Paeds · infectious-diseases
Hepatitis A, B, C and E in children
Also known as Viral hepatitis in children · Hepatitis A infection · Hepatitis B infection and chronic carriage · Hepatitis C infection · Hepatitis E infection · Acute viral hepatitis · Hepatotropic virus infection
Fellowship topic on the four hepatotropic viruses in children — hepatitis A, B, C and E — grouped by transmission route and chronicity. Hepatitis A and E are enteric, faecal-oral, acute and self-limited (with hepatitis E carrying disproportionate mortality in pregnancy); hepatitis B and C are blood-borne and perinatal, and become chronic when acquired at birth. The page covers the acute hepatitis presentation (and its anicteric form in young children), the serology and viral-load panels, the vertically-exposed neonate hepatitis B immunoprophylaxis bundle of birth-dose vaccine plus HBIG and maternal tenofovir suppression, the hepatitis C test-and-treat pathway with direct-acting antivirals, the support-and-survival pathway for hepatitis E, and the acute liver failure bundle where INR — not bilirubin — is the prognostic anchor — with ANZ, UK, US and Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Faecal-oral is A and E; blood-borne and perinatal is B and C — and the vowels mark the chronic divide
Overview & Definition
Picture a ten-year-old brought to the emergency department a week after returning from a family trip overseas with fever, nausea, dark urine and yellow eyes. Her liver enzymes are in the thousands, her INR is normal, and her hepatitis A IgM is positive. This is acute hepatitis A — a self-limited enteric infection that she caught from contaminated food or water, and that she will clear completely. Recognising it sets two priorities: support her through the acute illness with fluids and rest, and trace the household and school contacts for hygiene and immunisation. [1] [2]
Now picture a different child: a six-month-old brought to the outpatient clinic because her mother is hepatitis B surface-antigen positive. The baby received the birth-dose vaccine and hepatitis B immunoglobulin, and today's serology shows protective antibody. This is the prevention success story — the vertically-exposed neonate pathway working as designed, because the birth-dose bundle within twenty-four hours prevents the majority of chronic carriage. The two pictures sit at the heart of the topic: the acute, clearing virus that hygiene and vaccine tame, and the chronic, silent virus that immunoprophylaxis and maternal suppression hold at bay. [4] [6]
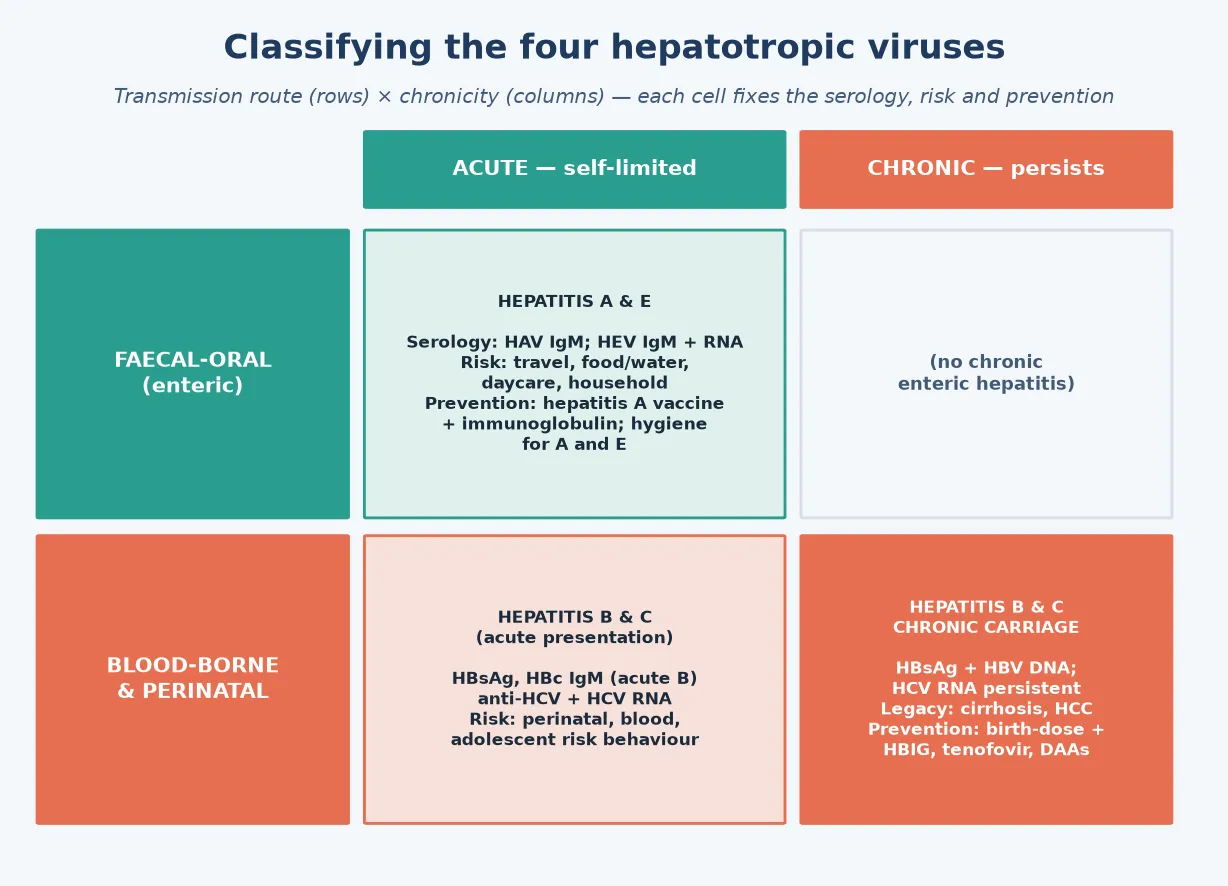
The four hepatotropic viruses — hepatitis A, B, C and E — are grouped by how the child meets them and what happens next. Hepatitis A and E are enteric RNA viruses transmitted by the faecal-oral route; they cause acute hepatitis that resolves without chronicity. Hepatitis B is a DNA virus and hepatitis C is an RNA virus, both blood-borne and perinatal; they cause chronic infection when acquired at birth, because the immature immune system enters an immune-tolerant state that lets the virus persist. The clinician's job has two halves: recognise and support the acute illness, and run the prevention and surveillance machinery that stops the chronic disease. [1] [5]
Classification
Classify the hepatotropic viruses by the two axes that decide everything that follows — how the child acquires them, and whether they persist. The transmission-route axis separates the enteric viruses, hepatitis A and E, transmitted faecal-orally through contaminated food, water and hands, from the blood-borne and perinatal viruses, hepatitis B and C, transmitted by blood exposure and from mother to baby around the time of birth. This single distinction frames the history you take, the contacts you trace, and the prevention you offer. [1] [5]
The chronicity axis is the one that decides the long-term destiny. Hepatitis A and E cause acute hepatitis and clear completely — there is no chronic carrier state, although rare relapsing or cholestatic hepatitis A and the dangerous hepatitis E of pregnancy are exceptions to watch. Hepatitis B and C, when acquired perinatally, become chronic in the majority, because the neonatal immune system tolerates rather than clears the virus. This is why a baby with hepatitis B is usually silent and well, yet carries a virus that may, decades later, cause cirrhosis and hepatocellular carcinoma — and why surveillance, not the acute encounter, is the heart of managing the chronic viruses in childhood. [6] [7]
A third, clinical lens matters at the bedside — the syndrome the child presents with. Acute hepatitis is the icteric or anicteric illness with high transaminases from A or E (and occasionally the acute presentation of B). Chronic hepatitis is the silent, screen-detected carrier state of B or C. Fulminant hepatitis, or acute liver failure, is the catastrophic, time-critical syndrome of massive hepatocyte necrosis with coagulopathy and encephalopathy — it can complicate any of the four but is the feared outcome of acute hepatitis B with delta coinfection, of hepatitis E in pregnancy, and rarely of hepatitis A. Holding the syndrome in mind directs the tempo of the response. [2] [11]
Epidemiology & Risk Factors
Where do children meet each virus, and who is at risk? Hepatitis A is acquired faecal-orally, and in high-income countries with universal childhood vaccination the burden has fallen dramatically — most cases now cluster in travellers, household and daycare contacts, and in outbreaks linked to contaminated food. Young children often have anicteric or subclinical infection, which makes them efficient silent spreaders in daycare and household settings; the classic scenario is an adult recognised with hepatitis A traced back to an asymptomatic child. [1] [3]
Hepatitis B remains a global paediatric burden because of vertical transmission. The risk that an hepatitis B e-antigen-positive, high-viraemic mother transmits the virus to her baby at birth is high, and without immunoprophylaxis the majority of infected neonates become chronic carriers — which is why the birth-dose vaccine and hepatitis B immunoglobulin, and maternal tenofovir suppression for the high-viraemic mother, are the foundation of hepatitis B elimination. In adolescence, horizontal blood-borne and sexual transmission re-enters the picture, and unvaccinated adolescents with risk behaviours are a second high-risk group. [4] [6]
Hepatitis C is also vertically transmitted, though far less efficiently than hepatitis B — roughly five to six percent of infants born to HCV-RNA-positive mothers become infected, with the risk higher in mothers with high viral loads and HIV coinfection. There is no hepatitis C vaccine and no immunoglobulin, so prevention rests on testing and treating women of childbearing age and the children they bear. The contemporary change is that hepatitis C is now curable in children with short, well-tolerated direct-acting antiviral regimens, transforming the prognosis of a once-chronic disease. [8] [10]
Hepatitis E is the most common cause of acute viral hepatitis worldwide, transmitted faecal-orally through contaminated water, and endemic across much of Asia, Africa and Central America. In children hepatitis E is usually mild and self-limited, often subclinical. Its notoriety rests on pregnancy: hepatitis E in the third trimester carries a high maternal case-fatality rate from acute liver failure, and adverse foetal outcomes including miscarriage and stillbirth. For a pregnant adolescent returned from an endemic area with acute hepatitis, hepatitis E is the diagnosis that must not be missed. [11] [12]
Pathophysiology
Why does one virus clear and another stay for life? The answer lies in how each virus enters the hepatocyte, how the immune system responds, and — for the chronic viruses — in the immune tolerance of the neonate. All four viruses target the hepatocyte, but the liver injury they cause is largely immune-mediated rather than directly cytopathic: it is the host's cytotoxic T-cell and cytokine response to infected hepatocytes that produces the inflammation, the transaminase release and the jaundice, not the virus lysing cells on its own. [5] [1]
For hepatitis A and E, the virus enters through the gut, reaches the liver via the portal blood, replicates in hepatocytes and is shed into the bile and back into the gut — completing the faecal-oral cycle. The immune response clears the infected hepatocytes over weeks, the liver regenerates, and the child recovers fully with no residual virus. The same enteric-replicative biology explains why hepatitis A and E are excreted in stool and spread by the faecal-oral route, and why hygiene and safe food and water are the durable prevention. [1] [11]
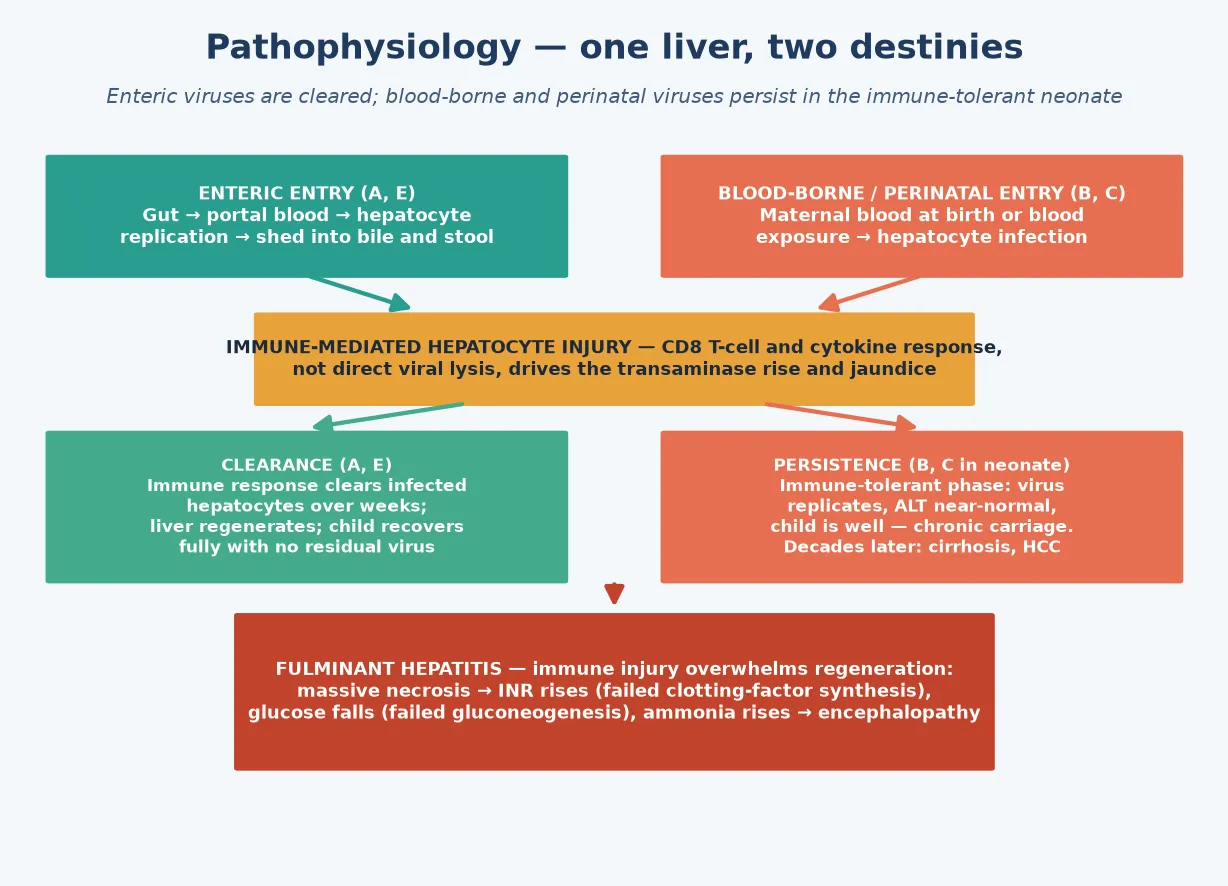
For hepatitis B and C, the pathophysiology turns on the moment of acquisition. When an adult meets hepatitis B, the mature immune system clears the virus in over ninety percent of cases. When a neonate meets it at birth, the immature immune system enters an immune-tolerant phase in which the virus replicates freely without significant hepatic inflammation — the child is well, the transaminases are near-normal, but the virus persists. Over years to decades the tolerant state may give way to immune-active disease, with flares of inflammation that drive fibrosis, cirrhosis and eventually hepatocellular carcinoma. This is why vertically-acquired hepatitis B is a chronic disease of childhood that declares itself in adulthood, and why the prevention and surveillance machinery is the heart of management. [6] [7]
Fulminant hepatitis is the catastrophe where immune-mediated hepatocyte injury overwhelms the liver's regenerative capacity. Massive necrosis collapses hepatic synthesis — coagulation factors fall and the INR rises, glucose falls as gluconeogenesis fails, ammonia accumulates as detoxification fails, and cerebral oedema and encephalopathy follow. The reason the INR, not the bilirubin or the transaminases, is the prognostic anchor is that the INR measures what the liver can still make: when synthesis fails, the child is in liver failure regardless of how high the bilirubin has climbed. [2] [5]
Clinical Presentation
The classic presentation of acute viral hepatitis in a child is a prodrome of fever, fatigue, anorexia, nausea, vomiting and abdominal discomfort, followed after several days by the icteric phase — dark urine, pale stools, and jaundice as conjugated bilirubin accumulates. Hepatomegaly and right-upper-quadrant tenderness are common, and some children have arthralgia, a transient rash or lymphadenopathy in the prodrome. This textbook picture is most often hepatitis A in the returned traveller or contact, and hepatitis E in the endemic or travel setting. [2] [11]
The presentation that examiners probe deliberately is the anicteric or subclinical child. Young children with hepatitis A frequently have a mild, non-specific febrile illness with vomiting and little or no jaundice — a child under six is often anicteric — and the diagnosis is missed unless the ALT is checked or a contact is traced. The corollary is that young children are the silent spreaders in households and daycare, and that a febrile, vomiting child after travel deserves a hepatitis screen even in the absence of jaundice. [1] [3]
Chronic hepatitis B and C are usually silent in childhood. The vertically-infected infant is well; the diagnosis is made by screening the infant of an infected mother, or by finding an abnormal liver function test on a panel done for another reason. Stigmata of chronic liver disease — splenomegaly, palmar erythema, spider naevi, ascites — are late and uncommon in children, which is why the chronic viruses are diseases of surveillance, not presentation. The long-term sequelae are cirrhosis and hepatocellular carcinoma, and the role of the paediatrician is to monitor, to time antiviral therapy, and to transition the young person to adult hepatology care. [6] [7]
The high-risk presentations are the ones that change disposition. Acute liver failure presents with deepening jaundice, a rising INR, hypoglycaemia and encephalopathy — drowsiness, irritability, asterixis and, in the worst case, coma. Hepatitis E in a pregnant adolescent presents as a rapidly progressive acute hepatitis with a high risk of fulminant course. And the adolescent with newly-identified chronic hepatitis B or C presents not with symptoms but with a positive test — and the encounter that follows, of disclosure, counselling and surveillance, is itself a clinical event that must be handled well. [11] [12]
Differential Diagnosis
For the child with acute jaundice and hepatitis, the differential is broad, and the hepatitis viruses are only one family among many. The other infectious causes — Epstein-Barr virus, cytomegalovirus, adenovirus, enterovirus, and arboviruses in the traveller — produce a similar hepatitis picture and are distinguished by serology and the clinical context. Drug and toxin-induced liver injury (paracetamol overdose is the archetype, alongside anticonvulsants, antibiotics and complementary medicines) must always be sought by history. Biliary obstruction — choledochal cyst, gallstones, biliary atresia in the neonate — produces a cholestatic pattern distinguished by ultrasound. [2] [5]
Autoimmune hepatitis and the metabolic liver diseases are the diagnoses not to miss in the child with chronic or relapsing hepatitis. Autoimmune hepatitis presents with high transaminases, hypergammaglobulinaemia and autoantibodies, often in an adolescent girl. Wilson disease produces a hepatitis that may be acute, chronic or fulminant, with a low caeruloplasmin and Kayser-Fleischer rings. Alpha-1-antitrypsin deficiency, glycogen storage disease and tyrosinaemia are the inherited metabolic causes in the younger child. Haemolysis produces jaundice with a high indirect bilirubin and a normal ALT — a different pattern from hepatocellular injury. [5] [7]
For the fulminant presentation, the differential narrows to the causes of acute liver failure. Acute viral hepatitis (B, with or without delta; E in pregnancy; rarely A) sits alongside paracetamol toxicity, mushroom poisoning, Reye syndrome, metabolic decompensation (Wilson disease) and autoimmune hepatitis. The history of drug ingestion, the metabolic and autoimmune screens, and the viral serology together resolve it — but the management is the same: support the liver, protect the brain and the glucose, correct the coagulation, and refer to a transplant centre early. [2] [11]
For the child with a positive hepatitis B or C screen, the differential is not of the virus — the test is the diagnosis — but of the stage and the co-pathology. Is this acute, chronic, or a resolved past infection (a serology-reading problem)? Is there co-infection with hepatitis D, HIV, or another hepatitis virus? Is there already fibrosis or cirrhosis? These questions direct the surveillance and the timing of treatment, and they are answered by the full serology and viral-load panel, the non-invasive fibrosis assessment and, occasionally, the liver biopsy. [6] [10]
Clinical & Bedside Assessment
The assessment begins with a focused history built around the liver and the exposure. For the child with acute hepatitis, ask about travel, food and water exposures, household and daycare contacts, recent blood exposure or procedures, drug and supplement ingestion, and the immunisation history. For the neonate, establish the maternal hepatitis B surface-antigen status, the hepatitis C status, and whether the birth-dose bundle was given. For the adolescent, ask about sexual contacts, blood and needle exposure, body piercing and tattooing, alcohol and substance use. [4] [10]
Establish the synthetic function and the encephalopathy grade precisely, because these frame the disposition. Ask about drowsiness, irritability, sleep reversal and confusion, and examine for asterixis, brisk reflexes and the level of consciousness. Measure the liver span and tenderness, look for splenomegaly and ascites, and examine for the stigmata of chronic liver disease in the child who may have long-standing disease. A raised or falling liver span in acute hepatitis can suggest massive necrosis — a collapsing liver — and is a grave sign. [2] [5]
Document the essentials that frame the response. Record the vaccination history and the maternal status, because they decide the prevention pathway. Record the INR, the glucose and the mental state at every assessment in the acutely unwell child, because they are the prognostic anchors. Record the transaminases and bilirubin to track the injury, but treat the INR as the test that changes disposition. For the chronic-carrier child, record the viral load, the ALT trend, the fibrosis assessment and the hepatocellular-carcinoma surveillance status, because these drive the timing of treatment. [6] [7]
Investigations
The investigation of viral hepatitis rests on two pillars: the serology and viral-load panels that identify the virus and its stage, and the liver-function and synthetic-function tests that gauge the injury and the prognosis. For suspected acute hepatitis, send a hepatitis A IgM, a hepatitis B surface antigen with core IgM, a hepatitis C antibody, and — in the traveller or pregnant adolescent — a hepatitis E IgM and RNA. The pattern distinguishes acute from chronic and resolved infection, and it directs the management. [1] [10]
The hepatitis B serology panel is the one most often tested, and it must be read as a set. Hepatitis B surface antigen marks infection; hepatitis B e-antigen and a high HBV DNA mark high infectivity and replication; hepatitis B core IgM marks acute infection while core total antibody marks past or chronic exposure; and hepatitis B surface antibody marks immunity, whether from vaccination (surface antibody alone) or resolved natural infection (surface antibody with core antibody). Reading the panel as a whole resolves the common pitfalls of the immunised-versus-infected child and the window period. [5] [6]
In Australia and Aotearoa New Zealand, the universal immunisation schedule includes hepatitis B vaccine from birth with subsequent doses through infancy, and the hepatitis A vaccine is funded for Aboriginal and Torres Strait Islander children in some jurisdictions, for travellers, and for high-risk groups. The Australian guidance and the New Zealand schedule set the hepatitis B birth-dose-and-HBIG bundle, the maternal tenofovir suppression threshold for high-viraemic mothers, and the hepatitis C test-and-treat pathway. Refugee and migrant children are offered catch-up immunisation and screening for hepatitis B and C. [3] [6]
Hepatitis C is diagnosed by antibody screening followed by a confirmatory HCV RNA — the antibody may reflect past exposure or active infection, and only a detectable RNA confirms current infection. This is a common pitfall: a positive antibody in an infant under eighteen months may reflect passively-transferred maternal antibody, so the infant is tested by HCV RNA, typically at two months and again later, with serology confirmed after eighteen months. The good news is that chronic hepatitis C is now curable in children with short direct-acting antiviral regimens. [9] [10]
The supporting tests are as important as the virology. In the acutely unwell child, the INR is the anchor: a raised or rising INR signals impaired synthesis and possible liver failure, regardless of the bilirubin. Add glucose (hypoglycaemia from failed gluconeogenesis), ammonia (encephalopathy), a full blood count and a coagulation screen, and an abdominal ultrasound for the biliary tree and liver texture. For the chronic-carrier child, non-invasive fibrosis assessment — transient elastography, ALT trends and the AST-to-platelet ratio — stages the disease, and alpha-fetoprotein and ultrasound form the hepatocellular-carcinoma surveillance. A liver biopsy is reserved for when staging, aetiology or co-pathology remain uncertain. [6] [7]
Management — Resuscitation
Resuscitation is about the child with acute liver failure — the catastrophic, time-critical syndrome that can complicate any of the four viruses. The principle is that hepatic synthetic failure (coagulopathy, hypoglycaemia, encephalopathy) is the emergency, and that the bilirubin and transaminases, however high, are not. The threshold to escalate is a rising INR, a falling glucose, or any encephalopathy — and the response is a bundle that protects the brain, the glucose and the coagulation while a transplant centre is mobilised. [2] [5]
The acute liver failure bundle is supportive and specific. Maintain the airway and the circulation; correct hypoglycaemia with dextrose infusions; correct coagulopathy with vitamin K and, where bleeding or before procedures, fresh frozen plasma; manage encephalopathy and cerebral oedema with head positioning, osmotic agents and, in severe cases, intubation; and treat the precipitant where one is identified. N-acetylcysteine is used in acute liver failure even when paracetamol is not the cause, because it supports hepatic glutathione and improves outcome. Involve the paediatric intensive care unit and a liver-transplant centre early, because the window for transfer closes as encephalopathy deepens. [2] [11]
Hepatitis E in pregnancy is a specific resuscitation scenario. A pregnant adolescent with acute hepatitis and rising transaminases is hepatitis-E-until-proven-otherwise in an endemic or travel setting, and the risk of fulminant course in the third trimester is high. The response is close monitoring of the INR and mental state, early PICU involvement if any synthetic failure appears, and multidisciplinary care with obstetrics and hepatology. The maternal and foetal risk is the reason hepatitis E earns its place among the red-flag hepatitides. [12] [11]
Management — Definitive & Stepwise
Definitive management is a stepwise pathway matched to the virus, the stage and the host. Acute hepatitis A and E receive supportive care — rest, hydration, antiemetics and analgesia, with attention to nutrition and the avoidance of hepatotoxic drugs and alcohol. Hygiene and exclusion prevent secondary spread: hand-washing, safe food and water, school and childcare exclusion while the child is symptomatic, and contact tracing and post-exposure prophylaxis (hepatitis A vaccine or immunoglobulin) for household and close contacts of hepatitis A. [2] [3]
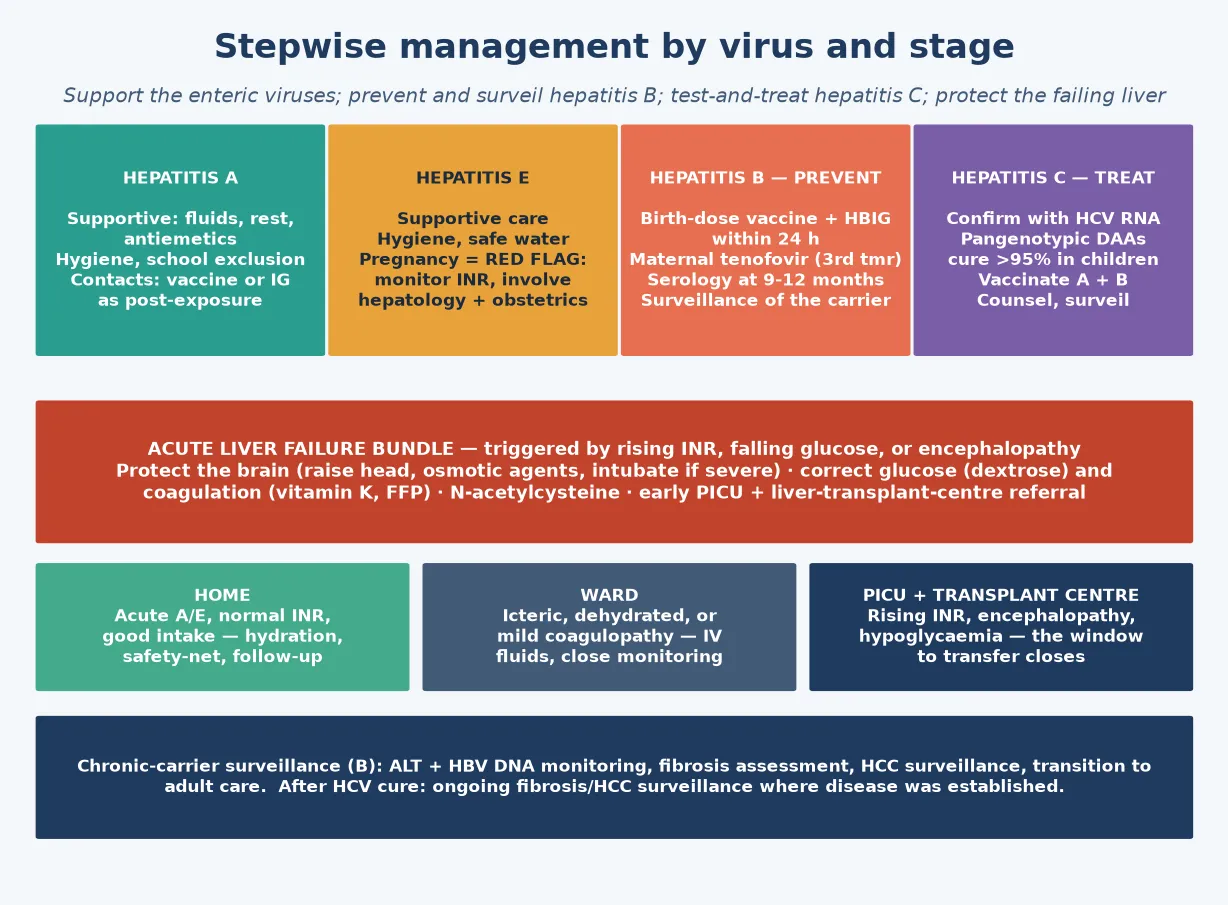
The hepatitis B prevention pathway is the centrepiece. The neonate of an hepatitis B surface-antigen-positive mother receives the birth-dose hepatitis B vaccine and hepatitis B immunoglobulin within twenty-four hours of birth — ideally within twelve — and the vaccine series is completed through infancy, with serological testing at nine to twelve months to confirm protection. For the high-viraemic mother, maternal tenofovir in the third trimester suppresses the viral load and further reduces the residual transmission that immunoprophylaxis alone does not prevent. This combined strategy is the global hepatitis B elimination backbone. [4] [6]
The hepatitis B vertically-exposed-neonate pathway
Antenatal: test every pregnant woman for hepatitis B surface antigen; for those positive, measure HBV DNA and hepatitis B e-antigen to gauge transmission risk.
Maternal suppression: offer tenofovir in the third trimester to mothers with high HBV DNA to reduce the viral load at delivery.
At birth: give the hepatitis B vaccine AND hepatitis B immunoglobulin within 24 hours (ideally within 12), at separate injection sites, regardless of mode of delivery.
Through infancy: complete the hepatitis B vaccine series on schedule; do not breastfeed-restrict (breastfeeding is safe once the baby has received immunoprophylaxis).
At 9-12 months: test the infant for HBsAg and anti-HBs to confirm protection versus chronic carriage, and arrange ongoing surveillance for the infected infant.
For the chronic hepatitis B carrier in childhood, management is surveillance-led. Most children are in the immune-tolerant phase with normal ALT and high viral load but no fibrosis, and antiviral therapy is withheld until the immune-active phase appears or fibrosis develops — a decision made with paediatric hepatology. The role of the general paediatrician is to monitor ALT and HBV DNA, to surveil for hepatocellular carcinoma in high-risk groups, to vaccinate susceptible contacts, and to plan the transition to adult care. The adolescent with chronic hepatitis B is counselled on blood and sexual transmission, on not donating blood, and on alcohol avoidance. [6] [7]
The hepatitis C pathway is test-and-treat. Confirm active infection with HCV RNA, genotype where it still guides therapy, and treat with direct-acting antivirals in age-appropriate, pangenotypic regimens — the contemporary reality is that chronic hepatitis C is curable in the great majority of children with short, well-tolerated oral courses, transforming a once-chronic disease into a treated one. The general paediatrician's role is to confirm the diagnosis, to refer for treatment, to counsel on transmission (hepatitis C is not spread by casual contact, and breastfeeding is not contraindicated), and to vaccinate against hepatitis A and B to prevent co-infection. [9] [10]
Specific Subtypes & Scenarios
A neonate born to an hepatitis B surface-antigen-positive mother. This is the prevention scenario that defines the topic. The baby receives the birth-dose vaccine and hepatitis B immunoglobulin within twenty-four hours, the vaccine series is completed through infancy, and serology at nine to twelve months confirms protection. If the mother is highly viraemic, maternal tenofovir in the third trimester adds a further layer of prevention. The infant who nonetheless becomes a chronic carrier enters lifelong surveillance, and the family is counselled and the contacts vaccinated. [4] [6]
An adolescent found to have chronic hepatitis C. Confirm with HCV RNA, treat with a pangenotypic direct-acting antiviral regimen, and cure is now expected. Counsel the young person on transmission — blood and sexual, not casual — on not sharing razors or toothbrushes, on not donating blood, and on alcohol avoidance. Vaccinate against hepatitis A and B. Plan the transition to adult hepatology, because the long-term surveillance for fibrosis and hepatocellular carcinoma continues even after cure in those with established disease. [9] [10]
A child returning from travel with acute hepatitis A. The picture is a prodrome then jaundice with high transaminases and a normal INR, confirmed by hepatitis A IgM. Management is supportive — fluids, rest, antiemetics, avoidance of hepatotoxins — with attention to hydration and nutrition. Trace household and close contacts for hepatitis A vaccine or immunoglobulin as post-exposure prophylaxis, exclude from childcare and food-handling while symptomatic, and reinforce hand hygiene and safe food and water for travel. Most children recover fully over weeks. [2] [3]
A pregnant adolescent with hepatitis E. This is the red-flag hepatitis. In an endemic or travel setting, acute hepatitis in the third trimester is hepatitis E until proven otherwise, and the risk of fulminant course and adverse foetal outcome is high. Monitor the INR and mental state closely, involve hepatology and obstetrics early, escalate to PICU at the first sign of synthetic failure, and counsel the family that the maternal risk is real. Children outside pregnancy generally recover fully, but pregnancy is the setting where hepatitis E earns its danger. [11] [12]
A child with chronic hepatitis B and an immunocompromised state or coinfection. Immunosuppression, chemotherapy, transplantation and HIV coinfection can reactivate or accelerate hepatitis B, and prophylactic antiviral therapy is given before immunosuppression where indicated. Co-infection with hepatitis D worsens the course and is sought in the chronically infected child. These children are managed jointly with paediatric hepatology and infectious diseases, and the surveillance is intensified. [6] [7]
Complications & Pitfalls
The complications split along the chronicity axis. For hepatitis A and E, the feared complication is fulminant hepatitis — rare overall, but disproportionately common with hepatitis E in pregnancy, and a catastrophic event when it occurs. Hepatitis A also has rare relapsing and cholestatic variants that prolong the illness but generally still resolve. For hepatitis B and C, the complications are the long-term sequelae of chronic carriage — cirrhosis, liver failure and hepatocellular carcinoma — that declare themselves decades after the silent perinatal acquisition. [2] [11]
The recurring clinical pitfall is reading the serology wrong. Misreading a hepatitis B panel — confusing a vaccinated child (surface antibody alone) with an infected one (surface antigen positive), or missing a window-period case where surface antigen has cleared but surface antibody has not yet appeared — leads to the wrong management. The defence is to read the panel as a set: surface antigen, e-antigen, core antibody and surface antibody together resolve the picture, with HBV DNA to quantify. Similarly, falsely reassuring an infant on a single hepatitis C antibody (which may be maternal) rather than HCV RNA is the neonatal pitfall. [5] [10]
The most preventable error in the whole topic is failing to deliver the hepatitis B birth-dose-and-HBIG bundle within twenty-four hours. This single bundle prevents the majority of vertical transmission and the chronic carriage that follows, and its omission — through a missed maternal screen, a missed handover, or a misplaced assumption that the vaccine alone suffices — is the avoidable source of lifelong chronic hepatitis B. The defence is universal antenatal screening, a clear handover at delivery, and a protocol that treats the birth-dose bundle as a never-miss event. [4] [6]
The second preventable error is missing acute liver failure by watching the bilirubin instead of the INR. The child whose bilirubin is climbing but whose INR, glucose and mental state are normal has severe hepatitis but not liver failure; the child whose INR is rising, glucose falling or consciousness clouding has liver failure regardless of the bilirubin. The defence is to treat the INR, the glucose and the mental state as the prognostic anchors, and to escalate to PICU and a transplant centre at the first sign of synthetic failure. [2] [5]
Prognosis & Disposition
Most children with acute hepatitis A and E recover fully over weeks, with morbidity driven by nausea, dehydration and fatigue, and full regeneration of the liver. The disposition is usually home management with hydration, nutrition, hygiene and a clear safety-net for deepening jaundice, drowsiness, bleeding or confusion. Admission is reserved for the dehydrated child, the child with coagulopathy or encephalopathy, and the pregnant adolescent with hepatitis E. [2] [11]
The chronic morbidity is concentrated in hepatitis B and C. Vertically-acquired hepatitis B carries a lifetime risk of cirrhosis and hepatocellular carcinoma that is reduced — though not eliminated — by surveillance and timely antiviral therapy. Hepatitis C, once a chronic disease of childhood, is now curable with direct-acting antivirals, transforming the prognosis for the treated child. The concentration of long-term harm in the chronic viruses is why the prevention and surveillance machinery is the heart of the topic. [6] [9]
Disposition follows the syndrome and the synthetic function. Manage at home, with a hydration plan and follow-up, the child with acute hepatitis A or E and a normal INR. Admit to the ward the icteric child needing intravenous fluids or close monitoring, and the child with mild coagulopathy for observation. Admit to the paediatric intensive care unit the child with acute liver failure — a rising INR, encephalopathy or hypoglycaemia — and refer early to a liver-transplant centre. The threshold for admitting a deteriorating child is deliberately low. [2] [5]
At discharge, complete the supportive course for acute hepatitis, and arrange the surveillance for the chronic carrier — ALT and viral-load monitoring, fibrosis assessment, and hepatocellular-carcinoma surveillance in high-risk groups. For the adolescent, plan the transition to adult hepatology care, because the long-term consequences of chronic hepatitis B and the surveillance after hepatitis C cure continue into adulthood. Give the family a clear safety-net for recurrence, deterioration, bleeding or confusion. [6] [10]
Special Populations
Neonates and vertically-exposed infants are the central special population. The hepatitis-B-exposed neonate receives the birth-dose bundle and serology at nine to twelve months; the hepatitis-C-exposed infant is tested by HCV RNA rather than antibody, because passively-transferred maternal antibody confounds the serology until eighteen months. These children depend on the prevention and testing pathway being run correctly, and the general paediatrician's role is to ensure the bundle is delivered and the follow-up serology is done. [4] [10]
Pregnant adolescents carry the specific hepatitis E risk. Acute hepatitis in the third trimester is hepatitis E until proven otherwise in an endemic or travel setting, and the maternal and foetal risk is high. The response is close monitoring, early hepatology and obstetric involvement, and escalation at the first sign of synthetic failure. Pre-conception counselling for the young woman with chronic hepatitis B or C — suppression, treatment and surveillance — is the durable prevention. [12] [11]
Immunocompromised children, transplant recipients and those with HIV coinfection are at risk of reactivation, accelerated disease and atypical presentations of hepatitis B and C. Prophylactic antiviral therapy is given before immunosuppression where indicated, co-infections are sought and treated, and surveillance is intensified. These children are managed jointly with hepatology, infectious diseases and oncology or transplantation. [6] [7]
Refugee, asylum-seeking and migrant children, Aboriginal and Torres Strait Islander, Maori and Indigenous children, and rural and remote families may face barriers to screening, immunisation and surveillance. Ensure culturally safe, equitable access to screening, catch-up immunisation, immunoprophylaxis and treatment, and use trained interpreters rather than family members. Disadvantage and distance should never be the reason a hepatitis B vertically-exposed neonate misses the birth-dose bundle or a chronic-carrier child misses surveillance. [3] [6]
Evidence, Guidelines & Regional Differences
The contemporary framing of hepatitis A as an enteric, vaccine-preventable disease is set out in the Van Damme, Pintó and Feng Nature Reviews Disease Primers primer, and the clinical manifestations and management by Jeong and Lee. Together they frame the acute self-limited course, the anicteric childhood presentation, the rare fulminant and relapsing variants, and the prevention strategy of vaccine and immunoglobulin. The AAP hepatitis A vaccine recommendations underpin the universal and targeted immunisation that has reduced the burden in high-income settings. [1] [2]
The hepatitis B evidence base is anchored by the Jeng, Yip and Lok JAMA review of hepatitis B and the Indolfi et al. Lancet Gastroenterology and Hepatology review of hepatitis B in children and adolescents. They set the vertically-acquired natural history, the immune-tolerance-to-immune-active progression, the chronicity that follows neonatal infection, and the prevention-and-surveillance strategy. The Cheung and Lao review of vertical transmission and mother-to-child prevention, and the Ni paediatric natural-history review, frame the birth-dose-and-HBIG bundle and the maternal tenofovir suppression that together drive hepatitis B elimination. [5] [6]
Hepatitis C direct-acting antivirals in children
Population: Synthesis of phase 2/3 trials of pangenotypic direct-acting antiviral regimens (ledipasvir-sofosbuvir, sofosbuvir-velpatasvir, glecaprevir-pibrentasvir) in children and adolescents with chronic hepatitis C, across age bands from early childhood through adolescence, and the 2023 AASLD-IDSA guidance recommending universal adult screening and pangenotypic treatment.
Key finding
Pangenotypic direct-acting antiviral regimens achieve sustained virological response (cure) rates above ninety-five percent in children and adolescents, with short, well-tolerated oral courses. Treatment is now recommended from early childhood, transforming chronic hepatitis C from a chronic disease into a curable one.
Practice change
Chronic hepatitis C in children is curable. The paediatrician's role is to confirm active infection with HCV RNA and refer for age-appropriate direct-acting antiviral treatment, rather than defer indefinitely. This is the test-and-treat model.
The hepatitis C evidence is set by the AASLD-IDSA 2023 guidance and the Deng et al. systematic review of viral load and mother-to-child transmission, which frame the roughly five-to-six-percent vertical transmission rate, the confounding of infant antibody by maternal antibody, and the test-and-treat model. The Indolfi, Serranti and Resti review of direct-acting antivirals in children frames the cure that has transformed the disease. The hepatitis E evidence rests on the Verghese and Robinson systematic review of hepatitis E in children and the Bergløv, Hallager and Weis systematic review of hepatitis E in pregnancy, which set the paediatric and the pregnancy phenotypes and the disproportionate maternal mortality. [10] [12]
The regional policy structure is consistent in principle and varies in detail. In ANZ, the universal schedule includes hepatitis B vaccine from birth, the birth-dose-and-HBIG bundle is standard, maternal tenofovir suppression is offered to high-viraemic mothers, and the hepatitis A vaccine is funded for high-risk groups and Aboriginal and Torres Strait Islander children in some jurisdictions. In the UK, the Green Book and the National Institute for Health and Care Excellence frame the antenatal hepatitis B screening, the neonatal immunoprophylaxis and the targeted hepatitis A vaccination. In the US, the American Academy of Pediatrics Red Book and the Centers for Disease Control and Prevention set the universal hepatitis B birth dose, the universal adult hepatitis C screening and the paediatric DAA treatment. In Canada, the Canadian Paediatric Society and the National Advisory Committee on Immunization deliver the equivalent strategy. The principle everywhere is that hepatitis B is prevented by immunoprophylaxis and maternal suppression, hepatitis C is cured by direct-acting antivirals, and the enteric viruses are tamed by hygiene, vaccine and surveillance. [3] [6]
The controversies are active: the optimal threshold for maternal tenofovir suppression, the age at which to treat chronic hepatitis C in young children versus deferral, the role of universal hepatitis C screening in pregnancy and the child, and the place of hepatitis E vaccination in endemic countries. The defence against each is the same: deliver the birth-dose-and-HBIG bundle without fail, screen and treat hepatitis C, watch the INR in the acutely unwell child, and treat hepatitis E in pregnancy as the emergency it is. [9] [12]
Exam Pearls
- Faecal-oral is A and E; blood-borne and perinatal is B and C — and the chronic divide runs along the same line. [1]
- The hepatitis B birth-dose vaccine AND hepatitis B immunoglobulin within 24 hours prevents the majority of vertical transmission; the bundle is a never-miss event. [4]
- Maternal tenofovir in the third trimester suppresses high HBV DNA and further reduces transmission. [6]
- Hepatitis C has no vaccine and no immunoglobulin — prevention is test-and-treat the mother and treat the child with direct-acting antivirals (cure rates above ninety-five percent). [9] [10]
- Hepatitis E is the most dangerous hepatitis in pregnancy, with case-fatality up to twenty to twenty-five percent in the third trimester. [12]
- INR — not bilirubin or ALT — is the prognostic anchor of acute liver failure: a rising INR, falling glucose or encephalopathy crosses the threshold to PICU and transplant. [2]
- Young children with hepatitis A are often anicteric — the silent spreaders in daycare; check the ALT and trace contacts. [3]
- Read the hepatitis B panel as a set: surface antigen (infection), e-antigen and HBV DNA (infectivity), core IgM (acute) versus total core (past/chronic), surface antibody (immunity, alone if vaccinated). [5]
- Hepatitis C antibody in an infant under eighteen months may be maternal — test with HCV RNA. [10]
- The vertically-acquired hepatitis B child is usually silent and well — the disease is one of surveillance, not presentation; the legacy is cirrhosis and hepatocellular carcinoma decades later. [7]
References
- [1]Van Damme P; Pintó RM; Feng Z; Cui F; et al Hepatitis A virus infection. Nat Rev Dis Primers, 2023.PMID 37770459
- [2]Jeong SH; Lee HS Hepatitis A: clinical manifestations and management. Intervirology, 2010.PMID 20068336
- [3]American Academy of Pediatrics Committee on Infectious Diseases Hepatitis A vaccine recommendations. Pediatrics, 2007.PMID 17606579
- [4]Cheung KW; Lao TT Hepatitis B - Vertical transmission and the prevention of mother-to-child transmission. Best Pract Res Clin Obstet Gynaecol, 2020.PMID 32249130
- [5]Jeng WJ; Yip TC; Lok AS Hepatitis B: A Review. JAMA, 2026.PMID 42081318
- [6]Indolfi G; Easterbrook P; Dusheiko G; Siberry G; et al Hepatitis B virus infection in children and adolescents. Lancet Gastroenterol Hepatol, 2019.PMID 30982722
- [7]Ni YH Natural history of hepatitis B virus infection: pediatric perspective. J Gastroenterol, 2011.PMID 20812021
- [8]Deng S; Zhong W; Chen W; Wang Z Hepatitis C viral load and mother-to-child transmission: A systematic review and meta-analysis. J Gastroenterol Hepatol, 2023.PMID 36066543
- [9]Indolfi G; Serranti D; Resti M Direct-acting antivirals for children and adolescents with chronic hepatitis C. Lancet Child Adolesc Health, 2018.PMID 30169301
- [10]Bhattacharya D; Aronsohn A; Price J; Lo Re V; et al Hepatitis C Guidance 2023 Update: AASLD-IDSA Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection. Clin Infect Dis, 2023.PMID 37229695
- [11]Verghese VP; Robinson JL A systematic review of hepatitis E virus infection in children. Clin Infect Dis, 2014.PMID 24846637
- [12]Bergløv A; Hallager S; Weis N Hepatitis E during pregnancy: Maternal and foetal case-fatality rates and adverse outcomes-A systematic review. J Viral Hepat, 2019.PMID 31095813