Paeds · infectious-diseases
Fever in the returned traveller
Also known as Travel-related fever · Imported fever · Tropical fever in a returning child · Post-travel fever · Fever after overseas travel
Fellowship topic on the febrile child who has returned from overseas travel: the time-critical imperative to exclude falciparum malaria with a same-day blood film; the use of incubation window, fever pattern and geography to narrow the differential; the five must-not-miss causes (malaria, dengue, enteric fever, rickettsial disease, viral haemorrhagic fever) and the common non-tropical mimics; the GeoSentinel evidence base for disease probability by region; the pathophysiology of the two paradigm killers (cytoadherence in falciparum and capillary leak in dengue); the bedside assessment and risk-stratification of the unwell child; the investigations and their pitfalls (the single negative film); the stepwise immediate-diagnose-treat pathway with severity-driven antimalarial choice (IV artesunate for severe disease per AQUAMAT) and empiric antibiotics for the septic or typhoid-suspected child; regional differences in artemisinin-resistance and XDR typhoid; special populations (visiting-friends-and-relatives travellers, immunocompromised, migrant and Indigenous children); and the disposition and public-health responsibilities (notifiable diseases, isolation for VHF).
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
M.A.L.A.R.I.A. — the questions you must ask of every febrile returning child
Overview & Definition
Picture a seven-year-old brought to the emergency department with two days of high fever, headache and a flushed face, two weeks after visiting grandparents in Papua New Guinea. The waiting room is full, the fever is common, and the easy assumption is a viral illness. The single question that changes the outcome is the one no one has yet asked: where has this child been? Fever in the returned traveller is not a diagnosis; it is a frame that re-weights the ordinary differential of childhood fever toward a short list of tropical infections, a few of which can kill a child within hours of the first febrile seizure. [2]
The defining act is therefore not a test but a question — the travel history, asked of every febrile child, every time. GeoSentinel, the global surveillance network of travel and tropical-medicine clinics, has shown that fever is the single most common reason an ill returned traveller seeks care, and that the pattern of disease tracks tightly with the destination, the type of travel and the time since exposure. The clinician's job is to use that structure to find the dangerous few without holding the many in hospital for every conceivable pathogen. [1] [2]
What makes this a fellowship-level topic is that the dangerous infections share a nondescript early phase — fever, malaise, headache, myalgia — that is indistinguishable from influenza or a simple gastroenteritis. The discriminator is not the symptom but the context, read against an incubation window and a geography. The skill is in holding two truths at once: most post-travel fever is benign and self-limiting, and a small, knowable fraction is a time-critical emergency whose outcome depends on a question asked in the first minute. [3]
Classification
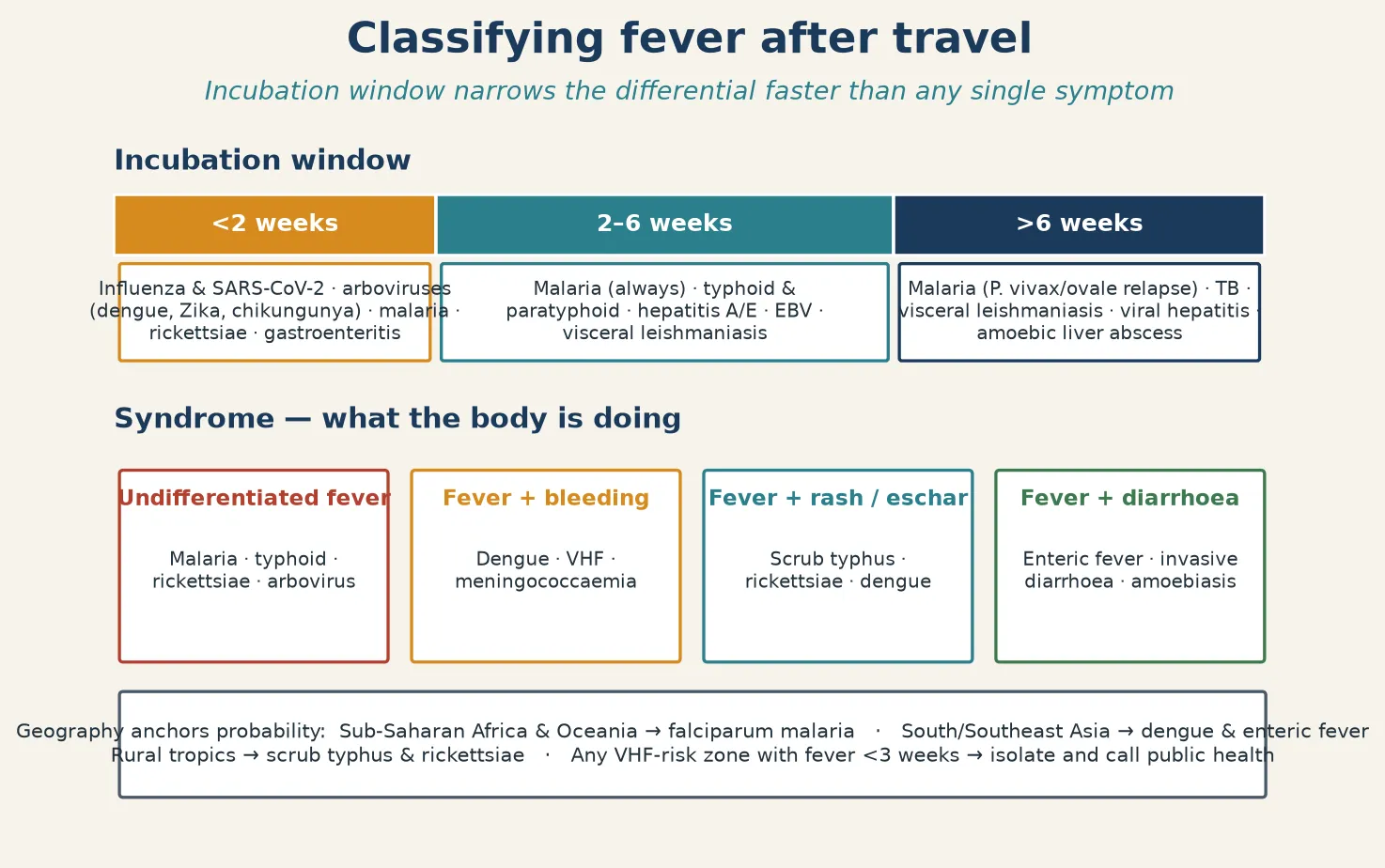
The most useful way to classify fever after travel is by the incubation window, because it immediately excludes large swathes of the differential. Fever beginning within two weeks of return points to the arboviruses (dengue, Zika, chikungunya), influenza and SARS-CoV-2, malaria, the rickettsiae and acute gastroenteritis. Fever presenting between two and six weeks widens the net to enteric fever, hepatitis A and E, Epstein–Barr virus and the early phase of visceral leishmaniasis — though malaria must still be considered at every interval. Fever beyond six weeks raises relapsing vivax or ovale malaria, tuberculosis, visceral leishmaniasis, chronic viral hepatitis and amoebic liver abscess. [2] [3]
The second axis is the clinical syndrome, because the body's response narrows the field faster than a pathogen list ever can. An undifferentiated fever — no localising feature — is the hallmark of malaria, typhoid, rickettsiae and the arboviruses. Fever with bleeding points to dengue, a viral haemorrhagic fever or meningococcaemia. Fever with a rash or an eschar raises scrub typhus and the spotted-fever rickettsiae. Fever with prominent diarrhoea suggests enteric fever, invasive bacterial diarrhoea or amoebiasis. A mononucleosis-like illness with fever and adenopathy brings Epstein–Barr virus, cytomegalovirus and acute retroviral syndrome into view. [2] [3]
The third axis is geography, which anchors the prior probability. Sub-Saharan Africa and the Oceania melanesian countries carry the highest falciparum malaria burden. South and Southeast Asia lead in dengue and enteric fever. Rural tropics across the Asia–Pacific tsutsugamushi triangle carry scrub typhus. Anywhere with a viral haemorrhagic fever outbreak and a child febrile within three weeks of return triggers a separate, isolation-driven pathway. Holding all three axes at once lets the clinician generate a working differential in the first minute of the consultation rather than after the bloods return. [1] [2]
The immediate-diagnose-treat pathway
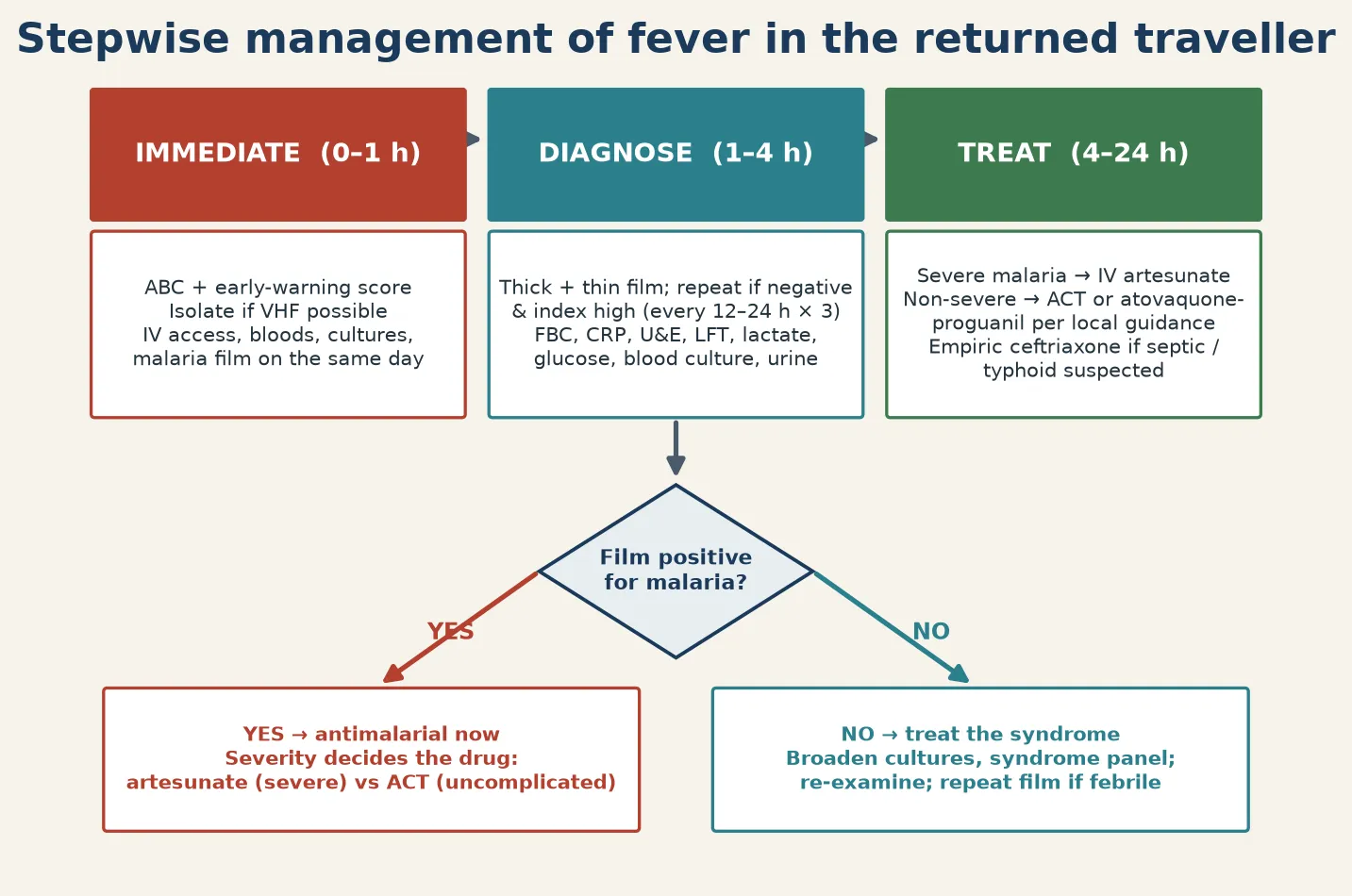
Immediate (0–1 h): structured ABC and early-warning score, isolate if VHF possible, IV access, first blood draw including the malaria film and cultures.
Diagnose (1–4 h): thick and thin film read same day — plan a repeat at 12–24 h if negative; add FBC, CRP, U&E, LFT, lactate, glucose, blood culture, urine, and syndrome-specific tests.
Treat (4–24 h): severity decides the drug — IV artesunate for severe malaria, oral ACT for uncomplicated, empiric ceftriaxone if septic or typhoid suspected, doxycycline if an eschar is found.
Monitor and disposition: track conscious level, lactate, haemoglobin and perfusion serially; admit by severity; give an explicit, dated safety net for the discharged child.
Epidemiology & Risk Factors
Fever is the cardinal presenting complaint of the ill returned traveller, accounting for roughly a third of all post-travel morbidity in GeoSentinel cohorts. The probability of a specific cause is overwhelmingly a function of where the child travelled, what they did there, and how long ago they returned, which is why a structured travel history outperforms any single laboratory test as a triage instrument. [1] [2]
Malaria dominates the life-threatening imported infections in most high-income surveillance systems. The disease is concentrated in returning travellers from sub-Saharan Africa, and within that group the highest-risk travellers are those visiting friends and relatives — families who migrate and then take their Australia-born or UK-born children back to a malarious home country, often without prophylaxis because the parents underestimate the risk to a non-immune child. Imported paediatric malaria carries a real risk of intensive-care admission and death, and severe disease is over-represented in children relative to adults because non-immune children tolerate high parasitaemia poorly. [3] [12]
Dengue is now the most common arboviral cause of febrile illness in returned travellers and its global burden has grown sharply, with modelled estimates of close to four hundred million infections a year and roughly a quarter of the world's population living in suitable transmission zones. Enteric fever remains common in returned travellers from South Asia, and antimicrobial resistance — including extensively drug-resistant (XDR) Salmonella Typhi — has reshaped empiric therapy, so the travel destination now dictates whether ceftriaxone or azithromycin is the safer first choice. [7] [10]
Risk is also shaped by the type of travel. Resort tourists staying in air-conditioned hotels have a different exposure profile to backpackers, rural visitors, or children staying in family villages with open housing, standing water and untreated water sources. Non-immune children, pregnant travellers, splenectomised or asplenic children, and the immunocompromised all convert a moderate-risk exposure into a high-risk one. The visiting-friends-and-relatives traveller is the single most important high-risk group to recognise, because they account for a disproportionate share of imported malaria and typhoid and are the group most often missed by pre-travel services. [1] [10]
Pathophysiology
Two pathogens dominate the risk of death in the febrile returning child, and each kills by a distinct mechanism that the clinician must be able to picture. Understanding the mechanism drives both the urgency and the monitoring — you watch for the complication the pathogen is actually capable of producing, not a generic set of observations. [5]
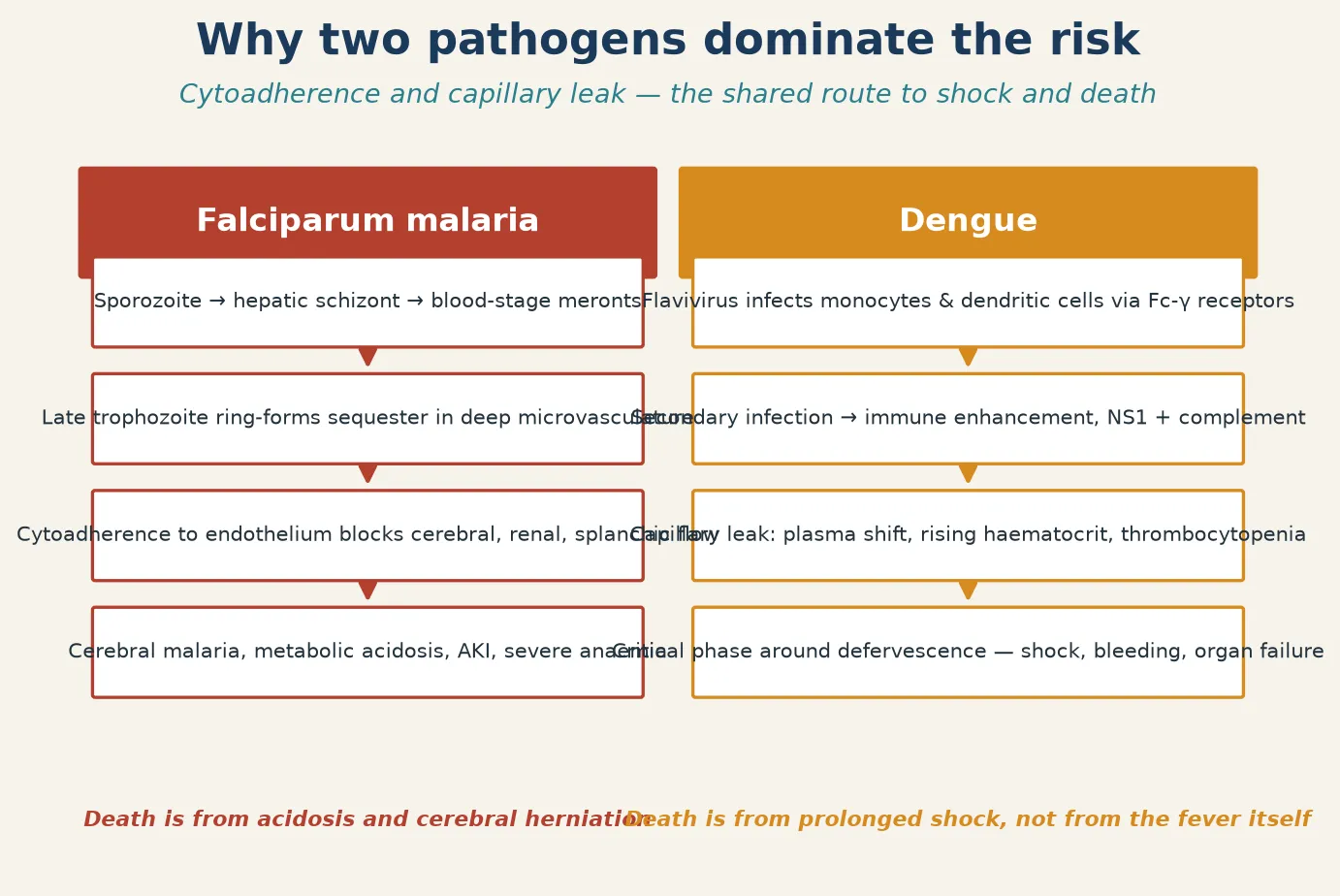
In falciparum malaria, the sporozoite inoculated by the anopheline mosquito travels to the liver, multiplies as hepatic schizonts, and releases merozoites that infect erythrocytes. The decisive virulence feature is that ring-stage parasites of Plasmodium falciparum express PfEMP-1 on the infected red-cell surface, causing cytoadherence to the vascular endothelium of deep microvascular beds — cerebral, renal, splanchnic and placental. Sequestered parasites evade splenic clearance and obstruct microvascular flow, producing the recognisable severe phenotypes: cerebral malaria (impaired consciousness, seizures), metabolic acidosis, acute kidney injury, severe anaemia from haemolysis and splenic clearance, and respiratory distress. Death is driven by acidosis and cerebral herniation, which is why the assessment of the returning child must include the conscious level, the lactate and the haemoglobin — the three numbers that tell you whether falciparum is killing this child now. [5]
In dengue, a flavivirus infects monocytes and dendritic cells, and in a secondary infection the pre-existing antibody does not neutralise but instead enhances uptake through Fc-γ receptors — the phenomenon of antibody-dependent enhancement. The NS1 viral protein and complement activation injure the endothelium, producing the defining lesion of severe dengue: increased capillary permeability and plasma leak. The haematocrit rises as plasma leaves the intravascular space, thrombocytopenia develops, and around the time of defervescence — typically day three to seven — the child enters a critical phase of leak that can progress to dengue shock syndrome. The dangerous paradox is that the child looks better as the fever falls, exactly when the risk of shock peaks, which is why the haematocrit trend, the pulse pressure and the capillary refill must be watched through and beyond defervescence. [7]
The other must-not-miss pathogens operate on shorter or different timelines. The rickettsiae (Rickettsia and Orientia tsutsugamushi) infect endothelial cells, producing a vasculitis with the characteristic eschar at the inoculation site and a rash that may be faint. Salmonella Typhi and Paratyphi cause a systemic illness dominated by sustained bacteraemia and macrophage dissemination to the reticuloendothelial system, with the classical stepwise-rising fever and relative bradycardia that are less reliable in children than the textbooks imply. The viral haemorrhagic fevers (Ebola, Lassa, Marburg, Crimean–Congo) share an early non-specific phase and a later bleeding-diathesis phase driven by endothelial dysfunction and platelet consumption, which is why the first action for any child febrile within three weeks of a risk area is isolation. [3] [8]
Clinical Presentation
The presentation of post-travel fever is, for most of its course, deliberately ordinary: fever, headache, myalgia, fatigue and anorexia — a picture indistinguishable from a viral upper-respiratory infection. This is the central trap, and the response to it is structural rather than diagnostic. The clinician does not try to recognise malaria from its symptoms; the clinician asks the travel history of every febrile child and then looks for the features that signal the dangerous diagnosis. [2]
Falciparum malaria classically produces a non-specific febrile illness that may or may not show the tertian periodicity the examinations love. In a non-immune child the more useful signs are those of severe disease: impaired consciousness, prostration, multiple seizures, respiratory distress (acidotic breathing), jaundice, dark urine (blackwater fever from haemolysis), pallor and bleeding. A child with any of these after return from a malarious area is in a resuscitation pathway, not an outpatient one. [11] [12]
Dengue presents with high fever, retro-orbital pain, severe myalgia and arthralgia (break-bone fever), a maculopapular rash, and sometimes minor bleeding manifestations — petechiae, mucosal bleeding, a positive tourniquet test. The warning signs that herald progression to severe dengue are the ones to elicit and document: abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation (ascites, pleural effusion), mucosal bleeding, lethargy or restlessness, liver enlargement greater than two centimetres, and a rising haematocrit with a falling platelet count. These signs declare the leak before the shock, and catching them is the difference between careful fluid titration and a crash resuscitation. [7]
Enteric fever in children is less classical than in adults. The systematic review of paediatric typhoid by Britto and colleagues showed that the stepwise fever, rose spots, relative bradycardia and splenomegaly are insensitive in young children, who more often present with a non-specific febrile illness, diarrhoea or constipation, cough, and hepatosplenomegaly — meaning typhoid is a diagnosis you suspect from the travel history and confirm by culture, not one you recognise at the bedside from textbook signs. Scrub typhus and the spotted-fever rickettsioses present with fever, headache, myalgia and, crucially, an eschar — a painless black necrotic lesion with a red halo at the site of the chigger or tick bite — together with a rash and, in severe cases, pneumonitis, meningoencephalitis or multi-organ failure. [8] [3]
Differential Diagnosis
The differential of post-travel fever is large, but it resolves quickly once the clinician fixes the three axes of incubation, syndrome and geography. The first move is always to decide whether malaria is possible, because the cost of missing it is death and the cost of excluding it is a competent same-day blood film. If the child has been in a malaria-endemic area within the relevant window, malaria is on the list until the film says otherwise — and a single negative film does not remove it. [2] [6]
Beyond malaria, the dangerous diagnoses to hold are dengue (especially in the child approaching defervescence), enteric fever (especially from XDR-prevalent regions of South Asia), the rickettsial diseases (especially with an eschar or rural exposure), meningococcal disease (which travel does not cause but does not exclude), and the viral haemorrhagic fevers (which demand immediate isolation and a public-health call). Each of these has a time-critical therapy: artesunate for severe malaria, careful fluid balance for dengue, ceftriaxone or azithromycin for typhoid, doxycycline for rickettsiae, and supportive isolation plus specific protocols for the viral haemorrhagic fevers. [3] [10]
The benign or self-limiting causes remain numerically dominant and must not be forgotten in the hunt for the exotic. The common childhood viral respiratory and gastrointestinal infections, otitis media, urinary tract infection, pneumococcal and staphylococcal sepsis, and viral exanthems all occur in returned travellers, and many of these are the actual diagnosis. The discipline is to exclude the dangerous few efficiently and then treat the common cause that remains, rather than investigating every conceivable tropical pathogen. [1] [2]
A short list of non-infectious mimics should be held for the atypical or prolonged case: Kawasaki disease (which travel can precede and confuse), malignancy presenting with fever, drug fever, and inflammatory conditions. Finally, dual pathology is common in the returned traveller — a child can have malaria and a bacterial co-infection, or dengue with leptospirosis — so a positive film or a consistent syndrome never closes the diagnostic loop, and the child who is not behaving as expected after the first diagnosis is made must be re-evaluated for a second. [3]
Clinical & Bedside Assessment
The bedside assessment begins before the examination, with a structured travel history taken from every febrile child regardless of how ordinary the illness looks. Ask the destination in detail (country, region, urban versus rural), the dates of travel and the time since return, the reason for travel (tourist, visiting friends and relatives, newly arrived migrant), the activities and exposures (fresh water, animals, insect bites, barefoot walking, unscreened accommodation), the prophylaxis taken (antimalarials — which, and were they completed? — and vaccinations), and the pre-existing conditions (asplenia, immunocompromise, pregnancy). This history is the single highest-yield investigation in the whole encounter. [2] [1]
The examination is then targeted to find the severe, not merely to confirm the febrile. Use a validated paediatric early-warning score and assess the airway, breathing and circulation first, because the returning child in shock from falciparum or dengue needs resuscitation in parallel with, not after, the diagnostic workup. Examine specifically for the features of severe malaria (conscious level using a paediatric Glasgow or Blantyre coma scale, pallor, jaundice, dark urine, hepatosplenomegaly, acidotic breathing), the warning signs of severe dengue (abdominal tenderness, persistent vomiting, fluid accumulation, mucosal bleeding, lethargy, a rising haematocrit), the eschar and rash of the rickettsial diseases, and the neck stiffness and petechiae of meningococcal disease. [11] [7]
Assess and document the hydration and perfusion, the respiratory rate and work of breathing, and the mental state at baseline and serially, because the trajectory matters more than any single reading. In the infant or pre-verbal child, behavioural change — irritability, lethargy, refusal to feed — is often the only signal of severe disease, so the threshold for investigation and observation is lower in the youngest returned travellers. Where the family speak a language other than English, use a trained interpreter rather than a family member, because the travel and exposure details are too important to lose in translation. [1] [3]
Investigations
There is no single panel for post-travel fever; the investigations follow the differential generated by the travel history. The non-negotiable test in any child with possible malaria exposure is the thick and thin blood film, examined urgently and on the same day as presentation. The thick film concentrates parasites for sensitivity; the thin film speciates and allows a parasitaemia percentage to be calculated. A rapid diagnostic test for malaria antigen (HRP-2 for falciparum, or a combination test) is a useful adjunct where microscopy is delayed or inexperienced, but it does not quantify parasitaemia and does not replace the film. [6] [11]
The single most important investigation pitfall in this topic is the false security of the negative film. A single negative malaria blood film does not exclude malaria, because parasitaemia fluctuates, the film quality depends on the microscopist, and low-level infection can be missed. The standard is to repeat the film at twelve- to twenty-four-hour intervals — and to repeat it sooner if the child deteriorates — until either malaria is found or an alternative diagnosis is secured and the clinical course is clearly consistent with it. A child with possible malaria who is sent home after one negative film, without a repeat, is the classic examination and real-world error. [6] [11]
The baseline panel for the unwell returning child includes a full blood count and film, C-reactive protein, urea and electrolytes, liver function tests, glucose, lactate, blood cultures (taken before antibiotics where possible but not delaying them in the septic child), and a urinalysis and urine culture. In the child with diarrhoea, send stool for culture and molecular testing including the travel-relevant pathogens. Dengue serology and NS1 antigen are sent where the syndrome or geography fits, with the understanding that the day of illness affects the sensitivity of each test (NS1 early, IgM later). Typhoid is confirmed by blood or marrow culture; bone marrow culture remains the gold standard but is rarely needed in practice, and a single negative blood culture does not exclude enteric fever. [8] [10]
Specific tests follow the differential: serology and PCR for the rickettsial diseases (treatment must never wait for these), viral hepatitis serology for the jaundiced or prolonged case, and tuberculosis screening for the long-standing febrile child. For any child with possible viral haemorrhagic fever, the laboratory workup is paused until isolation and public-health protocols are in place, because the routine blood sample from an unrecognised VHF case is a serious nosocomial hazard. [3]
Management — Resuscitation
The resuscitation of the unwell returning child follows the same structured priorities as any paediatric emergency, with two additions driven by the travel context. First, the malaria film is part of the resuscitation, not a downstream test — it is sent in the first blood draw alongside the cultures and venous gas. Second, the possibility of a viral haemorrhagic fever must be assessed before any aerosol-generating procedure or unprotected contact, because a single unrecognised case endangers the whole department. [11] [3]
Open and secure the airway, give high-flow oxygen to any child in shock or respiratory distress, and establish intravenous or intraosseous access. Take bloods for the full panel and cultures, then give empiric antibiotics to the septic or severely unwell child without waiting for the film result — a broad-spectrum agent such as ceftriaxone covers the common bacterial sepsis syndromes and typhoid, and the addition of antimalarial therapy is governed by the film and the severity assessment, run in parallel. [12] [6]
In suspected severe malaria, do not delay specific therapy for further confirmation. The child with possible severe falciparum malaria — impaired consciousness, multiple seizures, respiratory distress, severe anaemia, jaundice or a high parasitaemia — receives intravenous artesunate immediately. The AQUAMAT trial, a large open-label randomised trial in African children, showed that parenteral artesunate reduced mortality relative to quinine, and artesunate is faster-acting, safer (no cinchonism, hypoglycaemia or cardiac monitoring) and easier to give than quinine. If artesunate is not immediately available, intramuscular artesunate or, as a holding measure, quinine is used while the preferred drug is sourced — but the default is artesunate for severe disease. [5] [4]
For suspected dengue, the resuscitation principle is the opposite of sepsis: careful, titrated fluid rather than aggressive boluses, because the lesion is capillary leak and excessive crystalloid worsens the plasma shift and the risk of fluid overload and respiratory compromise. The child with compensated shock receives cautious isotonic crystalloid boluses with frequent reassessment of perfusion, haematocrit and urine output; the child in profound or decompensated shock needs more vigorous resuscitation and a higher level of care, but always with the understanding that the leak is time-limited and the fluids must be tapered as the critical phase passes. [7]
Management — Definitive & Stepwise
Definitive management is syndrome-driven and follows a three-lane pathway: immediate resuscitation, same-day diagnosis, and severity-driven treatment. The immediate lane (the first hour) is the structured ABC assessment, the early-warning-score-driven decision on stability, the isolation assessment for VHF risk, and the first blood draw including the malaria film and cultures. The diagnostic lane (one to four hours) completes the thick and thin films (with repeat planned if negative), the baseline panel, and the syndrome-specific tests. The treatment lane (four to twenty-four hours) delivers the definitive therapy chosen by the diagnosis and its severity. [6] [11]
For uncomplicated falciparum malaria in a child who is not severely unwell, oral artemisinin-based combination therapy (ACT) is first-line — the options and weight-based dosing are set by the national treatment guideline (atovaquone-proguanil, artemether-lumefantrine, or dihydroartemisinin-piperaquine depending on the region and resistance). For severe falciparum malaria, intravenous artesunate is mandatory, followed by a full course of ACT once the child can tolerate oral therapy and the parasitaemia is falling. The child is monitored for the complications of severe disease (anaemia, renal impairment, acidosis, cerebral oedema) and for post-artesunate delayed haemolysis, a recognised phenomenon two to three weeks after treatment that warrants a follow-up haemoglobin. [5] [6]
For enteric fever, the empiric choice is dictated by the destination and the local resistance pattern. For travel to South Asia, where XDR Salmonella Typhi resistant to ampicillin, chloramphenicol, co-trimoxazole, fluoroquinolones and third-generation cephalosporins has emerged, azithromycin is often the safer empiric oral choice while culture and sensitivity are awaited, with ceftriaxone reserved for severe disease or proven susceptibility. The GeoSentinel analysis of enteric fever in international travellers confirmed the rising resistance profile and the geographic pattern, underlining that the empiric antibiotic is a travel-history decision, not a generic one. [10] [8]
For the rickettsial diseases, doxycycline is first-line at all ages — the classical concern about dental staining in young children is outweighed by the mortality of untreated scrub or spotted-fever rickettsiosis, and short courses are acceptably safe. Treatment is started on clinical suspicion (eschar, rash, thrombocytopenia, appropriate exposure) and never waits for serology, because the antibody response takes weeks and the disease can kill in days. For dengue, definitive management is supportive and fluid-based through the critical phase, with transfusion reserved for significant bleeding, strict fluid tapering as the leak resolves, and a low threshold for higher-acuity care if shock is refractory. For the viral haemorrhagic fevers, management is isolation, supportive care, and immediate activation of the public-health and infectious-diseases protocol — the specific therapy (where one exists, as for Lassa) is delivered within that framework. [3] [7]
Specific Subtypes & Scenarios
The visiting-friends-and-relatives traveller is the single most important subtype to recognise. These families — often migrants returning to their country of origin with non-immune children born in Australia or New Zealand — account for a disproportionate share of imported malaria and typhoid. They are less likely to have sought pre-travel advice, less likely to have taken prophylaxis, and more likely to have had high-intensity rural exposure, because they stay in family homes rather than tourist accommodation. Recognising this group in the waiting room, and asking the travel question that surfaces them, is the difference between catching their malaria early and catching it in intensive care. [1] [10]
The child with severe falciparum malaria is the prototypical time-critical case. The AQUAMAT trial randomised over five thousand African children with severe falciparum malaria to artesunate versus quinine and showed a relative reduction in mortality with artesunate; the earlier SEAQUAMAT trial in Asian adults had shown the same direction of effect, establishing artesunate as the global standard for severe disease across age groups. The child receives artesunate immediately, is monitored for acidosis, renal failure, anaemia and seizures, and is watched for the post-artesunate delayed haemolysis that can appear weeks later. [5] [4]
The child approaching dengue defervescence is the deceptive case. As the fever falls on day three to seven the family relaxes and the clinician may be tempted to discharge, yet this is exactly when the capillary leak peaks and the shock declares. The management discipline is to measure the haematocrit and the pulse pressure through the transition, to recognise the warning signs (abdominal pain, persistent vomiting, lethargy, fluid accumulation), and to titrate fluids carefully through a leak that is time-limited but potentially profound. [7]
The child with scrub typhus or a spotted-fever rickettsiosis is the case where a single physical sign — the eschar — anchors the diagnosis. The eschar is a painless black necrotic lesion with an erythematous halo at the site of the chigger or tick bite, found in a febrile child with rural tropical exposure and often a faint maculopapular rash. Doxycycline is given on suspicion and is life-saving; the disease can progress to pneumonitis, meningoencephalitis and multi-organ failure within days, so serological confirmation is retrospective, not decisional. [3]
The child with possible viral haemorrhagic fever is the case that reorders the whole department. A child febrile within twenty-one days of returning from an area with an active outbreak of Ebola, Lassa, Marburg or Crimean–Congo haemorrhagic fever, especially with bleeding or unexplained organ failure, is placed in isolation and the public-health and infectious-diseases teams are contacted before any further assessment, blood test or aerosol-generating procedure. The risk to staff and other patients is the governing principle, and the decision to isolate is made on the travel history alone, before any laboratory confirmation. [3]
Complications & Pitfalls
The cardinal pitfall is failing to ask the travel history. Every examination, every guideline, and every mortality review of imported paediatric malaria returns to the same point: the child who dies of falciparum in a high-income hospital is the child whose travel history was not taken, whose malaria film was not sent, or whose negative film was believed. The structural defence is to make the travel question routine — asked of every febrile child, documented, and acted on. [12] [11]
The second pitfall is believing a single negative film. Malaria is a parasitaemic, fluctuating infection, and the sensitivity of a single film is imperfect; the repeat film is a standard of care, and the child who deteriorates is re-bled and re-filmed regardless of the previous result. Coupled with this is the error of treating the parasitaemia percentage as the sole determinant of severity — a child can be severely unwell with a modest parasitaemia and well with a high one, so the clinical severity, not the laboratory number, drives the decision between oral ACT and intravenous artesunate. [6] [5]
The third pitfall is discharging the child with dengue as the fever falls. The defervescence window is the highest-risk period, and the child sent home at the moment of falling fever is the child who returns in shock. The haematocrit trend, the warning signs and the perfusion are the guardrails, and observation through the transition is the safer default. [7]
The fourth pitfall is missing the eschar. The painless black lesion of scrub typhus is easy to overlook in a fretful, febrile child, yet it is the single most specific clue in the whole encounter, and finding it converts an undifferentiated fever into a treatable, life-saving diagnosis within the hour. Examine the whole skin, including the scalp, axillae, groin and flexures, in any febrile child with rural tropical exposure. [3]
The fifth pitfall is wrong empiric antibiotics for typhoid. In a child returning from South Asia, fluoroquinolones and even third-generation cephalosporins may not cover the XDR strain, and the empiric choice must reflect the destination's resistance pattern — azithromycin for uncomplicated suspected XDR typhoid, with escalation guided by culture. Treating all typhoid the same, regardless of where it was acquired, is an antimicrobial-stewardship and a patient-safety error. [10] [8]
Prognosis & Disposition
The prognosis of post-travel fever is overwhelmingly good once the dangerous diagnoses are found and treated promptly. Uncomplicated malaria treated with an ACT resolves fully; severe malaria treated with artesunate within hours of the onset of severity has a good outcome, but mortality rises with delay, acidosis, renal failure and deep coma — which is why the time from presentation to artesunate is the single most important prognostic variable in the severe case. The systematic GeoSentinel data on potentially life-threatening tropical disease in travellers confirm that the outcomes in well-resourced settings are driven less by the pathogen than by the speed of recognition. [3] [5]
Dengue is self-limiting in most children but carries a small, real mortality in those who progress to severe shock; the prognosis is determined by the quality of fluid management through the critical phase, and the children who do badly are those who present late, are discharged at defervescence, or receive fluid that is too aggressive or too timid. Enteric fever resolves with appropriate antibiotics, but the rising resistance profile means that a child treated with an inactive drug may deteriorate before culture returns — reinforcing that the empiric choice is a travel-history decision. [7] [10]
Disposition follows severity and the reliability of follow-up. The well child with a clear, benign, non-tropical diagnosis and a competent negative malaria film may be discharged with a safety net and a clear return pathway. The child with uncomplicated malaria is managed as an inpatient or under close supervision depending on age, parasitaemia and social factors. The child with severe malaria, dengue with warning signs, suspected typhoid from a high-resistance region, or any rickettsial or VHF suspicion is admitted to an appropriate level of care — ward, high-dependency or intensive care as the severity dictates — with paediatric infectious-diseases involvement. [11] [12]
The safety net is explicit and dated: return immediately if the fever pattern changes, if the child becomes lethargic, if bleeding or rash appears, if oral intake or urine output falls, or if the family is simply worried. Every child discharged after a negative malaria film is given a planned repeat-film review, and the family is told, in plain language, that one negative test does not exclude malaria. [6]
Special Populations
The visiting-friends-and-relatives family deserves a targeted approach in both the acute and the pre-travel setting. These children are the highest-risk group for imported malaria and typhoid, and the consultation is an opportunity to ensure the whole family has pre-travel advice for future visits, including prophylaxis, vaccination and a clear plan for febrile illness abroad. The acute-team and the primary-care team share this responsibility, because the next visit will happen and the risk will recur. [1] [10]
The newly arrived migrant, refugee or asylum-seeking child may present with fever acquired before or during migration and may have had incomplete or no screening. Consider tuberculosis, viral hepatitis, schistosomiasis, strongyloidiasis, malaria (depending on route), and the chronic consequences of incomplete vaccination. Use trained interpreters, and frame the assessment as comprehensive care rather than a narrow post-travel screen, because these children carry a heavier burden of undiagnosed disease than the tourist traveller. [3]
The immunocompromised or asplenic child converts a moderate tropical exposure into a high-risk one. The asplenic child is at catastrophic risk of severe malaria and of encapsulated-bacterial sepsis, and any fever is treated as an emergency; the immunocompromised child may present atypically and may have unusual or opportunistic pathogens, lowering the threshold for investigation, admission and infectious-diseases consultation. [11]
The Indigenous child travelling to or from remote communities may have different baseline infectious risk and may face access barriers to rapid diagnostics and to inpatient care. Rural and remote returning children need a low threshold for retrieval and a clear escalation pathway, because the window between recognising severe malaria and being able to deliver artesunate is longer when the child is far from a centre. [12]
The infant and the pre-verbal child are the groups in whom the dangerous diagnosis is easiest to miss, because the classical signs are absent and the only signal is behavioural change. Hold a lower threshold for investigation, observation and admission in the youngest returned travellers, and rely on the parents' reading of the child's behaviour as a clinical sign in its own right. [1]
Evidence, Guidelines & Regional Differences
The evidence base for post-travel fever rests on three pillars. The first is the GeoSentinel surveillance network, whose analyses define the probability of disease by destination, traveller type and syndrome: the foundational spectrum-of-disease paper by Freedman and colleagues, the fever-in-returned-travellers analysis by Wilson and colleagues, and the life-threatening-tropical-disease analysis by Jensenius and colleagues together give the clinician a data-driven prior for any given returning child. These papers are the backbone of the regional probability reasoning that anchors the differential. [1] [2] [3]
The second pillar is the severe-malaria treatment evidence. The SEAQUAMAT trial established artesunate over quinine for severe falciparum malaria in Asian adults, and the AQUAMAT trial confirmed the mortality benefit in African children, making intravenous artesunate the global standard of care for severe disease. The UK malaria treatment guidelines translate this and the broader evidence into a practical, severity-driven pathway that is widely used as a reference framework beyond the United Kingdom. [4] [5] [6]
The third pillar is the regional-resistance evidence. The spread of artemisinin resistance in Plasmodium falciparum across the Greater Mekong subregion, documented by Ashley and colleagues, complicates the management of malaria acquired in Southeast Asia and underlines the need to know the origin. The GeoSentinel analysis of enteric fever in travellers documented the rising prevalence of XDR Salmonella Typhi in South Asia, reshaping empiric typhoid therapy. The Bhatt dengue global-burden model redefined the scale of dengue and its reach into previously unaffected regions, and the Britto systematic review of paediatric enteric fever clarified that the classical typhoid signs are unreliable in children. [9] [10] [7] [8]
Regional differences are real and decisional. In Australia and New Zealand, the returning child from Papua New Guinea, the Solomon Islands or Vanuatu carries a high falciparum risk, and artesunate must be available in every tertiary paediatric centre; the child from Southeast Asia may have an artemisinin-resistant strain and a dengue co-risk; the child from South Asia may have XDR typhoid. The WHO guidelines for malaria treatment and the WHO dengue guidelines provide the global framework, and the national guidelines (Australia's Therapeutic Guidelines, the UK malaria treatment guidelines, the CDC Yellow Book, and the RCPCH and AAP travel-medicine resources) translate it for local practice. [6] [1]
Exam Pearls
Fever in the returned traveller is an examination favourite because it rewards structured reasoning over factual recall. The single highest-yield action is the travel history, asked of every febrile child — destination, dates, reason for travel, activities, prophylaxis, and pre-existing conditions — because it generates the differential in the first minute. [2] [1]
The five you must not miss are malaria, dengue, enteric (typhoid) fever, rickettsial or scrub typhus, and the viral haemorrhagic fevers. Each has a time-critical therapy: intravenous artesunate for severe malaria (AQUAMAT, mortality benefit over quinine), careful titrated fluid for dengue through defervescence, ceftriaxone or azithromycin for typhoid depending on regional resistance, doxycycline for the rickettsial diseases (started on suspicion, never waiting for serology), and immediate isolation with a public-health call for suspected viral haemorrhagic fever. [5] [3]
The single negative film never excludes malaria — repeat it at twelve to twenty-four hours, and sooner if the child deteriorates. The incuded incubation window narrows the differential: under two weeks points to dengue, malaria, influenza and the rickettsiae; two to six weeks brings in typhoid and viral hepatitis; beyond six weeks, relapsing malaria, tuberculosis and visceral leishmaniasis. The visiting-friends-and-relatives traveller is the highest-risk group and the one most often missed. [6] [11]
For the orals and the long case, be ready to defend the severity-driven antimalarial choice: oral ACT for uncomplicated falciparum, intravenous artesunate for severe disease, with the threshold for severe defined by the clinical severity (impaired consciousness, acidosis, severe anaemia, renal failure, high parasitaemia) rather than the parasitaemia percentage alone. Know that XDR typhoid from South Asia has reshaped empiric therapy, that doxycycline is acceptable in young children with rickettsial disease, and that dengue kills by shock at defervescence, not during the fever. And always — always — isolate first and ask questions later for the child with possible viral haemorrhagic fever. [10] [7]
References
- [1]Freedman DO; Weld LH; Kozarsky PE; et al Spectrum of disease and relation to place of exposure among ill returned travelers. N Engl J Med, 2006.PMID 16407507
- [2]Wilson ME; Weld LH; Boggild A; et al Fever in returned travelers: results from the GeoSentinel Surveillance Network. Clin Infect Dis, 2007.PMID 17516399
- [3]Jensenius M; Han PV; Schlagenhauf P; et al Acute and potentially life-threatening tropical diseases in western travelers--a GeoSentinel multicenter study, 1996-2011. Am J Trop Med Hyg, 2013.PMID 23324216
- [4]Dondorp A; Nosten F; Stepniewska K; et al Artesunate versus quinine for treatment of severe falciparum malaria: a randomised trial. Lancet, 2005.PMID 16125588
- [5]Dondorp AM; Fanello CI; Hendriksen IC; et al Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, randomised trial. Lancet, 2010.PMID 21062666
- [6]Lalloo DG; Shingadia D; Bell DJ; et al UK malaria treatment guidelines 2016. J Infect, 2016.PMID 26880088
- [7]Bhatt S; Gething PW; Brady OJ; et al The global distribution and burden of dengue. Nature, 2013.PMID 23563266
- [8]Britto C; Pollard AJ; Voysey M; et al An Appraisal of the Clinical Features of Pediatric Enteric Fever: Systematic Review and Meta-analysis of the Age-Stratified Disease Occurrence. Clin Infect Dis, 2017.PMID 28369224
- [9]Ashley EA; Dhorda M; Fairhurst RM; et al Spread of artemisinin resistance in Plasmodium falciparum malaria. N Engl J Med, 2014.PMID 25075834
- [10]Hagmann SHF; Angelo KM; Huits R; et al Epidemiological and Clinical Characteristics of International Travelers with Enteric Fever and Antibiotic Resistance Profiles of Their Isolates: a GeoSentinel Analysis. Antimicrob Agents Chemother, 2020.PMID 32816733
- [11]Kiang KM; Bryant PA; Shingadia D; et al The treatment of imported malaria in children: an update. Arch Dis Child Educ Pract Ed, 2013.PMID 23171589
- [12]Garbash M; Round J; Whitty CJ; et al Intensive care admissions for children with imported malaria in the United kingdom. Pediatr Infect Dis J, 2010.PMID 21099654