Paeds · infectious-diseases
Dengue and other arboviral infections
Also known as Dengue fever · Dengue haemorrhagic fever · Dengue shock syndrome · Severe dengue · Zika virus disease · Congenital Zika syndrome · Chikungunya
Fellowship guide to dengue and other paediatric arboviral infections: Aedes-borne dengue, Zika and chikungunya; the WHO 2009 classification and warning signs; the reversible capillary plasma leak that defines severe dengue; serial haematocrit and platelet monitoring; titrated isotonic crystalloid through the critical phase around defervescence; the harmful-no-bolus lesson; the CYD-TDV and TAK-003 vaccines; congenital Zika syndrome; and chikungunya arthropathy in children.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Dengue is a mosquito-borne flavivirus illness that has become the most important arboviral cause of severe paediatric disease worldwide, with an estimated 100 to 400 million infections and around half the world's population now living at risk.[1] In children the dangerous form is not the fever itself but a narrow, reversible window of capillary plasma leakage that can tip a previously well child into shock over a matter of hours, so the clinical task is less to treat the fever and more to escort the child safely through that leak.[2]
Three Aedes-borne viruses dominate paediatric practice: dengue, Zika and chikungunya. They share a vector and an early febrile-rash presentation, but each has a distinct signature that the examiner expects you to separate. Dengue's signature is plasma leakage and shock; Zika's is injury to the developing fetal brain; and chikungunya's is severe, relapsing small-joint arthritis.[3]
Classification
The first bedside question is whether this child has dengue at all, and the second is whether the dengue is severe. The 2009 World Health Organization scheme replaces the older dengue fever versus dengue haemorrhagic fever split with a severity-graded triad that is easier to apply prospectively and was validated in multicentre prospective studies across South-East Asia and Latin America.[4]
The three 2009 categories are dengue without warning signs, dengue with warning signs, and severe dengue. Dengue without warning signs is a probable acute febrile illness with two or more of nausea or vomiting, rash, aches, leucopenia or a positive tourniquet test, in a child with no other obvious cause. Dengue with warning signs adds any of the seven warning signs, and severe dengue is defined by plasma leakage causing shock or respiratory distress, by severe bleeding, or by organ impairment such as hepatitis, encephalopathy or myocarditis.[3]
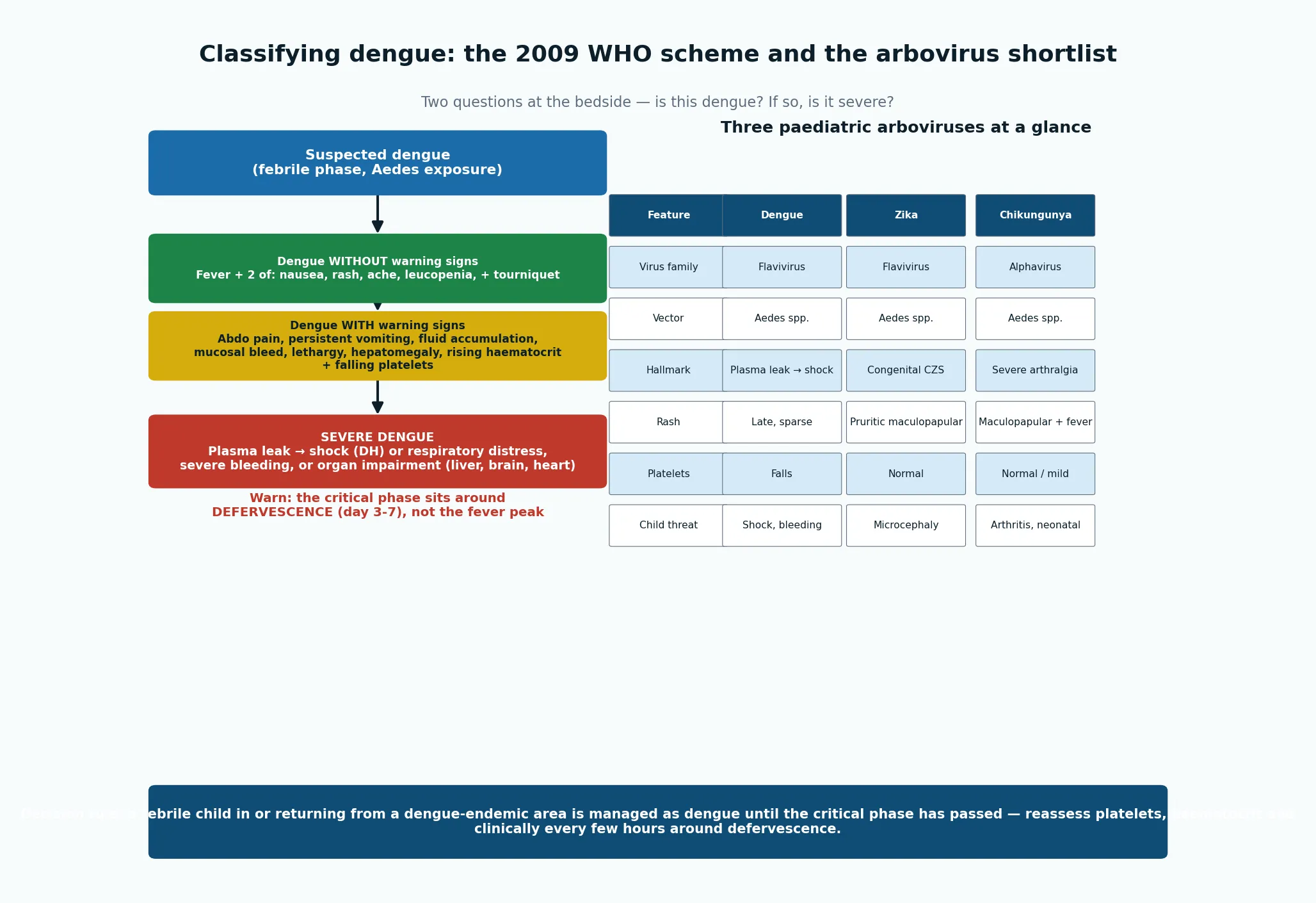
The seven warning signs are the testable list every fellowship candidate must carry into the exam: abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation such as ascites or pleural effusion, mucosal bleeding, lethargy or restlessness, hepatomegaly greater than two centimetres, and a rising haematocrit with a falling platelet count.[3] A systematic review and meta-analysis of nearly 4000 children confirmed that abdominal pain, vomiting, clinical fluid accumulation, hepatomegaly, haematocrit rise with platelet fall and lethargy each roughly double the odds of progressing to severe dengue, and that combinations of warning signs carry the highest risk.[9]
Epidemiology & Risk Factors
Dengue is hyperendemic across South and South-East Asia, the Pacific, the Caribbean, Latin America and parts of Africa, with all four serotypes now circulating in many of these regions. The 2013 global burden modelling estimated that around 390 million infections occur each year, of which about 96 million are clinically apparent, and that the burden falls hardest on children in endemic countries.[1]
In Australia and New Zealand locally-acquired dengue is uncommon and is driven by imported cases seeding Aedes aegypti populations in tropical north Queensland during the wet season; in the UK, Canada and most of Australia the cases seen are imported travellers returning from South-East Asia, the Pacific, or the Americas.[3] The Pacific island nations, Indonesia, the Philippines, Vietnam and Thailand are the commonest sources for ANZ paediatric cases, and a returned-traveller child with fever and thrombocytopenia must be assumed to have dengue (and malaria, depending on the country) until testing proves otherwise.
The single most important severity risk factor is a secondary heterotypic infection: a child who has had one dengue serotype and is later infected by a different serotype carries a substantially higher risk of severe disease because of antibody-dependent enhancement.[2] Other recognised risk factors include infancy, obesity, female sex, certain DENV-2 genotypes, and chronic conditions such as asthma, diabetes and sickle cell disease.[9]
Zika caused a major 2015 to 2016 outbreak in the Americas that exposed the teratogenic potential of what had been regarded as a trivial illness, producing an epidemic of microcephaly in north-east Brazil.[11] Chikungunya re-emerged in the Americas from 2013 onward and has since established itself across Aedes-endemic regions, with large paediatric outbreaks reported from the Caribbean, South Asia and the Indian Ocean.[14]
Pathophysiology
The defining lesion of severe dengue is transient capillary plasma leakage. When you understand the leak, the monitoring and the fluid strategy make sense. Endothelial dysfunction opens gaps in the capillary wall of a magnitude that lets albumin and plasma water escape into the extravascular space, so the intravascular volume falls and the haematocrit rises even as the child loses total circulating protein.[2]
This is not a true vasculitis — the vessel wall recovers within 24 to 48 hours, which is why cautious, titrated fluid carries most children through the critical window without long-term vascular injury. The leak is patchy rather than uniform, which is why it shows up first as a right-sided pleural effusion, ascites, gallbladder wall thickening and a rising haematocrit.[3]
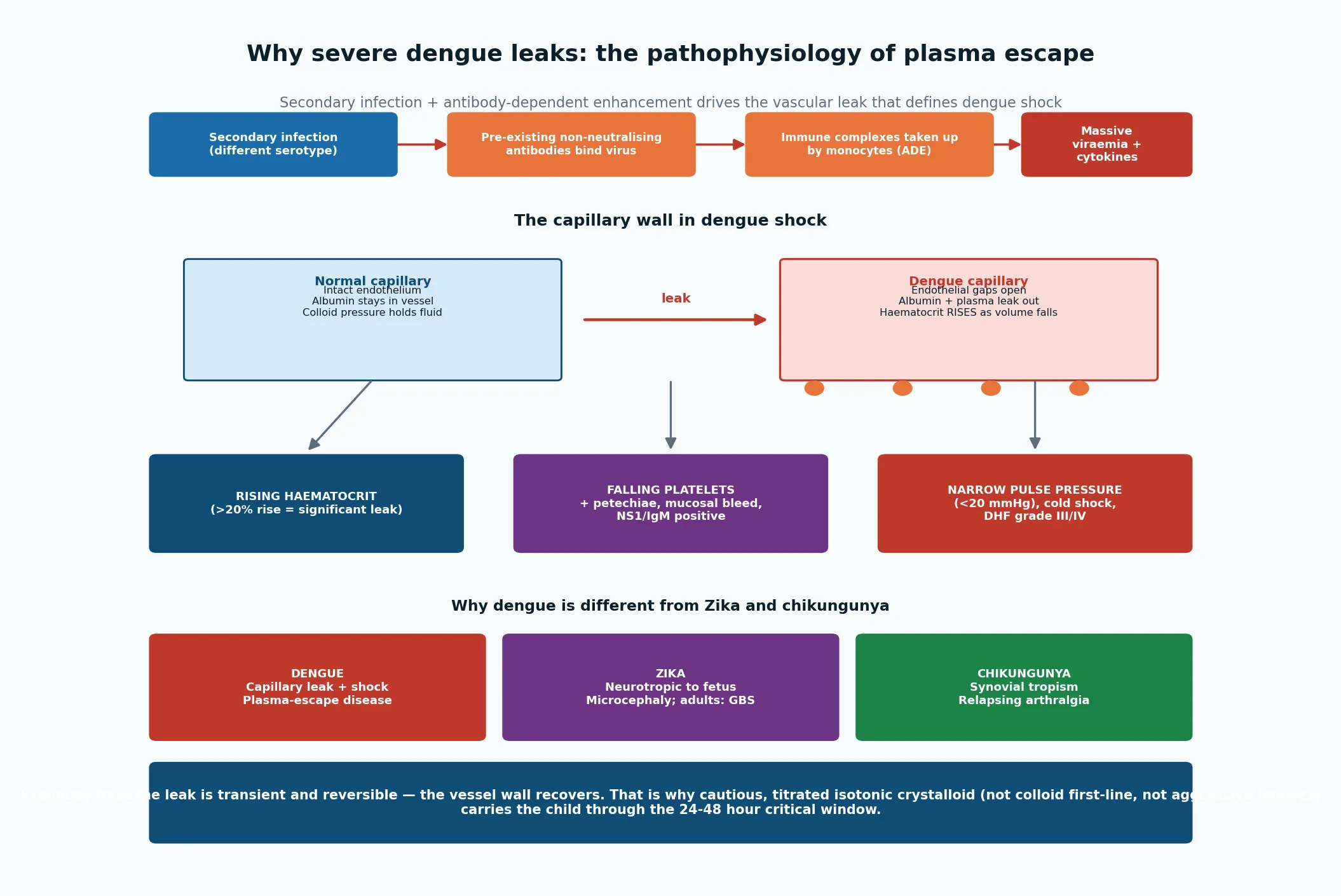
Secondary heterotypic infection amplifies the process through antibody-dependent enhancement. Pre-existing non-neutralising antibody from a first serotype binds the new serotype and shuttles the virus into monocytes via Fc receptors, producing higher viraemia, heavier cytokine release and more endothelial injury than a primary infection.[2] This is the mechanism behind the well-recognised clinical observation that second dengue infections are the dangerous ones, and it is also the reason the CYD-TDV vaccine increased hospitalisation rates in seronegative recipients, as a vaccine given to a child with no prior immunity can mimic that first, priming infection.[5]
Thrombocytopenia in dengue has a dual origin: bone-marrow suppression of megakaryocyte production and peripheral immune-mediated platelet consumption. Bleeding is driven by thrombocytopenia combined with capillary fragility, and disseminated intravascular coagulation is uncommon except in the most severe, shocked children.[3]
The other two arboviruses injure different tissues. Zika virus crosses the placenta and targets neural progenitor cells in the developing fetal brain, producing the characteristic pattern of microcephaly, intracranial calcifications, arthrogryposis and ocular and auditory injury now called congenital Zika syndrome.[13] Chikungunya is an alphavirus with marked synovial tropism, producing an intense synovitis and relapsing arthralgia that can persist for months after the acute illness.[15]
Clinical Presentation
A child with dengue typically presents with sudden high fever lasting two to seven days, accompanied by headache, retro-orbital pain, myalgia, arthralgia, anorexia, nausea and a flushed face. The classical "breakbone" pains, a positive tourniquet test, and a late maculopapular rash that appears as the fever settles are all supportive features, but none is diagnostic on its own.[2]
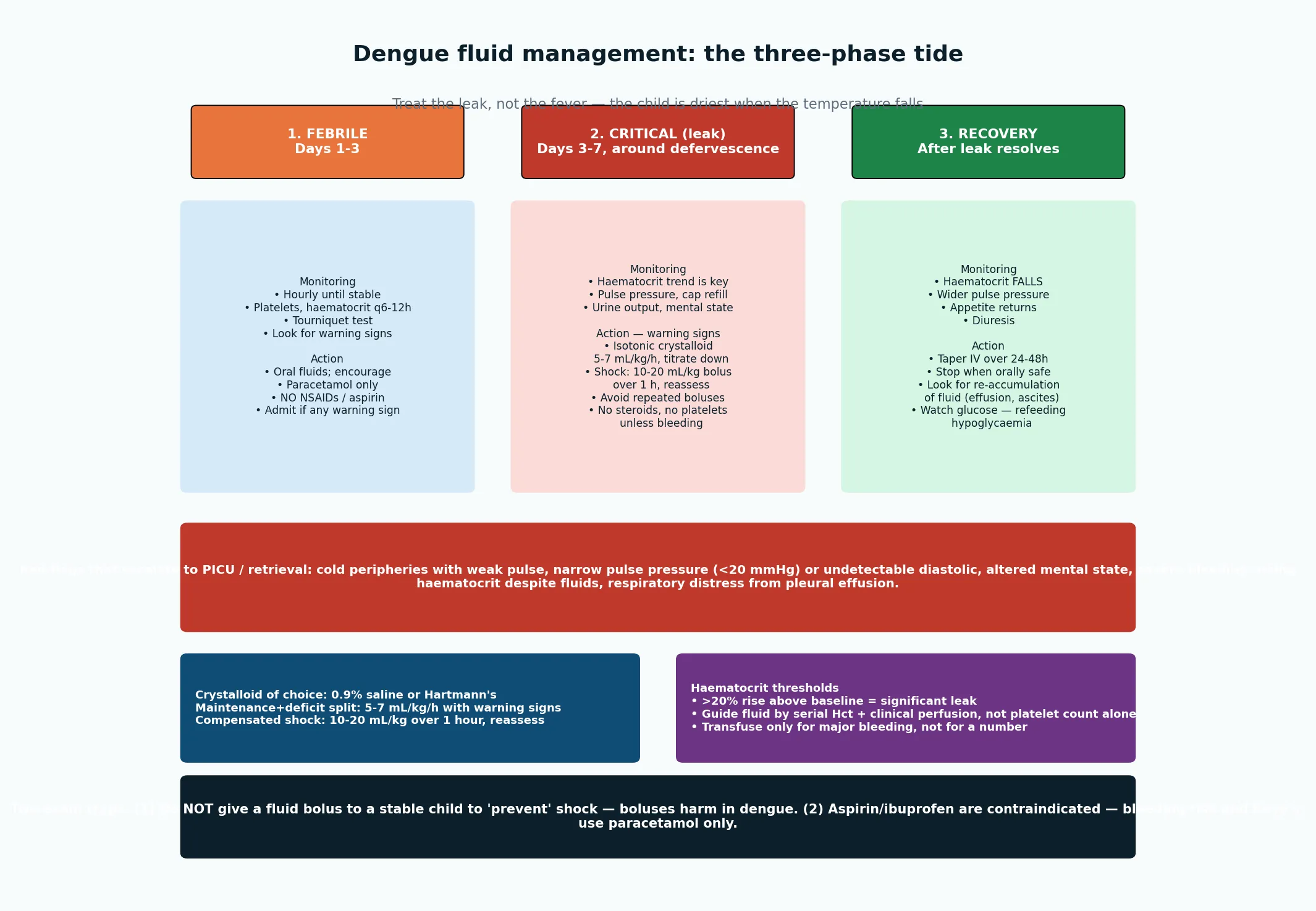
The crucial teaching point is that the dangerous phase begins as the fever falls. Defervescence marks the start of the 24 to 48 hour critical phase, during which plasma leakage peaks. A child who looked well during the febrile phase can develop a rising haematocrit, a narrowing pulse pressure, a pleural effusion, ascites and hepatomegaly precisely as the temperature normalises, so the period of apparent clinical improvement is the period of greatest risk.[3]
Dengue shock declares itself with the haemodynamic signs of plasma loss: a narrow pulse pressure below 20 mmHg, cold clammy peripheries, delayed capillary refill, a rapid thready pulse, oliguria and altered consciousness. In the older WHO 1997 scheme this is dengue haemorrhagic fever grade III (compensated shock) or grade IV (profound hypotension with undetectable blood pressure), and these map directly onto the 2009 category of severe dengue with shock.[3]
Zika in children is usually a mild febrile illness with a pruritic maculopapular rash that spreads from the face, low-grade fever, conjunctival injection (non-purulent), arthralgia and headache; many infections are subclinical. The clinically devastating presentation is not in the infected child but in her fetus — congenital Zika syndrome in the infant of a mother infected in pregnancy.[13]
Chikungunya in children presents with sudden high fever, a maculopapular rash, and characteristically severe polyarthralgia that targets the small joints of the hands, wrists, ankles and feet. Neonates infected through vertical transmission at delivery can develop a severe febrile illness with rash, encephalopathy and bleeding.[15]
Differential Diagnosis
The febrile phase of dengue is indistinguishable from many common paediatric fevers, so the differential is built around the travel and exposure history, the platelet and haematocrit trend, and the pace of the illness. Influenza and other respiratory viruses, enterovirus and measles, scrub typhus and other rickettsial fevers, leptospirosis, typhoid and malaria all sit on the list, and the first job is to separate dengue and malaria because both can kill a returned traveller quickly and their treatments are entirely different.[2]
Dengue shock must be separated from septic shock. Dengue shock is classically cold and narrow-pulse-pressure with a relatively preserved conscious level until late, with a high haematocrit and a normal or low white cell count, whereas septic shock in a child often shows a focus of infection, a wider or warm early phase, and a raised or markedly shifted white cell count. The haematocrit trend is the discriminator: a rising haematocrit with a falling platelet count points to dengue leak, while a stable haematocrit points away from it.[3]
The rash illnesses of Zika, chikungunya, rubella, measles and parvovirus overlap, and the differentiation rests on epidemiology (outbreak, travel, pregnancy), the constellation of conjunctivitis, arthralgia or fever pattern, and confirmatory PCR or serology. Congenital Zika microcephaly must be distinguished from genetic and chromosomal causes of microcephaly, other congenital infections in the TORCH group, and fetal brain disruption sequence; the combination of microcephaly with intracranial calcifications (often at the grey-white junction), arthrogryposis and hypertonia is highly characteristic.[11]
Chikungunya arthralgia is distinguished from juvenile idiopathic arthritis and reactive arthritis by its acute onset in an outbreak setting, the high fever and rash that precede the joint pain, and its typically self-limiting course, although a subset of children develop persistent post-chikungunya rheumatism.[15]
Clinical & Bedside Assessment
Start with the exposure: where has the child been in the last two weeks, has there been a local outbreak, are there other family members affected, and has the child had dengue before. A history of a prior dengue infection raises the suspicion of a secondary, more severe course and lowers the threshold for admission.[2]
Examine for the warning signs and for evidence of leak. Look for a flushed face, a faint early rash, petechiae and a positive tourniquet test. Palpate for hepatomegaly, which is an early sign of plasma accumulation. Auscultate for a pleural rub or reduced breath sounds at the right base, and look for ascites. Reassess perfusion serially: feel the peripheries, time the capillary refill, measure the pulse pressure, and record the mental state.[3]
The synthesis for an exam long case is a one-sentence problem representation that names the syndrome, the severity and the immediate plan. A model statement is: "A six-year-old returned from Bali four days ago with high fever, now at defervescence with abdominal pain, a rising haematocrit, a platelet count of 70, and a pulse pressure of 24 mmHg, has dengue with warning signs and is being admitted for group B management with titrated isotonic crystalloid and serial monitoring." That single sentence tells the examiner you have classified the disease, graded the severity and committed to a plan.[3]
The common bedside error is to anchor on the fever, treat it with antipyretics and discharge the child at the temperature nadir. The second common error is to chase the platelet count as the sole marker of severity; the platelet count is supportive but the haematocrit trend and the clinical perfusion are the markers that drive fluid decisions.[9]
Investigations
Confirming dengue depends on the day of illness. The NS1 antigen test is most sensitive in the first five days and confirms infection before antibody has developed; from about day four the IgM rises, and paired serology showing a rise in IgG or a high IgG titre supports secondary infection.[3] In the first one to three days a reverse-transcriptase PCR can also detect virus and serotype the infection, which is useful for outbreak surveillance.
The full blood count is the workhorse investigation. Look for a rising haematocrit against the child's baseline — a rise of more than 20 per cent is significant haemoconcentration and a marker of leak — and a falling platelet count, typically below 100 times ten to the ninth per litre. Leucopenia with a left shift and atypical lymphocytes is common.[2]
The single most important habit is to trend the haematocrit rather than read a single value. Compare today's haematocrit to the baseline taken at first contact, repeat it every six to twelve hours through the critical phase, and use the trend alongside clinical perfusion to decide fluid volume.[3]
Supportive investigations for a child with warning signs or severe disease include liver function tests, albumin, coagulation profile, lactate, glucose, urea and electrolytes, and a chest X-ray or ultrasound to detect an occult right pleural effusion, gallbladder wall thickening or ascites. Blood cultures are sent to exclude bacterial co-infection, particularly in a shocked child where sepsis is in the differential.[3]
For Zika, request RT-PCR on serum and urine in the acute phase (most sensitive in the first one to two weeks), and IgM serology later; in pregnancy, fetal ultrasound and, where indicated, amniocentesis PCR have a role in the assessment of fetal infection.[11] For chikungunya, RT-PCR in the first week and IgM serology thereafter confirm the diagnosis.[14]
A Thai prospective cohort showed that adding a peripheral venous lactate to the 2009 WHO warning signs improved the prediction of severe dengue in the febrile phase, so a lactate is a reasonable addition to the panel of a child who is being risk-stratified.[10]
Management — Resuscitation
The first action in a child who is shocked from dengue is airway, breathing and circulation: give high-flow oxygen, establish intravenous access, take a fingerprick glucose and draw blood for the investigations above while resuscitation proceeds.[3] The defining resuscitation principle in dengue is that aggressive fluid boluses cause harm — this is the dengue translation of the broader lesson from the FEAST trial that boluses are not benign in severe febrile illness in children.[9]
For compensated shock with a narrow pulse pressure but a preserved systolic blood pressure, give 10 to 20 mL per kilogram of isotonic crystalloid (0.9 per cent saline or Hartmann's solution) over one hour, then reassess perfusion, haematocrit and urine output before deciding whether to continue.[3] For hypotensive shock, give a 20 mL per kilogram bolus of crystalloid or colloid more rapidly and reassess within 15 to 30 minutes; if shock persists, repeat the bolus and escalate to a critical-care setting, because ongoing shock in dengue signals active leak, major bleeding, or both.
Correct hypoglycaemia with intravenous glucose, treat acidosis by improving perfusion rather than by bicarbonate, and transfuse packed red cells for major bleeding. Platelet and fresh-frozen plasma transfusions are reserved for active, clinically significant bleeding or a clear bleeding tendency, not for a low platelet number on its own.[3]
Medications to avoid are as important as those to give. Aspirin and other non-steroidal anti-inflammatories are contraindicated because of the bleeding risk and the association of aspirin with Reye syndrome; corticosteroids have no proven benefit and are not used; prophylactic platelet transfusion for thrombocytopenia without bleeding does not improve outcome.[3] Paracetamol is the only antipyretic recommended for fever control.
Management — Definitive & Stepwise
The WHO three-group scheme operationalises the 2009 classification into a management plan. Group A children — dengue without warning signs, orally tolerated, with adequate urine output and no co-morbidity — are managed as outpatients with oral fluids, paracetamol, daily review and a clear safety-net for the warning signs.[3]
Group B children — those with any warning sign, with co-morbidity such as asthma or a chronic illness, or with social factors that compromise review — are admitted for close monitoring and titrated intravenous isotonic crystalloid at a maintenance rate adjusted to the haematocrit and clinical perfusion. The WHO handbook recommends 5 to 7 mL per kilogram per hour for the first few hours in a child with warning signs, titrated down as the haematocrit stabilises.[3]
Group C children — severe dengue with shock, respiratory distress, severe bleeding or organ impairment — are managed in a high-dependency or intensive-care setting with the resuscitation above, hourly reassessment, and transfusion for bleeding. The transition to recovery is marked by a falling haematocrit, a widening pulse pressure, returning appetite and a diuresis, and intravenous fluids are tapered over 24 to 48 hours to avoid overload.[3]
The seven WHO warning signs — 'ABDOMEN'
The key disposition thresholds for discharge are an afebrile child who is drinking, passing urine, has a stable or falling haematocrit, a rising platelet count, a widening pulse pressure, and no respiratory distress. A platelet count that has not yet normalised is not a barrier to discharge in a clinically well child.[3]
Zika has no specific antiviral treatment; management is supportive and the focus is on identifying pregnancy (so that fetal surveillance can be arranged), counselling on the risk of sexual and vertical transmission, and arranging developmental surveillance for infants with confirmed or suspected congenital Zika syndrome.[11] Chikungunya is also managed supportively, with paracetamol for fever and, once dengue is excluded, non-steroidal anti-inflammatories for the arthralgia; physiotherapy helps children with persistent joint involvement.[15]
Specific Subtypes & Scenarios
Secondary dengue infection is the highest-severity scenario and the one most likely to be tested in a viva or structured oral. A child with a documented or probable prior dengue infection who presents with a new febrile illness in an endemic or outbreak setting should be admitted earlier, monitored more closely, and treated with a lower threshold for intravenous fluid.[2]
Dengue in infancy is atypical. Maternal dengue antibody wanes over the first six to twelve months of life, creating a window in which residual non-neutralising maternal antibody can drive antibody-dependent enhancement on first infection, so infants can present with a sepsis-like illness, a rapid progression to shock, and atypical features such as coryza or poor feeding that mislead toward a bacterial diagnosis.[2]
Congenital Zika syndrome is the subtype that has reshaped travel medicine and prenatal counselling since 2015. The infant presents with microcephaly, hypertonia and irritability, feeding difficulty, seizures, arthrogryposis, ocular findings such as chorioretinal scars, and sensorineural hearing loss. A nationwide Brazilian cohort confirmed a substantial excess mortality in the first years of life for children with congenital Zika syndrome, so these infants need long-term multidisciplinary developmental, seizure, feeding and sensory surveillance.[12]
Neonatal chikungunya is acquired through vertical transmission when the mother has viraemia around the time of delivery. The neonate develops fever, rash, irritability and, in severe cases, encephalopathy and bleeding, and needs admission, supportive care and exclusion of bacterial sepsis.[15]
Dengue in pregnancy carries a higher risk of severe maternal disease, of vertical transmission producing neonatal dengue, and of adverse fetal outcomes including preterm birth and fetal loss, so a pregnant adolescent with dengue needs inpatient monitoring and obstetric involvement.[3]
A returned-traveller child with fever and thrombocytopenia in a non-endemic country brings dengue, malaria and enteric fever together in the differential, and the first-hour investigations must include a thick and thin blood film and rapid malaria test, dengue NS1 and serology, blood cultures and a full blood count, because each of these diagnoses has a different time-critical treatment.[2]
Complications & Pitfalls
Dengue shock syndrome is the most feared complication and, if fluid is mismanaged, can progress to multiorgan failure. Severe bleeding — gastrointestinal, intracranial or mucosal — is the other major life-threatening complication and is the indication for blood product support.[3]
Less common but important complications include dengue encephalopathy and encephalitis, myocarditis, hepatitis with acute liver failure, acute kidney injury, and a haemophagocytic syndrome. In the recovery phase the chief iatrogenic complication is fluid overload, which produces pulmonary oedema and respiratory distress when intravenous fluids are not tapered as the leak resolves.[3]
The classic pitfalls are worth memorising because examiners return to them. Giving prophylactic platelets for a low platelet count without bleeding, using aspirin or ibuprofen for fever, treating a stable child with a "preventive" fluid bolus, discharging a child at defervescence because the temperature has settled, and labelling a child with secondary dengue as a simple viral illness are the five errors that cost the most marks and the most lives.[3]
In congenital Zika syndrome the long-term complications are neurological: epilepsy that is often difficult to control, cerebral palsy with marked hypertonia, severe global developmental delay, cortical visual impairment, sensorineural hearing loss, and feeding difficulty requiring gastrostomy.[12] After chikungunya a subset of children develop a chronic relapsing arthropathy that lasts months to years and needs rheumatology and physiotherapy input.[15]
Prognosis & Disposition
Uncomplicated dengue in a well-monitored child recovers fully within a week to ten days, with a case fatality below one per cent when warning signs are recognised and fluid is managed well. Severe dengue untreated carries a case fatality approaching 20 per cent, and this falls to below one per cent with early, titrated fluid and supportive care — a margin that is the entire point of the disease for an exam candidate.[3]
The discharge criteria, restated, are clinical and laboratory stability: an afebrile child who is eating and drinking, passing urine, has a stable or falling haematocrit, a rising platelet count, a widened pulse pressure, and no respiratory distress. Follow-up is arranged to confirm platelet recovery over the following one to two weeks, and the family is counselled that a future dengue infection with a different serotype carries a higher risk of severe disease.[3]
The prognosis for congenital Zika syndrome is dominated by the severity of the brain injury, which ranges from subtle developmental delay in mildly affected children to severe cerebral palsy, epilepsy and visual impairment in the classic syndrome; a Brazilian nationwide cohort demonstrated a marked excess of early mortality in the most severely affected infants.[12] Chikungunya arthralgia resolves in most children within weeks, but a minority have persistent post-chikungunya rheumatism.[15]
Special Populations
Infants are a high-risk group because of the maternal-antibody enhancement window and because they present atypically. A febrile infant under one year with a dengue exposure needs a lower threshold for admission, a haematocrit and platelet trend, and a clear plan for escalation.[2]
Returned travellers, recent migrants, and refugee and asylum-seeker families arriving from dengue-, Zika- or chikungunya-endemic regions may present in a non-endemic country where the diagnosis is not the first thought, so a routine travel history on every febrile child is the safeguarding habit that catches arboviral disease.[2] An interpreter should be offered where language is a barrier, and the family's understanding of the safety-net should be checked.
Pregnant adolescents exposed to Zika need urgent assessment of the pregnancy, fetal ultrasound surveillance for microcephaly and intracranial calcifications, counselling about the risk of congenital Zika syndrome, and a plan for the neonate.[11] Immunocompromised children and those with complex chronic disease are at higher risk of severe dengue and atypical courses, and need a lower threshold for inpatient management.[3]
Indigenous and remote-rural children in tropical northern Australia are exposed to locally-acquired dengue during outbreaks and may also carry comorbidities such as rheumatic heart disease, chronic lung disease or skin infection that complicate the course. Housing quality, the presence of intact fly-screens, and standing water around the home are the social determinants that turn an imported case into an outbreak, and vector control plus community engagement are part of the paediatric response.[3]
Children living in socioeconomic disadvantage face a higher exposure through water-storage practices that breed Aedes and through limited access to repellent, screens and timely care, so the preventive conversation is as much about the home as about the bite.[1]
Evidence, Guidelines & Regional Differences
The 2009 WHO dengue classification and the companion TDR handbook for diagnosis, treatment, prevention and control are the foundation documents for paediatric dengue management, and their three-category scheme was validated prospectively in multicentre studies that showed better agreement and earlier recognition of severe disease than the older 1997 scheme.[4] The 2018 WHO dengue vaccine position paper, updated in 2024, sets out the current recommendations for the two principal live-attenuated tetravalent vaccines.[8]
The first licensed vaccine, CYD-TDV (Dengvaxia, Sanofi), showed overall efficacy in phase 3 but a worrying signal: in seronegative recipients it increased the rates of hospitalisation and severe dengue, consistent with vaccine-mediated primary sensitisation and later antibody-dependent enhancement.[5] On that basis CYD-TDV is recommended only for seropositive children, typically those aged nine to sixteen years living in high-transmission settings, and prevaccination screening is essential.
The newer vaccine, TAK-003 (Qdenga, Takeda), showed efficacy against symptomatic dengue in a phase 3 trial of children and adolescents, with strong protection against DENV-1 and DENV-2 and a good short-term safety profile.[6] The 4.5-year follow-up confirmed durable protection against hospitalisation but showed waning efficacy against DENV-3 and an uncertain benefit in seronegative recipients, which has kept the WHO recommendation cautious about use in seronegative individuals.[7]
The fluid-management evidence base has been shaped by the broader lesson from the FEAST trial in African children with severe febrile illness, that bolus fluids are not benign; dengue guidelines therefore favour crystalloid over colloid as first-line and emphasise titration and reassessment over protocol-driven boluses.[9] The systematic review of warning-sign predictors by Sangkaew and colleagues quantified the prognostic value of each warning sign and underpins the current emphasis on early admission for any child with one.[9]
Regional practice differs in operational ways. Australia and New Zealand see imported cases and the rare north-Queensland local outbreak, with no routine vaccine; the UK, Canada and much of Europe report increasing imported paediatric dengue alongside travel; and endemic countries in Asia and the Americas integrate TAK-003 and CYD-TDV into national programmes for seropositive children.[8] For Zika, the Americas retain the largest cohort of affected children and the deepest experience of congenital Zika syndrome surveillance, while ANZ and European practice is dominated by travel-related exposure counselling in pregnancy.
Exam Pearls
Carry these single-testable facts into the written and clinical exam. The dangerous phase of dengue begins at defervescence, not at the fever peak. The leak is reversible and lasts 24 to 48 hours. A rising haematocrit with a falling platelet count is the leak signature, and you recheck it every six to twelve hours. Pulse pressure below 20 mmHg defines dengue shock. NS1 antigen is positive in the first five days; IgM rises from day four to five. Aspirin and non-steroidal anti-inflammatories are contraindicated; paracetamol only.[3]
The vaccine facts are high-yield because they test mechanism as well as policy. CYD-TDV (Dengvaxia) is contraindicated in seronegative children because it increased hospitalisation in that group; TAK-003 (Qdenga) has good efficacy against DENV-1 and DENV-2 with waning DENV-3 protection and caution in seronegatives.[5][7] Zika questions test your knowledge that it is teratogenic: ask about pregnancy, recognise congenital Zika syndrome as microcephaly with intracranial calcifications and arthrogryposis, and counsel on sexual and vertical transmission.[11] Chikungunya questions test the triad of fever, rash and severe small-joint arthralgia, and the neonatal vertical-transmission risk at delivery.[14]
Finally, the vector-control and prevention answer is the same for all three: the day-biting Aedes mosquito, breeding-site elimination, long sleeves, intact screens and repellent containing DEET or picaridin — and, where indicated, selective vaccination of seropositive children against dengue.[1]
References
- [1]Bhatt S, Gething PW, Brady OJ, et al. The global distribution and burden of dengue. Nature, 2013.PMID 23563266
- [2]Guzman MG, Harris E Dengue. Lancet, 2015.PMID 25230594
- [3]Wilder-Smith A, Ooi EE, Horstick O, Wills B Dengue. Lancet, 2019.PMID 30696575
- [4]Alexander N, Balmaseda A, Coelho IC, et al. Multicentre prospective study on dengue classification in four South-east Asian and three Latin American countries. Trop Med Int Health, 2011.PMID 21624014
- [5]Hadinegoro SR, Arredondo-García JL, Capeding MR, et al. Efficacy and Long-Term Safety of a Dengue Vaccine in Regions of Endemic Disease. N Engl J Med, 2015.PMID 26214039
- [6]Biswal S, Reynales H, Saez-Llorens X, et al. Efficacy of a Tetravalent Dengue Vaccine in Healthy Children and Adolescents. N Engl J Med, 2019.PMID 31693803
- [7]Tricou V, Yu D, Valdez I, et al. Long-term efficacy and safety of a tetravalent dengue vaccine (TAK-003): 4.5-year follow-up of a randomised controlled trial. Lancet Glob Health, 2024.PMID 38245116
- [8]World Health Organization Dengue vaccine: WHO position paper, September 2018 - Recommendations. Vaccine, 2019.PMID 30424888
- [9]Sangkaew S, Ming D, Boonyasiri A, et al. Risk predictors of progression to severe disease during the febrile phase of dengue: a systematic review and meta-analysis. Lancet Infect Dis, 2021.PMID 33640077
- [10]Thanachartwet V, Wattanathum A, Oer-Areemitr N, et al. Diagnostic accuracy of peripheral venous lactate and the 2009 WHO warning signs for identifying severe dengue in Thai adults: a prospective cohort study. BMC Infect Dis, 2016.PMID 26832147
- [11]Rasmussen SA, Jamieson DJ, Honein MA, Petersen LR Zika Virus and Birth Defects - Reviewing the Evidence for Causality. N Engl J Med, 2016.PMID 27074377
- [12]Paixao ES, Cardim LL, Brickley EB, et al. Mortality from Congenital Zika Syndrome - Nationwide Cohort Study in Brazil. N Engl J Med, 2022.PMID 35196428
- [13]Coyne CB, Lazear HM Zika virus - reigniting the TORCH. Nat Rev Microbiol, 2016.PMID 27573577
- [14]Fischer M, Staples JE Notes from the field: chikungunya virus spreads in the Americas - Caribbean and South America, 2013-2014. MMWR Morb Mortal Wkly Rep, 2014.PMID 24898168
- [15]Carrillo FAB, Ojeda S, Balmaseda A, et al. Comparison of dengue, chikungunya, and Zika among children in Nicaragua across 18 years: a single-centre cohort study. Lancet Child Adolesc Health, 2025.PMID 40774783