Paeds · infectious-diseases
Device-associated and healthcare-associated infection
Also known as Device-associated infection · Healthcare-associated infection · CLABSI · CAUTI · Ventilator-associated pneumonia · Hospital-acquired infection
A fellowship approach to device-associated and healthcare-associated infection in children, covering NHSN surveillance definitions (CLABSI, CAUTI, ventilator-associated events), Clostridioides difficile and surgical-site infection, biofilm pathophysiology, multimodal prevention bundles, antimicrobial stewardship, source control, regional surveillance systems, and the disproportionate burden borne by neonatal, critical-care and technology-dependent children.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A previously well toddler admitted for a seizure now has a central venous catheter for antibiotics, and on day five spikes a fever with a positive blood culture drawn through the line. A preterm infant in neonatal intensive care develops apnoea and a raised C-reactive protein while on parenteral nutrition through a long line. A ventilated adolescent in paediatric intensive care grows Pseudomonas from a deep respiratory specimen after a week of intubation. Each is a healthcare-associated infection, and each is bound to a device that has become its own portal of entry. [1] [12]
A healthcare-associated infection is one that was neither present nor incubating at admission, with onset conventionally more than 48 hours after admission or clearly linked to a prior healthcare exposure such as an indwelling device, a procedure, or recent hospitalisation. The device-associated subset — central-line-associated bloodstream infection (CLABSI), catheter-associated urinary tract infection (CAUTI), and ventilator-associated pneumonia or ventilator-associated event — is where prevention work yields its largest returns, because the device is a modifiable risk factor that can be inserted well, maintained well, and removed early. [1] [3] [12]
Three ideas run through this topic and bind it together. Prevent with a bundle rather than a single intervention, because device infection is multifactorial and no one action is sufficient. Survey with standard NHSN definitions so that rates are comparable across units and time, and so that outbreaks are detected. Steward devices and antimicrobials together, because every additional device-day and antibiotic-day selects for the resistant, biofilm-forming organisms that cause the hardest infections. [1] [2] [12]
From device insertion to infection prevention
Insert well
Hand hygiene, maximal sterile barriers, chlorhexidine skin preparation, optimal site selection — performed by a trained operator.
Maintain well
Aseptic access, scrub the hub, daily review of necessity, intact dressing, and removal as soon as the device is no longer essential.
Survey
Apply NHSN definitions; track CLABSI, CAUTI and ventilator-associated events as rates per 1000 device-days; feed data back to the unit.
Recognise and respond
Sample before antibiotics, remove or replace the infected device, treat with targeted antimicrobials, and review the bundle for the system failure.
Classification
Device-associated infections are best understood through their surveillance definitions, because the definitions drive both clinical care and the quality data that compare units. CLABSI is a laboratory-confirmed bloodstream infection in a patient with a central line in place for more than two calendar days, where the infection is not related to an infection at another site. CAUTI requires a urinary catheter in place for more than two calendar days together with symptoms and a urine culture meeting the set threshold. Ventilator-associated pneumonia, now nested within the broader ventilator-associated event algorithm, follows intubation for more than two days with worsening oxygenation and radiological or microbiological evidence of lung infection. [1] [3] [7]
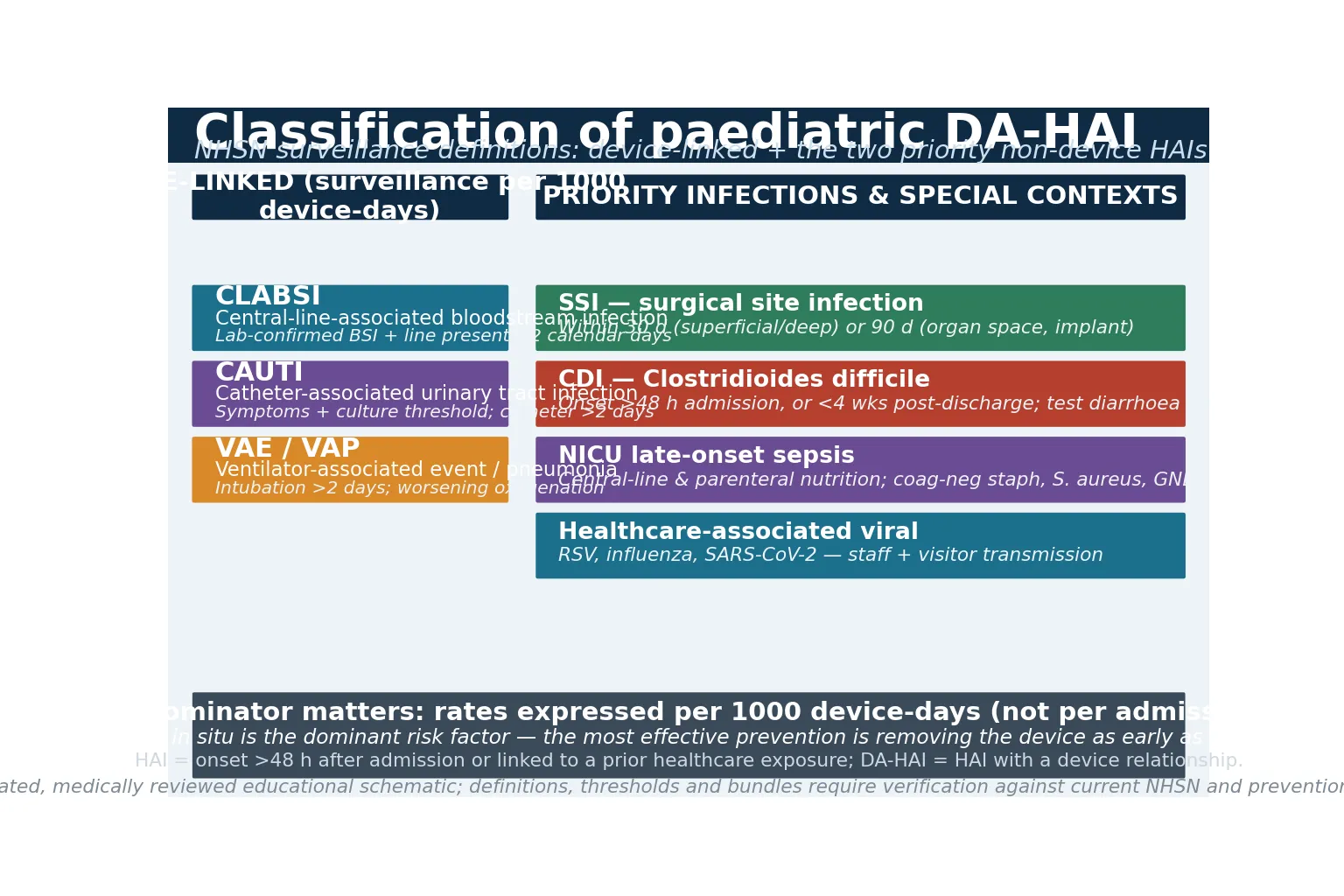
Two priority infections are not device-linked but share the same prevention logic and belong in the same answer. Surgical-site infection occurs within 30 days of a procedure (or within 90 days if an implant is placed), classified as superficial incisional, deep incisional, or organ-space. Clostridioides difficile infection is defined by clinically significant diarrhoea together with a positive test or endoscopic evidence of pseudomembranous colitis, with onset more than 48 hours after admission or within four weeks of discharge. Both are quintessentially iatrogenic: the first from a breach in sterile technique, the second from antimicrobial disruption of the gut microbiome. [9] [10] [12]
A useful distinction to state plainly to an examiner is the difference between a surveillance definition and a clinical decision. A unit counts a CLABSI against its denominator to drive quality work, but at the bedside the clinician treats the child with bacteraemia and removes the line on clinical grounds regardless of whether every surveillance nuance is met. Holding definitive treatment while the infection prevention team adjudicates a definition is a common and harmful error. [1] [3]
Epidemiology & Risk Factors
The burden of healthcare-associated infection falls on the smallest and the sickest children. A large analysis of critically ill children across United States hospitals from 2013 to 2018 found that the majority of device-associated infections were concentrated in paediatric and neonatal intensive care, and that infection independently prolonged length of stay and increased mortality. The same pattern holds internationally: the risk is carried by neonates, by technology-dependent and complex-chronic children, and by those with long hospitalisations and multiple device-days. [1] [2]
Antimicrobial resistance compounds the harm. A National Healthcare Safety Network summary of paediatric data from 2015 to 2017 showed that a substantial proportion of device-associated pathogens were resistant to first-line agents, with particularly high resistance among Gram-negative bacilli and staphylococci. Resistant infections lengthen stay, narrow therapeutic options, and concentrate where device and antibiotic exposure are greatest — neonatal units, oncology, and intensive care. [2]
The single greatest risk factor for a device-associated infection is the device itself, and the risk rises with each day it remains in situ. Beyond dwell time, prematurity and very low birth weight, immunocompromise from malignancy or transplantation, parenteral nutrition, breaks in sterile or aseptic technique, dense skin colonisation, hand-hygiene lapses, and broad-spectrum antibiotic exposure each add risk. The good news is that most of these are modifiable, which is why bundles work. [1] [5] [6]
Neonate / NICU
Highest CLABSI rate
- Very low birth weight, immature skin, long lines and parenteral nutrition
- Late-onset sepsis often device-related; coag-neg staph, S. aureus, Gram-negatives
- Bundle insertion and removal reduces bacteraemia
- Every line-day is a measured risk
PICU / ventilated
Multi-device
- Central lines, arterial lines, urinary catheters, endotracheal tubes together
- Ventilator-associated pneumonia follows prolonged intubation
- Daily sedation interruption and device review
- Chlorhexidine bathing reduces Gram-positive bacteraemia
Ward / complex-chronic
Community devices
- Long-term central lines for oncology, short bowel, metabolic disease
- Caregivers perform line care at home
- Maintenance bundle and clear safety-net
- Plan removal or replacement at the first sign of tunnel infection
Pathophysiology
A device becomes infected because it breaches the defences that normally keep organisms out — skin, mucosa, and the urinary and respiratory tracts — and because it offers a surface on which organisms settle into a biofilm. The cascade begins at insertion or at later access: skin flora or water-borne organisms gain entry at the exit site or the hub, migrate along the external surface or the internal lumen, and adhere to the device material. [3] [12]
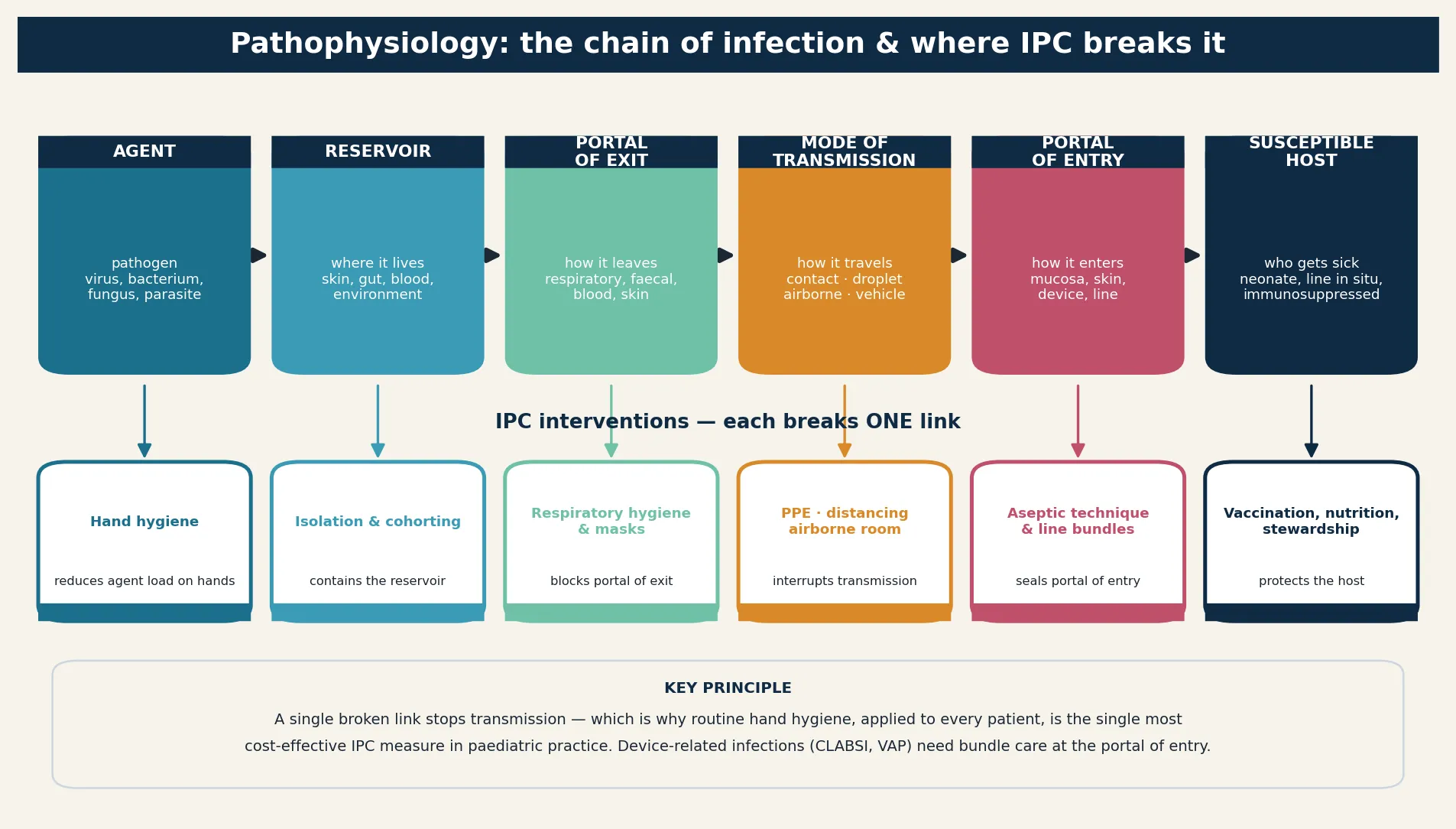
Once organisms adhere, they secrete an extracellular matrix and grow as a sessile biofilm community. Within the biofilm, bacteria and fungi are metabolically quiescent and physically shielded, so antibiotics that kill planktonic cells in a blood culture may fail to eradicate the device nidus. Periodically, planktonic cells shed into the bloodstream, the bladder, or the lower airway, producing the clinical infection and seeding distant foci. This is why a single negative culture does not prove a line is uninfected, and why removing an infected device is often both diagnosis and cure. [3] [12]
The organisms follow the device. Central lines grow coagulase-negative staphylococci, Staphylococcus aureus, enterococci, Candida, and water-borne Gram-negative bacilli such as Klebsiella, Enterobacter, and Pseudomonas. Urinary catheters favour Escherichia coli, other Enterobacterales, enterococci, Pseudomonas, and Candida. Endotracheal tubes are colonised first, then seeded by Staphylococcus aureus, Pseudomonas, and other hospital-acquired Gram-negatives. Broad-spectrum antibiotics reshape this flora toward resistance, which is why stewardship and device removal are inseparable. [2] [7] [12]
Clinical Presentation
Presentation depends on the device and the organism, but the common thread is a new clinical change in a child who has a device in place. Fever is the most frequent signal, but in neonates and immunocompromised children the signs are blunted: temperature instability, apnoea, feeding intolerance, lethargy, or simply a deterioration in observations that the nurse or caregiver attributes to the child not being themselves. Any such change in a device-dependent child should trigger sampling before antibiotics. [1] [5]
A central-line infection declares itself at the line or in the blood. Look for erythema, tenderness, pus, or induration at the exit site, and for a tunnel or pocket infection along the subcutaneous tract or around a port. Rigors during or immediately after line access are a strong clue to an intraluminal source. Bacteraemia may present as sepsis with cardiovascular instability, and Staphylococcus aureus bacteraemia raises the stakes because of its tendency to seed distant foci such as endocarditis, osteomyelitis, or septic arthritis. [3] [12]
A urinary catheter infection presents with fever, dysuria or suprapubic tenderness where the child can report it, cloudy or malodorous urine, or new confusion in a vulnerable child — though many catheterised children are pre-verbal or neurologically impaired, so haemodynamic change or unexplained deterioration may be the only sign. A ventilator-associated pneumonia presents with new or worsening infiltrates on chest imaging, purulent respiratory secretions, worsening oxygenation, and fever or leucocytosis after 48 hours of ventilation. C. difficile presents with watery, sometimes bloody diarrhoea in a child exposed to antibiotics, and may progress to severe colitis with abdominal pain, distension, and shock. [7] [9] [10]
Differential Diagnosis
The differential splits into three questions held at once: is this device infection, what else could explain the picture, and which organism is most likely? The hardest decision is often whether fever in a device-dependent child is infection at all. Drug fever, transfusion or reaction to blood product, postoperative inflammatory response, atelectasis, and a coincidental viral illness can all mimic device infection, and a single positive culture of a skin commensal may reflect contamination rather than true bacteraemia. [1] [3]
Separating true bacteraemia from contamination matters because overtreatment drives resistance and C. difficile. A single bottle of coagulase-negative staphylococci in an otherwise well child is more likely contamination, whereas the same organism in multiple bottles drawn from separate sites, with clinical deterioration and rising inflammatory markers, is a line infection until proven otherwise. The time to positivity, the identity of the organism, and the clinical context together guide the call. [3] [12]
Other hospital-acquired infections belong in the same differential because they coexist and overlap. Surgical-site infection after an operation, a healthcare-acquired respiratory virus such as respiratory syncytial virus or influenza transmitted on the unit, and C. difficile after antibiotics can each explain fever in a hospitalised child and may coexist with a device infection. A child with a central line and new diarrhoea after broad antibiotics could have both line sepsis and C. difficile, and each must be sought deliberately. [9] [10] [11]
Clinical & Bedside Assessment
Bedside assessment begins with the primary survey, because a device-dependent child with new fever can deteriorate quickly. Address airway, breathing, and circulation, attach monitoring, estimate weight, and measure capillary refill, pulse quality, perfusion, and mentation. A bedside glucose is essential, because the septic infant is often hypoglycaemic. Once the child is stable, examine the device itself with the same rigour as any organ. [1] [3]
Inspect every vascular access device at the exit site and along its tunnel. Look for erythema, warmth, tenderness, pus, and the extent of any induration, and compare it with the documented baseline dressing and appearance. Inspect the urinary catheter for blockage or bypass, and the endotracheal tube for position, secretions, and cuff integrity. Ask when the device was inserted and when it was last accessed, reviewed, and dressed, and check that a daily indication is documented. [3] [7]
The focused history targets the device, the host, and the trajectory. Ask about the indication for the device, the planned duration, any recent manipulation or break in the dressing, the antimicrobial history, the immune status, the underlying diagnosis, and exactly what the nurse or caregiver has noticed change. A surgical child needs the wound examined and the operative and antibiotic prophylaxis history taken, and any child with recent antibiotics and diarrhoea needs a C. difficile assessment. [9] [10] [12]
Investigations
Investigations serve two purposes: to confirm the device syndrome and to find the organism so that therapy can be narrowed. For suspected line infection, draw blood cultures from a peripheral vein and from each lumen of the line before starting antibiotics, because a culture from the line that turns positive much faster than the peripheral culture (a short differential time to positivity) supports an intraluminal source. Add a full blood count and differential, C-reactive protein, electrolytes, renal and liver function, and coagulation, and a lactate if the child is unwell. [3] [12]
A urinary catheter infection is confirmed by a culture meeting the colony-forming-unit threshold from a specimen collected aseptically, ideally after replacing the catheter so that the specimen reflects the bladder rather than the biofilm on an old catheter. A ventilator-associated pneumonia is supported by lower respiratory tract sampling — semi-quantitative aspirate or bronchoalveolar lavage — interpreted with the radiological and clinical picture. Imaging is targeted: chest radiograph or ultrasound for pneumonia and effusion, abdominal imaging for suspected C. difficile colitis with distension, and echocardiography for Staphylococcus aureus bacteraemia to exclude endocarditis. [7] [9]
LINE — preventing central-line-associated bloodstream infection
For suspected C. difficile, send a stool toxin assay or a nucleic acid amplification test on a formed-or-loose but not faunally-formed specimen, remembering that testing asymptomatic children and infants is unhelpful because carriage is common in infancy. Molecular tests are sensitive but cannot distinguish colonisation from disease, so the result must be interpreted with the clinical picture of significant diarrhoea. [9] [10]
Management — Resuscitation
Resuscitation and source control run together, and both begin the moment device infection is suspected. A device-dependent child with new fever and signs of sepsis is treated as septic until proven otherwise: assign a leader, call for senior and critical-care help, attach monitoring, give oxygen and fluid aliquots for shock, and take cultures before the first antibiotic only if it does not delay the dose. The principles of paediatric sepsis resuscitation apply without modification here. [1] [3]
Source control for device infection is, above all, removal of the device. An infected central line should be removed and, if access is still required, replaced at a new site or over a wire only when strict criteria are met and never if there is a tunnel or pocket infection, sepsis, or a resistant organism. An infected urinary catheter should be removed or replaced, with a specimen taken before the catheter is changed. For ventilator-associated pneumonia, source control means reducing the duration of intubation through daily sedation interruption, spontaneous breathing trials, and extubation readiness. [3] [7] [8]
Empiric antimicrobials cover the likely device organisms modified by local resistance and the child's immune status. For suspected line infection in a stable child, cover coagulase-negative staphylococci and Staphylococcus aureus; broaden to Gram-negative and anti-pseudomonal cover, and add antifungal cover, for the septic, neutropenic, or long-stay child according to local guidance. For ventilator-associated pneumonia, cover early with anti-MRSA and anti-pseudomonal agents if risk factors exist, then narrow rapidly to culture results. For C. difficile, stop the offending antibiotic where possible and start oral metronidazole or, for severe or recurrent disease, oral vancomycin or fidaxomicin per current paediatric guidance. [7] [9] [12]
Management — Definitive & Stepwise
Definitive management converts empiric therapy into targeted therapy as the organism and its sensitivities return. The aims are to remove the infected nidus, to narrow the antimicrobial to the narrowest effective agent, and to shorten the course to the shortest duration that achieves cure. Every clinical decision is paired with a system decision: which bundle element failed, and how the unit will prevent the next infection. [1] [12]
Antimicrobial principles in device-associated infection (verify against current local guidance)
Antimicrobial therapy is de-escalated the moment sensitivities allow, and stopped when infection is excluded. A contaminated culture, a sterile source of fever, or an alternative diagnosis should end the antibiotic course rather than extend it. The duration of therapy follows the syndrome and the organism: a short course for an uncomplicated CLABSI after line removal and rapid clearance of bacteraemia, a longer course for Staphylococcus aureus bacteraemia or endocarditis, and a defined course for ventilator-associated pneumonia guided by clinical resolution. Daily stewardship review is what prevents the harm of unnecessary, prolonged, or broad therapy. [2] [7] [12]
Source control is completed by addressing the underlying reason the device was needed in the first place. A child whose central line is required only because enteral feeding has not been established should have a feeding plan that makes the line redundant; a child whose ventilator dependence reflects failure of a sedation wean should have that addressed. The most reliable prevention for every device-associated infection is a device that has been removed. [3] [12]
Specific Subtypes & Scenarios
Different device syndromes demand different first moves, and a candidate should be able to state them clearly. CLABSI needs paired cultures, a clinical decision on line removal, and antistaphylococcal cover broadened for the septic or immunocompromised host. CAUTI needs a specimen taken before antibiotics and ideally after catheter replacement, removal of the catheter where possible, and explicit avoidance of treating asymptomatic bacteriuria. Ventilator-associated pneumonia needs lower respiratory sampling, de-escalation of sedation, head-up positioning, oral care, and antimicrobials narrowed and shortened to the clinical response. [3] [7] [8]
Recognise-to-resolution pathway for device infection
The surgical-site infection scenario turns on the depth of infection and the operative context. A superficial infection may need opening the wound, culture, and oral antibiotics; a deep or organ-space infection needs imaging, drainage or debridement, intravenous antibiotics, and review of perioperative antibiotic prophylaxis and sterile technique. C. difficile after antibiotics requires stopping the inciting agent, testing stool, and starting targeted therapy, with escalation of care for severe colitis characterised by pseudomembranous change, toxic megacolon, or shock. [9] [10]
The technology-dependent child at home with a long-term central line turns on the personal baseline and the caregiver's report. A caregiver who says the child is not themselves, with fever and a line in situ, should be assessed urgently with paired cultures and a low threshold to remove the line if it is infected. These children and their families carry out line care at home, so the maintenance bundle and a clear, written safety-net for fever are part of their discharge plan. [3] [6]
Complications & Pitfalls
The complications of device infection and of its treatment overlap, and both must be sought actively. Untreated or late-treated device sepsis causes bacteraemia, septic shock, disseminated intravascular coagulation, acute kidney injury, and metastatic infection — endocarditis, osteomyelitis, and septic arthritis — particularly with Staphylococcus aureus. Treatment-related harm includes antimicrobial adverse effects, C. difficile after broad therapy, line and procedure complications, and the selection of resistant organisms that cause the next infection. [1] [2] [9]
Define
- Onset >48 h after admission or healthcare-linked
- Device in situ >2 days defines device-association
- Rates per 1000 device-days
- Count CLABSI, CAUTI, VAE, SSI, CDI
Prevent
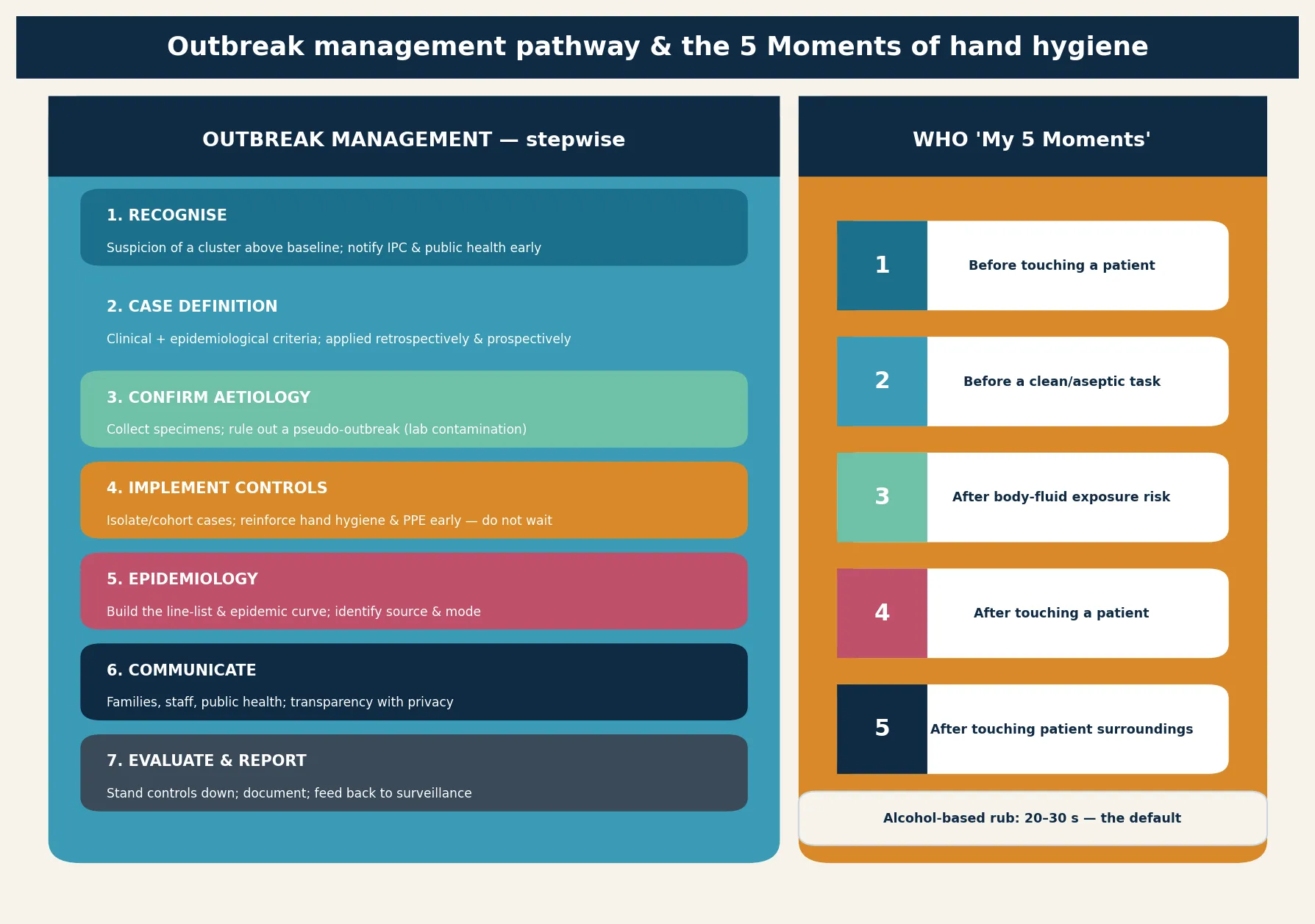
- Hand hygiene at the 5 moments
- Maximal sterile barriers at insertion
- Chlorhexidine preparation and site choice
- Daily review of device necessity
Recognise
- New fever or deterioration with a device
- Line-site signs or rigors on access
- Avoid treating asymptomatic bacteriuria
- Treat sepsis while the definition is adjudicated
Manage
- Cultures before antibiotics
- Remove or replace the infected device
- De-escalate to the organism
- Shorten to the shortest effective course
System
- Surveillance and feedback of rates
- Stewardship of devices and antibiotics
- Outbreak detection and response
- DA-HAI is an avoidable harm, not an inevitability
“Device in situ >2 days + HAI → surveillance definition → bundle (hand hygiene, barriers, chlorhexidine, daily review) → cultures before antibiotics → remove the device → de-escalate and shorten → feed rates back to the unit.”
The common cognitive pitfalls cluster around three failures. Failure to prevent happens when a device is inserted without a full bundle or left in place with no documented indication. Failure to recognise happens when fever in a device-dependent child is attributed to a coincidental viral illness, or when a single culture of a skin commensal is dismissed without the full clinical context. Failure to remove happens when an infected line is salvaged in the face of sepsis, a tunnel infection, or a high-risk organism because removing it is inconvenient. Each failure is preventable with bundle discipline and a low threshold to remove. [3] [5] [12]
A subtle pitfall is treating the surveillance definition as the trigger for clinical action. The infection prevention team may reclassify a case weeks later; the bedside clinician must treat the child and remove the device on clinical grounds the day the infection is suspected. Waiting for adjudication is the same error as waiting for cultures in sepsis — the child is treated first. [1] [3]
Prognosis & Disposition
Prognosis depends on early recognition, prompt source control, and timely targeted antimicrobials, and on the host. Children who recover quickly after device removal and de-escalated therapy do well; those with delayed recognition, resistant organisms, or metastatic infection face prolonged stays, organ failure, and higher mortality. Healthcare-associated infection independently prolongs length of stay and increases mortality in critically ill children, which is why it is treated as a patient-safety event rather than a complication to be accepted. [1] [2]
Disposition follows severity, trajectory, and the need for ongoing device access. Any child with device sepsis, persistent bacteraemia, or haemodynamic instability belongs in a high-dependency or intensive-care setting. The child who responds to device removal and de-escalated therapy may step down to the ward with clear escalation criteria. A plan to replace a needed device must specify the site, the operator, and the bundle, so that the next line is not inserted under the same conditions that caused the first infection. [1] [12]
Recovery is not the end of the episode for the unit or the family. The child needs follow-up of the organism and sensitivities, completion of the antimicrobial course, and surveillance for recurrence, relapse, or C. difficile after broad therapy. The unit needs a review of which bundle element failed and how rates are trending, and the family needs a clear, written safety-net and a plan for any device that remains. A device-associated infection that recurs on the same unit is a signal that the system, not the child, needs fixing. [2] [6] [12]
Special Populations
The neonate carries the highest burden and the bluntest signs. Late-onset sepsis in the neonatal intensive care unit is frequently device-related, driven by central lines, parenteral nutrition, and the immature skin and immune system of very low birth weight infants. Bundle-based insertion and maintenance, chlorhexidine preparation where age-appropriate, and early removal of lines reduce bacteraemia, and any unwell neonate with a line in situ is treated as having line sepsis until proven otherwise. [5] [6]
The immunocompromised child — oncology, transplant, primary immunodeficiency — deteriorates with muted signs and resistant, atypical organisms, including Candida and moulds. Cover broadly from the outset, remove any infected central line, and involve the oncology, transplant, or immunology team early, because their input shapes both the empiric regimen and the source-control plan. The technology-dependent child with a long-term line brings the prevention bundle into the home, where caregivers perform line care and a clear safety-net for fever is part of discharge. [2] [3] [12]
Australia and Aotearoa New Zealand: the Australian Commission on Safety and Quality in Health Care healthcare-associated infection program sets the national strategy, surveillance standards, and the National Hand Hygiene Initiative, while Royal Children's Hospital Melbourne intravenous-access and central-line guidance translates evidence into local pathways. Care for Aboriginal and Torres Strait Islander and Māori children must be culturally safe, given documented inequity in avoidable nosocomial harm for indigenous children. State and territory surveillance definitions, formularies, and retrieval rules vary and must be checked against the current local source.
[1][12]Global and low-resource settings: device-associated infection burdens are higher where staffing, consumables, and surveillance infrastructure are limited, and where antimicrobial stewardship is constrained. Apply the same bundle principles — hand hygiene, sterile barriers, hub care, daily review of necessity, and early removal — adapted to local resources, and prioritise the lowest-cost, highest-yield elements: hand hygiene and prompt device removal. Antimicrobial resistance is amplified where stewardship is weak, so narrow and shorten therapy wherever possible.
[1][2]Evidence, Guidelines & Regional Differences
The evidence for device-associated infection prevention is mature and unusually consistent: multimodal bundles work. The NACHRI quality-transformation collaborative showed that a standardised insertion and maintenance bundle reduced central-line-associated bloodstream infections across paediatric intensive care units in the United States, and comparable neonatal quality-improvement initiatives have reduced CLABSI in neonatal intensive care. Daily chlorhexidine bathing in critically ill children, tested in a multicentre cluster-randomised crossover trial, reduced Gram-positive bacteraemia, though its role in neonates is weighed against skin integrity and local guidance. [4] [5] [6]
The compendium of strategies to prevent healthcare-associated infections, and its periodic updates, distil the evidence into bundle elements for each device and each priority infection, and are the practical reference for acute-care hospitals. The IDSA/SHEA C. difficile guideline and the AAP clinical report on C. difficile in children set the diagnostic and therapeutic standard for that syndrome, including the central rule that testing and treating asymptomatic children, especially infants, is unhelpful. [9] [10] [12]
Antimicrobial resistance is the field's most pressing frontier. The NHSN paediatric summary documented substantial resistance among device-associated pathogens, and subsequent surveillance shows resistant Gram-negatives and staphylococci concentrating in neonatal and critical-care settings. The synthesis is a single, dual stewardship: steward the device by inserting well and removing early, and steward the antimicrobial by narrowing and shortening. Each prevents the resistant infection the next child would otherwise acquire. [2] [1]
Board and assessment distinctions
RACP current PREP curriculum candidates in 2026 must keep current learning objectives separate from the renewed curriculum goals applying to first-year trainees from 2027. RCPCH Progress+ outcomes are curriculum expectations, while MRCPCH Foundation of Practice, Theory and Science, and Applied Knowledge in Practice are theory classifications. The ABP General Pediatrics Content Outline classifies written examinations and includes patient-safety and quality domains that map directly to infection prevention. [12]
| Board or format | What the candidate must demonstrate |
|---|---|
| RACP DWE | Interpret a vignette of a hospitalised child with a device, identify the syndrome from its surveillance definition, and choose the safest first action |
| RACP DCE long case | Integrate device, host, organism and system factors into a prevention-to-disposition plan for a complex-chronic child |
| MRCPCH theory / clinical | Recognise device infection, state the prevention bundle, and explain the role of surveillance and stewardship to a family |
| ABP | Apply content and patient-safety domains to prevent, recognise and treat healthcare-associated infection |
| RCPSC structured oral | Manage an outbreak or a resistant device infection across rural or tertiary contexts with surveillance and escalation |
Exam Pearls
Viva: fever in a child with a central line at home
Treat as line sepsis until proven otherwise. Take paired peripheral and line cultures before antibiotics, give a broad empiric dose that covers staphylococci and the child's known flora, examine the exit site and tunnel, and arrange removal of the line if there is a tunnel infection, sepsis, persisting bacteraemia, or a high-risk organism. State the bundle that prevents the next infection and the safety-net the family carries at home. [3] [6] [12]
Structured oral: an outbreak of CLABSI on the NICU
Declare the cluster, convene the infection-prevention team, and review the bundle systematically — insertion technique, hub care, hand hygiene, and daily review of line necessity. Apply NHSN definitions to confirm cases and calculate rates per 1000 line-days, look for a common organism and a common failure by molecular typing and observation, and act on the highest-yield element first. Feed rates back to staff and sustain the audit, because outbreaks recur where surveillance lapses. [1] [5] [12]
References
- [1]Hsu, H E; Mathew, R; Wang, R Health Care-Associated Infections Among Critically Ill Children in the US, 2013-2018. JAMA pediatrics, 2020.PMID 33017011
- [2]Weiner-Lastinger, L M; Abner, S; Benin, A L Antimicrobial-resistant pathogens associated with pediatric healthcare-associated infections: Summary of data reported to the National Healthcare Safety Network, 2015-2017. Infection control and hospital epidemiology, 2020.PMID 31762428
- [3]O'Grady, N P; Alexander, M; Burns, L A Guidelines for the prevention of intravascular catheter-related infections. American journal of infection control, 2011.PMID 21511081
- [4]Miller, M R; Griswold, M; Harris, J M 2nd Decreasing PICU catheter-associated bloodstream infections: NACHRI's quality transformation efforts. Pediatrics, 2010.PMID 20064860
- [5]Bizzarro, M J; Sabo, B; Noonan, M A quality improvement initiative to reduce central line-associated bloodstream infections in a neonatal intensive care unit. Infection control and hospital epidemiology, 2010.PMID 20102278
- [6]Milstone, A M; Elward, A; Song, X Daily chlorhexidine bathing to reduce bacteraemia in critically ill children: a multicentre, cluster-randomised, crossover trial. Lancet (London, England), 2013.PMID 23363666
- [7]Klompas, M; Branson, R; Eichenwald, E C Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infection control and hospital epidemiology, 2014.PMID 25376073
- [8]Patel, P K; Advani, S D; Kofman, A D Strategies to prevent catheter-associated urinary tract infections in acute-care hospitals: 2022 Update. Infection control and hospital epidemiology, 2023.PMID 37620117
- [9]McDonald, L C; Gerding, D N; Johnson, S Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 2018.PMID 29562266
- [10]Schutze, G E; Willoughby, R E; Committee on Infectious Diseases Clostridium difficile infection in infants and children. Pediatrics, 2013.PMID 23277317
- [11]Saiman, L; Coffin, S E; Kociolek, L K Healthcare-Associated Respiratory Syncytial Virus in Children's Hospitals. Journal of the pediatric infectious diseases society, 2023.PMID 37144945
- [12]Yokoe, D S; Anderson, D J; Berenholtz, S M A compendium of strategies to prevent healthcare-associated infections in acute care hospitals: 2014 updates. Infection control and hospital epidemiology, 2014.PMID 25026611