Paeds · infectious-diseases
Epstein-Barr virus and cytomegalovirus infection
Also known as Infectious mononucleosis · Glandular fever · Epstein-Barr virus infection · Cytomegalovirus infection · Congenital cytomegalovirus · Heterophile-negative mononucleosis
Fellowship topic on Epstein-Barr virus (EBV) and cytomegalovirus (CMV) infection in children: EBV as a gamma-herpesvirus transmitted by saliva that infects B cells via the CD21 receptor, whose CD8 T-cell response produces the atypical lymphocytes and the symptoms of infectious mononucleosis; CMV as a beta-herpesvirus and the most common congenital infection, causing direct cytopathic injury and sensorineural hearing loss; the classic adolescent mononucleosis triad and the amoxicillin rash, and the symptomatic congenital CMV newborn with petechiae, jaundice and thrombocytopenia; the differential of heterophile-positive versus heterophile-negative mononucleosis and of the sick neonate; heterophile antibody, EBV-specific serology, CMV IgG/IgM and PCR, and the 21-day saliva/urine PCR window; stepwise management from supportive care and activity restriction for EBV through corticosteroids for airway obstruction, valganciclovir for symptomatic congenital CMV, and pre-emptive ganciclovir for CMV in the immunocompromised; the splenic-rupture and return-to-play rules, EBV-lymphoproliferation, the EBV-multiple-sclerosis association, and congenital CMV screening; and ANZ/UK/US/Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
EBV serology — the four markers and what each means
Overview & Definition
Picture a sixteen-year-old brought to the emergency department with a week of fever, a sore throat so severe she cannot swallow her own saliva, and a exhaustion so complete she has stopped going to school. Her tonsils meet in the midline, her neck is draped in lymph nodes, and the registrar reaches for amoxicillin — only to see a confluent maculopapular rash erupt across her trunk two days later. This is Epstein-Barr virus infectious mononucleosis, and recognising the pattern — and withholding the antibiotic — is the clinical act that defines the encounter. [1] [2]
Now picture a different child: a ten-day-old baby on the postnatal ward who is jaundiced, covered in petechiae, and has a head circumference below the third centile. This is congenital cytomegalovirus, the most common congenital infection in the developed world, and the baby who will lose his hearing before his second birthday if the diagnosis is missed. The saliva or urine PCR must be sent now, inside the 21-day window, because once that window closes the chance to prove the infection is congenital is gone. [10] [9]
Epstein-Barr virus and cytomegalovirus are both human herpesviruses, and both establish lifelong latency after primary infection — but their clinical burden falls on entirely different patients. EBV is the adolescent's glandular fever: a self-limiting lymphoproliferative illness whose symptoms are largely the host immune response. CMV is the newborn's congenital infection and the immunocompromised host's opportunistic threat: a virus whose direct cytopathic injury damages brain, ear, blood and gut. The clinician's job is to recognise which child sits in front of them, to use the right test in the right window, and to match treatment to the host — supportive for the well adolescent, antiviral for the symptomatic newborn and the transplant recipient. [1] [8]
Classification
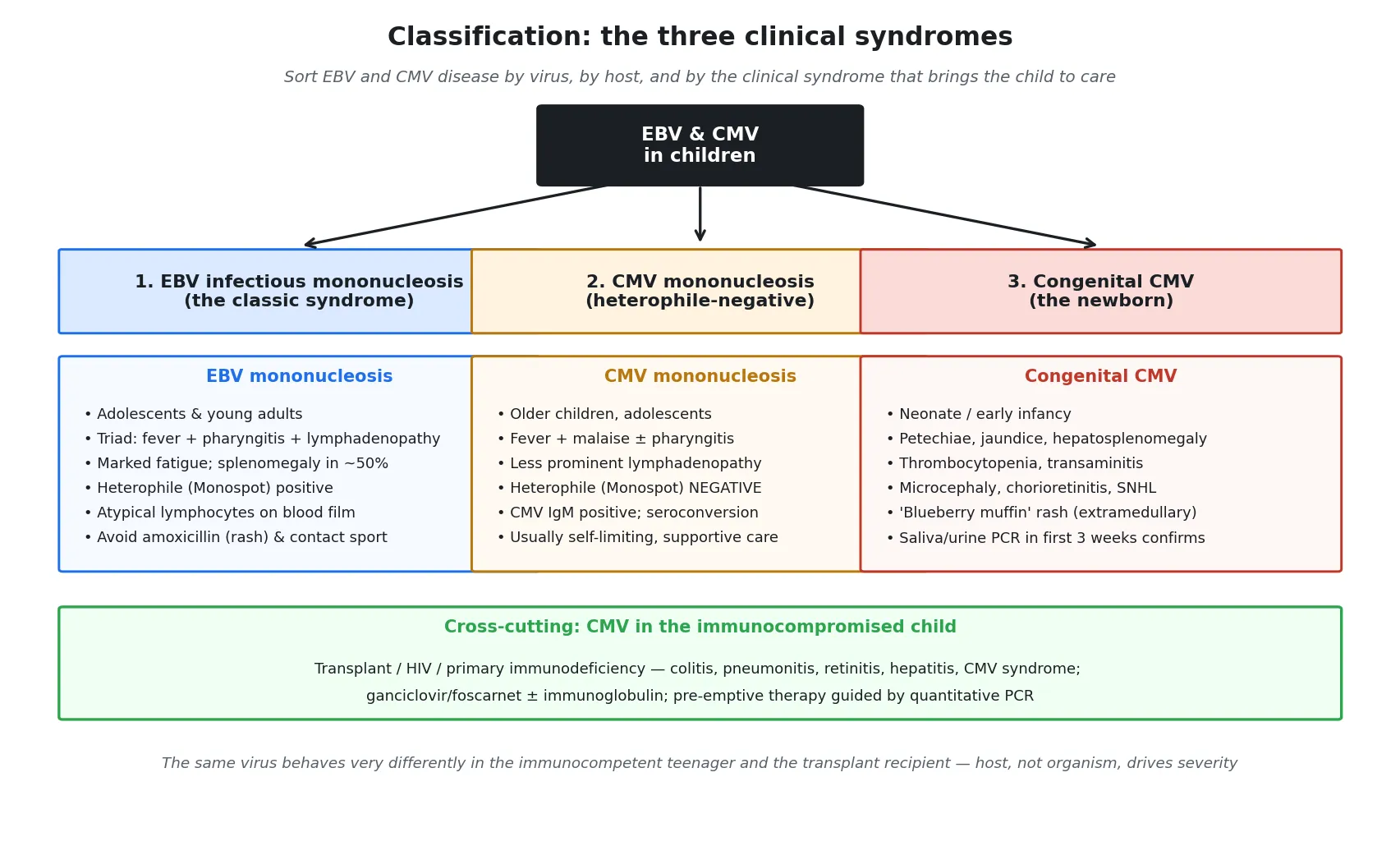
Sort EBV and CMV disease the way it arrives at the bedside — by the syndrome that brings the child to care — because the same virus behaves very differently in different hosts. The first syndrome is EBV infectious mononucleosis, the classic fever-sore-throat-fatigue illness of the adolescent and young adult. The second is CMV mononucleosis, a heterophile-negative illness of older children and adolescents that mimics EBV mononucleosis but is milder and lacks the prominent lymphadenopathy. The third, and the one with the greatest lifelong consequence, is congenital CMV — the multi-system disease of the newborn that is the leading non-genetic cause of sensorineural hearing loss. [1] [2]
The fourth syndrome cuts across all of this and is the one that most threatens life: CMV end-organ disease in the immunocompromised host. In the solid-organ or stem-cell transplant recipient, in the child with HIV, and in the child with a primary T-cell immunodeficiency, CMV reactivates from latency or arrives as a new donor-derived infection and invades tissue — colitis, pneumonitis, retinitis, hepatitis, encephalitis. This is the host for whom quantitative CMV PCR monitoring and pre-emptive antiviral therapy define care, and it is the host an examiner probes when asking "how does CMV disease differ by immune status?". [9] [4]
A useful fifth distinction for EBV is the rare but devastating lymphoproliferative spectrum. When T-cell surveillance of EBV fails — in transplant immunosuppression, in X-linked lymphoproliferative disease, or in other primary immunodeficiencies — the virus escapes immune control and drives uncontrolled B-cell proliferation: post-transplant lymphoproliferative disorder, fulminant EBV-haemophagocytic lymphohistiocytosis, and EBV-associated malignancies. This is EBV behaving not as a self-limiting glandular fever but as an oncogenic and immunopathological threat, and it is the bridge between the common and the life-threatening ends of the EBV spectrum. [4] [1]
Epidemiology & Risk Factors
EBV infects most of the world's population, but the age at which a child first meets the virus decides whether they notice. In low- and middle-income settings most children acquire EBV in early childhood, where primary infection is mild, nonspecific, and easily mistaken for an ordinary viral illness. In high-income settings the infection is often delayed into adolescence, and it is delayed primary infection in a half-immune adolescent that produces symptomatic infectious mononucleosis — roughly half of adolescents who seroconvert will develop the classic illness. The epidemiology teaches the clinical point: the same virus is silent in a toddler and dramatic in a teenager. [1] [2]
Congenital CMV is the most common congenital infection in developed countries, with a birth prevalence of roughly 0.5 to 1 percent — far higher than any of the other classic congenital infections. The Kenneson and Cannon meta-analysis established this burden, and it is the foundation for the public-health case for screening. The sequelae are concentrated in, but not confined to, the symptomatic newborn: sensorineural hearing loss is the most common and the most consequential, and a meaningful proportion of hearing loss is late-onset or progressive in children who were asymptomatic at birth. [12] [10]
The risk factors for severe EBV are the states in which T-cell control of the virus fails. X-linked lymphoproliferative disease (Duncan syndrome) is the prototypic inherited vulnerability: a boy with a mutation in the SH2D1A gene mounts a dysregulated, often fatal response to primary EBV. Post-transplant immunosuppression — especially with calcineurin inhibitors and T-cell depleting agents — sets the stage for EBV-driven lymphoproliferation. And a primary T-cell immunodeficiency of any cause removes the very cell population that holds EBV in check. [4] [1]
For congenital CMV, the dominant risk factor is primary maternal infection in pregnancy, which carries the highest transmission rate (around 30 to 40 percent) and the most severe fetal outcomes. Non-primary infection — reactivation of latent virus, or reinfection with a new strain — transmits less often but still contributes a large share of congenital CMV cases because most women of childbearing age are already seropositive. The implication for counselling is that a seropositive woman is not wholly protected, and a seronegative pregnant woman in contact with young children's saliva and urine is the highest-risk host. [9] [12]
Pathophysiology
Why does a virus that infects B cells produce a sore throat, a huge spleen, and a rash when you give the wrong antibiotic? The answer lies in EBV's choice of host cell and the immune response that choice provokes. EBV enters through the oropharynx, infects the epithelium of the nasopharynx, and then crosses to B lymphocytes by binding the CD21 complement receptor (also called CR2). Once inside a B cell, the virus drives polyclonal B-cell activation and proliferation — in the laboratory EBV can immortalise B cells indefinitely — and seeds a latent reservoir in memory B cells that persists for life. [1] [4]
The symptoms of infectious mononucleosis are not, for the most part, the virus damaging tissue. They are the CD8 cytotoxic T-cell response to the army of infected B cells. The atypical lymphocytes that characterise the blood film are reactive T cells, not infected B cells, and the fever, fatigue and lymphadenopathy reflect this massive T-cell activation and the cytokines it releases. This single fact — that the illness is the immune response — explains why EBV mononucleosis resolves as T-cell control is established, and why the same virus becomes lethal when T-cell control is absent. [4] [3]
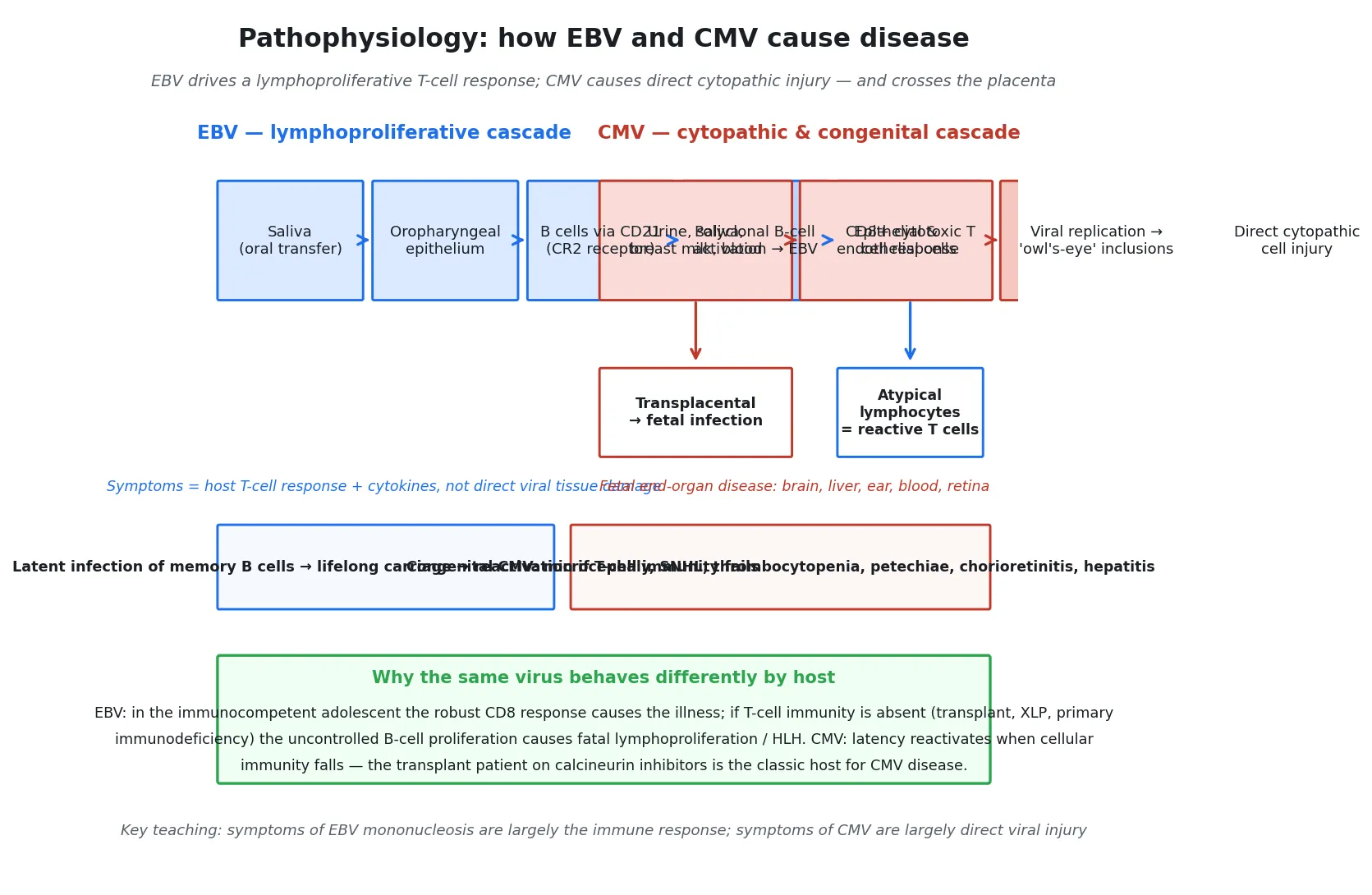
CMV works by a different mechanism. It infects epithelial, endothelial and mononuclear cells, replicates in the nucleus, and produces the characteristic owl's-eye intranuclear inclusions that pathologists recognise on cytology and histology. These inclusions are swollen, virus-laden cells, and their presence is direct evidence of the cytopathic injury that defines CMV disease. Where EBV disease is largely immunopathology, CMV disease is largely direct viral damage — colitis when the gut mucosa is destroyed, retinitis when the retina is invaded, pneumonitis when the lung is injured. [9] [4]
Congenital CMV arises when maternal viraemia spreads the virus across the placenta and into the fetus. The highest transmission and the most severe disease follow primary maternal infection, and the virus then attacks the developing organs with the greatest cellular turnover — the brain, the liver, the blood-forming tissue and the inner ear. The result is the multi-system congenital syndrome: microcephaly and intracranial calcifications from brain injury, petechiae and thrombocytopenia from marrow suppression, hepatitis and jaundice from liver injury, chorioretinitis from retinal infection, and the progressive sensorineural hearing loss that is the signature long-term consequence. The biology is direct cytopathic injury applied to a developing organism. [10] [9]
The unifying principle is that host cellular immunity governs outcome for both viruses. The immunocompetent adolescent contains EBV with a T-cell response and recovers; the transplant recipient or the boy with XLP loses that control and faces lymphoproliferation or HLH. Likewise, CMV stays latent in the healthy child but reactivates to cause end-organ disease when cellular immunity falls. Knowing which host sits in front of you — immunocompetent adolescent, newborn, or immunocompromised recipient — is the single most important judgement in EBV and CMV medicine. [4] [9]
Clinical Presentation
The classic EBV presentation is the adolescent with the mononucleosis triad. Fever, often lasting one to two weeks, is joined by an exudative pharyngitis that can rival group A streptococcal infection, and by lymphadenopathy that is most striking in the posterior cervical chain. Fatigue is often the most disabling symptom and can outlast the fever by weeks. Splenomegaly is detectable in roughly half of patients, and a palatal petechial rash and periorbital oedema are recognised but less common features. The child looks unwell and tired but is rarely systemically toxic between febrile episodes. [2] [3]
The amoxicillin rash is a presentation in its own right and a high-yield examination point. When a child with EBV mononucleosis is given ampicillin or amoxicillin — often because the sore throat was mistaken for streptococcal pharyngitis — a maculopapular rash erupts in nearly all of them within days. This is not a true penicillin allergy; it is an EBV-driven immune phenomenon, and it resolves when the antibiotic is stopped. The clinical lesson is double: withhold the antibiotic in the first place, and recognise the rash as a diagnostic clue rather than a reason to label the child penicillin-allergic for life. [6] [2]
The symptomatic congenital CMV newborn is the presentation that must never be missed. The baby may have petechiae (the "blueberry muffin" purpura of extramedullary haematopoiesis), jaundice with direct hyperbilirubinaemia, hepatosplenomegaly, thrombocytopenia, microcephaly with intracranial calcifications, chorioretinitis, and intrauterine growth restriction. Many of these findings overlap with neonatal sepsis and haemolytic disease, which is why congenital CMV sits firmly in the differential of the sick or jaundiced newborn. Critically, many newborns are asymptomatic at birth yet still develop late-onset or progressive sensorineural hearing loss — so the absence of signs does not exclude congenital CMV or its sequelae. [10] [9]
CMV mononucleosis in the older child mimics EBV mononucleosis but is a milder, heterophile-negative illness. The fever and malaise are present, the liver enzymes may be abnormal, but the pharyngitis and lymphadenopathy are less prominent than in EBV. The clue is the Monospot that comes back negative in a child who still looks as though they have glandular fever — that is the moment to send CMV serology. The illness is self-limiting, and the role of the clinician is to make the diagnosis, avoid unnecessary investigation, and reassure. [2] [3]
The complications are part of the presentation because they bring the child back to care. In EBV these include impending airway obstruction from massive tonsillar hypertrophy (the registrar's airway emergency), splenic rupture (the surgical emergency), autoimmune haemolytic anaemia, thrombocytopenia, hepatitis, and rare neurological complications such as encephalitis, Guillain-Barre syndrome and facial nerve palsy. In congenital CMV the complications are the long-term sequelae — hearing loss, cerebral palsy, cognitive impairment, seizures and visual impairment — that define the child's future. Recognising these early changes the disposition and the counselling. [1] [10]
Differential Diagnosis
For the adolescent with fever, sore throat and lymphadenopathy, the differential centres on the mimics of mononucleosis. Group A streptococcal pharyngitis is the most common alternative and the reason amoxicillin is so often given in error — but streptococcal pharyngitis lacks the marked fatigue, the splenomegaly and the atypical lymphocytosis. CMV mononucleosis is the closest mimic and is heterophile-negative. Acute toxoplasmosis produces a mononucleosis-like illness with prominent lymphadenopathy but little pharyngitis. Primary HIV infection (seroconversion illness) is the cannot-miss mimic and warrants an HIV test when the risk history is present. Adenovirus, influenza and, in the right context, lymphoma round out the list. [2] [3]
For the symptomatic neonate, the differential is the classic congenital-infection and neonatal-sepsis framework. Congenital CMV is the most common and must head the list. Toxoplasmosis produces similar findings with intracranial calcifications that are typically scattered rather than periventricular. Rubella (now rare in vaccinated populations) adds cataracts and cardiac defects. Congenital syphilis produces a desquamating rash, hepatosplenomegaly and bony changes. Neonatal bacterial sepsis and haemolytic disease of the newborn can present with jaundice, thrombocytopenia and hepatosplenomegaly and must be excluded. The practical approach is to send the congenital-infection screen alongside the septic workup, and to obtain the saliva or urine CMV PCR within the 21-day window. [9] [10]
For the immunocompromised child with a rising CMV PCR and fever, the differential includes CMV syndrome or end-organ disease versus other opportunistic infection, graft-versus-host disease or transplant rejection, and post-transplant lymphoproliferative disorder. The key step is tissue diagnosis to define end-organ disease — a colon biopsy for colitis, a bronchoalveolar lavage for pneumonitis — because a positive blood PCR alone establishes viraemia, not tissue-invasive disease. Distinguishing CMV disease from its mimics in this host is the job of the infectious diseases and transplant team working together. [9] [4]
Clinical & Bedside Assessment
The focused history for EBV builds around the throat and the fatigue. Ask about the duration of fever and sore throat, whether swallowing is impaired (a clue to impending airway obstruction), whether a rash appeared after any antibiotic, and whether there is left-upper-quadrant or shoulder-tip pain (a clue to splenic pathology). Quantify the fatigue and its functional impact — has the adolescent stopped attending school? — because this frames the activity counselling and the safety-netting. Ask about contact with other glandular-fever cases, recognising that the incubation period is long. [2] [7]
For the neonate with suspected congenital CMV, the history turns to the pregnancy and the newborn screen. Ask about maternal serology and any illness in pregnancy, the growth parameters, the feeding, the jaundice, any bruising or petechiae, and any abnormal movements or tone. Establish the newborn hearing-screen result, because a referred or failed screen is a red flag for congenital CMV. Document the day of life precisely, because it determines whether the confirmatory PCR is still within the 21-day window. [9] [10]
Examine the adolescent with EBV for the red flags that change disposition. Look for dysphagia, drooling, a muffled "hot-potato" voice or stridor — the signs of impending airway obstruction that demand urgent ENT and anaesthetic involvement. Palpate carefully for splenomegaly and elicit any abdominal or shoulder-tip tenderness that might signal splenic irritation or rupture. Look for pallor, bruising or mucosal bleeding that might point to autoimmune haemolytic anaemia or thrombocytopenia. A child who is maintaining their airway, feeding and mobilising can be managed as an outpatient; one who is not needs admission. [1] [7]
Examine the neonate for the stigmata of congenital CMV. Look for petechiae and the blueberry-muffin rash, assess for jaundice and hepatosplenomegaly, measure the head circumference against the growth chart, examine the eyes for chorioretinitis, and assess the tone and neurology. Document the hearing-screen status explicitly. These findings not only support the diagnosis but define the baseline against which treatment response and long-term surveillance will be measured. [10] [9]
Document the public-health and follow-up essentials at the bedside. For EBV, record the activity and contact-sport restriction and the planned return-to-play date. For congenital CMV, record the audiology referral, the developmental-surveillance plan, the ophthalmology review, and the maternal counselling that will follow. A careful first encounter prevents the late, disorganised scramble when a hearing loss appears at two years of age and the congenital-CMV diagnosis was never secured. [9] [13]
Investigations
The heterophile antibody test (Monospot) is the rapid first-line test for EBV mononucleosis in older children and adolescents. It detects agglutinating antibodies that appear in the first or second week of illness and persist for several months. It is positive in roughly 90 percent of adults with EBV mononucleosis, but it is insensitive in young children, who often do not produce heterophile antibodies at all. A positive Monospot in an adolescent with the right clinical picture confirms EBV; a negative one in a young child does not exclude it. [2] [3]
When the Monospot is negative but the suspicion of EBV remains — especially in a young child — EBV-specific serology defines the stage of infection. Viral capsid antigen (VCA) IgM marks acute primary infection. VCA IgG appears early and persists for life, so on its own it only confirms past exposure. EBV nuclear antigen (EBNA) IgG appears late (after several weeks) and also persists, so a VCA IgM positive with EBNA negative is the pattern of acute primary EBV. Early antigen (EA) suggests recent infection or reactivation. Reading these four markers together lets you stage the infection precisely — a skill an examiner rewards. [1] [2]
In Australia and Aotearoa New Zealand, the heterophile antibody test remains the practical first-line screen for adolescent mononucleosis, with EBV-specific serology reserved for negative or equivocal results and for young children. CMV diagnosis in the older child relies on CMV IgM and IgG serology with paired titres or CMV PCR; congenital CMV is confirmed by saliva or urine PCR within the first 21 days of life, in line with the international consensus. Quantitative CMV PCR is the standard for monitoring the transplant recipient. [9] [2]
For CMV, the diagnostic approach depends on the host. In the older child with heterophile-negative mononucleosis, CMV IgM with seroconversion on paired IgG titres makes the diagnosis. In the transplant or immunocompromised host, quantitative CMV PCR is the cornerstone — it detects viraemia, guides pre-emptive therapy, and monitors response. Critically, in suspected congenital CMV, the diagnosis is confirmed by saliva or urine PCR within the first 21 days of life. The Boppana saliva-PCR study established saliva as a sensitive screening sample; after 21 days, a positive result cannot distinguish congenital from perinatally acquired infection, because the baby may have acquired CMV from breast milk or the birth canal. This window is the single most testable fact in congenital CMV. [11] [9]
Basic supportive tests round out the workup. In EBV the full blood count frequently shows atypical lymphocytes (reactive T cells, often 10 to 20 percent or more) and a mild lymphocytosis; liver enzymes are often mildly raised. In congenital CMV the count may show thrombocytopenia, anaemia and neutropenia, with raised direct bilirubin and transaminases. A cranial ultrasound, ophthalmology review and a baseline audiology assessment complete the congenital CMV workup, defining the extent of disease at the outset. [10] [3]
Management — Resuscitation
Resuscitation for EBV is about the airway and the spleen. The adolescent who develops drooling, dysphagia, a muffled voice or stridor has impending airway obstruction from massive tonsillar hypertrophy, and this is an ENT and anaesthetic emergency. Secure the airway — humidified oxygen, nebulised adrenaline, and early senior involvement — and give a short course of corticosteroids to reduce the tonsillar swelling. A child who cannot protect their own airway needs the operating theatre, not the outpatient clinic. [1] [3]
Splenic rupture is the other EBV emergency. An adolescent with mononucleosis who develops abdominal or shoulder-tip pain, with hypotension and a falling haemoglobin, has a torn spleen until proven otherwise. Resuscitate with intravenous fluids, cross-match, image with ultrasound or computed tomography, and involve the surgical team. Most splenic ruptures in mononucleosis can be managed non-operatively with monitoring and transfusion, but the diagnosis must be made fast, and a sudden collapse in a child with known splenomegaly is this diagnosis until excluded. [7] [2]
For the symptomatic congenital CMV newborn, resuscitation means stabilising the multi-system disease while confirming the diagnosis within the 21-day window. Address thrombocytopenia and its bleeding risk, manage the jaundice and any hepatic dysfunction, support feeding and thermoregulation, and obtain the saliva or urine PCR promptly. The decision to start valganciclovir is made once the diagnosis is confirmed or strongly suspected and the disease is symptomatic — and the earlier antiviral therapy begins, the better the long-term hearing outcome. [8] [13]
For CMV end-organ disease in the immunocompromised host, resuscitation means confirming tissue-invasive disease and reducing immunosuppression while starting antiviral therapy. A child with CMV colitis may be bleeding or perforated; CMV pneumonitis may cause respiratory failure; CMV retinitis threatens sight. Stabilise the failing organ, obtain tissue for diagnosis, measure the quantitative PCR, and begin ganciclovir induction — coordinated with the transplant or immunology team, because reducing immunosuppression must be balanced against the risk of graft rejection. [9] [4]
Provide supportive care throughout. For EBV this is hydration, analgesia and antipyretics. For the neonate it is fluid, glucose and temperature management with careful monitoring. For any child starting ganciclovir or valganciclovir it is neutrophil and renal monitoring, because both drugs are myelosuppressive and nephrotoxic, and dose adjustment or a switch to foscarnet may be needed if toxicity emerges. [8] [9]
Management — Definitive & Stepwise
Definitive management of EBV mononucleosis is supportive, and the most important prescription is often what you withhold. Rest, hydration, analgesia and antipyretics treat the symptoms; no antibiotic is indicated because EBV is a virus, and giving amoxicillin only triggers the rash. No antiviral is routine for uncomplicated mononucleosis — aciclovir has activity against EBV in vitro but has not been shown to change the clinical course, and it is not standard care. Corticosteroids are reserved for specific indications: impending airway obstruction, massive tonsillar hypertrophy, severe autoimmune haemolytic anaemia, or aplastic anaemia. Routine steroids for uncomplicated disease are not justified. [1] [3]
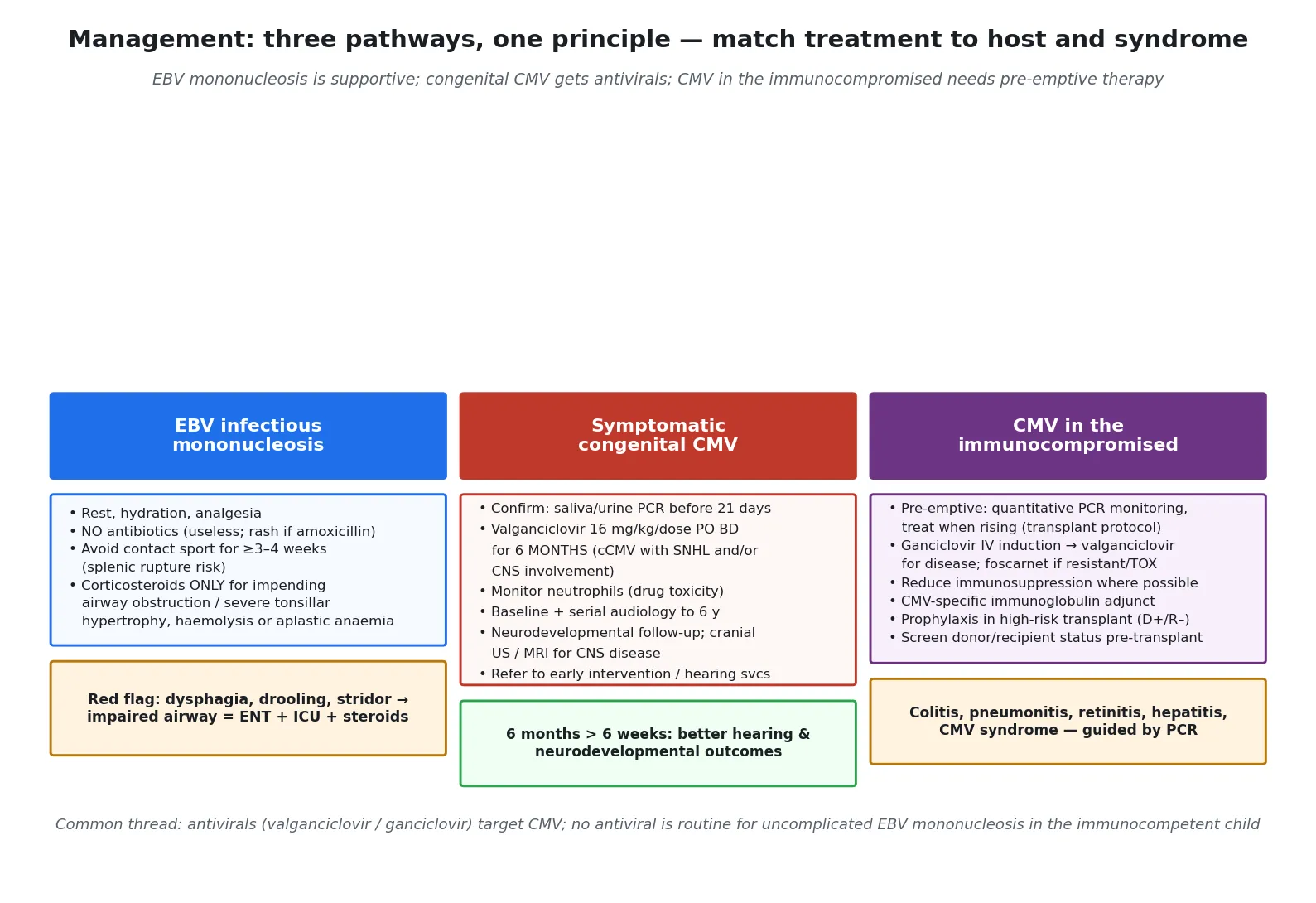
The splenic-rupture and return-to-play rule is a defining part of EBV management. Because the spleen is enlarged and softened, it is vulnerable to rupture from even minor trauma, and spontaneous rupture can occur. The American Medical Society for Sports Medicine position statement advises avoiding contact sport and heavy lifting for at least three to four weeks from the onset of symptoms, and longer if splenomegaly persists, with a graded return to activity once the child is asymptomatic and the spleen has returned to normal size. A premature return to the rugby field is the preventable disaster in EBV mononucleosis. [7] [2]
The stepwise EBV mononucleosis pathway
Confirm the diagnosis: Monospot in the adolescent, EBV-specific serology (VCA IgM, EBNA) if negative or in a young child.
Supportive care: rest, hydration, analgesia, antipyretics; reassure that fatigue may last weeks to months.
Withhold antibiotics — amoxicillin triggers the rash and treats no infection; manage any confirmed bacterial co-infection with a non-penicillin where possible.
Restrict activity: no contact sport or heavy lifting for at least three to four weeks, and longer if splenomegaly persists; then graded return to play.
Reserve corticosteroids for impending airway obstruction, massive tonsillar hypertrophy, severe autoimmune haemolytic anaemia or aplastic anaemia.
Safety-net: return immediately for dysphagia or drooling, abdominal or shoulder-tip pain, pallor, bruising, or breathing difficulty.
For symptomatic congenital CMV, the definitive treatment is valganciclovir at 16 mg/kg/dose orally twice daily for six months. The Kimberlin valganciclovir trial established that antiviral therapy improves audiologic outcomes in symptomatic congenital CMV, and the extension of that work showed that a six-month course improves hearing and neurodevelopmental outcomes beyond a six-week course. Treatment is indicated for congenital CMV with sensorineural hearing loss and/or central nervous system involvement (microcephaly, intracranial calcifications, chorioretinitis, cerebrospinal fluid pleocytosis). Neutrophil counts must be monitored because of the drug's myelosuppression, and audiology and developmental follow-up continue into school age to detect late-onset or progressive hearing loss. [8] [13]
For CMV end-organ disease in the immunocompromised host, management is pre-emptive therapy guided by quantitative PCR. The transplant protocol monitors CMV PCR at intervals; a rising titre triggers treatment before end-organ disease develops. Established disease is treated with intravenous ganciclovir induction followed by oral valganciclovir, with foscarnet reserved for resistance or for toxicity that precludes ganciclovir. Reduce immunosuppression where the graft allows, use CMV-specific immunoglobulin as an adjunct for severe disease, and match prophylaxis to risk — the highest-risk transplant recipient is the donor-positive, recipient-negative mismatch, who receives targeted prophylaxis. [9] [4]
Layer on surveillance and prevention. For congenital CMV this is audiology and developmental follow-up into school age, because hearing loss can emerge or progress years after the neonatal period. For the transplant recipient it is lifelong PCR-guided monitoring. For the pregnant woman it is hygiene counselling — no sharing of cutlery or food with young children, careful hand-washing after contact with toddler saliva and urine, and no kissing young children on the mouth — the measures that reduce CMV acquisition in the seronegative mother. [9] [10]
Specific Subtypes & Scenarios
An adolescent with classic EBV mononucleosis and an amoxicillin rash. Reassure the family that the rash is an EBV-driven immune phenomenon, not a true penicillin allergy, and that it will resolve. Provide supportive care, withhold further antibiotics, restrict contact sport for at least three to four weeks, and safety-net for airway and splenic complications. This is the bread-and-butter EBV encounter and the one most likely to appear in a written or OSCE station. [2] [6]
A young child with primary EBV infection. In toddlers and preschool children, primary EBV is often mild, nonspecific and easily mistaken for an ordinary viral illness — and the Monospot is frequently negative because young children do not reliably produce heterophile antibodies. Confirm with EBV-specific serology (VCA IgM) if the diagnosis matters, and manage supportively. The contrast with the dramatic adolescent presentation is the teaching point. [1] [3]
A newborn with symptomatic congenital CMV. Confirm with saliva or urine PCR within the 21-day window, assess the full extent of disease with a cranial ultrasound, ophthalmology review and baseline audiology, and start valganciclovir 16 mg/kg/dose twice daily for six months for disease with hearing loss or CNS involvement. Arrange audiology and developmental follow-up into school age, and counsel the family on the prognosis and the long-term surveillance. [8] [13]
An immunocompromised child with a rising CMV PCR. Use pre-emptive therapy guided by the quantitative PCR trend, balancing the risk of progression to end-organ disease against the myelosuppressive and nephrotoxic cost of ganciclovir. Confirm tissue-invasive disease with biopsy when the clinical picture points to a specific organ. Coordinate with the transplant or immunology team and reduce immunosuppression where the graft or the underlying condition allows. [9] [4]
A transplant recipient with EBV-driven lymphoproliferation. The first step is to reduce immunosuppression — this alone can induce regression of post-transplant lymphoproliferative disorder by restoring T-cell control of EBV. Monitor the EBV quantitative PCR, and involve haemato-oncology early; rituximab (anti-CD20) and, in more advanced disease, chemotherapy are the next steps. The principle is that EBV lymphoproliferation is primarily a disorder of immune dysregulation, and restoring immunity is itself treatment. [4] [1]
A pregnant contact of a child with CMV. Counsel on serostatus and hygiene measures, and investigate suspected primary infection with serology and PCR. Primary maternal infection carries the highest fetal risk; non-primary infection transmits less often but still contributes. Hyperimmune globulin and antivirals in pregnancy remain areas of active evidence, and the pregnant seronegative woman in close contact with young children's secretions is the host for whom prevention through hygiene matters most. [9] [12]
Complications & Pitfalls
The EBV complications cluster around the airway, the spleen and the blood. Airway obstruction from massive tonsillar hypertrophy is the life-threatening early complication and the indication for corticosteroids. Splenic rupture is rare but potentially fatal and is the reason for the contact-sport restriction. Autoimmune haemolytic anaemia (often with cold agglutinins) and thrombocytopenia are recognised haematological complications, and rare but serious neurological complications include encephalitis, Guillain-Barre syndrome, facial nerve palsy and transverse myelitis. A child who deteriorates neurologically during EBV mononucleosis needs urgent assessment. [1] [2]
The congenital CMV sequelae are the long-term consequences that define the child's future. Sensorineural hearing loss is the most common, is often late-onset or progressive, and is the reason audiology surveillance must continue into school age. Cognitive and motor impairment, cerebral palsy, seizures, chorioretinitis and visual impairment add to the burden in the severely affected child. The Jones review of current thinking frames these as the outcomes that antiviral treatment and surveillance aim to modify. [10] [13]
The central diagnostic pitfall in congenital CMV is missing the 21-day window. A saliva or urine PCR obtained at four weeks of age that comes back positive cannot distinguish congenital from perinatally acquired CMV, because by then the baby may have acquired the virus from breast milk or the birth canal. If a clinician suspects congenital CMV at any point in the neonatal period, the PCR must be sent before 21 days of life — and if the baby is already past that window, stored newborn screening blood spots (Guthrie cards) can sometimes be retrieved for retrospective CMV PCR to establish congenital infection. This is the single most testable pitfall in the topic. [11] [9]
The second pitfall is treating EBV mononucleosis with amoxicillin. The maculopapular rash that follows is not a penicillin allergy, but it is a clear sign that the antibiotic was the wrong choice — the sore throat of mononucleosis is viral. The third pitfall is routine corticosteroids for EBV — steroids are reserved for airway obstruction, severe haemolysis or aplastic anaemia, and routine use carries harm without benefit. The fourth is over-treating CMV in the transplant host: ganciclovir and foscarnet carry significant myelosuppression and nephrotoxicity, so pre-emptive PCR-guided therapy avoids unnecessary toxicity. [6] [9]
The fifth pitfall is discharging a congenital CMV child without audiology surveillance. Because hearing loss can emerge years after the neonatal period, a single normal newborn hearing screen does not close the case. Long-term audiology follow-up into school age is part of the treatment, not an optional extra. [10] [13]
Prognosis & Disposition
EBV infectious mononucleosis in the immunocompetent adolescent is self-limiting. The fever and sore throat resolve over one to two weeks, but the fatigue often persists for weeks to months, and a full return to energy and to sport can take longer still. Most adolescents recover completely without sequelae, and the role of the clinician is supportive care, activity counselling and safety-netting. The disposition is outpatient for the stable adolescent, admission for airway compromise, splenic rupture, significant haemolysis or dehydration, and a graded return to activity guided by splenic recovery. [2] [7]
Symptomatic congenital CMV carries substantial long-term morbidity. Roughly half of symptomatic neonates develop sensorineural hearing loss or neurodevelopmental impairment, and even asymptomatic newborns can develop late-onset hearing loss. This is why the disposition for congenital CMV is inpatient initiation of valganciclovir with monitoring, followed by six months of outpatient therapy with audiology, ophthalmology and developmental surveillance extending into school age. The prognosis is not made at discharge — it unfolds over years, and the surveillance must match that timescale. [10] [13]
For CMV end-organ disease in the immunocompromised host, the prognosis depends on the speed of diagnosis, the reduction of immunosuppression, and the response to antiviral therapy. CMV colitis, pneumonitis and retinitis are life- and sight-threatening, and early pre-emptive therapy guided by quantitative PCR prevents progression. The disposition is inpatient management for end-organ disease, coordinated with the transplant or immunology team, with outpatient PCR monitoring thereafter. [9] [4]
At discharge from any EBV or CMV encounter, complete the safety-netting and the follow-up plan. For EBV, document the return-to-play date and the warning signs for airway and splenic complications. For congenital CMV, confirm the audiology, developmental and ophthalmology referrals and the valganciclovir monitoring plan. For the immunocompromised host, confirm the PCR-monitoring schedule and the reduction-of-immunosuppression plan. The discharge encounter is also the prevention opportunity — the hygiene counselling for the pregnant contact, the family screening for XLP, and the audiology referral that catches the late-onset hearing loss. [1] [9]
Special Populations
Adolescents and young adults are the classic symptomatic EBV mononucleosis group. Counsel on the prolonged recovery, the activity and contact-sport restriction, the amoxicillin-rash interaction, and the warning signs for airway and splenic complications. A respectful, developmentally appropriate conversation about glandular fever — what to expect, what to avoid, when to return — is a communication skill an examiner rewards. [2] [7]
Neonates and infants are the congenital CMV group. The 21-day diagnostic window, the valganciclovir decision for symptomatic disease, and the long-term audiology and developmental surveillance define care. Perinatally acquired CMV from breast milk is usually benign in the term infant, but in the very preterm or extremely-low-birthweight baby it can cause symptomatic infection, and the decision to use frozen or donor milk involves weighing the benefits of breast milk against the small CMV risk. [10] [9]
Transplant recipients and the immunocompromised are the pre-emptive-therapy group. Match the donor and recipient CMV status before transplant to avoid the highest-risk donor-positive, recipient-negative mismatch, monitor the quantitative PCR, and treat pre-emptively. For EBV in this group, monitor the EBV PCR for lymphoproliferation and reduce immunosuppression at the first sign of rising titres. The transplant and immunology teams own the long-term plan, but the general paediatrician must recognise the patterns. [9] [4]
Children with primary immunodeficiency and X-linked lymphoproliferative disease face the fulminant end of the EBV spectrum. A boy with XLP who meets EBV can develop fatal EBV-haemophagocytic lymphohistiocytosis, and the presentation — fever, hepatosplenomegaly, pancytopenia, hyperferritinaemia — demands urgent haematology and immunology involvement. Haematopoietic stem-cell transplant is curative for XLP, and family screening and genetic counselling apply. The general paediatrician's role is to recognise the dysregulated EBV response and escalate. [4] [1]
Pregnant women need CMV-aware counselling. The preventive measures for the seronegative pregnant woman in contact with young children are simple and powerful: no sharing of utensils, food or drinks with toddlers, careful hand-washing after contact with saliva and urine (especially after nappy changes), and no kissing young children on the mouth. Investigate suspected primary infection with serology and PCR, and recognise that primary maternal infection carries the highest fetal risk. A maternal CMV vaccine remains in development and is not yet available. [9] [12]
Indigenous, migrant, refugee and socioeconomically disadvantaged children need equitable access to the services that change congenital CMV outcomes — audiology, developmental services and antiviral treatment. Use trained interpreters rather than family members, and recognise that disadvantage should never be the reason a hearing loss is detected late or a valganciclovir course is not completed. [10] [13]
Evidence, Guidelines & Regional Differences
The valganciclovir evidence transformed congenital CMV management. The Kimberlin randomised trial showed that valganciclovir improves audiologic outcomes in symptomatic congenital CMV at six weeks of therapy, and the extension of that work established that a six-month course improves hearing and neurodevelopmental outcomes beyond a six-week course — shifting the standard of care from six weeks to six months for symptomatic disease. This is the evidence that anchors valganciclovir as the treatment of symptomatic congenital CMV. [8] [13]
Valganciclovir for symptomatic congenital CMV
Population: Neonates with symptomatic congenital cytomegalovirus disease with and without central nervous system involvement, randomised to valganciclovir versus placebo for six weeks.
Key finding
Valganciclovir improved audiologic outcomes at six months; the extension study showed that a six-month course improved hearing and neurodevelopmental outcomes beyond a six-week course.
Practice change
Treat symptomatic congenital CMV (with sensorineural hearing loss and/or CNS involvement) with valganciclovir 16 mg/kg/dose twice daily for six months, with neutrophil monitoring and long-term audiology follow-up.
The international consensus on congenital CMV (Rawlinson et al.) set out prevention, diagnosis and therapy recommendations and is the reference against which national guidance is compared. The Boppana saliva-PCR study established saliva as a sensitive screening sample for newborn CMV, providing the methodological basis for universal screening programmes now being piloted. The Kenneson and Cannon meta-analysis defined the birth prevalence and sequelae burden that justify the public-health investment, and the Fowler and Boppana review set out the natural history, including the critical fact that hearing loss is often late-onset or progressive. [9] [11]
For EBV, the Cohen NEJM review remains the definitive account of the virus's biology and latency, and the Ebell and Peter paediatric reviews anchor the clinical approach to infectious mononucleosis. The Bjornevik cohort study in Science established EBV as a near-necessary cause of multiple sclerosis — a finding that reframed EBV as not merely a cause of glandular fever but as the precursor event in a major neurological disease, and a current target for vaccine development. The Putukian position statement codified the return-to-play rules that govern the contact-sport restriction. [1] [5] [7]
The regional guidance converges on the same principles with local detail. In ANZ, the heterophile antibody is the first-line adolescent EBV screen with EBV-specific serology in reserve, congenital CMV is confirmed by saliva or urine PCR within 21 days, and valganciclovir is the treatment for symptomatic disease, in line with the international consensus. In the UK, NICE and RCPCH-equivalent guidance direct congenital CMV diagnosis and management, and the National Hearing Screening programme intersects with CMV surveillance. In the US, the CDC and AAP set the standard, with universal CMV screening being adopted state by state. In Canada, the Canadian Paediatric Society guidance mirrors this approach. In every region the principle is the same: supportive care for EBV, valganciclovir for symptomatic congenital CMV, pre-emptive therapy for CMV in the immunocompromised, and long-term audiology surveillance for the congenital CMV child. [9] [10]
The controversies are active. Universal versus targeted congenital CMV screening is being decided region by region. The role of a maternal CMV vaccine — now in clinical development — would transform prevention if proven effective. Antiviral treatment of asymptomatic congenital CMV remains debated, balancing the small benefit against six months of drug exposure. Corticosteroid use in EBV mononucleosis, beyond the clear airway-obstruction indication, is another area of honest uncertainty. The defence against each is the same: use the right test in the right window, match treatment to the host, and keep the long-term surveillance that catches the late-onset hearing loss. [13] [9]
Exam Pearls
- EBV infects B cells via the CD21 (CR2) receptor; the atypical lymphocytes of mononucleosis are reactive CD8 T cells, not infected B cells. [1]
- The Monospot (heterophile antibody) is positive in roughly 90 percent of adults but is insensitive in young children, who need EBV-specific serology — VCA IgM positive with EBNA negative marks acute primary EBV. [1] [2]
- The amoxicillin rash appears in nearly all children with EBV mononucleosis given ampicillin or amoxicillin — a diagnostic clue, not a true penicillin allergy. [6]
- Congenital CMV is the most common congenital infection and the leading non-genetic cause of sensorineural hearing loss; the hearing loss is often late-onset or progressive, so audiology must continue into school age. [10] [12]
- The congenital CMV diagnostic window is 21 days: saliva or urine PCR must be sent within three weeks of life to confirm congenital infection. [11] [9]
- Symptomatic congenital CMV is treated with valganciclovir 16 mg/kg/dose twice daily for six months; six months beats six weeks for hearing and neurodevelopment. [8]
- Reserve corticosteroids in EBV for impending airway obstruction, severe autoimmune haemolytic anaemia or aplastic anaemia — not for routine use. [1]
- Avoid contact sport for at least three to four weeks after EBV mononucleosis because of splenic rupture; the AMSSM position statement guides return to play. [7]
- CMV in the immunocompromised is managed by pre-emptive therapy guided by quantitative PCR; ganciclovir is first-line, foscarnet for resistance or toxicity. [9]
- EBV is a near-necessary cause of multiple sclerosis (Bjornevik 2022) and drives post-transplant lymphoproliferative disorder and X-linked lymphoproliferative disease when T-cell surveillance fails. [5] [4]
References
- [1]Cohen JI Epstein-Barr virus infection. N Engl J Med, 2000.PMID 10944566
- [2]Ebell MH Epstein-Barr virus infectious mononucleosis. Am Fam Physician, 2004.PMID 15508538
- [3]Peter J; Ray CG Infectious mononucleosis. Pediatr Rev, 1998.PMID 9707718
- [4]Taylor GS; Long HM; Brooks JM; Rickinson AB; Hislop AD The immunology of Epstein-Barr virus-induced disease. Annu Rev Immunol, 2015.PMID 25706097
- [5]Bjornevik K; Cortese M; Healy BC; Kuhle J; et al Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science, 2022.PMID 35025605
- [6]Abreu A; Nunes S; Botelho C Eosinophilia in Amoxicillin-Induced Rash in Infectious Mononucleosis. Cureus, 2023.PMID 36756024
- [7]Putukian M; McGrew CA; Benjamin HJ; et al American Medical Society for Sports Medicine Position Statement: Mononucleosis and Athletic Participation. Clin J Sport Med, 2023.PMID 37186809
- [8]Kimberlin DW; Jester PM; Sánchez PJ; Ahmed A; et al Valganciclovir for symptomatic congenital cytomegalovirus disease. N Engl J Med, 2015.PMID 25738669
- [9]Rawlinson WD; Boppana SB; Fowler KB; Kimberlin DW; et al Congenital cytomegalovirus infection in pregnancy and the neonate: consensus recommendations for prevention, diagnosis, and therapy. Lancet Infect Dis, 2017.PMID 28291720
- [10]Fowler KB; Boppana SB Congenital cytomegalovirus infection. Semin Perinatol, 2018.PMID 29503048
- [11]Boppana SB; Ross SA; Shimamura M; Palmer AL; et al Saliva polymerase-chain-reaction assay for cytomegalovirus screening in newborns. N Engl J Med, 2011.PMID 21631323
- [12]Kenneson A; Cannon MJ Review and meta-analysis of the epidemiology of congenital cytomegalovirus (CMV) infection. Rev Med Virol, 2007.PMID 17579921
- [13]Jones CE; Bailey H; Bamford A; Galm F; et al Managing challenges in congenital CMV: current thinking. Arch Dis Child, 2023.PMID 36442957