Paeds · infectious-diseases
Congenital syphilis and perinatal sexually transmitted infections
Also known as Congenital syphilis · Early congenital syphilis · Late congenital syphilis (Hutchinson triad) · Neonatal herpes simplex virus disease · Ophthalmia neonatorum
Fellowship topic on congenital syphilis and the perinatal sexually transmitted infections: the spirochaete Treponema pallidum crossing the placenta in untreated or inadequately treated maternal disease, with transmission highest in primary, secondary and early-latent syphilis; the early phenotype of snuffles, hepatosplenomegaly, rash and osteochondritis and the late Hutchinson triad of notched incisors, interstitial keratitis and eighth-nerve deafness; the other vertical infections — neonatal herpes, gonococcal and chlamydial ophthalmia neonatorum, and perinatal HIV and hepatitis B; the differential of the septic or hydropic newborn and neonatal conjunctivitis by onset day; maternal non-treponemal (RPR/VDRL) and treponemal (TPPA) serology with neonatal titre comparison, CSF and long-bone films; stepwise management from immediate maternal benzathine penicillin G through risk-stratified neonatal evaluation and ten-day aqueous penicillin to long-term surveillance, with penicillin desensitisation for the allergic pregnant woman and ocular prophylaxis at birth; the resurgent Australian Indigenous and remote epidemic and missed-prevention failures; and ANZ/UK/US/Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The Hutchinson triad of late congenital syphilis
Overview & Definition
Picture a two-week-old admitted from a remote community with poor feeding, a swollen abdomen and a copper-coloured rash spreading onto the palms and soles. The nose is streaming a blood-tinged discharge. The mother booked late to antenatal care and her syphilis serology was treated only ten days before delivery. This is early congenital syphilis, and the decisions made in the next hour — confirm, treat with ten days of penicillin, review the maternal treatment gap, and trigger public-health follow-up — decide whether the child carries permanent injury or recovers. Recognising it is the difference between a missed-prevention failure and a survivable, surveilled illness. [3] [6]
Congenital syphilis is the multisystem infection of the fetus and infant caused by transplacental transmission of Treponema pallidum subspecies pallidum. The perinatal sexually transmitted infections are the wider group of infections a mother can pass to her baby around the time of delivery: neonatal herpes simplex, gonococcal and chlamydial conjunctivitis (ophthalmia neonatorum), and vertically acquired HIV and hepatitis B. They are bound together because they share one prevention frame — screen the mother, treat the mother, protect the birth — and because they present in the same vulnerable window, the first weeks of life. [6] [3]
The clinician's work has three faces. The maternal face is to screen every pregnancy for syphilis and the other STIs, treat immediately with the right penicillin regimen, and document the titre response. The neonatal face is to risk-stratify the exposed newborn, recognise the septic or hydropic infant, and deliver the right drug for the right organism. And the population face is to run the screening programme, close the equity gaps that drive the resurgent epidemic, and ensure partner treatment — because the child who never acquires syphilis is the child the programme has protected. [7] [9]
Classification
Sort these infections the way the bedside forces you to — by the organism and the timeline, because the same spirochaete does very different things at different ages, and a conjunctivitis means very different things on different days. Congenital syphilis is one disease graded by the child's age at presentation. The perinatal STIs are a panel of organisms distinguished by their route in and the day they declare themselves. Keeping the timeline in the classification is what stops a clinician dismissing a day-three purulent eye as a blocked tear duct when it is gonococcal. [6] [3]
Congenital syphilis classifies by age of presentation into early (under two years) and late (over two years) disease. Early congenital syphilis reflects active, multi-organ infection: the organism is dividing and the infant is sick, with hepatosplenomegaly, rash, snuffles, osteochondritis and haematological disturbance. Late congenital syphilis reflects the permanent stigmata of the fetal injury that has already happened: the organism has been controlled but the structures it damaged — teeth, cornea, cochlea, bone — have grown into their distorted adult shape. This age split is the single most useful classification because it maps directly onto whether you are treating active infection or managing fixed sequelae. [6] [14]
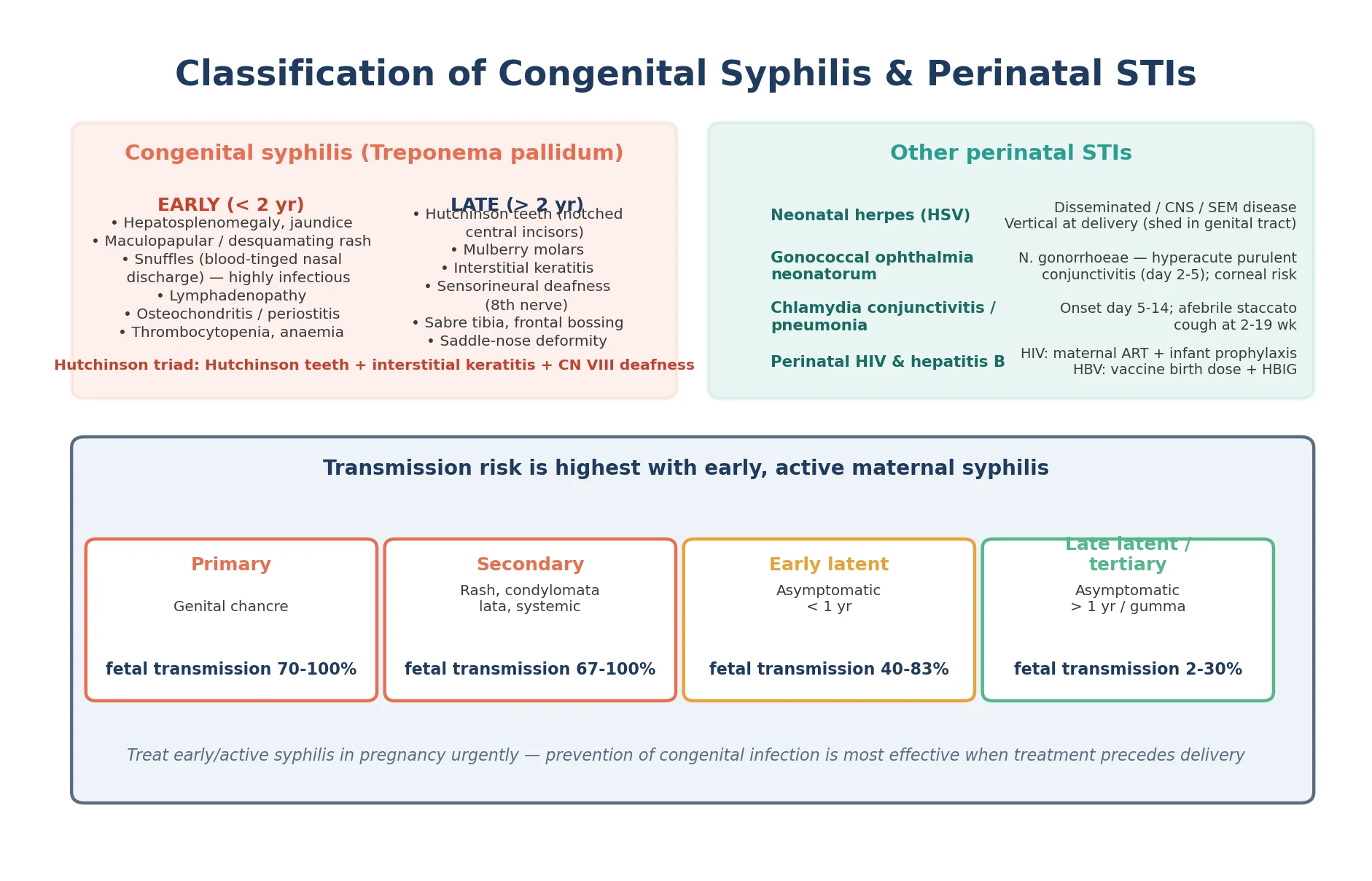
Neonatal conjunctivitis classifies by onset day, because the day the eye becomes red tells you which organism to fear. Chemical conjunctivitis appears on day one after prophylaxis irritation. Gonococcal conjunctivitis declares itself at day two to five as a hyperacute, profuse, purulent discharge with lid swelling and a real risk of corneal perforation. Chlamydial conjunctivitis comes later, at day five to fourteen, as a milder mucopurulent discharge, and is followed weeks later by an afebrile staccato-cough pneumonia. Herpetic keratoconjunctivitis comes with vesicles and keratitis. The day is the discriminator the examiner rewards. [6] [12]
The perinatal STIs also classify by their route of acquisition. Congenital syphilis is transplacental, so it can injure the fetus from the second trimester onward. Neonatal herpes is usually intrapartum, acquired as the baby passes through a genital tract shedding virus, so it presents in the second to third week. Gonococcal and chlamydial infection are likewise intrapartum, acquired at the eye and mucosae during birth. HIV and hepatitis B are vertically acquired with antepartum, intrapartum and postnatal components, and their prevention depends on maternal suppression, infant prophylaxis and, for hepatitis B, the birth-dose vaccine and immunoglobulin. The route in determines the prevention lever. [6] [5]
Epidemiology & Risk Factors
Congenital syphilis is resurgent. After years of decline, notification rates have risen sharply in Australia, Aotearoa New Zealand, the United States and many other high-income settings over the past decade, driven by rising syphilis in women of reproductive age. Australian national notifications data show that syphilis in women of reproductive age and congenital syphilis rose across 2011 to 2021, with a disproportionate burden among Aboriginal and Torres Strait Islander women and in remote northern and central communities where an outbreak has been sustained for years. Victoria saw a marked re-emergence of female and congenital syphilis from 2010 to 2020, framing the disease as a public-health priority. [9] [10]
The dominant risk factor at the individual level is a missed-prevention failure. The CDC analysis of congenital syphilis cases in 2022 found that most were attributable to absent or late antenatal testing, no timely maternal treatment, or inadequate maternal therapy — and a New York City analysis of 2010 to 2016 cases identified the same pattern. These are not failures of biological therapy; penicillin works. They are failures of the screening-and-treatment pathway, which means they are preventable one encounter at a time. [7] [8]
The structural risk factors compound the individual ones. Late or absent antenatal care, social disadvantage, substance use, remoteness and limited access to testing all increase the chance a woman reaches labour untreated. Reinfection after an adequately treated episode — through an untreated partner — can place a second, later pregnancy at risk, which is why partner treatment and repeat serology matter as much as the index treatment. These drivers are concentrated in Indigenous and remote communities, making equity the central prevention question. [9] [7]
Pathophysiology
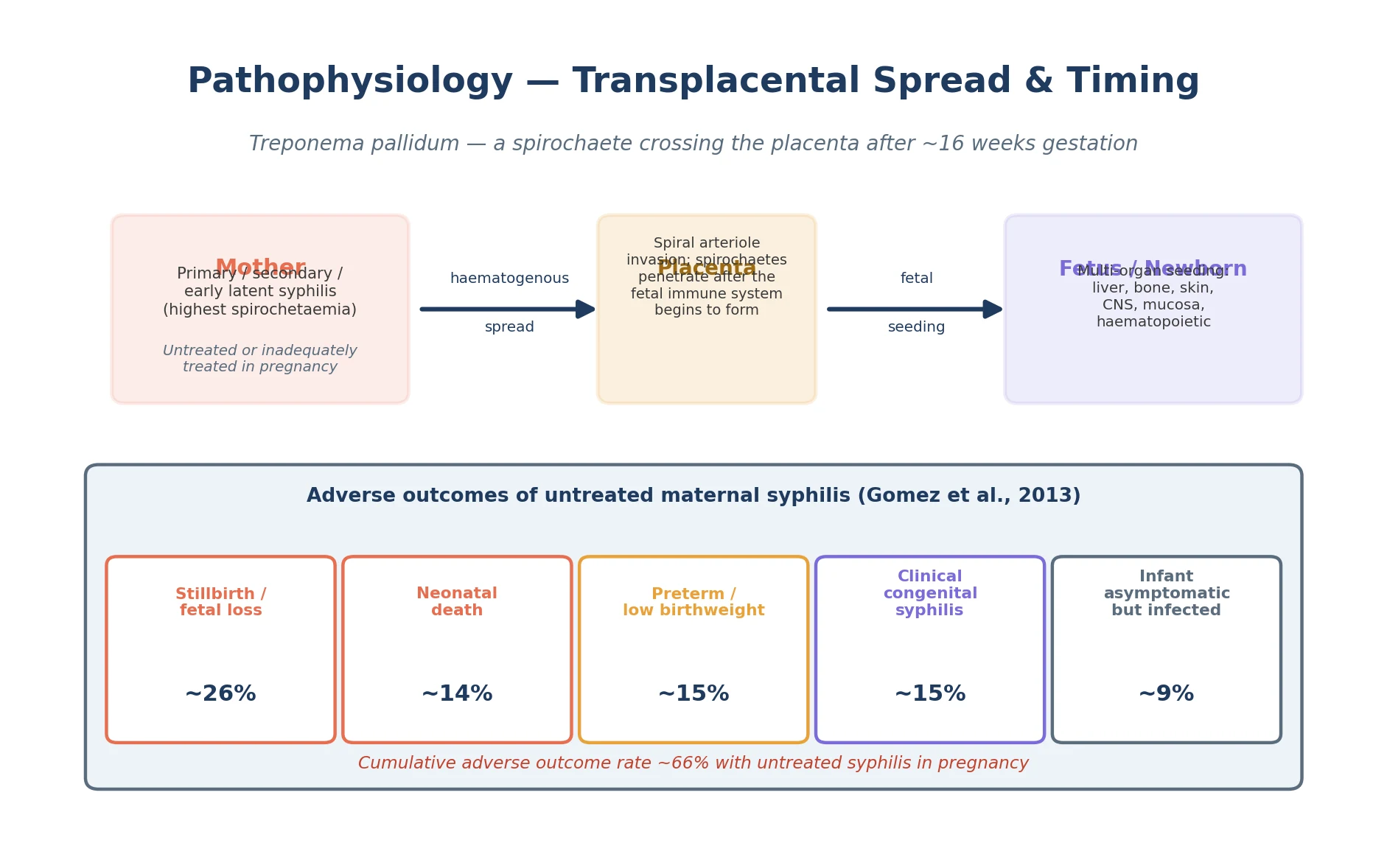
Why does syphilis in the mother wreck the fetus, and why does it depend so much on how active her disease is? The answer is that Treponema pallidum is a spirochaete that circulates in the blood during active disease, and the spirochitaemic mother seeds the placenta and fetus haematogenously. Transmission becomes efficient after about sixteen weeks gestation, as the placental barrier matures and the fetal circulation is established. The more active the maternal disease — primary chancre, secondary rash, or early-latent bacteraemia — the heavier the spirochaetal load and the higher the transmission risk. Late-latent and tertiary syphilis carry much lower risk because bacteraemia has largely subsided. [1] [11]
Once the spirochaete reaches the fetus, the mechanism of injury is vascular. T. pallidum invades endothelium and perivascular tissue, producing a proliferative endarteritis and obliterative vascular changes that choke the organs forming around those vessels. The liver, with its rich vasculature, bears the brunt — hence the hepatosplenomegaly and jaundice. Bone, actively growing, shows osteochondritis and periostitis. The skin and mucous membranes erupt with the copper-coloured rash and the highly infectious snuffles. The bone marrow is suppressed, producing anaemia and thrombocytopenia. When the injury is overwhelming, the fetus develops hydrops and dies in utero. The same vascular mechanism, operating at a slower tempo, fixes the late stigmata into the still-forming teeth, cornea and cochlea. [3] [6]
The pathophysiology of the other perinatal STIs is about the route in. Neonatal herpes is usually acquired at delivery, when the baby contacts HSV shed in the maternal genital tract — most often HSV-2, increasingly HSV-1. Once mucocutaneous entry occurs, virus either stays localised to skin, eye and mouth (SEM disease), ascends to the central nervous system (CNS disease with lethargy and seizures), or disseminates with hepatitis, pneumonitis and septic shock (disseminated disease). The later two phenotypes carry the highest mortality and the worst neurodevelopmental outcome, and the speed of acyclovir governs that outcome. [5] [4]
Gonococcal and chlamydial infection are likewise intrapartum. Neisseria gonorrhoeae contaminates the conjunctiva during birth and, within two to five days, produces an aggressive purulent conjunctivitis that can perforate the cornea. Chlamydia trachomatis takes longer to declare — five to fourteen days for conjunctivitis, two to nineteen weeks for the afebrile staccato-cough pneumonia that follows aspiration of the organism. HIV and hepatitis B reach the infant through antepartum, intrapartum and postnatal routes, and their pathophysiology is the domain of the dedicated HIV-exposure and hepatitis pages — here, the point is that their prevention is woven into the same perinatal STI screen-and-treat encounter. [6] [12]
Clinical Presentation
The early congenital syphilis presentation is the one the examiner wants you to picture in order. The infant is unwell — febrile or irritable, feeding poorly, failing to thrive. Snuffles is the signature sign: a profuse, blood-tinged nasal discharge that is teeming with spirochaetes and is therefore highly infectious, distinguishing it from the clear discharge of viral coryza. Hepatosplenomegaly with conjugated jaundice follows, often with generalised lymphadenopathy. The rash is copper-coloured and maculopapular, and it characteristically involves the palms and soles and may desquamate. Painful osteochondritis makes the limb immobile — the pseudoparalysis of Parrot, where the baby holds the limb still because moving the inflamed bone hurts. Thrombocytopenia and anaemia may be severe enough to cause bleeding or pallor. [6] [3]
The late congenital syphilis presentation is a set of permanent stigmata in the older child, each reflecting organ injury at a vulnerable developmental window. The Hutchinson triad is the classic: notched, screwdriver-shaped central incisors (Hutchinson teeth) and mulberry molars from enamel hypoplasia of the developing tooth bud; interstitial keratitis with photophobia, pain and corneal opacity that can blind; and eighth-nerve sensorineural deafness from cochlear injury. Add sabre-shaped tibiae, frontal bossing, a saddle-nose deformity from destroyed nasal cartilage, and rhagades (linear scars at the angles of the mouth), and the picture of fixed fetal injury is complete. A modern case report of Hutchinson's triad reminds the clinician that these stigmata still walk into clinic. [14] [6]
Neonatal herpes presents in the second to third week of life as one of three phenotypes. SEM disease is vesicles and superficial erosion of skin, eye and mouth — the mildest phenotype but a warning that dissemination may follow. CNS disease presents with lethargy, poor feeding, irritability and seizures, with CSF pleocytosis and a positive PCR. Disseminated disease presents as sepsis with hepatitis, coagulopathy, pneumonitis and shock, and carries the highest mortality. The trap is that SEM disease can look trivial and then progress, and that the mother may have no history of genital lesions — which is why any vesicle or unexplained sepsis in the second to third week demands empiric acyclovir. [5] [4]
Gonococcal ophthalmia neonatorum is an emergency that announces itself at day two to five with a profuse, purulent, often blood-tinged conjunctival discharge, dramatic lid oedema and chemosis. The cornea can perforate within hours if untreated, blinding the child. Chlamydial conjunctivitis is milder, appearing at day five to fourteen with mucopurulent discharge, and its later companion — chlamydial pneumonia at two to nineteen weeks — is an afebrile infant with a staccato cough, tachypnoea and interstitial infiltrates. Both demand maternal screening and treatment, because the eye and the lung are signs of a wider perinatal transmission. [6] [12]
Differential Diagnosis
For the septic or hydropic newborn, the differential is broad and the discriminator is the maternal and neonatal serology alongside the pattern of organ involvement. Congenital syphilis is distinguished by the combination of hepatosplenomegaly, a rash involving palms and soles, snuffles, thrombocytopenia and the characteristic long-bone changes. The mimics include congenital cytomegalovirus (petechiae, sensorineural hearing loss, intracranial calcifications), congenital toxoplasmosis (chorioretinitis, hydrocephalus, diffuse intracranial calcifications), haemolytic disease of the newborn (positive direct antiglobulin test, spherocytes), congenital leukaemia (blasts on the blood film), and bacterial sepsis. The TORCH framework is useful precisely because syphilis sits within it — but syphilis is distinguished from the viral TORCH infections by the rash distribution, the long-bone periostitis, and the spirochaetal serology. [3] [6]
[6] [3]For neonatal conjunctivitis, the discriminator is the onset day and the organism, and the operational rule is to send a gram stain and culture (or nucleic-acid amplification) rather than guess. Chemical conjunctivitis (day one, after prophylaxis) is mild and self-limiting. Gonococcal disease (day two to five) is hyperacute and purulent with gram-negative diplococci on stain. Chlamydial disease (day five to fourteen) is mucopurulent with inclusion bodies. Herpetic keratoconjunctivitis comes with vesicles and dendritic keratitis. Each demands a different systemic treatment, and topical therapy alone is never adequate for gonococcal or chlamydial disease. [6] [12]
For a vesicular or septic neonate, the differential of neonatal herpes includes bacterial sepsis, enteroviral sepsis (often with myocarditis and a summer peak), and bullous impetigo. The discriminator is the vesicle itself, the CSF profile, and the maternal history — but the operational rule is that any neonate with vesicles, unexplained sepsis, or lethargy and seizures in the second to third week gets empiric intravenous acyclovir while PCR confirms. Delaying acyclovir for confirmation costs brain and life. [5] [4]
Clinical & Bedside Assessment
The assessment of the suspected case begins with the maternal history, because the baby's risk is the mother's treatment story. Establish the antenatal syphilis serology results and their timing, the treatment given (drug, dose and dates), the titre response, partner treatment and reinfection risk, and the other STI screening results (HIV, hepatitis B, chlamydia, gonorrhoea). The single most important number is the interval between the last maternal treatment and delivery — if it was less than four weeks, the infant is at higher risk regardless of how well the mother seemed to respond. Add the social and cultural context: remoteness, access, and any barrier to follow-up. [11] [6]
On examination of the symptomatic infant, work systematically. Look for hepatosplenomegaly and jaundice, the rash and its distribution (palms and soles are key), the nasal discharge and its character, generalised lymphadenopathy, pallor or bruising, and a limp or immobile limb suggesting painful osteochondritis. Examine the eyes, listen to the chest, and assess tone and feeding. For conjunctivitis, record the day of onset, the character of the discharge, and any vesicles, keratitis or lid oedema. For suspected neonatal herpes, screen for skin vesicles, lethargy, poor feeding, temperature instability and seizures. [6] [3]
Document the public-health essentials at the bedside because they drive the response. Record the maternal stage and treatment adequacy, the treatment-to-delivery interval, the titre trend, and the partner and sexual-health details that will frame partner notification and reinfection assessment. For ophthalmia neonatorum and HSV, record the maternal history of genital symptoms and any known STI. A careful record at the first encounter prevents the late, disorganised public-health scramble that misses the partner and the next pregnancy. [7] [8]
For the older child with possible late stigmata, examine the teeth (Hutchinson incisors, mulberry molars), the eyes (interstitial keratitis, corneal opacity), the hearing (sensorineural loss), and the facial and skeletal features (frontal bossing, saddle nose, sabre tibia). These fixed findings, alongside persistent treponemal serology, anchor the diagnosis years after the fetal injury. [14] [6]
Investigations
Diagnosis rests on two complementary test types. Non-treponemal tests — the rapid plasma reagin (RPR) or Venereal Disease Research Laboratory (VDRL) test — measure disease activity and are reported as a quantitative titre that rises with active infection and falls with successful treatment. Treponemal tests — the T. pallidum particle agglutination (TPPA), treponemal immunoassay or immunoblot — confirm past or present treponemal infection and, once positive, stay positive for life. The maternal workup uses both: a reactive non-treponemal titre with a positive treponemal test defines active syphilis needing treatment. [6] [11]
In the exposed or symptomatic infant, the serological strategy is comparative. Send a quantitative non-treponemal test on the infant and compare it with the maternal titre — a neonatal titre fourfold or more higher than the maternal strongly suggests true congenital infection rather than passive transfer of maternal antibody. Treponemal IgM (the 19S-IgM fraction), where available, confirms active neonatal infection because maternal IgM does not cross the placenta. Round out the workup with a full blood count and film (anaemia, thrombocytopenia), liver function tests, a lumbar puncture for CSF cell count, protein and CSF VDRL, and long-bone radiographs for the osteochondritis and periostitis that are nearly pathognomonic. [6] [3]
Direct demonstration of the organism is possible and powerful. Dark-field microscopy or PCR of lesional fluid, rash scrapings or the nasal discharge can show the spirochaete directly — and it underlines the point that snuffles and moist rash lesions are highly infectious, so gloves and isolation are mandatory. For neonatal herpes, send HSV PCR on CSF, surface swabs and vesicle fluid, with liver function tests and coagulation studies to assess dissemination. For conjunctivitis, send a gram stain and culture, and nucleic-acid amplification testing for chlamydia and gonorrhoea, guided by the onset day. [6] [5]
In Australia and Aotearoa New Zealand, antenatal syphilis screening is universal and recommended at the first antenatal visit, with repeat testing at twenty-eight to thirty-two weeks and again at delivery for women in high-prevalence settings (including many Aboriginal and Torres Strait Islander and remote communities). Point-of-care testing is used in remote and outreach settings to close the access gap. Syphilis is a nationally notifiable disease, and public-health units coordinate partner notification. The Australian STI Management Guidelines (ASHM) for Aboriginal and Torres Strait Islander populations and the New Zealand Sexual Health Society guidance set the operational standard. [9] [6]
Management — Resuscitation
Resuscitation in congenital syphilis is about the unstable newborn. The red flags are shock, severe anaemia with bleeding, respiratory distress from syphilitic pneumonia or hepatitis, and the sepsis-like picture. Resuscitate with airway and breathing support, circulatory support with fluid and transfusion for severe anaemia, and start empiric penicillin without waiting for the full serological workup — the diagnosis is clear enough from the maternal history and the phenotype, and the treatment is safe. [6] [3]
For the symptomatic or proven infant, the treatment is aqueous crystalline penicillin G intravenously for ten days. The ten-day course matters because the central nervous system must be penetrated to treat neurosyphilis, and shorter or depot regimens risk undertreating CNS disease. Where intravenous access is genuinely impossible, procaine penicillin intramuscularly for ten days is the alternative. The symptomatic infant is never managed with a single benzathine dose, because benzathine penicillin does not achieve reliable CSF concentrations. [6] [11]
For the other perinatal STIs, resuscitation is equally time-critical. Gonococcal ophthalmia neonatorum demands urgent ceftriaxone (a single dose, with weight-based dosing) plus frequent eye irrigation with saline, because corneal perforation can occur within hours — topical therapy alone is inadequate and dangerous. Suspected neonatal herpes demands immediate empiric high-dose intravenous acyclovir while PCR confirms, because every hour of delay worsens the neurological outcome. The chlamydial pneumonia infant may need oxygen and support for the work of breathing while oral therapy takes effect. [6] [5]
Isolate the infant with congenital syphilis for the infectious secretions — snuffles and moist rash lesions shed spirochaetes — using standard precautions and gloves for contact with secretions. For suspected neonatal herpes, use contact precautions. Notify public health, because every case of congenital syphilis triggers a maternal and partner investigation that protects the next pregnancy. [6] [7]
Management — Definitive & Stepwise
Definitive management is a stepwise pathway matched to the host: treat the mother to prevent the case; evaluate and treat the exposed or symptomatic newborn; and prevent the perinatal STIs with the right drug at the right time. At the population end, the screening programme — universal antenatal testing, repeat testing in high-prevalence settings, and partner treatment — does the work that no single encounter can. [6] [7]
The stepwise congenital syphilis pathway
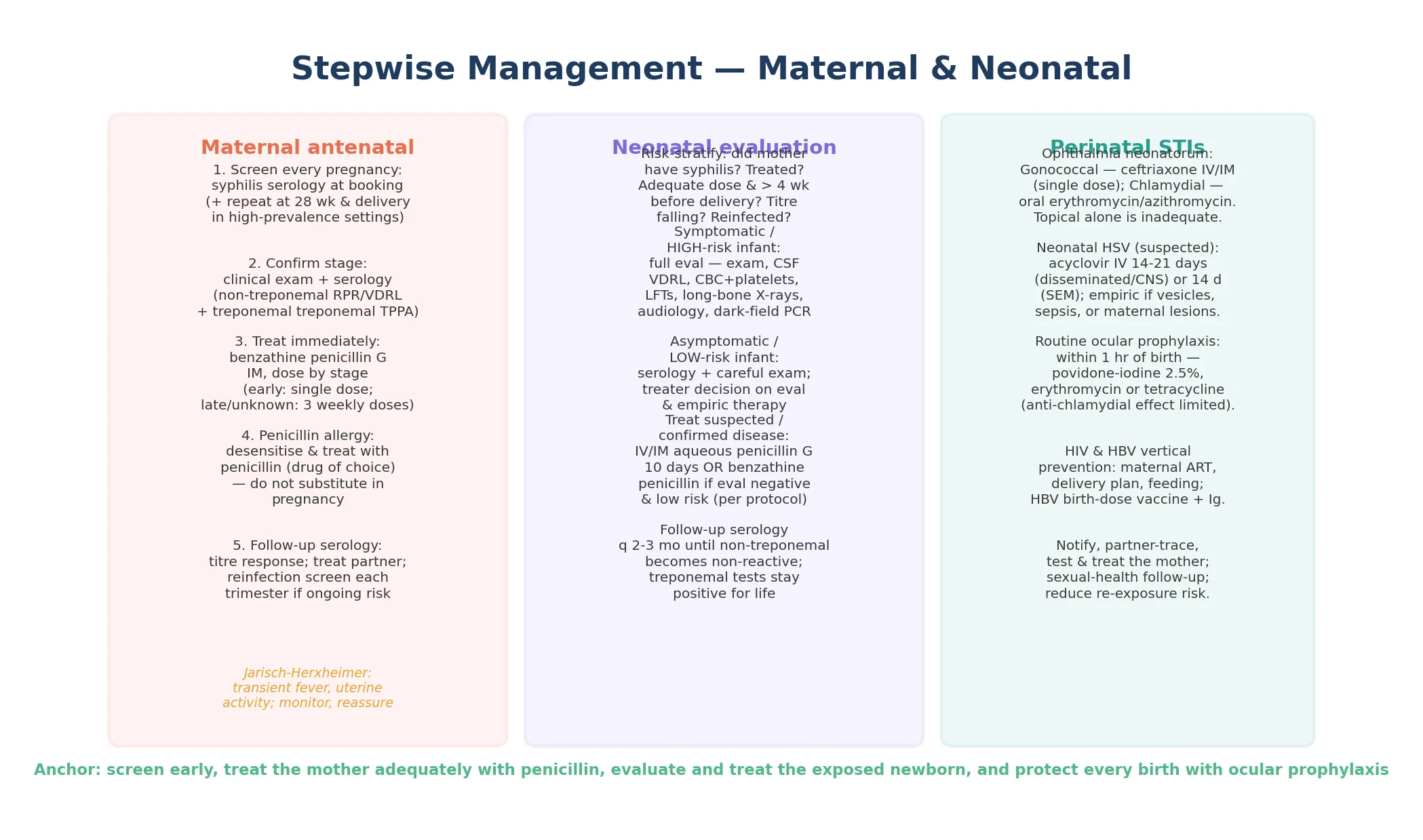
Screen every pregnancy for syphilis at booking; repeat at 28 to 32 weeks and at delivery in high-prevalence settings or where reinfection is possible.
Treat maternal syphilis immediately on diagnosis with benzathine penicillin G intramuscularly, dosed by stage — single dose for primary, secondary and early-latent disease; three doses one week apart for late-latent or unknown-duration disease.
Ensure treatment is completed at least four weeks before delivery, because prevention of congenital infection depends on this interval; manage penicillin allergy by desensitisation and penicillin, not substitution.
Risk-stratify the newborn by maternal treatment adequacy: symptomatic infants, or infants of untreated, inadequately treated, treated within four weeks of delivery, or reinfected mothers, are high risk and need full evaluation and treatment.
Evaluate the high-risk or symptomatic infant with quantitative non-treponemal serology (compared with maternal), treponemal IgM, full blood count, liver function tests, CSF cell count protein and VDRL, and long-bone radiographs.
Treat confirmed or suspected congenital syphilis with aqueous crystalline penicillin G intravenously for ten days; use benzathine penicillin only when evaluation is fully normal and risk is low, per protocol.
Follow up treated infants with quantitative non-treponemal serology every two to three months until non-reactive, and provide developmental, audiological and ophthalmological surveillance for the late stigmata.
The maternal treatment regimen is the cornerstone of prevention. Benzathine penicillin G, given intramuscularly and dosed by the stage of maternal disease, is the only regimen proven to prevent congenital infection effectively. A single dose treats primary, secondary and early-latent syphilis; three doses, one week apart, treat late-latent and unknown-duration disease. The treatment must be completed at least four weeks before delivery — a mother treated only days before labour remains a transmission risk. After treatment, monitor the non-treponemal titre for a fourfold fall over the following months, treat the partner, and re-screen each trimester if ongoing risk. [6] [1]
Penicillin allergy in pregnancy is a desensitisation problem, not a substitution problem. Erythromycin and the other macrolides do not cross the placenta reliably and do not cure fetal infection; ceftriaxone has limited evidence in pregnancy. The proven approach, established by Wendel and colleagues, is to desensitise the pregnant woman and treat her with penicillin, the only agent reliably effective against established fetal infection. Anticipate the Jarisch-Herxheimer reaction — the transient fever, myalgia and uterine activity that follow the release of spirochaetal antigens as the organism dies — and monitor the fetus during the reaction while reassuring the woman. [13] [11]
For the perinatal STIs, the management is organism-specific. Gonococcal ophthalmia neonatorum needs systemic ceftriaxone plus eye irrigation. Chlamydial conjunctivitis and pneumonia need oral erythromycin or azithromycin, and the mother needs treatment to prevent the next pregnancy's transmission. Neonatal herpes needs high-dose intravenous acyclovir for fourteen to twenty-one days depending on phenotype, followed by suppressive acyclovir for survivors to cut recurrence. Routine ocular prophylaxis at birth — povidone-iodine, erythromycin or tetracycline — is given to every newborn within the first hour to prevent gonococcal disease, recognising that its effect against chlamydia is limited. Vertical HIV and hepatitis B prevention run in parallel and are detailed in the dedicated pages. [6] [12]
Specific Subtypes & Scenarios
A hydropic or stillborn infant of an untreated mother. This is severe congenital syphilis presenting at its worst. Confirm with maternal and fetal serology, recognise the hepatosplenomegaly, anaemia and long-bone changes, and treat any live-born sibling exposed to the same untreated pregnancy. The encounter triggers partner notification, public-health follow-up, and a review of why the antenatal screen was missed. [1] [6]
A septic-appearing two-week-old with hepatosplenomegaly, rash and snuffles. This is classic early congenital syphilis. Confirm with comparative maternal and neonatal serology, send the full workup including CSF and long-bone films, and treat with ten days of aqueous penicillin. Review the maternal treatment gap and ensure partner treatment. [3] [6]
A newborn with profuse purulent conjunctivitis at day three. This is gonococcal ophthalmia neonatorum until proven otherwise. Send an urgent gram stain and culture, treat with systemic ceftriaxone and frequent eye irrigation, and screen and treat the mother and partner. Corneal perforation is the threat, so do not wait for confirmation to treat. [6] [12]
A twelve-day-old with vesicles, lethargy and poor feeding. This is neonatal herpes until excluded. Start empiric high-dose intravenous acyclovir immediately and send HSV PCR on CSF, surface swabs and vesicle fluid. The mother may have no history of genital lesions, and the vesicles may be few — do not let either reassure you out of treating. [5] [4]
An afebrile six-week-old with a staccato cough and tachypnoea. This is chlamydial pneumonia. Treat with oral erythromycin or azithromycin, support the work of breathing, and screen and treat the mother. The afebrile, well-appearing infant with a staccato cough in the second month is the classic aetiology-specific presentation examiners reward. [6] [12]
An adolescent or a remote-community woman with a positive antenatal syphilis screen. Treat immediately with the stage-appropriate benzathine regimen, repeat the serology to confirm the titre response, address reinfection through partner treatment, and ensure culturally safe sexual-health follow-up. In remote and Indigenous communities, point-of-care testing and outreach close the access gap that drives the resurgent epidemic. [9] [7]
Complications & Pitfalls
The serious consequences of congenital syphilis are stillbirth, hydrops and neonatal death, neurosyphilis with developmental consequence, and the permanent late stigmata. For the perinatal STIs, the consequences are corneal perforation and blindness from untreated gonococcal conjunctivitis, and death or severe neurodevelopmental disability from untreated disseminated or CNS neonatal herpes. Recognising these threats early and treating with the right drug is what changes the outcome. [1] [5]
The central diagnostic pitfall is trusting a single negative antenatal screen. A woman who acquires syphilis after the booking test still transmits to her fetus, which is why repeat serology at twenty-eight to thirty-two weeks and at delivery is essential in high-prevalence settings. A 'negative booking screen' is not a permanent reassurance — it is a snapshot. The rule that protects against this error is to repeat the test where the epidemiology demands it. [7] [8]
A second pitfall is substituting an alternative antibiotic for penicillin in the penicillin-allergic pregnant woman. Erythromycin, azithromycin and the tetracyclines do not reliably cross the placenta or cure fetal infection. The proven approach is desensitisation and penicillin, and anything less exposes the fetus to ongoing infection. [13] [11]
A third pitfall is treating the asymptomatic exposed infant as 'low risk' without reviewing the maternal treatment adequacy. An infant whose mother was treated within four weeks of delivery, whose titre did not fall, or who was reinfected, is at high risk and needs full evaluation and treatment — not a single benzathine dose and discharge. The treatment story governs the infant's risk. [6] [3]
A fourth pitfall is relying on topical therapy for ophthalmia neonatorum. Gonococcal and chlamydial disease are systemic infections that need systemic treatment, and herpetic keratoconjunctivitis needs systemic acyclovir. Topical therapy alone is inadequate and dangerous, and the hour spent applying eye ointment is an hour the cornea is perforating. [6] [12]
The final pitfall is missing the Jarisch-Herxheimer reaction. The treated pregnant woman can develop a transient fever with myalgia and uterine activity as the spirochaetes die and release antigen, and the fetus can show transient distress. Anticipate the reaction, monitor the fetus, and reassure the woman that it is expected and self-limiting. [13] [11]
Prognosis & Disposition
Adequate maternal treatment before delivery prevents the great majority of congenital syphilis, whereas untreated or late-treated infection carries a cumulative adverse-outcome rate around two-thirds, including stillbirth and neonatal death. Treated early congenital syphilis usually resolves, with residual stigmata depending on the timing of the fetal injury — long-bone changes heal, but established neurological, dental and sensory injury may persist. The treponemal serology stays positive for life, which is a diagnostic clue in the older child but a source of confusion if mistaken for active disease. [1] [6]
Neonatal herpes prognosis is governed by phenotype and the speed of acyclovir. SEM disease has the best prognosis and lowest mortality, but CNS and disseminated disease carry significant mortality even with treatment, and survivors frequently have neurodevelopmental sequelae. Suppressive acyclovir for six months after the acute illness cuts the rate of cutaneous recurrence and the cognitive decline associated with recurrent SEM disease. [5] [4]
Disposition follows severity. Admit the symptomatic infant for intravenous penicillin or acyclovir. Manage the well, low-risk exposed infant with examination, serology and close follow-up. For every case, complete the public-health follow-up — partner treatment, repeat maternal serology, and notification — because the next pregnancy depends on it. The discharge encounter is also a prevention opportunity: close the screening gap that allowed the case. [7] [6]
Special Populations
Pregnant women are the population prevention target. Universal antenatal syphilis screening at booking, with repeat testing at twenty-eight to thirty-two weeks and at delivery in high-prevalence settings, treats the mother and prevents the case. Document the titre response, treat the partner, and re-screen for reinfection. [11] [7]
Penicillin-allergic pregnant women must be desensitised and treated with penicillin, the only agent reliably effective against fetal infection. Substitution with an alternative antibiotic fails the fetus. The desensitisation is usually performed in a supervised setting with the penicillin dose given immediately afterward. [13] [11]
Aboriginal and Torres Strait Islander, Maori and Pacific peoples, and women in remote northern and central Australia carry the disproportionate burden of the resurgent epidemic. Ensure culturally safe, timely screening and treatment, use point-of-care testing in remote and outreach settings, provide sexual-health follow-up that respects community, and address the access barriers — distance, staffing, continuity of care — that drive missed prevention. [9] [10]
Refugee, asylum-seeking and migrant families may have a higher background prevalence of syphilis and other STIs and may face access barriers. Screen at first contact in pregnancy, use trained interpreters rather than family members, treat empirically where infection is confirmed, and link to sexual-health and primary care. [6] [11]
Adolescents and young adults need confidential, non-judgemental STI screening and treatment, partner notification, contraception and sexual-health care. A positive syphilis test in a pregnant adolescent is managed exactly as in the older woman — immediately and completely. [6] [7]
Substance-using and socially disadvantaged women need the access wraparound — housing, coordination of care, treatment of reinfection, and a public-health layer that does not stop at the bedside. These are the women most at risk of the missed-prevention failure, and they are the women the programme must reach. [7] [8]
Evidence, Guidelines & Regional Differences
The global evidence base for the burden of maternal syphilis rests on the Gomez systematic review and meta-analysis, which quantified the adverse pregnancy outcomes of untreated maternal syphilis — stillbirth, neonatal death, preterm birth, low birthweight and clinical congenital syphilis — and the Korenromp global burden estimates for 2016, which mapped the worldwide scale of the problem and the progress since 2012. Together these anchor the prevention argument: the disease is common, the outcomes are severe, and treatment works. [1] [2]
The operational standard for treatment is the CDC Sexually Transmitted Infections Treatment Guidelines (Workowski et al., 2021), which set the benzathine penicillin regimen by stage, the neonatal evaluation and treatment algorithm, the management of ophthalmia neonatorum and the approach to neonatal herpes. A modern state-of-the-art review of congenital syphilis synthesises current strategies and the future directions for a resurgent disease. [6] [3]
Untreated maternal syphilis and adverse pregnancy outcomes
Population: Systematic review and meta-analysis of pregnancies with untreated or inadequately treated maternal syphilis, plus a global burden estimate for 2016.
Key finding
Untreated maternal syphilis carried a cumulative adverse-outcome rate around 66 per cent — stillbirth around 26 per cent, neonatal death around 14 per cent, preterm or low birthweight around 15 per cent, and clinical congenital syphilis around 15 per cent; the global burden estimate counted nearly a million adverse pregnancy outcomes attributable to syphilis in 2016.
Practice change
Screen every pregnancy for syphilis and treat immediately with the stage-appropriate benzathine penicillin regimen — the single most effective prevention lever for congenital syphilis.
The neonatal herpes evidence is anchored by the American Academy of Pediatrics guidance on the asymptomatic neonate born to a woman with active genital herpes lesions (Kimberlin et al., 2013) and the Samies et al. review of neonatal HSV disease, which together set the approach to risk stratification, empiric acyclovir and suppression. The missed-prevention evidence comes from the CDC's analysis of congenital syphilis cases in the United States in 2022 (McDonald et al.) and the New York City analysis of 2010 to 2016 (Slutsker et al.), both showing that most cases were attributable to failures of testing or treatment rather than biology. [4] [7]
The Australian evidence comes from the Hengel et al. national notifications analysis (2011 to 2021) and the Borg et al. Victoria analysis (2010 to 2020), documenting the re-emergence of syphilis in women of reproductive age and of congenital syphilis, with a disproportionate Indigenous and remote burden. A practical guide for prenatal providers (Desjardins et al., 2025) and the ophthalmia neonatorum epidemiology review (Asiamah et al., 2025) round out the perinatal-STI operational picture. [9] [10]
The regional policy structure is consistent in principle and varies in detail. In ANZ, antenatal syphilis screening is universal with repeat testing in high-prevalence settings, the Australian STI Management Guidelines (ASHM) for Aboriginal and Torres Strait Islander populations and the New Zealand Sexual Health Society guidance set the operational standard, and syphilis is nationally notifiable. In the UK, the BASHH national guideline for the management of syphilis and the UK National Screening Committee antenatal programme deliver the equivalent strategy. In the US, the CDC STI treatment guidelines and surveillance drive the response, with the resurgent epidemic framed as a missed-prevention problem. In Canada, the Canadian Guidelines on Sexually Transmitted Infections and provincial programmes deliver the same. In every region the principle is the same: screen every pregnancy, treat with penicillin, and protect every birth with ocular prophylaxis. [6] [9]
The controversies are real: the optimal frequency of repeat antenatal screening in different prevalence settings; the role of point-of-care testing and empirical treatment in high-prevalence remote communities; whether doxycycline or ceftriaxone have a role when penicillin is unavailable; and the equity gap that drives Indigenous and remote congenital syphilis. The defence against each is the same: universal screening with targeted repeat testing, immediate and adequate treatment, partner care, and a public-health layer that reaches the women the system currently misses. [7] [3]
Exam Pearls
- Snuffles — a profuse blood-tinged nasal discharge teeming with spirochaetes — is the most specific sign of early congenital syphilis and is highly infectious. [6]
- The Hutchinson triad of late congenital syphilis is notched incisors, interstitial keratitis and eighth-nerve sensorineural deafness; add mulberry molars, sabre tibia and saddle-nose. [14]
- Transmission risk is highest in primary, secondary and early-latent maternal syphilis (around 70 to 100 per cent); late-latent disease carries a much lower risk. [1]
- A neonatal non-treponemal titre fourfold higher than the maternal strongly suggests true congenital infection; treponemal tests stay positive for life. [6]
- Treat maternal syphilis with benzathine penicillin G intramuscularly — single dose for early disease, three weekly doses for late-latent — completing treatment at least four weeks before delivery. [6]
- Penicillin-allergic pregnant women must be desensitised and treated with penicillin; alternatives do not reliably cure fetal infection. [13]
- Anticipate the Jarisch-Herxheimer reaction in the treated pregnant woman — transient fever and uterine activity warrant fetal monitoring. [13]
- Gonococcal ophthalmia neonatorum presents at day two to five as hyperacute purulent conjunctivitis; treat with systemic ceftriaxone urgently — topical therapy alone is inadequate. [6]
- Chlamydial conjunctivitis appears at day five to fourteen and chlamydial pneumonia at two to nineteen weeks with an afebrile staccato cough; treat with oral erythromycin or azithromycin. [6]
- Start empiric high-dose intravenous acyclovir immediately on suspicion of neonatal herpes — never wait for PCR confirmation. [5]
- Most congenital syphilis is a missed-prevention failure: no timely test, no timely treatment, or inadequate therapy — so repeat antenatal screening in high-prevalence settings. [7]
References
- [1]Gomez GB; Kamb ML; Newman LM; Mark J; Broutet N; Hawkes SJ Untreated maternal syphilis and adverse outcomes of pregnancy: a systematic review and meta-analysis. Bull World Health Organ, 2013.PMID 23476094
- [2]Korenromp EL; Rowley J; Alonso M; Mello ML; Wijesooriya NS; Mahiane SG; et al Global burden of maternal and congenital syphilis and associated adverse birth outcomes-Estimates for 2016 and progress since 2012. PLoS One, 2019.PMID 30811406
- [3]Flores JM; Arguello E; Beddard R; Ahmed A; et al State-of-the-Art Review: Congenital Syphilis in the Modern Era: Current Strategies and Future Directions. Clin Infect Dis, 2026.PMID 41638217
- [4]Kimberlin DW; Baley J; Committee on Infectious Diseases; Committee on Fetus and Newborn Guidance on management of asymptomatic neonates born to women with active genital herpes lesions. Pediatrics, 2013.PMID 23378604
- [5]Samies NL; Lakeman M; Cantey JR; Demmler-Harrison G; Hyun J; Kennedy JL; Nisbet JW; Ochoa JB; Schutze GE; Shakib JH; Siegel JD; Baker CJ Neonatal Herpes Simplex Virus Disease: Updates and Continued Challenges. Clin Perinatol, 2021.PMID 34030813
- [6]Workowski KA; Bachmann LH; Chan PA; Johnston CM; Muzny CA; Park I; Reno H; Zenilman JM; Bolan GA Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep, 2021.PMID 34292926
- [7]McDonald R; Flagg EW; Leichliter J; Sherwood J; Johnson HL; Thrun M; Peacock G; Barrow L; Thigpen MC; Weinstock HS Vital Signs: Missed Opportunities for Preventing Congenital Syphilis - United States, 2022. MMWR Morb Mortal Wkly Rep, 2023.PMID 37971936
- [8]Slutsker JS; Schillinger JA; Zucker JR; Johnson-Masciello M; Pupalaza I; Ashenburg A; Sandulescu O; Gorgos M; Rosenblum LS Factors Contributing to Congenital Syphilis Cases - New York City, 2010-2016. MMWR Morb Mortal Wkly Rep, 2018.PMID 30286056
- [9]Hengel B; Pham A; Guy R; Dyda A; Law M; Maher L; Ward JS; McGregor S; Whiley DM; Dutt K; Causer L; Kaldor JM; Ali H Notification rates for syphilis in women of reproductive age and congenital syphilis in Australia, 2011-2021: a retrospective cohort analysis of national notifications data. Med J Aust, 2024.PMID 39010298
- [10]Borg SA; Lee MH; Sacks R; Norton L; Farmer L; Peel M; Catton M; Fehler G; Callander D; McNulty A; O'Sullivan MVN; Armishaw J; Read P; Whiley D; Lahra MM; Donovan B; Ward JS; Guy R; Craig ME The Reemergence of Syphilis Among Females of Reproductive Age and Congenital Syphilis in Victoria, Australia, 2010 to 2020: A Public Health Priority. Sex Transm Dis, 2023.PMID 37155648
- [11]Desjardins AA; Saxinger L; Robinson JL Syphilis in pregnancy: A practical guide for prenatal care providers. Int J Gynaecol Obstet, 2025.PMID 40977496
- [12]Asiamah R; Bekoe-Tabiri S; Naafs B; Walraven G; Asinobi OS; Sankhwar S; Khereibek I; Yelverton J; Bonsu FA; Prasad N; Kaona FA; Anabwani G; Bauai WA; Adam V; Khatoon L; Iwuala N; Okoronkwo C; Jagnoor J; Bhandari M; Wanyonyi G; Ekure EN; Mulholland K; Gray K; Boyle R; Gray A; Bailey RC; Kisia L; Ram P; Russell FM Epidemiology of ophthalmia neonatorum: a systematic review and meta-analysis. BMC Pediatr, 2025.PMID 39810179
- [13]Wendel GD Jr; Stark BJ; Jamison RB; Molina RD; Sullivan TJ Penicillin allergy and desensitization in serious infections during pregnancy. N Engl J Med, 1985.PMID 3921835
- [14]Pessoa L; Atri S; Laca J; Guerra C; Perez K Clinical aspects of congenital syphilis with Hutchinson's triad. BMJ Case Rep, 2011.PMID 22670010