease is contagious before the rash appears; the child with the rash is no longer contagious — school exclusion once the rash is out has little value beyond the period the child is unwell. [2]
- A non-immune pregnant contact of parvovirus B19 needs urgent IgG and IgM, fetal ultrasound for hydrops, and possible intrauterine transfusion — never reassure without serology. [3]
- Transient aplastic crisis in a child with sickle cell disease: precipitous haemoglobin fall and reticulocytopenia — transfuse urgently and involve haemato-oncology. [1]
- HHV-6 is a leading cause of febrile seizures in infants because the fever is high and sustained — manage the seizure, exclude meningitis in the atypical case, reassure on prognosis. [6]
- Never miss the dangerous mimics behind a benign exanthem: non-blanching purpura (meningococcal), five-day fever with mucocutaneous change (Kawasaki), toxic desquamating child (staphylococcal scalded skin). [1]
- The numbered exanthems: measles (first), scarlet fever (second), rubella (third), fourth (disputed), erythema infectiosum (fifth), roseola (sixth) — a memory scaffold, not a list to recite. [2]
- Diagnose these benign exanthems clinically; serology is for the pregnant contact and the atypical case, and PCR is for the immunocompromised host. [4]
- Persistent parvovirus B19 in immunodeficiency is a treatable cause of chronic anaemia — diagnose with PCR, treat with intravenous immunoglobulin. [4]
- HHV-7 causes a minority of roseola, usually later and milder — explains "second" roseola and rounds out the roseolovirus picture. [9] [10]
References
- [1]Young NS; Brown KE Parvovirus B19. N Engl J Med, 2004.PMID 14762186
- [2]Heegaard ED; Brown KE Human parvovirus B19. Clin Microbiol Rev, 2002.PMID 12097253
- [3]Enders M; Klingel K; Weidner A; Baisch C; Kandolf R; Schalasta G; Hentschel R; Jilg W; Modrow S Risk of fetal hydrops and non-hydropic late intrauterine fetal death after gestational parvovirus B19 infection. J Clin Virol, 2010.PMID 20729141
- [4]Frickhofen N; Abkowitz JL; Safford M; Berry JM; Antunez-de-Mayolo J; Astrow A; Cohen R; Halperin I; King L; Mintzer D; et al Persistent B19 parvovirus infection in patients infected with human immunodeficiency virus type 1 (HIV-1): a treatable cause of chronic anemia in AIDS. Ann Intern Med, 1990.PMID 2173460
- [5]Yamanishi K; Okuno T; Shiraki K; Takahashi M; Kondo T; Asano Y; Kurata T Identification of human herpesvirus-6 as a causal agent for exanthem subitum. Lancet, 1988.PMID 2896909
- [6]Hall CB; Long CE; Schnabel KC; Caserta MT; McIntyre KM; Costanzo MA; Knott A; Dewhurst S; Insel RA; Epstein LG Human herpesvirus-6 infection in children. A prospective study of complications and reactivation. N Engl J Med, 1994.PMID 8035839
- [7]Zerr DM; Meier AS; Selke SS; Frenkel LM; Huang ML; Wald A; Rhoads MP; Nguy L; Bornemann R; Morrow RA; Corey L A population-based study of primary human herpesvirus 6 infection. N Engl J Med, 2005.PMID 15728809
- [8]Tesini BL Clinical impact of primary infection with roseoloviruses. Curr Opin Virol, 2014.PMID 25462439
- [9]Hall CB; Caserta MT; Schnabel KC; Boeckh M; Carnahan JA; Petheram L; Shelley GA; Dewhurst S Characteristics and acquisition of human herpesvirus (HHV) 7 infections in relation to infection with HHV-6. J Infect Dis, 2006.PMID 16544246
- [10]Caserta MT; Hall CB; Schnabel K; McIntyre K; Long C; Costanzo M Primary human herpesvirus 7 infection: a comparison of human herpesvirus 7 and human herpesvirus 6 infections. J Pediatr, 1998.PMID 9738722