Paeds · infectious-diseases
Fungal infections in immunocompetent and immunocompromised children
Also known as Paediatric mycoses · Invasive candidiasis in children · Invasive aspergillosis in children · Pneumocystis jirovecii pneumonia in children · Mucormycosis in children · Tinea capitis · Oral candidiasis (thrush) in children
Fellowship topic on fungal infections in children: the medically important fungi as yeasts (Candida, Cryptococcus, Malassezia), moulds (Aspergillus, Mucorales, dermatophytes), dimorphics and Pneumocystis; the superficial and mucocutaneous disease of the immunocompetent child (oral thrush, napkin candidiasis, tinea capitis, tinea corporis) and the invasive disease of the immunocompromised child (candidaemia, invasive aspergillosis, Pneumocystis pneumonia, mucormycosis, cryptococcosis, neonatal invasive candidiasis); neutrophil-versus-hyphae and T-cell-versus-Pneumocystis host defence and the breach points of central lines, neutropenia, total parenteral nutrition, broad-spectrum antibiotics, steroids, HIV and prematurity; blood-culture and non-culture diagnostics (beta-D-glucan, galactomannan, CT halo sign, biopsy histopathology, CSF cryptococcal antigen); the tiered antifungal armamentarium from topical azoles to oral griseofulvin and terbinafine to intravenous echinocandins, liposomal amphotericin B and voriconazole, with line removal, surgical debridement and reversal of immunosuppression; prophylaxis with fluconazole, caspofungin and trimethoprim-sulfamethoxazole; and ANZ, UK, US and Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The host-defence tiers that decide the antifungal strength
Overview & Definition
Picture a six-month-old brought to the clinic with white plaques on her tongue and a fretful, scaly scalp in a toddler in the next room. Both are common, everyday fungal infections of childhood — one a superficial yeast, one a dermatophyte — and both clear with a topical gel or an oral course. Now picture the child two beds away on the oncology ward, febrile for a week with no neutrophils and a central line in situ. The same kingdom of organisms that caused a harmless plaque in the clinic is now a life-threatening invasive disease. Recognising where any child sits on that spectrum — well host with superficial disease, or immunocompromised host with invasive disease — is the single judgement the fellowship examiner probes. [2] [14]
The medically important fungi are eukaryotic organisms that fall, clinically, into four groups. The yeasts — Candida, Cryptococcus and Malassezia — are single-celled and reproduce by budding. The moulds — Aspergillus, the Mucorales, and the dermatophytes that cause tinea — grow as branching hyphae. The dimorphic fungi (Histoplasma, Blastomyces, Coccidioides, Talaromyces) grow as moulds in the environment and as yeasts in tissue. And Pneumocystis jirovecii, once classified as a protozoan, is a fungus that behaves like an opportunistic pneumonitis of the T-cell-deficient host. Knowing which group an organism belongs to points to the host defence that contains it and the antifungal that kills it. [6] [14]
The clinician's job has two halves, and the second is what the fellowship rewards. The superficial half is to recognise the common mucocutaneous presentations — thrush, napkin candidiasis, tinea — and treat them with topical agents or a short oral course, while never missing the immunocompromised host in whom a "minor" fungal infection is the first clue to a deeper defect. The invasive half is to recognise the immunocompromised child at the point of breakdown — the persistent febrile neutropenia, the necrotic nasal eschar, the hypoxaemia out of proportion to the X-ray — and treat with the right intravenous antifungal, the right source control, and the right reversal of immunosuppression. [1] [7]
Classification
Classify fungal disease the way you meet it at the bedside — by host, by depth, and by organism — because each lens changes the drug, the route and the urgency. The host lens separates the immunocompetent child, whose intact neutrophils and T-cells confine fungi to the skin and mucosa, from the immunocompromised child, whose broken defences let the same organisms invade the bloodstream, the lung and the brain. This is the lens that matters most, because it is the host, not the organism name, that decides whether a child gets a cream or an amphotericin drip. [14] [2]
The depth lens runs alongside it. Superficial disease — skin, mucosa, hair and nail — is managed topically or with a short oral course, almost always as an outpatient. Invasive disease — bloodstream, lung, sinus, central nervous system, bone — demands intravenous antifungals, inpatient care, source control and a far higher mortality. A superficial yeast in a well child and a bloodstream yeast in a neutropenic child may share a name, but they are not the same illness, and treating them as the same is the dangerous default. [2] [6]
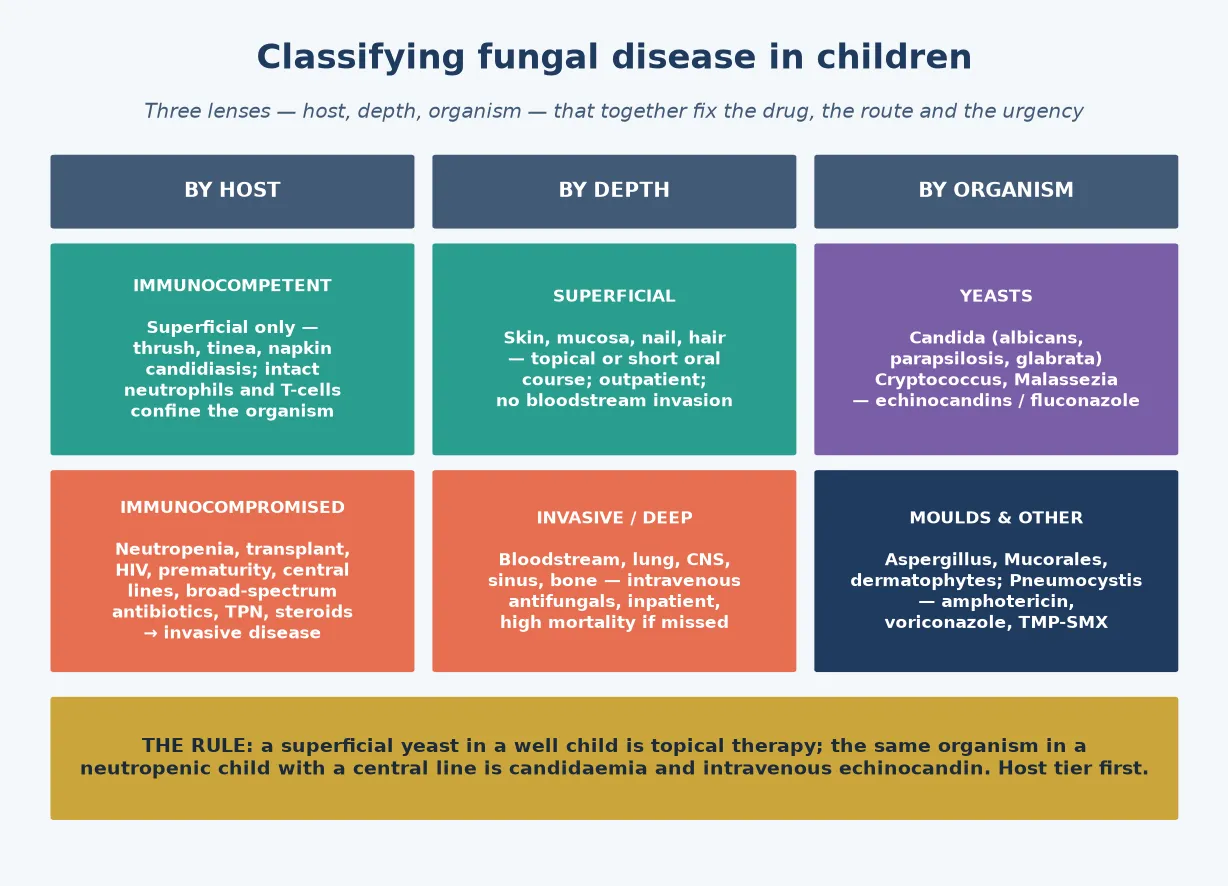
The organism lens completes the picture. The yeasts (Candida, Cryptococcus, Malassezia) are bud-forming single cells that drive bloodstream and meningeal disease and are treated with echinocandins, amphotericin or fluconazole. The moulds (Aspergillus, the Mucorales, the dermatophytes) grow as hyphae; the angioinvasive moulds invade vessel walls to cause thrombosis and infarction, while the dermatophytes live in keratin and cause tinea. The dimorphic fungi and Pneumocystis round out the list, each pointing to a specific host defence (T-cell) and a specific syndrome. [6] [10]
Within candidiasis, a final distinction matters: mucocutaneous disease (oropharyngeal thrush, oesophageal, vulvovaginal, napkin and cutaneous, chronic mucocutaneous candidiasis) versus invasive disease (candidaemia, deep-tissue, hepatosplenic, endocarditis, meningitis, endophthalmitis). Candidaemia is overwhelmingly line-related in children, and the non-albicans species — Candida parapsilosis in neonates and on lines, Candida glabrata and Candida krusei after prior fluconazole — influence the empirical choice because some are fluconazole-resistant. [2] [4]
Epidemiology & Risk Factors
Where do fungal infections sit in children, and who do they hurt? Superficial fungal infection is common: oral thrush peaks in the first months of life, tinea capitis is the commonest cause of hair loss in prepubertal children, and tinea corporis and tinea pedis are familiar across childhood and adolescence. Invasive fungal disease, by contrast, is concentrated in the immunocompromised — and the burden of severe disease falls squarely on a small group of high-risk hosts. [12] [4]
Candida remains the commonest invasive fungal pathogen in children. Candida albicans predominates, but non-albicans species take an increasing share: Candida parapsilosis thrives on central lines and in neonates, while Candida glabrata and Candida krusei emerge after prior fluconazole exposure and are often resistant to it. Candidaemia carries significant mortality in the immunocompromised child, and the neonate is especially vulnerable — invasive candidiasis in the very-low-birth-weight infant is associated with substantial mortality and long-term neurodevelopmental impairment. [2] [4]
The host-risk factors are the ones the examiner expects you to list. Prolonged and profound neutropenia, haematological malignancy, and stem-cell transplant (especially with graft-versus-host disease) drive invasive candidiasis and mould disease. Solid-organ transplant on calcineurin-inhibitor immunosuppression, HIV with a low CD4 count, prematurity and very low birth weight, central venous catheters, total parenteral nutrition, broad-spectrum antibiotics, and chronic corticosteroids each erode a specific limb of fungal defence. Holding these in mind turns a vague "immunocompromised" label into a precise risk profile. [14] [1]
The mould diseases have their own triggers worth naming. Invasive aspergillosis tracks prolonged neutropenia and graft-versus-host disease. Mucormycosis associates with iron overload, diabetic ketoacidosis, profound neutropenia, and deferoxamine therapy. Environmental dust and hospital construction can aerosolise mould spores that an immunocompromised child inhales. And Pneumocystis pneumonia selects the T-cell-deficient host — the HIV-exposed infant, the transplant recipient, and the child on chronic steroids. Recognising the trigger focuses the differential and the empirical cover. [6] [7]
Pathophysiology
Why is a fungus trivial in a well child and lethal in a neutropenic one? The answer lies in the host-defence cascade — three limbs of innate and adaptive immunity that each contain a different fungal group. Neutrophils phagocytose and kill Candida and Aspergillus hyphae, which is why a fall in neutrophils is the key risk for invasive yeast and mould disease. Macrophages ingest and contain the inhaled mould spores that reach the alveolus. And T-cell-mediated immunity holds Pneumocystis and the dimorphic fungi in check, which is why HIV and transplant immunosuppression open that door. [14] [6]
The breach points convert a superficial coloniser into an invasive pathogen. The central venous line is a highway for Candida into the bloodstream, which is why candidaemia is overwhelmingly line-related in children and why line removal shortens the bacteraemia. Mucositis from chemotherapy and the flora disruption of broad-spectrum antibiotics select for Candida overgrowth in the gut. Total parenteral nutrition is a growth substrate for yeast. And neutropenia simply removes the cell that would have killed the organism. Each breach is a point where prophylaxis, source control or empirical therapy intervenes. [4] [14]
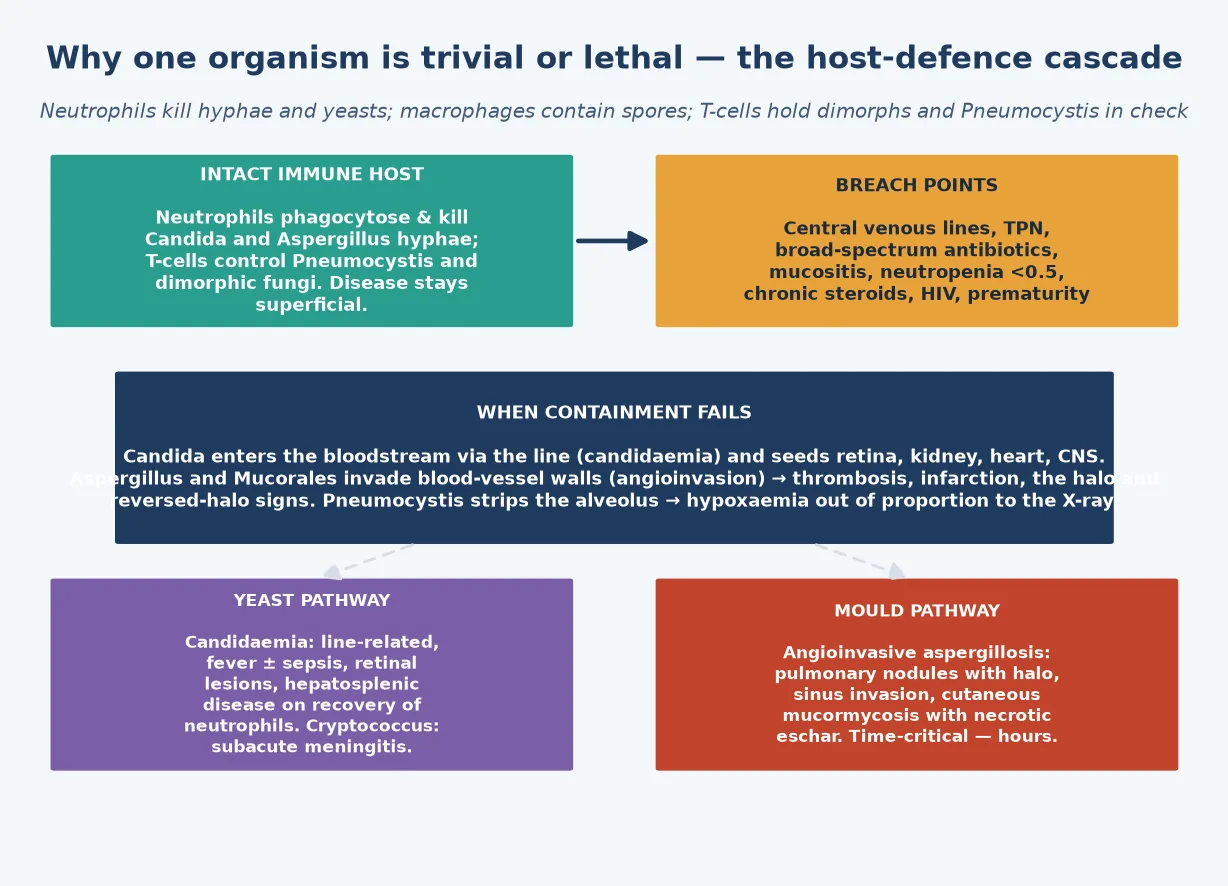
Angioinvasion is the hallmark of the moulds. Aspergillus and Mucorales hyphae invade blood-vessel walls, producing thrombosis, tissue infarction and the radiographic halo and reversed-halo signs. The necrotic palate or black nasal eschar in rhino-orbito-cerebral mucormycosis is infarcted tissue — not infection of intact skin — which is exactly why medical therapy alone cannot sterilise it and why surgical debridement is non-negotiable. The same angioinvasive mechanism underlies the catastrophic haemoptysis of pulmonary aspergillosis when an infarcted cavity erodes a bronchial vessel. [7] [6]
Pneumocystis jirovecii has its own biology. The organism fills the alveoli with a foamy exudate, producing hypoxaemia out of proportion to the chest X-ray and a characteristic diffuse bilateral interstitial pattern. Because it is controlled by T-cell immunity, it predominates in the HIV-exposed infant and the steroid-treated or transplant patient — and the inflammatory response to dying organisms during treatment is why adjunctive steroids improve survival in severe disease. Cryptococcus, likewise, exploits the T-cell-deficient host: inhaled organisms spread to the meninges, producing a subacute meningitis with a characteristically high CSF antigen and often a strikingly low inflammatory cell count. [9] [10]
Clinical Presentation
The immunocompetent child presents with the familiar superficial syndromes. Oral candidiasis (thrush) is a white, adherent plaque on the buccal mucosa, tongue and palate of the infant, with an erythematous base; it is distinguished from milk curd by adherence and bleeding on scraping. Tinea capitis presents with scaling, hair loss with black-dot broken hairs and occipital lymphadenopathy in the prepubertal child, and the inflammatory kerion is a boggy, tender, purulent mass. Tinea corporis is the annular, scaly, advancing plaque with central clearing, and tinea pedis affects the adolescent foot. [12] [8]
Candidaemia and invasive candidiasis present with fever — often the only sign in the neutropenic child — together with sepsis and the seeded sites that declare themselves on examination. Retinal lesions on fundoscopy (endophthalmitis) threaten vision, skin nodules declare disseminated disease, hepatosplenic lesions appear as neutrophils recover, and endocarditis and central nervous system disease deepen the illness. The point is that candidaemia is a systemic disease with a checklist of seeded sites, and each must be sought — fundoscopy is part of the management, not an afterthought. [2] [4]
Invasive aspergillosis presents with persistent fever despite antibiotics in the neutropenic patient, pleuritic chest pain, haemoptysis, and pulmonary nodules with the halo sign on computed tomography. Invasive sinus aspergillosis brings facial pain and orbital involvement. Rhino-orbito-cerebral mucormycosis brings facial or palatal pain, a black necrotic eschar, and rapidly progressive cranial-nerve or orbital signs. And Pneumocystis pneumonia presents with a subacute onset of dyspnoea, dry cough, tachypnoea and hypoxaemia out of all proportion to the chest X-ray in the HIV-exposed infant or the immunosuppressed child. [6] [7]
Cryptococcal meningitis presents subacutely in the T-cell-deficient host — headache, fever, cranial-nerve signs and altered mentation over days to weeks — and the clinical pitfall is attributing the indolent course to a viral illness while the meninges fill with organisms. Neonatal invasive candidiasis presents as line-related sepsis in the very-low-birth-weight infant — temperature instability, apnoea, feeding intolerance and a central line in situ — and the candidaemia is the reason to examine the retina, the skin and the central nervous system, remove the line, and treat systemically. [10] [4]
Differential Diagnosis
For the child with oral white plaques, the differential turns on whether the lesion wipes away. Milk curd wipes off an otherwise normal mucosa; thrush is adherent and leaves an erythematous base on scraping. Aphthous ulcers are discrete, non-adherent and non-febrile. Viral stomatitis — herpes simplex gingivostomatitis and coxsackievirus herpangina — produces painful ulcers and fever rather than adherent plaques. The key red flag is thrush outside infancy in a child with no inhaled-steroid exposure, which warrants investigation for immunocompromise. [12] [11]
For the annular scaly plaque, the differential distinguishes tinea corporis from its mimics. Granuloma annulare has a similar ring but no scale and no advancing border. Nummular eczema is scaly but wet and crusted, and psoriasis has a silvery scale on an erythematous base. The decisive error is treating an undiagnosed plaque with a topical steroid — the "tinea incognito" trap — which abolishes the scale and the itch, masks the diagnosis, and lets the fungus spread. Confirm tinea with a skin scraping for hyphae before reaching for a steroid. [12] [8]
For hair loss with scaling in a child, tinea capitis is the commonest cause in the prepubertal age group and must be distinguished from alopecia areata (smooth, hairless patches with no scale or inflammation), seborrhoeic dermatitis (greasy scale without hair loss), and traction alopecia (hair loss at the hairline from tight styling). Occipital lymphadenopathy alongside scaling and black-dot hairs is characteristic of tinea capitis. [12] [8]
For persistent fever in neutropenia, the differential includes invasive fungal disease (candidaemia, invasive aspergillosis, mucormycosis) alongside unresolving bacterial infection, viral reactivation (cytomegalovirus, Epstein-Barr virus), and drug fever. The persistent fever beyond four to seven days on appropriate broad-spectrum antibiotics is the trigger to add empirical antifungal therapy and to image the chest and sinuses — because the day the fever persists is the day a missed invasive fungal disease begins to cost the child. [1] [14]
Clinical & Bedside Assessment
The assessment begins with a focused history of the immune status, because the immune profile fixes the differential and the empirical cover. Establish the oncology diagnosis and the chemotherapy timing, the transplant type and date, the graft-versus-host status, the HIV status and the latest CD4, the corticosteroid and immunosuppressant doses, and the neutrophil count and its trajectory. Add the central-line and parenteral-nutrition status and the broad-spectrum antibiotic exposure, because each is a breach point that converts colonisation into invasion. [14] [4]
Examine for the focal signs that localise invasive fungal disease. Perform fundoscopy to look for candidal retinal lesions, examine the skin for ecthyma-gangrenosum-like nodules and necrotic eschars, inspect the nose and palate for the black eschar of mucormycosis, auscultate the chest for aspergillosis, and assess the neurological state for cryptococcal or candidal central nervous system disease. For the child with superficial disease, examine the distribution and character of the lesion — the annular scaly border, the black-dot hairs and occipital nodes, the boggy kerion, the erythematous napkin folds. [6] [2]
Document the elements that frame the antifungal choice and route. Record the absolute neutrophil count and trajectory, the central-line presence and site, the organ dysfunction, and the concurrent medications — because voriconazole, posaconazole and the calcineurin inhibitors interact, and a child on tacrolimus who starts voriconazole needs a level check and a dose reduction. Record the allergy history, the renal and hepatic function (amphotericin nephrotoxicity, azole hepatotoxicity), and the baseline electrolytes, because amphotericin wastes potassium and magnesium. [14] [13]
Recognise the time-critical findings that demand urgent imaging and empirical therapy. Persistent febrile neutropenia, a necrotic palatal or nasal eschar (mucormycosis), haemoptysis with a pulmonary halo sign (angioinvasive aspergillosis), and hypoxaemia disproportionate to the chest X-ray (Pneumocystis) are each reasons to act before the confirmatory test returns. A careful first encounter sets the host tier, the differential and the tempo of the response. [7] [9]
Investigations
Blood cultures are the cornerstone of invasive-candidiasis diagnosis. Take peripheral samples and samples from each lumen of the central line, recognise that Candida may take longer to grow than bacteria, and use the differential time to positivity to localise a line-related source. Pair the cultures with the decision to remove the central line, because a positive culture in a child with a line is both a diagnosis and a source-control mandate. [2] [3]
Non-culture diagnostics are used selectively and interpreted with care. Serum beta-D-glucan is positive in invasive Candida and Pneumocystis disease (but also with some bacterial infections and haemodialysis filters). Serum and bronchoalveolar-lavage galactomannan supports invasive aspergillosis (but is affected by piperacillin-tazobactam in some regions). CSF cryptococcal antigen, with its high sensitivity, is the key test for cryptococcal meningitis. None of these replaces biopsy histopathology for mould disease, and each carries false positives and negatives the candidate must name. [3] [6]
In Australia and Aotearoa New Zealand, blood cultures remain the standard for invasive candidiasis, with beta-D-glucan and galactomannan used as adjuncts in the oncology and transplant populations. The Australian Therapeutic Guidelines and the eviQ cancer-treatment protocols guide empirical and directed antifungal therapy and prophylaxis. Liposomal amphotericin B, the echinocandins (caspofungin, micafungin) and voriconazole are the workhorse inpatient agents, with therapeutic drug monitoring for voriconazole and posaconazole. [14]
Computed tomography is the imaging test for suspected mould disease. The halo sign — a pulmonary nodule surrounded by a ground-glass halo of haemorrhage — is the early finding of invasive pulmonary aspergillosis, and the reversed-halo sign favours mucormycosis. A plain chest radiograph is insensitive early in the neutropenic patient, so a normal film does not exclude invasive mould disease when the clinical picture fits. For Pneumocystis, the combination of hypoxaemia disproportionate to the chest X-ray, a raised serum lactate dehydrogenase and beta-D-glucan, and bronchoalveolar-lavage immunofluorescence or polymerase chain reaction frames the diagnosis. [6] [9]
Biopsy histopathology is the definitive test for mould disease when the child is stable enough. Tissue invasion by hyphae confirms invasive aspergillosis or mucormycosis, and the morphology points the way — broad, ribbon-like, non-septate hyphae favouring the Mucorales and narrower, acute-angle, septate hyphae favouring Aspergillus. The principle, as ever, is to investigate before, not instead of, starting empirical therapy, because the cost of a missed or delayed mould disease is measured in infarcted tissue and lives. [7] [6]
Management — Resuscitation
Resuscitation is about the time-critical invasive presentations: the persistent febrile neutropenia, the angioinvasive mould, the hypoxaemic Pneumocystis pneumonia, and the neonate with candidaemia and sepsis. Each is a reason to admit, to monitor closely, and to start empirical antifungal therapy promptly. The principle is that delaying therapy in the immunocompromised host who cannot contain the organism is the avoidable error, so the threshold to treat is low and the treatment is empirical. [14] [1]
Start empirical antifungal therapy for the persistent febrile neutropenic child after four to seven days of fever on broad-spectrum antibiotics. The choices are an echinocandin (caspofungin or micafungin) or liposomal amphotericin B, selected by the suspected organism, the local epidemiology, the toxicity profile and the concurrent medications. The decision is empirical because the cultures and biomarkers lag the clinical deterioration, and a neutropenic child's margin for delay is narrow. [1] [14]
Provide supportive care for the child with invasive fungal sepsis. Oxygen, fluid resuscitation and vasopressors treat shock. Correct the reversible immunosuppression where possible — granulocyte colony-stimulating factor in selected profound neutropenia, reducing the steroid dose, treating graft-versus-host disease, and controlling diabetic ketoacidosis in mucormycosis. The antifungal is necessary but not sufficient: source control and immune reconstitution together determine survival. [7] [4]
Manage severe Pneumocystis pneumonia with oxygen, high-dose intravenous trimethoprim-sulfamethoxazole and adjunctive corticosteroids for hypoxaemia. Steroids are given when the partial pressure of oxygen falls below about 70 millimetres of mercury or the saturation sits below about 92 percent on room air, because the steroid dampens the inflammatory pneumonitis that flares as the organisms die — and this single adjunct improves survival. For rhino-orbito-cerebral mucormycosis, treat the disease as a surgical emergency: urgent imaging, high-dose liposomal amphotericin B, and early surgical debridement of necrotic tissue, because mortality rises with every hour of delay. [9] [7]
Management — Definitive & Stepwise
Definitive management is a stepwise pathway matched to depth and host, with topical agents at one end, oral therapy in the middle, and intravenous antifungals at the other. The well child with superficial disease receives a topical agent. The child with tinea capitis receives oral griseofulvin or terbinafine. The child with invasive candidiasis receives an echinocandin or liposomal amphotericin B with line removal. The child with invasive mould disease receives a mould-active agent and surgical debridement. Each tier follows from the host-risk judgement made at the first encounter. [8] [14]
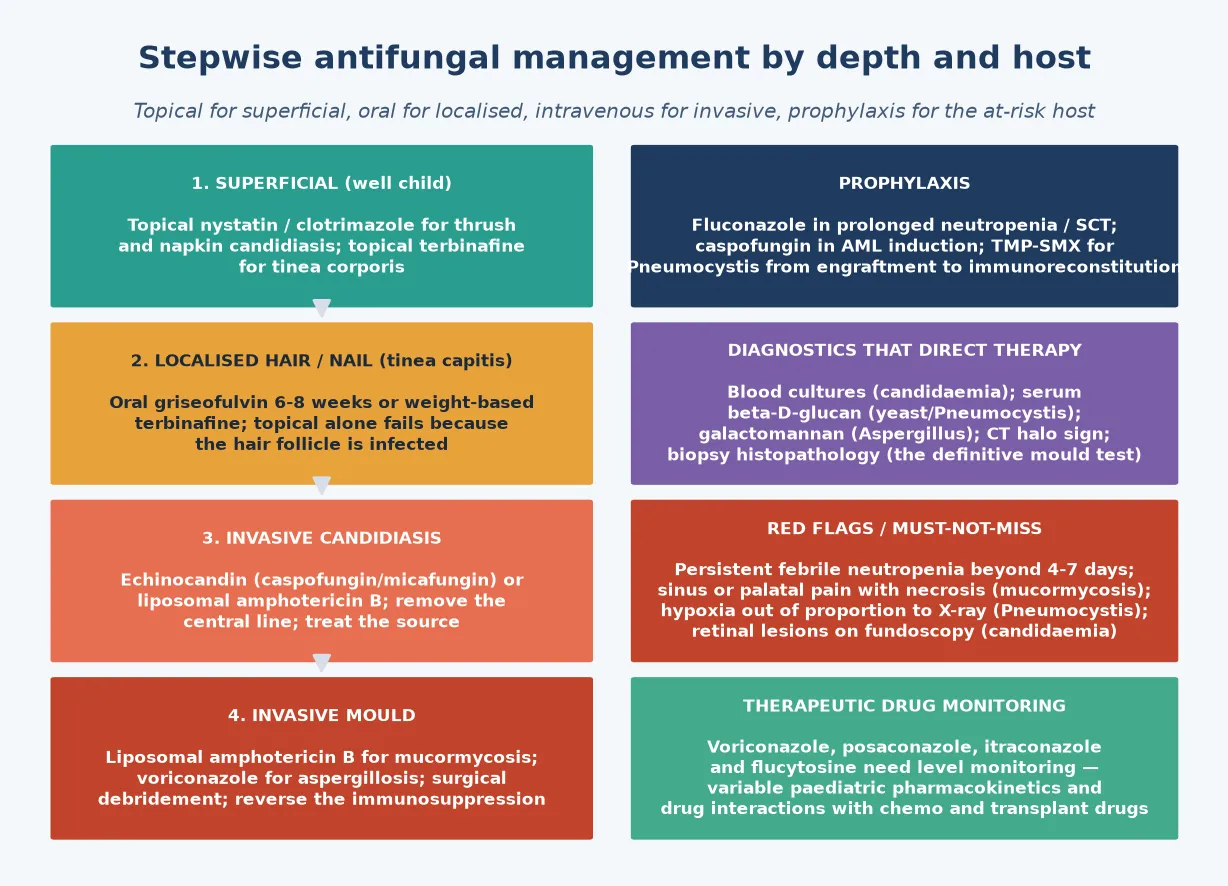
For the immunocompetent child with superficial disease, management is straightforward and outpatient. Oral candidiasis in the infant responds to oral nystatin suspension or miconazole oral gel, with treatment of the mother's nipples if she is breastfeeding. Refractory thrush, or thrush in the immunocompromised host, warrants oral fluconazole. Napkin candidiasis responds to a topical azole (clotrimazole, miconazole) with attention to the underlying napkin dermatitis. Tinea corporis and tinea pedis respond to a topical azole or terbinafine. [12] [8]
The stepwise antifungal pathway
Set the host-risk tier at first contact: immunocompetent with superficial disease (topical), tinea capitis (oral), immunocompromised with invasive disease (intravenous plus source control).
Superficial candidiasis and tinea corporis: topical nystatin, azole or terbinafine; outpatient; treat the underlying trigger (napkin wear, steroid exposure, household contacts in tinea).
Tinea capitis: oral griseofulvin for 6-8 weeks or weight-based terbinafine; selenium or ketoconazole shampoo to reduce shedding; exclude from school until treatment started; the kerion is an inflammatory variant needing oral antifungal, not incision.
Invasive candidiasis: echinocandin (caspofungin or micafungin) or liposomal amphotericin B; remove the central line; daily blood cultures to clearance; minimum two weeks of therapy after the first negative culture; fundoscopy for retinal seeding.
Invasive aspergillosis: voriconazole first-line (with liposomal amphotericin B as an alternative); mucormycosis: high-dose liposomal amphotericin B plus urgent surgical debridement; reverse immunosuppression; therapeutic drug monitoring for voriconazole, posaconazole and itraconazole.
Prophylaxis for the at-risk host: fluconazole or caspofungin in AML induction and prolonged neutropenia; posaconazole in graft-versus-host disease; trimethoprim-sulfamethoxazole for Pneumocystis from engraftment to immune reconstitution.
For tinea capitis, the management is oral, because topical therapy fails to reach the fungus in the hair follicle. The traditional first-line is oral griseofulvin for six to eight weeks, but the Fleece meta-analysis found terbinafine at least as effective for Trichophyton species with a shorter course, while griseofulvin remains preferred for Microsporum infections. Selenium or ketoconazole shampoo reduces contagious shedding, and the child is excluded from school until treatment has started. The boggy kerion is an inflammatory variant that needs oral antifungal therapy, not incision and drainage. [8] [12]
For invasive candidiasis and candidaemia, the first-line is an echinocandin (caspofungin or micafungin) or liposomal amphotericin B, with the choice guided by the Fisher comparative-effectiveness data in children. The central line is removed, daily blood cultures are taken until clearance, and a minimum of two weeks of therapy follows the first negative culture, with fundoscopy to detect retinal seeding. For invasive aspergillosis, voriconazole is first-line, with liposomal amphotericin B as an alternative. For mucormycosis, high-dose liposomal amphotericin B and urgent surgical debridement are the bundle, because the infarcted, avascular tissue cannot be sterilised by drugs alone. [2] [7]
Specific Subtypes & Scenarios
An infant with oral thrush. White adherent plaques on the buccal mucosa and tongue, with an erythematous base, in an otherwise well baby under a year of age. Treat with oral nystatin suspension or miconazole oral gel, treat the mother's nipples if she breastfeeds, and investigate thrush outside infancy for immunocompromise or inhaled-steroid technique. Most infants clear with topical therapy; refractory disease warrants oral fluconazole and an immune-status review. [12] [11]
A school-age child with tinea capitis. Scaling and hair loss with black-dot broken hairs and occipital lymphadenopathy, or a boggy, tender, purulent kerion. Treat with oral griseofulvin for six to eight weeks or weight-based terbinafine, add a selenium or ketoconazole shampoo, and exclude from school until treatment has started. The kerion is an inflammatory variant that needs oral antifungal therapy — never incision and drainage — and a short course of oral steroids is sometimes added for severe inflammation. [8] [12]
A neutropenic oncology child with persistent fever. Fever beyond four to seven days on broad-spectrum antibiotics in a child with profound neutropenia and a central line. Add empirical antifungal therapy — an echinocandin or liposomal amphotericin B — image the chest and sinuses, send galactomannan and beta-D-glucan, and review the differential for persistent fever. The early empirical cover is the safeguard against the missed invasive candidiasis or aspergillosis. [1] [14]
A transplant or HIV-exposed infant with hypoxaemic pneumonia. Subacute dyspnoea, dry cough, tachypnoea and hypoxaemia out of proportion to the chest X-ray. This is Pneumocystis jirovecii pneumonia. Start high-dose intravenous trimethoprim-sulfamethoxazole and adjunctive steroids for hypoxaemia, confirm with bronchoalveolar lavage where feasible, and arrange prophylaxis (trimethoprim-sulfamethoxazole) from immune-deficiency to immune reconstitution. [9] [10]
A diabetic or neutropenic child with facial and palatal pain and a black necrotic eschar. This is rhino-orbito-cerebral mucormycosis, a surgical and medical emergency. Obtain urgent imaging of the sinuses and orbit, start high-dose liposomal amphotericin B, and arrange aggressive surgical debridement of necrotic tissue. Reverse the metabolic defect — control diabetic ketoacidosis, reduce immunosuppression where possible — because medical therapy alone cannot sterilise infarcted tissue. [7] [6]
A very-low-birth-weight neonate with line-related sepsis. Temperature instability, apnoea and feeding intolerance in an extremely preterm infant with a central line and parenteral nutrition. This is invasive neonatal candidiasis. Remove the central line, give systemic amphotericin B (with flucytosine for central nervous system disease), examine the retina and the central nervous system, and address the line, parenteral nutrition and antibiotic exposures that drove the infection. [4] [5]
Complications & Pitfalls
Candidaemia seeds distant sites that declare themselves if they are not sought. Retinal seeding threatens vision, endocarditis seeds the valve, central nervous system disease seeds the meninges, and hepatosplenic candidiasis appears as neutrophils recover. The recurring pitfall is treating the positive blood culture and forgetting the seeded sites — fundoscopy is part of the candidaemia workup, and a persistently febrile child after bloodstream clearance may have hepatosplenic disease declaring itself as the neutrophils return. [2] [3]
Invasive aspergillosis and mucormycosis carry the heaviest morbidity. Pulmonary infarction and catastrophic haemoptysis, tissue loss and disfigurement from mucormycosis, and death in untreated disease are the serious complications. The outcome is decided by the speed of diagnosis, the adequacy of surgical debridement for mucormycosis, and the reversal of immunosuppression — because the antifungal cannot sterilise infarcted, avascular tissue, and the mould will relapse if the host defence is not restored. [6] [7]
The tinea-incognito error is the recurring cutaneous pitfall. Treating an undiagnosed annular plaque with a topical steroid abolishes the scale and the itch, masks the diagnosis, and lets the dermatophyte spread. The safeguard is to confirm tinea with a skin scraping for hyphae before prescribing a steroid, and to recognise that an annular plaque that "improved" on steroid but relapsed is tinea until proven otherwise. The kerion, similarly, must not be incised — it is an inflammatory fungal mass that needs oral antifungal therapy. [8] [12]
The drug-interaction and toxicity errors are the iatrogenic pitfalls. Voriconazole and posaconazole interact with calcineurin inhibitors and chemotherapy, requiring level monitoring and dose adjustment. Amphotericin B is nephrotoxic and wastes potassium and magnesium, demanding electrolyte and renal-function surveillance. Flucytosine is myelosuppressive and needs level and count monitoring. The candidate who names these — and the therapeutic drug monitoring that governs voriconazole, posaconazole, itraconazole and flucytosine — avoids the avoidable harms. [14] [13]
The recurring pitfall across all invasive fungal disease is delay. Delay in adding empirical antifungal therapy for persistent febrile neutropenia, delay in imaging the chest and sinuses, delay in removing the central line, and delay in surgical debridement for mucormycosis are each avoidable sources of harm. Host-tier recognition at the first encounter — setting the threshold to treat empirically in the immunocompromised host — is the safeguard. The well-child topical default applied to these hosts is the dangerous error the fellowship examiner probes. [7] [1]
Prognosis & Disposition
Superficial fungal infection in the immunocompetent child resolves fully with appropriate topical or oral therapy, with recurrence driven by ongoing risk — napkin wear, inhaled-steroid technique, untreated household contacts in tinea, and unrecognised immunocompromise in persistent thrush. The disposition is outpatient, with a clear safety-net for spread, recurrence or non-response, and the recognition that thrush outside infancy is a flag worth investigating. [12] [11]
The mortality and morbidity of invasive fungal disease are concentrated in the high-risk hosts. Invasive candidiasis mortality in children remains substantial and is highest in the very-low-birth-weight neonate, the neutropenic oncology patient and the stem-cell transplant recipient; early echinocandin therapy and line removal improve the outcome. Invasive aspergillosis and mucormycosis carry the highest mortality of all, decided by the speed of diagnosis, the adequacy of debridement and the reversal of immunosuppression. Pneumocystis mortality falls sharply with early steroids and trimethoprim-sulfamethoxazole. [2] [7]
Disposition follows the depth and the host. Manage at home, with topical or oral therapy and a safety-net, the well child with superficial disease. Admit to the ward the child needing intravenous therapy for invasive candidiasis or oral-therapy monitoring for extensive tinea. Admit to the paediatric intensive care unit the child with invasive fungal sepsis, respiratory failure from Pneumocystis, or the surgical emergency of mucormycosis. The threshold for admitting an immunocompromised or deteriorating host is deliberately low. [4] [14]
At discharge, complete the antifungal course and the secondary prophylaxis while immunosuppression persists — fluconazole, posaconazole, voriconazole or trimethoprim-sulfamethoxazole as the host demands. Arrange fundoscopy and imaging follow-up for seeded disease, and therapeutic drug monitoring for the azoles and flucytosine. Give the family a clear safety-net for new fever, recurrence, or any deterioration. The discharge encounter is also a prevention opportunity: address line-care, antibiotic stewardship, prophylaxis adherence, and the underlying immunosuppression that drove the disease. [13] [5]
Special Populations
Neonates, especially very-low-birth-weight infants, are the highest-risk group for invasive candidiasis. The disease is overwhelmingly line-related, and the extremely preterm infant with parenteral nutrition, broad-spectrum antibiotics and a central vascular line is the prototypical host. Treat by removing the central line and giving systemic amphotericin B (with flucytosine for central nervous system disease), and prevent by meticulous line-care bundles, reducing parenteral nutrition, and limiting broad-spectrum antibiotic exposure. [4] [5]
Children with oncology disease and stem-cell transplant are at the highest risk of invasive candidiasis and mould disease. Prophylaxis is the durable prevention — fluconazole or caspofungin in acute myeloid leukaemia induction (as the Fisher JAMA trial established), posaconazole in graft-versus-host disease — alongside a low threshold for empirical therapy in febrile neutropenia. Reversal of immunosuppression, where it can be achieved, is the partner of every antifungal prescription. [1] [13]
Children with HIV and a low CD4 count are at risk of Pneumocystis pneumonia (the AIDS-defining illness of infancy), oesophageal candidiasis and cryptococcal meningitis. Trimethoprim-sulfamethoxazole prophylaxis and antiretroviral therapy are the durable prevention, and the combination has transformed the prognosis of these once-lethal opportunistic infections. Oesophageal candidiasis in the HIV-positive child is an indication for systemic fluconazole, not topical therapy. [9] [10]
Children with chronic mucocutaneous candidiasis or a primary immunodeficiency — the STAT1, DOCK8 and CARD9 defects — present with recurrent and recalcitrant mucocutaneous fungal disease that resists topical therapy and recurs after oral courses. This is the child whose "minor" fungal infection is the first clue to an underlying immune defect, and the correct response is immunology assessment alongside the antifungal therapy, not a repeated cycle of topical agents. [11] [12]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children, and refugee, asylum-seeking and migrant families may face barriers to timely diagnosis and treatment of both superficial and invasive fungal disease. Ensure culturally safe, equitable access to diagnostics, antifungals and follow-up, treat actively when disease is suspected, and use trained interpreters rather than family members. Disadvantage should never be the reason an invasive fungal diagnosis is delayed or a prophylaxis pathway is missed. [4] [5]
Rural and remote children need timely access to imaging, biomarker testing, antifungals and retrieval for invasive disease. The plan accounts for what is locally available — a remote hospital may not run a galactomannan or hold liposomal amphotericin B in stock — and retrieval is mobilised early when an immunocompromised host deteriorates, because distance can delay the care that a sick neutropenic child cannot afford to wait for. [14] [1]
Evidence, Guidelines & Regional Differences
The contemporary paediatric prophylaxis evidence is the Fisher et al. JAMA 2019 randomised trial, which showed that caspofungin prophylaxis reduced invasive fungal disease compared with fluconazole in children and young adults with acute myeloid leukaemia. It is the study that underpins the modern move from fluconazole toward echinocandin prophylaxis in the highest-risk induction, and the candidate should be able to state its population, finding and implication. [1]
The echinocandin-first therapy and non-culture diagnostics for invasive paediatric candidiasis rest on the Fisher et al. comparative-effectiveness study (JPIDS 2021) and the Fisher et al. multicentre biomarker study (Clin Infect Dis 2022). Together they frame the echinocandin as the preferred initial directed therapy for invasive candidiasis in children, and the beta-D-glucan and related biomarkers as adjuncts to blood culture in the diagnosis. [2] [3]
Caspofungin versus fluconazole prophylaxis in paediatric AML
Population: Randomised trial of children and young adults with newly diagnosed acute myeloid leukaemia, assigned to caspofungin versus fluconazole prophylaxis during induction chemotherapy, with invasive fungal disease as the primary outcome.
Key finding
Caspofungin prophylaxis resulted in a lower rate of invasive fungal disease than fluconazole during induction. Both agents were tolerable, with the expected echinocandin and azole safety profiles.
Practice change
Echinocandin prophylaxis is a credible, evidence-based option for the highest-risk paediatric induction, shifting practice beyond fluconazole alone. The choice of prophylaxis agent balances efficacy, toxicity, mould coverage and local epidemiology.
The neonatal invasive candidiasis evidence is the Kilpatrick et al. Lancet Child and Adolescent Health 2022 review and the Kaufman and Mukhopadhyay Clin Perinatol 2025 review, which together frame the line-related epidemiology, the amphotericin-B-based therapy, the role of flucytosine in central nervous system disease, and the prevention bundle of line-care, parenteral-nutrition minimisation and antibiotic stewardship. The invasive-aspergillosis-in-children evidence is the Warris et al. ESCMID-ECMM 2019 guideline. [4] [6]
The mould-disease guidelines are the Cornely et al. global mucormycosis guideline (Lancet Infect Dis 2019) and the Tissot et al. ECIL-6 guidelines for the treatment of invasive candidiasis, aspergillosis and mucormycosis in leukaemia and transplant patients (Haematologica 2017). They set the high-dose liposomal amphotericin B and surgical debridement bundle for mucormycosis, the voriconazole-first stance for aspergillosis, and the empirical therapy framework for the persistent febrile neutropenic patient. [7] [14]
The superficial-disease evidence is the Fleece et al. Pediatrics 2004 meta-analysis and the Leung et al. 2020 review for tinea capitis therapy (griseofulvin versus terbinafine, by species), the Stern et al. Cochrane review for Pneumocystis prophylaxis, and the Perfect et al. IDSA 2010 guideline and the Gifford et al. 2024 paper for paediatric cryptococcosis. The Takpradit et al. 2021 study frames posaconazole versus fluconazole prophylaxis in neutropenic children after stem-cell transplant. [8] [13]
The controversies are real and active: empirical versus pre-emptive (biomarker-driven) antifungal therapy in febrile neutropenia, weighed against cost, toxicity and resistance; the duration of therapy after candidaemia; the role of universal versus targeted antifungal prophylaxis; echinocandin versus amphotericin as first-line for paediatric invasive candidiasis; and the optimal mould-active prophylaxis in graft-versus-host disease. The defence against each is the same: a host-tier-first judgement, a low threshold to treat the immunocompromised host, and the recognition that the cost of a missed or delayed invasive fungal disease is measured in lives. [14] [1]
Exam Pearls
- The host-risk tier is the key determinant — a superficial yeast in a well child is topical therapy; the same organism in a neutropenic child with a central line is candidaemia and an echinocandin. [2]
- Neutrophils kill Candida and Aspergillus hyphae (neutropenia risk); T-cells control Pneumocystis and the dimorphic fungi (HIV and transplant risk); macrophages contain inhaled mould spores. [14]
- Persistent febrile neutropenia beyond 4 to 7 days on broad-spectrum antibiotics is the trigger to add empirical antifungal therapy (an echinocandin or liposomal amphotericin B) and to image the chest and sinuses. [1]
- Invasive candidiasis first-line in children is an echinocandin (caspofungin, micafungin) or liposomal amphotericin B, with central-line removal, daily cultures to clearance, a minimum two weeks after the first negative culture, and fundoscopy. [2]
- Voriconazole is first-line for invasive aspergillosis; high-dose liposomal amphotericin B plus urgent surgical debridement is the mucormycosis bundle; reverse immunosuppression. [6] [7]
- Pneumocystis pneumonia: hypoxaemia out of proportion to the chest X-ray in the HIV-exposed infant or immunosuppressed child; high-dose intravenous trimethoprim-sulfamethoxazole for 21 days, with adjunctive steroids for hypoxaemia (PaO2 below ~70 mmHg). [9]
- Tinea capitis needs oral therapy (griseofulvin for 6 to 8 weeks or weight-based terbinafine) — topical therapy fails because the hair follicle is infected; the boggy kerion needs oral antifungal, not incision. [8] [12]
- The halo sign on CT is early invasive aspergillosis; the necrotic palatal or nasal eschar is mucormycosis; the reversed-halo sign favours mucormycosis over aspergillosis. [6] [7]
- CSF cryptococcal antigen (often with a very low cell count) in the immunocompromised host is characteristic of cryptococcal meningitis; treat with amphotericin B plus flucytosine induction, then fluconazole consolidation. [10] [11]
- Amphotericin B is nephrotoxic (monitor electrolytes and renal function); voriconazole, posaconazole, itraconazole and flucytosine need therapeutic drug monitoring — variable paediatric pharmacokinetics and interactions with chemo and transplant drugs. [14] [13]
References
- [1]Fisher BT; Zaoutis T; Dvorak CC; et al Effect of Caspofungin vs Fluconazole Prophylaxis on Invasive Fungal Disease Among Children and Young Adults With Acute Myeloid Leukemia. JAMA, 2019.PMID 31688884
- [2]Fisher BT; Zaoutis TE; Xiao R; et al Comparative Effectiveness of Echinocandins vs Triazoles or Amphotericin B Formulations as Initial Directed Therapy for Invasive Candidiasis in Children. J Pediatric Infect Dis Soc, 2021.PMID 34374424
- [3]Fisher BT; Boge CLK; Xiao R; et al Multicenter Prospective Study of Biomarkers for Diagnosis of Invasive Candidiasis in Children and Adolescents. Clin Infect Dis, 2022.PMID 35134165
- [4]Kilpatrick R; Scarrow E; Hornik C; et al Neonatal invasive candidiasis: updates on clinical management and prevention. Lancet Child Adolesc Health, 2022.PMID 34672994
- [5]Kaufman DA; Mukhopadhyay S Neonatal Invasive Fungal Infections: Epidemiology, Microbiology, and Controversies in Practice. Clin Perinatol, 2025.PMID 39892954
- [6]Warris A; Lehrnbecher T; Roilides E; et al ESCMID-ECMM guideline: diagnosis and management of invasive aspergillosis in neonates and children. Clin Microbiol Infect, 2019.PMID 31158517
- [7]Cornely OA; Alastruey-Izquierdo A; Arenz D; et al Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis, 2019.PMID 31699664
- [8]Fleece D; Gaughan JP; Aronoff SC Griseofulvin versus terbinafine in the treatment of tinea capitis: a meta-analysis of randomized, clinical trials. Pediatrics, 2004.PMID 15520113
- [9]Stern A; Green H; Paul M; et al Prophylaxis for Pneumocystis pneumonia (PCP) in non-HIV immunocompromised patients. Cochrane Database Syst Rev, 2014.PMID 25269391
- [10]Perfect JR; Dismukes WE; Dromer F; et al Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the Infectious Diseases Society of America. Clin Infect Dis, 2010.PMID 20047480
- [11]Gifford A; Jayawardena N; Carlesse F; et al Pediatric Cryptococcosis. Pediatr Infect Dis J, 2024.PMID 38241632
- [12]Leung AKC; Hon KL; Leong KF; et al Tinea Capitis: An Updated Review. Recent Pat Inflamm Allergy Drug Discov, 2020.PMID 31906842
- [13]Takpradit C; Wangkittikal C; Rungmaitree S; et al Antifungal Prophylaxis with Posaconazole versus Fluconazole in Children with Neutropenia Following Allogeneic Hematopoietic Stem Cell Transplantation. J Blood Med, 2021.PMID 34354383
- [14]Tissot F; Agrawal S; Pagano L; et al ECIL-6 guidelines for the treatment of invasive candidiasis, aspergillosis and mucormycosis in leukemia and hematopoietic stem cell transplant patients. Haematologica, 2017.PMID 28011902