Paeds · infectious-diseases
Hand-foot-and-mouth disease and enterovirus infection
Also known as Hand-foot-and-mouth disease (HFMD) · Enterovirus 71 infection · EV71 brainstem encephalitis · Coxsackievirus A6 atypical HFMD · Eczema coxsackium · Enteroviral vesicular stomatitis with exanthem
Fellowship topic on hand-foot-and-mouth disease (HFMD) and enterovirus infection in children: the causative enteroviruses (coxsackievirus A16, enterovirus 71 and the atypical coxsackievirus A6) and their faecal-oral, droplet and vesicle-fluid transmission; the classic vesicular oral-and-acral picture; the atypical CVA6 phenotype with onychomadesis; and the feared EV71 neurological spectrum from aseptic meningitis through brainstem encephalitis to neurogenic pulmonary oedema and death; the differential of oral ulcers and vesicular rashes; PCR and serology interpreted by sample type and duration; stepwise management from outpatient analgesia and hydration through PICU care with fluid restriction and milrinone for EV71 cardiopulmonary failure, the weak-evidence role of IVIG, and the absence of any proven antiviral; childcare exclusion, outbreak notification and household hygiene; the inactivated EV71 vaccines licensed in China and the WHO SAGE 2016 position; special populations (infants, immunocompromised, Asia-Pacific and migrant communities, rural and remote children); and ANZ/UK/US/Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
EV71 escalation — the signs that change everything
Overview & Definition
Picture a two-year-old brought to the general practice with two days of fever, drooling and refusing to eat. On examination there are shallow grey ulcers on the tongue and buccal mucosa, and a handful of oval vesicles on the palms, the soles and around the buttocks. The child is miserable but alert and well hydrated. This is textbook hand-foot-and-mouth disease, and the task is to recognise it, manage the discomfort, advise the family on infectivity — and stay alert for the small minority in whom the same rash heralds a life-threatening neurological illness. [2] [8]
Hand-foot-and-mouth disease is an acute, self-limiting enterovirus infection whose hallmark is a vesicular enanthem in the mouth paired with a vesicular exanthem on the hands, feet and around the buttocks. It is caused by non-polio enteroviruses, most often coxsackievirus A16 and enterovirus 71, and increasingly by coxsackievirus A6. The illness spreads readily among young children in childcare through saliva, vesicle fluid and the faecal-oral route, which is why it sweeps through kindergartens each season. [1] [2]
The clinician's job has two halves that rarely overlap. The common half is reassurance and symptomatic care for the child with the classic rash. The dangerous half is recognising enterovirus 71 disease, in which the identical rash is the portal to a brainstem encephalitis that can progress to autonomic dysregulation, neurogenic pulmonary oedema and death within hours. Holding both halves in mind at once — ordinary and lethal — is the core skill this topic asks of you. [2] [9]
Classification
Sort HFMD the way it matters at the bedside: by the causative virus, by the clinical phenotype, and — for enterovirus 71 — by the grade of neurological severity, because that grade dictates where the child is managed and how urgently. The causative-virus lens matters because coxsackievirus A16, enterovirus 71 and coxsackievirus A6 produce the same rash but very different risks. Coxsackievirus A16 causes the classic, usually mild illness that most families know. Enterovirus 71 shares that rash but is neurotropic and virulent, driving the brainstem encephalitis and pulmonary oedema that dominate mortality. Coxsackievirus A6 produces an atypical, more extensive phenotype that fools clinicians expecting a few palm-and-sole lesions. [1] [8]
The clinical-phenotype lens separates typical HFMD, atypical HFMD and enterovirus neurological disease. Typical HFMD pairs oral ulcers with palm-and-sole vesicles and fever, and resolves over a week. Atypical HFMD — usually coxsackievirus A6 — throws vesicles far beyond the palms and soles onto the trunk, perioral skin and limbs, sometimes overlying eczema ("eczema coxsackium"), and is followed weeks later by nail shedding. Enterovirus neurological disease is the third phenotype, and it is the one that demands escalation. [8] [2]
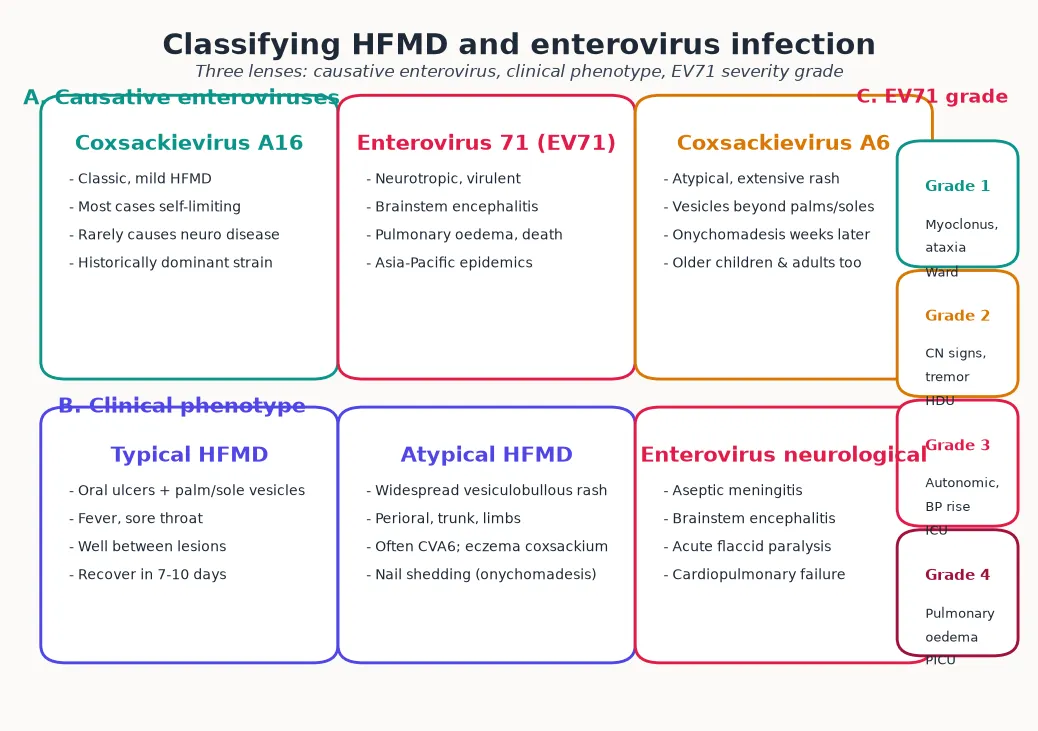
For enterovirus 71 specifically, the Sarawak and Taiwan groups developed a severity grade that maps clinical findings to the level of care needed. Low-grade disease — myoclonus and ataxia — can be observed on the ward. Higher-grade disease adds cranial-nerve signs, autonomic dysfunction with hypertension and tachycardia, and finally pulmonary oedema and cardiopulmonary failure, each step moving the child toward the intensive-care unit. Knowing this grade by heart is what lets you triage the child with the rash and the tremor before the deterioration begins. [2] [5]
Epidemiology & Risk Factors
Where does HFMD sit, and who does it hurt? The disease is worldwide, but it is in the Asia-Pacific region that enterovirus 71 has shown its full lethal potential. The 1998 Taiwan outbreak, in which EV71 caused hundreds of cases of brainstem encephalitis and pulmonary oedema in young children, defined the modern understanding of this virus, and large recurrent epidemics across mainland China, Vietnam, Cambodia, Malaysia and Singapore have followed. In temperate climates HFMD peaks in summer and early autumn; in the tropics it circulates year-round with rainy-season amplification. [1] [8]
Age is the dominant risk factor. The burden falls on children under five, and especially on those under two, because they have had little prior exposure and because their close-contact behaviours — mouthing toys, sharing saliva, toileting accidents — maximise transmission. Childcare and preschool attendance multiply exposure, and household spread to siblings and parents is the rule rather than the exception during an outbreak. The disease is so contagious that a single case often seeds a classroom. [2] [5]
For the dangerous end of the spectrum, the risk factors narrow to enterovirus 71 itself, young age and virulent viral genotypes. The Sarawak predictors study identified clinical features that flag a child with HFMD at higher risk of neurological involvement, including fever duration, lethargy and a history compatible with EV71 circulation — findings that justify a lower threshold for admission and observation during an EV71 season. Host factors such as immature immunity and small physiological reserve convert the same viral injury into life-threatening disease in the youngest children. [5] [2]
Pathophysiology
Why does a virus that gives most children a rash sometimes kill within a day? The answer lies in which enterovirus is involved and where it travels in the body. The non-polio enteroviruses are small, non-enveloped RNA viruses that enter through the faecal-oral route, respiratory droplets and direct contact with vesicle fluid. They first replicate in the gastrointestinal and upper-respiratory epithelium and the associated lymphoid tissue, then seed the skin and mucosa through a short viraemia to produce the characteristic vesicles. [9] [1]
For coxsackievirus A16 and A6, the story largely ends at the skin and mucosa, which is why these strains cause a self-limiting vesicular illness. The vesicles form as viral replication destroys basal epithelial cells, producing an intra-epidermal blister filled with fluid rich in infectious virus — a detail that explains both the high transmissibility from contact with lesions and the value of vesicle fluid for PCR diagnosis. CVA6's tendency to erupt over inflamed eczema and to involve more skin accounts for its atypical, extensive phenotype. [8] [2]
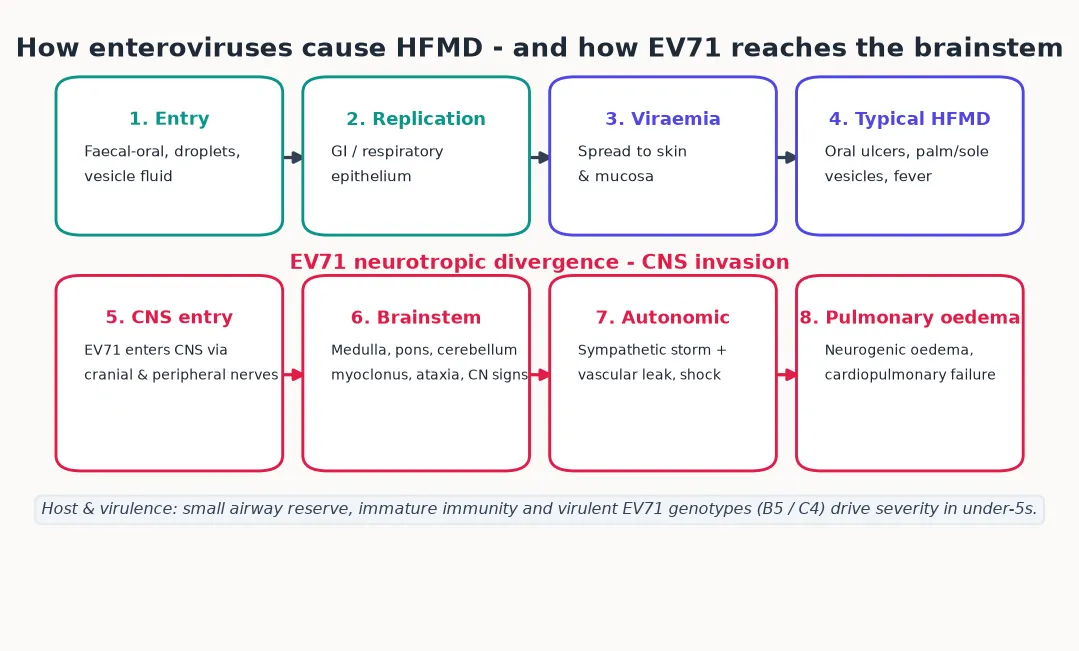
Enterovirus 71 diverges because it is neurotropic. After the same gut and respiratory replication, EV71 can enter the central nervous system, travelling along cranial and peripheral nerve pathways to reach the brainstem, particularly the medulla, pons and cerebellum. This neural spread, rather than bloodstream entry alone, explains why the worst disease targets the brainstem control centres for respiration, autonomic tone and motor function — producing myoclonus, ataxia, cranial-nerve palsies and acute flaccid weakness. [9] [1]
The terminal pathophysiology is the autonomic storm. EV71 injury to the medullary centres triggers sympathetic overdrive, hypertension and vascular leak, which together flood the lungs with protein-rich fluid — neurogenic pulmonary oedema. The result is a child who was playing one day and in cardiopulmonary failure the next. Markers of this catastrophic turn include the inflammatory and cardiac predictors described in EV71 cohorts, and an elevated N-terminal pro-B-type natriuretic peptide has been shown to predict severe EV71 disease, reflecting the cardiac strain that accompanies autonomic dysregulation. [7] [10]
Clinical Presentation
The classic presentation is unmistakable once you have seen it. After a three-to-seven-day incubation and a short prodrome of fever and sore throat, the child develops painful oral ulcers on the tongue, palate and buccal mucosa alongside vesicles on the palms, soles, around the buttocks and on the knees and elbows. The oral lesions are what bring most children to care, because they hurt enough to stop a toddler feeding. The child is often febrile and miserable but systemically well, and the rash evolves over several days before crusting and fading over a week to ten days. [2] [8]
The atypical coxsackievirus A6 presentation breaks the textbook rules and is the one clinicians increasingly meet. Instead of a few discrete palm-and-sole vesicles, the child develops widespread vesicles and bullae over the trunk, perioral skin, proximal limbs and even the scalp, often concentrated over areas of pre-existing eczema. Lesions may be large and bullous rather than tiny, and fever is often higher and more prolonged. The clue to CVA6 rather than classic HFMD is the extent and distribution of the rash, and a characteristic late feature — shedding of the nails (onychomadesis) weeks after the rash has resolved — often brings the family back and confirms the retrospective diagnosis. [8] [2]
The dangerous presentation is enterovirus 71 neurological disease, and it usually emerges two to five days into what looks like ordinary HFMD. The earliest and most specific sign is myoclonus — brief jerks, often of the limbs, that frequently occur during sleep. This may be joined by ataxia, tremor, cranial-nerve palsies such as squint or facial weakness, and acute flaccid limb weakness. A child with HFMD who suddenly becomes ataxic, starts jerking, or cannot bear weight must be treated as having EV71 brainstem or spinal-cord disease until proven otherwise. [2] [5]
The pre-terminal presentation is autonomic and cardiopulmonary. Tachycardia, hypertension, cold peripheries, poor perfusion and irritability signal the autonomic dysregulation that precedes collapse, and tachypnoea, desaturation and frothy secretions signal the neurogenic pulmonary oedema itself. The interval between a tremor and a respiratory arrest can be measured in hours, so the neurological and autonomic signs are not curiosities to chart — they are triggers to move the child to intensive care. [7] [2]
Differential Diagnosis
For the child with oral ulcers, the differential turns on whether the palms and soles are involved. Herpangina — also enteroviral, typically coxsackievirus A — confines its ulcers to the posterior mouth and soft palate and spares the extremities, which is the key distinction from HFMD. Primary herpes simplex gingivostomatitis produces more widespread, painful oral disease with marked gum involvement and high fever, but it lacks the acral vesicular rash of HFMD and tends to affect younger infants. Aphthous stomatitis recurs in the same child, has no fever and no palm-and-sole lesions. [2] [8]
For the child with a vesicular rash, varicella is the principal mimic, but chickenpox lesions appear in crops across the trunk and face at different stages simultaneously and are far more centrally distributed than the acral-and-buttock pattern of HFMD. Impetigo and scabies produce papules and crusted lesions rather than the oval grey vesicles of HFMD. The atypical CVA6 phenotype with widespread bullae can resemble Stevens-Johnson syndrome or erythema multiforme, but CVA6 lacks the target lesions and mucosal destruction of those diagnoses — a distinction that matters because Stevens-Johnson needs urgent immune intervention while HFMD does not. [8] [2]
For the child who presents with acute neurological signs and a vesicular rash, the differential is the dangerous one, and EV71 brainstem encephalitis sits squarely within it. Other enteroviruses cause aseptic meningitis, Japanese encephalitis and other arboviruses cause encephalitis in endemic regions, and acute flaccid paralysis raises polio, Guillain-Barré and transverse myelitis. The coexistence of the HFMD rash with brainstem or myelitic signs in a young child during an outbreak strongly favours EV71, and the point is to escalate for that diagnosis rather than attribute the weakness to a self-limiting virus. [2] [9]
Clinical & Bedside Assessment
The assessment begins with the history of the illness and its setting. Ask about the onset and progression of fever, oral pain and rash, the child's feeding and urine output, and whether there has been any unusual movement — the sleep myoclonus of EV71 is easily missed unless you ask directly. Ask about childcare attendance and whether classmates or siblings have a similar illness, because the epidemiological setting often makes the diagnosis. Document the interval since rash onset, because EV71 neurological disease typically declares itself in the first few days. [2] [5]
Examine with two questions in mind: how well hydrated is the child, and are there any neurological or autonomic signs? Assess feeding tolerance, urine output, mucous membranes and capillary refill for dehydration. Inspect the mouth, palms, soles, buttocks and knees, and — for suspected CVA6 — look beyond the classic sites to the trunk, scalp and nail folds. Then perform a focused neurological examination: look for myoclonus, ataxia on walking if age allows, tremor, squint or facial weakness, and test limb tone, power and reflexes for acute flaccid weakness. [5] [2]
Score the red flags that change disposition. Myoclonus, ataxia, tremor, limb weakness, cranial-nerve signs, marked lethargy or irritability are neurological red flags that mandate admission and observation. Tachycardia, hypertension, poor perfusion, cold extremities, tachypnoea or desaturation are autonomic and cardiopulmonary red flags that mandate PICU referral without delay. A well child with classic HFMD and good hydration can be managed at home; any red flag moves the child up the acuity ladder. [7] [2]
Document the public-health essentials at the bedside. Record the date of rash onset, childcare or school attendance, and the household contacts, because these details drive exclusion advice, outbreak notification and the family's understanding of infectivity. A clear contact and exclusion record at the first encounter prevents the confused return-to-childcare conversation a week later, and it equips public health to track the dominant serotype through the season. [1] [8]
Investigations
Most HFMD is a clinical diagnosis, and laboratory confirmation changes little for the well child managed at home. Testing becomes important when the picture is atypical, when neurological complications are present or suspected, or when an outbreak demands serotype surveillance to distinguish a benign coxsackievirus A16 season from a dangerous enterovirus 71 one. The choice of test depends on what question you are asking and how far into the illness the child is. [6] [2]
PCR is the workhorse, and the sample matters. The evaluation of different clinical sample types in EV71-associated HFMD showed that vesicle fluid, throat swabs and stool all carry detectable virus, with vesicle fluid offering high sensitivity while lesions are present, throat swabs capturing early replication, and stool remaining positive for weeks because enteroviruses are shed through the gut. For a child with a typical rash, vesicle or throat PCR confirms an enterovirus; during an outbreak, public-health laboratories subtype to identify EV71. [6] [1]
In Australia and Aotearoa New Zealand, HFMD itself is not a nationally notifiable disease, but outbreaks — especially in childcare and aged-care-adjacent settings — are reported to public-health units. Enterovirus PCR is available through reference laboratories for atypical or severe cases, and EV71 subtyping is coordinated at the state or national level to track whether a season is dominated by benign coxsackieviruses or by EV71. The Australian Department of Health and equivalent New Zealand guidance frame childcare exclusion and infection control. [1]
For the child with neurological signs, the investigation escalates. Lumbar puncture typically shows an aseptic-meningitis picture of lymphocytic pleocytosis; cerebrospinal fluid PCR may detect EV71, though sensitivity is lower than from throat or stool. Magnetic resonance imaging of the brain and spine can demonstrate the characteristic brainstem signal change of EV71 encephalitis and the anterior-horn-cell lesion of the myelitic form. These investigations are part of confirming and grading EV71 disease in a child who has already been moved to a higher level of care. [2] [9]
Prognostic biomarkers refine severity prediction in EV71 disease. Studies of children with EV71 encephalitis and cardio-respiratory compromise identified elevated interleukin-1β and related cytokines as markers of poor prognosis, and an elevated N-terminal pro-B-type natriuretic peptide predicts severe EV71-associated HFMD by reflecting the cardiac strain of autonomic dysregulation. These markers do not replace bedside red-flag recognition, but they help the intensive-care team anticipate deterioration. [7] [10]
Management — Resuscitation
Resuscitation is about the child who is deteriorating from enterovirus 71 neurological disease. The triggers are the red flags already named: myoclonus, ataxia, weakness, autonomic instability or any respiratory compromise. A child with any of these in the setting of HFMD belongs in a monitored bed, and any sign of autonomic dysfunction or pulmonary oedema belongs in the paediatric intensive care unit, because the window between tremor and arrest can be brief. The decision to escalate should be deliberately low-threshold during an EV71 season. [2] [7]
Airway and breathing support come first. Give supplemental oxygen for desaturation, secure the airway early when pulmonary oedema is developing rather than waiting for respiratory failure, and use lung-protective ventilation. Neurogenic pulmonary oedema is managed with positive-pressure ventilation, careful fluid balance and the respiratory-support strategies used for any cause of acute lung injury, and extracorporeal membrane oxygenation has been used in refractory cardiopulmonary failure in centres that can deliver it. [2] [8]
The haemodynamic management of EV71 autonomic dysregulation is specific and counter-intuitive. Because the pathophysiology is sympathetic overdrive with vascular leak, the instinct to bolus fluid can worsen pulmonary oedema, so care is built around judicious fluid restriction and vasoactive support. Milrinone, a phosphodiesterase inhibitor that reduces the sympathetic surge and supports cardiac output, has become a favoured agent in EV71 brainstem disease with autonomic dysfunction, reflecting the understanding that the cardiac and vascular failure is driven from the brainstem rather than by primary pump failure. [7] [2]
There is no proven antiviral for enterovirus 71, and IVIG is used empirically in severe EV71 disease on the basis of neutralising-antibody and immunomodulatory effects rather than strong trial evidence. The honest framing for families and for examiners is that definitive therapy for severe EV71 disease is meticulous intensive-care support aimed at the brainstem-driven autonomic and respiratory failure, while the search for a specific antiviral continues. Recognising complications such as secondary bacterial infection and treating dehydration completes the resuscitation bundle. [8] [2]
Management — Definitive & Stepwise
Definitive management is a stepwise pathway matched to severity, with outpatient support at one end, ward care for the dehydrated or at-risk child in the middle, and PICU care for EV71 neurological disease at the other. The pathway deliberately over-triages upward during an EV71 season, because the cost of missing early brainstem disease is a preventable death. [2] [8]
The stepwise HFMD pathway
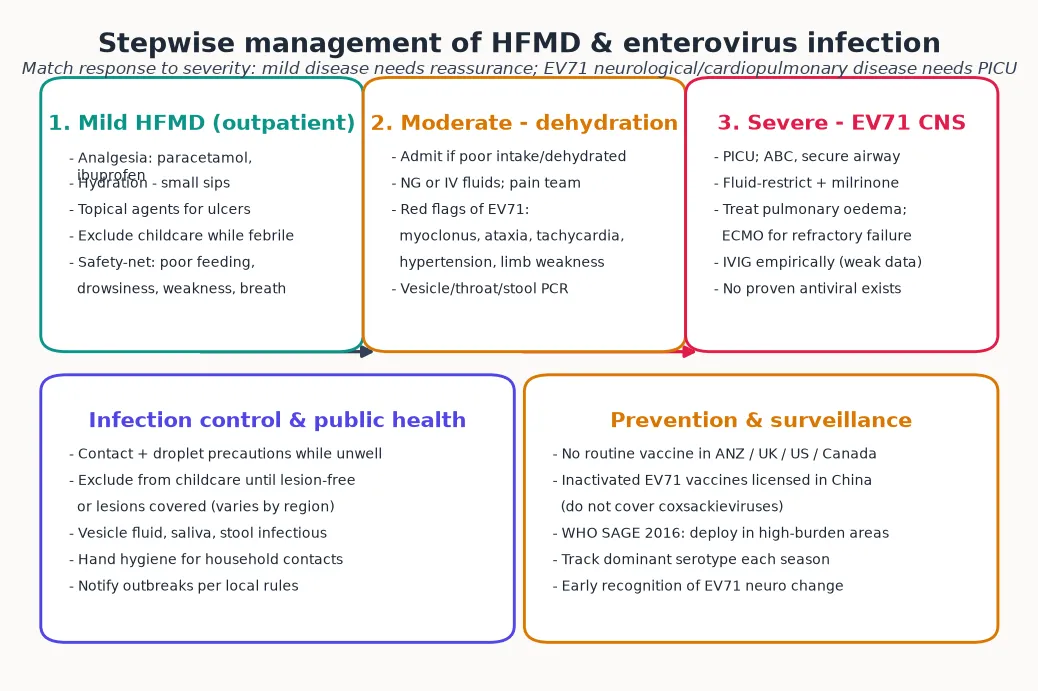
Mild HFMD: analgesia with paracetamol or ibuprofen, encourage fluids as small frequent sips, soft cool foods, topical oral agents for comfort, and exclude from childcare while febrile and until lesions have healed.
Safety-net the family: return immediately for poor feeding or reduced urine output, drowsiness or irritability, weakness, unsteadiness, tremor or breathing difficulty.
Moderate disease — dehydration, persistent fever or any EV71 red flag: admit, give NG or IV fluids, involve the pain team for severe oral pain, and send vesicle/throat/stool PCR with EV71 subtyping.
Neurological or autonomic signs: transfer to PICU, secure the airway, monitor continuously, and arrange CSF and MRI to confirm and grade EV71 disease.
Cardiopulmonary compromise: lung-protective ventilation, judicious fluid restriction, milrinone and vasoactive support, and consider ECMO for refractory failure; IVIG is used empirically.
Infection control: contact and droplet precautions while unwell, childcare exclusion, household hand hygiene, and notify outbreaks to public health to track the dominant serotype.
For the mild case managed at home, the goals are comfort, hydration and containment. Paracetamol and ibuprofen ease fever and oral pain, and soft cool foods and small frequent drinks sustain intake through the few days the mouth is sore. Topical anaesthetic or antacid mouthwashes can help older children. Parents should understand that the child is infectious while lesions are present and through stool shedding for weeks, so hand hygiene and avoidance of sharing utensils matter even after the fever settles. Clear safety-netting is the single most important safety element of the discharge. [2] [1]
For the moderate case, admission is driven by dehydration, persistent fever or any feature that raises EV71 concern. Give nasogastric or intravenous fluids to correct dehydration, involve the pain team when oral pain is the rate-limiting step for feeding, and observe for neurological and automatic signs. Send enterovirus PCR for subtyping, because knowing whether the season's cases are EV71 or coxsackievirus shapes the threshold for admission across the whole service. Most moderate cases recover and are discharged within days. [8] [5]
For the severe case, the pathway is intensive-care as described above, with the addition of multidisciplinary rehabilitation planning for survivors of EV71 neurological disease, who may have persistent motor, bulbar or cognitive sequelae. The evidence base for specific therapies remains thin — there is no licensed antiviral and IVIG rests on weak data — which is exactly why the research effort has turned toward prevention through the inactivated EV71 vaccines. [7] [3]
Specific Subtypes & Scenarios
A toddler with classic HFMD and poor oral intake. This is the bread-and-butter presentation. Confirm the diagnosis clinically, optimise analgesia, encourage fluids, advise soft foods and childcare exclusion, and safety-net for the red flags. Admit only if dehydration cannot be managed at home or if any EV71 sign appears. Most of these children recover fully within ten days without ever needing to come back. [2] [8]
A child with widespread bullous lesions, fever and nail involvement — coxsackievirus A6. Recognise the atypical phenotype: the extent and distribution of the rash, the eczema coxsackium overlay, and the later onychomadesis. Distinguish it from Stevens-Johnson syndrome, which has target lesions and severe mucosal destruction and needs urgent immune therapy. CVA6 HFMD is still self-limiting and managed supportively, though the rash is more extensive and the fever often longer than classic disease. [8] [2]
A febrile child with HFMD who develops sleep myoclonus and ataxia — enterovirus 71 brainstem encephalitis. This is the presentation you must not send home. Admit for observation, arrange confirmatory PCR and imaging, and watch continuously for autonomic signs. Any tachycardia, hypertension or respiratory change moves the child to PICU. The whole point of recognising the early neurological signs is to be in the right place before the autonomic storm begins. [2] [5]
A child with EV71 disease who develops tachypnoea and desaturation — neurogenic pulmonary oedema. This is the pre-terminal event. Secure the airway and ventilate with lung-protective settings, restrict fluids, start milrinone and vasoactive support, and mobilise ECMO capability early in centres that have it. The mortality is high, and survival depends on anticipating the deterioration rather than reacting to it. [7] [2]
A pregnant household or childcare worker contact. HFMD in pregnancy is usually mild for the mother, but the family will be anxious, and the role of the clinician is honest reassurance with careful safety-netting. There is no specific intervention beyond standard hygiene, and no routine vaccine to offer. The more important contact to protect is the young infant in the household, who is the one at risk of severe disease. [1] [8]
An outbreak in a childcare centre. Coordinate with public health, reinforce hand hygiene and surface cleaning, exclude children while they are unwell and shedding, and arrange serotype surveillance to identify whether the outbreak is benign coxsackievirus or dangerous EV71. Outbreak management is where the individual clinical encounter becomes a population-health task, and early serotype identification protects the infants at the edge of the cluster. [1] [6]
Complications & Pitfalls
The defining complications are neurological and cardiopulmonary, and they cluster with enterovirus 71. Aseptic meningitis is the mildest, brainstem encephalitis the most characteristic, and acute flaccid paralysis the spinal-cord manifestation. Neurogenic pulmonary oedema with cardiopulmonary failure is the terminal event and the leading cause of EV71 death, concentrated in children under five. Survivors of severe EV71 neurological disease may be left with motor, bulbar or cognitive deficits that require long-term rehabilitation. [2] [9]
The central diagnostic pitfall is dismissing HFMD as always-trivial. It is, for coxsackievirus strains — but the same rash with enterovirus 71 can kill a toddler within a day. A clinician who reassures every HFMD case equally will miss the brainstem signs at the moment they appear. The defence is to look actively for myoclonus, ataxia and weakness in every HFMD case during an EV71 season, and to treat any such sign as an escalation trigger. [2] [5]
A second pitfall is fluid-bolusing the child with EV71 autonomic dysregulation. Because the failure is sympathetic overdrive with leak, generous fluid resuscitation can worsen pulmonary oedema, and the correct strategy is fluid restriction with milrinone and vasoactive support. Applying the standard sepsis-style bolus reflex to a child whose brainstem is failing is an avoidable error that the EV71 critical-care literature specifically warns against. [7] [2]
A third pitfall is confusing coxsackievirus A6 atypical HFMD with Stevens-Johnson syndrome. Both can present with widespread blistering and mucosal involvement, but Stevens-Johnson needs urgent immune therapy while HFMD is managed supportively, and the misclassification either over-treats or dangerously under-observes. The distribution, the target lesions of erythema multiforme, and the later onychomadesis of CVA6 are the distinguishing features. [8]
The fourth error is neglecting the public-health layer. Failing to exclude an infectious child, to reinforce household hand hygiene, or to notify an outbreak allows ongoing transmission to the infants who will bear the severe end of the disease. The clinical encounter does not end with the individual child; it ends when the household and the childcare cohort have been protected. [1] [6]
The final pitfall is over-promising a therapy. There is no proven antiviral for EV71, and IVIG rests on weak evidence, so families and examiners should be told honestly that definitive care is meticulous intensive support. Promising that a drug will change the course misrepresents the evidence and obscures the fact that early recognition and prevention are what actually save lives. [8] [3]
Prognosis & Disposition
Most children with HFMD recover fully within seven to ten days, and the morbidity is driven by oral pain, feeding disruption and a few missed days of childcare rather than by danger. For this large majority, the disposition is home management with analgesia, hydration, clear safety-netting and a return-to-childcare plan once lesions have healed. [2] [8]
The mortality is concentrated in enterovirus 71 neurological and cardiopulmonary disease, and within that it is concentrated in children under five, most often from neurogenic pulmonary oedema. This is the single most important prognostic fact in HFMD, and it is the reason every prevention and triage strategy is built around early EV71 recognition. The inflammatory and cardiac markers identified in EV71 cohorts — the cytokine profile of poor prognosis and the prognostic value of N-terminal pro-B-type natriuretic peptide — quantify this risk and help intensive-care teams anticipate deterioration. [7] [10]
Disposition follows severity. Manage at home, with safety-netting, the well child with classic HFMD and good hydration. Admit to the ward the dehydrated child or any child with an EV71 red flag needing observation. Take to PICU any child with autonomic dysfunction, pulmonary oedema or cardiopulmonary compromise. The threshold for moving a young child up this ladder during an EV71 season is deliberately low. [2] [8]
At discharge, complete the isolation and exclusion advice, finish the contact and outbreak notification, and give the family a clear safety-net for return — poor feeding, reduced urine output, drowsiness, weakness, unsteadiness or breathing difficulty. Reinforce household hand hygiene, because the child remains infectious through stool shedding for weeks after the rash fades. For survivors of severe EV71 disease, arrange multidisciplinary rehabilitation for any persistent neurological deficit. [1] [2]
Recurrence is possible, because the enterovirus family is large and cross-immunity between serotypes is limited. A child who has had coxsackievirus A16 HFMD can later develop CVA6 or EV71 disease, so a history of HFMD does not rule out a new episode — and does not protect against the EV71 spectrum in a future season. [8] [2]
Special Populations
Infants and children under five carry most of the burden and all of the mortality risk of enterovirus 71. Their immature immunity, small physiological reserve and close-contact behaviours combine to produce both the highest incidence and the most severe disease, and every system of care should be designed to catch their neurological signs early. The threshold to admit and observe an infant with HFMD during an EV71 season is deliberately low. [2] [5]
Immunocompromised children may have more severe or prolonged enterovirus disease and depend on the protection of the people around them, since no routine vaccine is available. A low threshold for investigation, admission and intensive support is the right stance, and meticulous hygiene in the household and the healthcare setting matters more for these children than for others. [8] [2]
Aboriginal and Torres Strait Islander, Maori and Pacific, and other Indigenous children, and refugee, asylum-seeking and migrant families may face barriers to timely care and to the health-literacy needed to recognise danger signs, and many originate from or travel through the Asia-Pacific region where EV71 circulates most intensely. Ensure culturally safe, equitable access to care, provide information in the family's language using trained interpreters, and treat actively when disease is suspected. Disadvantage should never be the reason an EV71 brainstem sign is missed. [1] [8]
Rural and remote children need timely access to assessment and to retrieval when an infant deteriorates, because the EV71 window between tremor and arrest cannot wait for distance. The plan for a remote family accounts for what is available locally, escalates early, and mobilises retrieval at the first autonomic or respiratory sign rather than at collapse. Telehealth can support local assessment but cannot substitute for retrieval when intensive care is needed. [2] [8]
Children in childcare and their household contacts are the population in whom prevention is most active. Childcare exclusion while unwell, surface cleaning and hand hygiene, and household awareness of the red flags are the practical tools, and the goal is to interrupt transmission to the youngest, least-protected members of the cluster. [1] [6]
Evidence, Guidelines & Regional Differences
The modern understanding of enterovirus 71 rests on the Asia-Pacific clinical and laboratory literature. The Solomon et al. review of the virology, epidemiology, pathogenesis and control of EV71, and the Ooi et al. review of its clinical features, diagnosis and management, are the canonical references that frame the disease for a global audience. The Sarawak clinical-predictors study gave clinicians the bedside tools to flag neurological risk, and the cytokine and cardiac-marker studies refined prognostication for the intensive-care team. [1] [2]
The treatment evidence is honest about its limits. No antiviral has proven efficacy against EV71 in rigorous trials, and IVIG is used empirically on the basis of biological plausibility rather than strong outcome data. The Cochrane-style appraisal of the enterovirus treatment landscape — represented by the Abzug overview of the problems in need of treatments — confirms that definitive therapy for severe EV71 disease remains meticulous intensive care, which is exactly why prevention through vaccination has become the priority. [8] [9]
Inactivated EV71 vaccines in healthy children (China)
Population: Two large phase-3 randomised trials of inactivated enterovirus 71 vaccines in healthy infants and young children in China during high-burden EV71 seasons.
Key finding
Both vaccines showed high efficacy against EV71-associated HFMD and, importantly, against EV71-associated neurological disease, with acceptable safety and immunogenicity profiles. Neither vaccine covers coxsackieviruses, so vaccinated children can still develop non-EV71 HFMD.
Practice change
Inactivated EV71 vaccines are a real preventive tool and are licensed in China; WHO SAGE endorses their use in high-burden settings. They are not yet in routine schedules in ANZ, the UK, the US or Canada.
The vaccine evidence is the most important recent development. Two large phase-3 trials published in the New England Journal of Medicine in 2014 — Zhu et al. and Li et al. — demonstrated that inactivated EV71 vaccines protect against EV71-associated HFMD and its neurological complications in Chinese infants and young children. These trials established efficacy and safety, and they reshaped the prevention landscape, though the vaccines are serotype-specific and do not cover coxsackieviruses, so vaccinated children can still develop non-EV71 HFMD. [3] [4]
The regional policy structure is where the global gap is most visible. The WHO position paper on enterovirus 71 vaccines, following the 2016 SAGE review, endorses the use of EV71 vaccines in settings with a significant burden of EV71 disease. In China, inactivated EV71 vaccines are licensed and in use. In ANZ, the UK, the US and Canada, no EV71 vaccine is part of the routine schedule, so prevention rests on hygiene, childcare exclusion, outbreak management and clinician vigilance for the neurological signs. The principle is consistent across regions: recognise EV71 early, support the severe case intensively, and interrupt transmission through basic public-health measures. [1] [8]
The controversies and gaps are real and active: whether EV71 vaccines should be introduced into routine schedules beyond China, whether multivalent enterovirus vaccines covering coxsackieviruses can be developed, the optimal treatment of severe EV71 disease in the absence of a proven antiviral, and the equity of access to care for the Asia-Pacific and migrant communities who bear the burden. The defence against each is the same: high-quality supportive care, early neurological recognition, rigorous outbreak surveillance, and ongoing vaccine development. [4] [2]
Exam Pearls
- HFMD is an enterovirus illness — coxsackievirus A16 (classic, mild), enterovirus 71 (neurotropic, lethal) and coxsackievirus A6 (atypical, extensive with onychomadesis). [1] [8]
- The classic picture is oral ulcers plus palm-and-sole vesicles after a febrile prodrome; most children recover in 7–10 days with supportive care. [2]
- The danger is EV71 brainstem encephalitis: watch for myoclonus, ataxia, tremor, cranial-nerve signs and acute flaccid weakness two to five days into the rash. [2] [5]
- The pre-terminal event is neurogenic pulmonary oedema from brainstem-driven autonomic storm; mortality is high in under-fives. [7]
- Diagnose with PCR of vesicle fluid, throat and stool; CSF PCR and MRI brain/spine confirm and grade EV71 neurological disease. [6] [9]
- Mild disease = analgesia, hydration, childcare exclusion, safety-net; any EV71 red flag = admit and observe; autonomic or respiratory compromise = PICU. [2] [8]
- EV71 haemodynamic care is fluid restriction + milrinone, not generous boluses — the failure is sympathetic overdrive with leak, not pump failure. [7]
- No proven antiviral; IVIG is used empirically on weak evidence. Prevention = hygiene and exclusion. [8]
- Inactivated EV71 vaccines (Zhu, Li — NEJM 2014) work and are licensed in China, but are not in routine ANZ/UK/US/Canada schedules. [3] [4]
- Onychomadesis weeks after a febrile vesicular illness points back to coxsackievirus A6 atypical HFMD. [8]
References
- [1]Solomon T; Lewthwaite P; Perera D; Cardosa MJ; Ooi MH; et al Virology, epidemiology, pathogenesis, and control of enterovirus 71. Lancet Infect Dis, 2010.PMID 20961813
- [2]Ooi MH; Wong SC; Lewthwaite P; Cardosa MJ; Solomon T Clinical features, diagnosis, and management of enterovirus 71. Lancet Neurol, 2010.PMID 20965438
- [3]Zhu F; Xu W; Xia J; Liang Z; et al Efficacy, safety, and immunogenicity of an enterovirus 71 vaccine in China. N Engl J Med, 2014.PMID 24571754
- [4]Li R; Liu L; Mo Z; Wang X; Xia J; et al An inactivated enterovirus 71 vaccine in healthy children. N Engl J Med, 2014.PMID 24571755
- [5]Ooi MH; Wong SC; Mohan A; Podin Y; et al Identification and validation of clinical predictors for the risk of neurological involvement in children with hand, foot, and mouth disease in Sarawak. BMC Infect Dis, 2009.PMID 19152683
- [6]Ooi MH; Solomon T; Podin Y; Mohan A; et al Evaluation of different clinical sample types in diagnosis of human enterovirus 71-associated hand-foot-and-mouth disease. J Clin Microbiol, 2007.PMID 17446325
- [7]Griffiths MJ; Ooi MH; Wong SC; Mohan A; et al In enterovirus 71 encephalitis with cardio-respiratory compromise, elevated interleukin 1β, interleukin 1 receptor antagonist, and granulocyte colony-stimulating factor levels are markers of poor prognosis. J Infect Dis, 2012.PMID 22829643
- [8]Cox JA; Hiscox JA; Solomon T; Ooi MH; et al Immunopathogenesis and Virus-Host Interactions of Enterovirus 71 in Patients with Hand, Foot and Mouth Disease. Front Microbiol, 2017.PMID 29238324
- [9]Weng KF; Chen LL; Huang PN; Shih SR Neural pathogenesis of enterovirus 71 infection. Microbes Infect, 2010.PMID 20348010
- [10]Qiu J; Lu X; Liu P; Zhang X; et al N-terminal pro-B-type natriuretic peptide for the prognostic prediction of severe enterovirus 71-associated hand, foot, and mouth disease. Int J Infect Dis, 2017.PMID 27818360