Paeds · infectious-diseases
Herpes simplex infection in children
Also known as Herpes simplex virus infection · HSV-1 and HSV-2 infection · Primary herpetic gingivostomatitis · Cold sores · Neonatal herpes · Eczema herpeticum
Fellowship topic on herpes simplex virus infection in children: HSV-1 and HSV-2 as neurotropic herpesviruses that establish lifelong latency in sensory ganglia; the disease spectrum from primary herpetic gingivostomatitis and recurrent cold sores to eczema herpeticum, HSV keratitis, herpes simplex encephalitis and the three classes of neonatal HSV (skin-eye-mouth, CNS and disseminated); the mucosal-entry, ganglionic-latency and dermatomal-reactivation biology; PCR diagnosis of CSF and surface disease; the tiered aciclovir strategy from supportive care and oral therapy to high-dose intravenous aciclovir for neonatal and CNS disease with post-treatment suppression; and the maternal-neonatal prevention pathway of suppressive therapy, caesarean for active lesions and the exposed-neonate assessment — with ANZ, UK, US and Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
How to tell HSV gingivostomatitis from herpangina at a glance
Overview & Definition
Picture an eighteen-month-old brought to the emergency department with a fever, drooling, and a mouth so painful she has not drunk for a day. Inside her lips and on her gums are clusters of shallow grey ulcers on inflamed bases, and her cervical nodes are enlarged and tender. This is primary herpetic gingivostomatitis — the commonest first encounter with herpes simplex virus in childhood — and recognising it instantly sets two priorities: relieve the pain and protect the hydration, and remember that this child now carries the virus for life. [10] [9]
Herpes simplex virus types 1 and 2 are neurotropic double-stranded DNA human herpesviruses. HSV-1 is transmitted mainly through oral secretions and causes most orolabial and central nervous system disease in childhood; HSV-2 is transmitted mainly sexually and causes most genital and neonatal disease. After primary infection the virus travels up sensory nerves to a ganglion — the trigeminal for orolabial disease, the sacral for genital — and establishes lifelong latency. Reactivation sends it back down the same nerve to the same dermatome, producing recurrent lesions at the original site. [1] [3]
For most children the encounter is a self-limiting mucocutaneous illness. The clinician's job has two halves, and the second is what the fellowship examiner tests. The acute half is to recognise the syndrome, gauge the host-risk tier, treat with the right strength of aciclovir, and protect hydration and vision. The preventive half is to understand that the same virus can devastate a neonate or a temporal lobe, and to run the maternal-neonatal prevention pathway that stops that happening. [1] [2]
Classification
Classify herpes simplex disease the way it presents at the bedside — by virus type, by clinical syndrome, and by host risk — because each lens changes the management. The virus-type lens separates HSV-1, the cause of most childhood orolabial and CNS disease, from HSV-2, the cause of most genital and neonatal disease. The distinction matters because it frames transmission and prevention, but it is not absolute: HSV-1 neonatal disease is increasingly recognised wherever orogenital practices have shifted the epidemiology. [1] [2]
The syndrome lens is the one that matters most at the bedside. Orolabial disease covers primary gingivostomatitis and recurrent herpes labialis. Cutaneous disease covers eczema herpeticum, herpetic whitlow and the clustered vesicles of contact sport exposure. Ocular disease covers keratoconjunctivitis and the vision-threatening dendritic keratitis. Genital disease is an adolescent sexually transmitted infection. Neonatal disease splits into skin-eye-mouth, central nervous system, and disseminated. And central nervous system disease in the older child is herpes simplex encephalitis. Each syndrome carries its own treatment strength and its own danger. [1] [8]
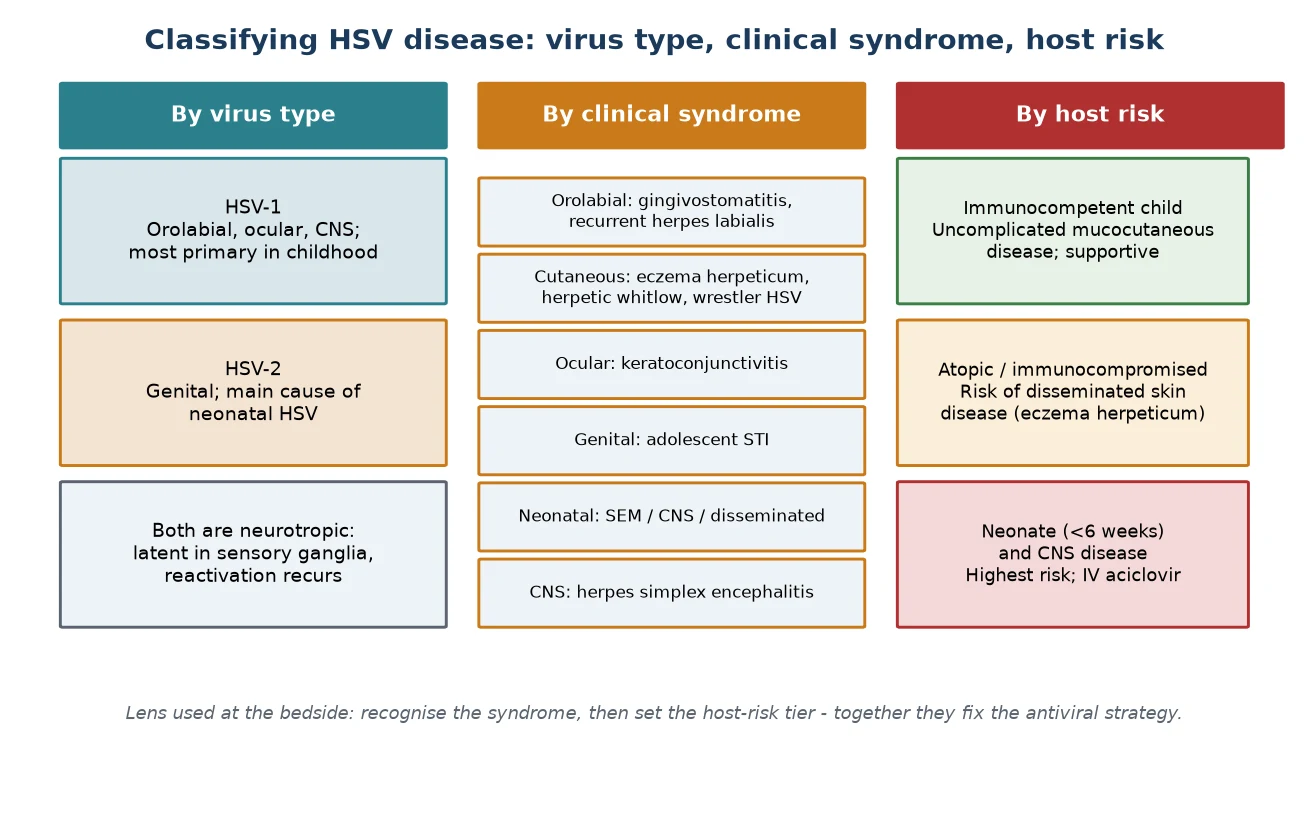
The host-risk lens decides treatment strength. The immunocompetent child usually has uncomplicated mucocutaneous disease managed supportively, with oral aciclovir reserved for severe or early presentations. The atopic or immunocompromised child is at risk of disseminated skin disease and receives systemic aciclovir. And the neonate or the child with central nervous system disease is the highest-risk host, for whom high-dose intravenous aciclovir is given at the earliest suspicion. Holding the risk tier in mind at the first encounter prevents the dangerous default of treating every case as a cold sore. [2] [8]
A fourth distinction matters for neonatal disease. Neonatal HSV is classified into skin-eye-mouth disease (vesicles, keratitis, mouth ulcers — the best prognosis), central nervous system disease (lethargy, seizures, a CSF pleocytosis), and disseminated disease (a sepsis-like illness with hepatitis, pneumonitis and coagulopathy — the worst prognosis). This three-way split is not academic: it sets the duration of aciclovir, the decision to give post-treatment suppression, and the prognosis you offer the family. [3] [4]
Epidemiology & Risk Factors
Where does HSV sit, and who does it hurt? HSV-1 infection is near-universal by adulthood in many populations, with primary infection peaking between one and five years of age and presenting most often as gingivostomatitis. HSV-2 is acquired mainly through sexual contact in adolescence and adulthood, and most genital herpes in young people now reflects a mix of both types. Understanding the age-stratified epidemiology directs both the clinical encounter and the preventive response. [1] [10]
Neonatal HSV is uncommon — roughly one in three thousand to one in twenty thousand live births depending on the region — but it carries high mortality and lifelong morbidity. The majority is acquired intrapartum from maternal genital HSV, and the decisive risk factor is a maternal primary genital infection near delivery, which transmits far more readily than recurrent disease because the mother has not yet made antibody to pass to the baby. This is why a first genital lesion in late pregnancy is the situation that most threatens the neonate. [1] [6]
The burden of severe disease falls on the high-risk hosts. The neonate, especially the premature infant, cannot contain the virus and is at risk of dissemination. The child with atopic dermatitis has a broken skin barrier that HSV invades, producing eczema herpeticum. The immunocompromised child has impaired cell-mediated immunity and is at risk of severe, prolonged and recurrent disease. And the child with HSV keratitis carries a threat to vision that is easy to miss on a busy day. [12] [1]
Reactivation is driven by triggers that erode cell-mediated immunity locally or systemically. Fever, ultraviolet light, stress, fatigue, immunosuppression and local trauma all precipitate cold sores in the latently infected host. The key biology is that cell-mediated immunity rather than antibody controls latency, which is why immunosuppression triggers reactivation and why passive antibody alone does not prevent it. Recognising the trigger helps the family anticipate and the clinician consider suppressive therapy for frequent recurrences. [1] [8]
Pathophysiology
Why does one virus cause a sore mouth today, a cold sore next winter, and devastation in a newborn? The answer lies in the neurotropic, latency-and-reactivation biology of herpes simplex virus. The virus enters through mucosal surfaces or broken skin and replicates in the epithelial cells, producing the vesicle that is the morphological hallmark of the disease. From the epithelium it is taken up by sensory nerve endings and travels by retrograde axonal transport to the sensory ganglion. [1] [8]
In the ganglion — the trigeminal for orolabial disease, the sacral for genital — the virus establishes lifelong latency in the neuronal cells. The host's cell-mediated immunity, rather than antibody, is what holds the latent virus in check, which is why immunosuppression and the immaturity of the neonatal immune system are the principal drivers of severe disease. Antibody alone does not prevent reactivation, and the antibody that a mother has not yet made is exactly the antibody a neonate exposed to a primary maternal infection does not receive. [1] [3]
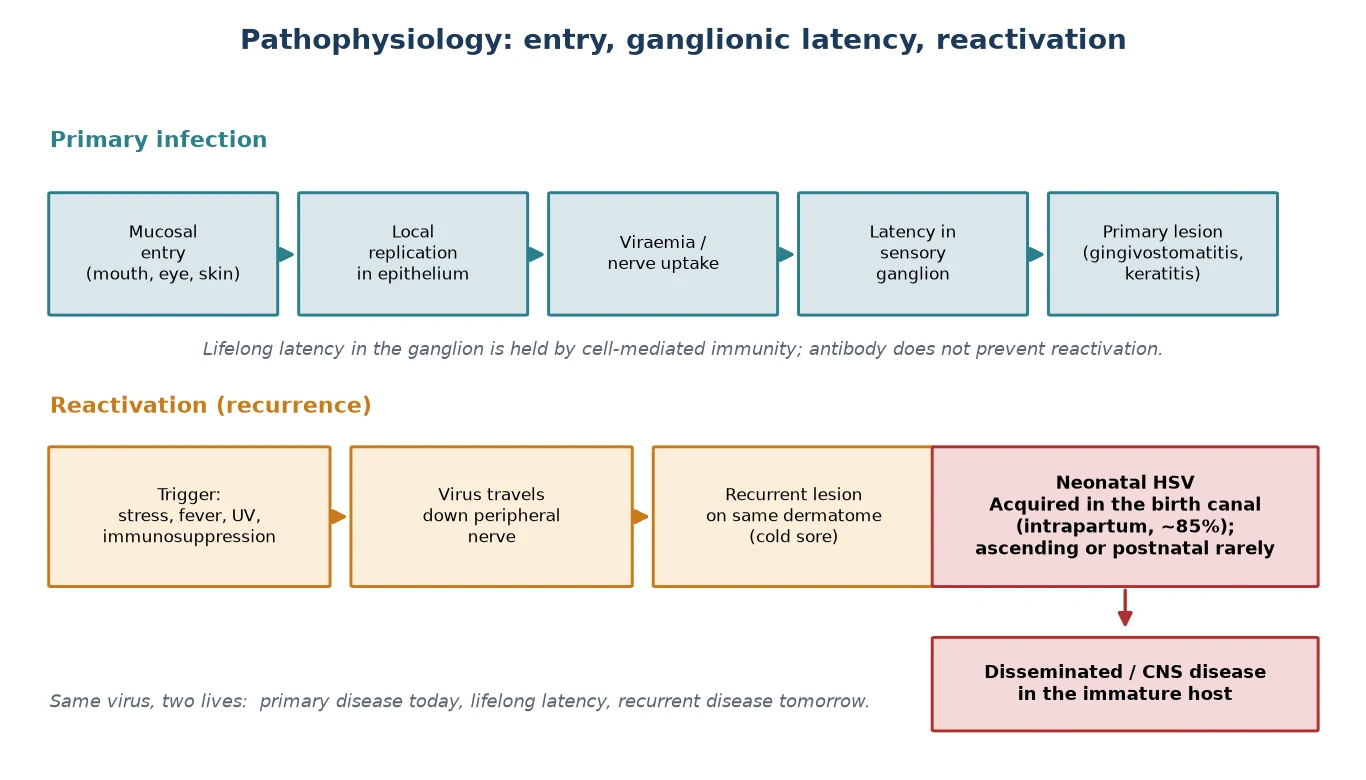
Reactivation within the ganglion sends virus back down the peripheral nerve to the dermatome it supplies, producing a cluster of vesicles at or near the original site — the familiar cold sore. The trigger may be a fever, sun exposure or stress, and the lesion recurs at the same place because the same nerve is involved each time. The biology of recurrence is the bridge between the childhood sore mouth and the adult cold sore, and it is why the latently infected host never truly clears the virus. [1] [8]
The severe-disease biology follows from uncontrolled viral replication in a host who cannot contain it. In the neonate, the immature immune system permits the virus to disseminate beyond the skin to the liver, lungs and brain, producing the disseminated and central nervous system phenotypes. In herpes simplex encephalitis, the virus reaches the temporal lobe and produces a haemorrhagic, necrotising, focal encephalitis that is rapidly progressive and destructive. In eczema herpeticum, the virus exploits the barrier-deficient skin of atopic dermatitis to spread widely across broken skin. The same cascade that is self-limiting in a healthy mouth becomes fulminant when immunity or barrier is absent. [3] [12]
Clinical Presentation
The classic presentation of primary herpetic gingivostomatitis is a prodrome of fever, irritability and malaise followed by the appearance of painful vesicles and ulcers on the gums, tongue, palate and buccal mucosa. The gums are typically swollen, red and bleed easily, and the anterior mouth is preferentially involved. Tender cervical lymphadenopathy, drooling, and refusal to eat or drink are prominent, and it is the refusal to drink — and the dehydration that follows — that most often brings the child to hospital. The illness lasts ten to fourteen days. [10] [9]
Recurrent herpes labialis is the reactivation phenotype: a prodromal tingling or burning at a fixed site on the lip vermillion border, followed by a cluster of vesicles that progress through pustule and crust to healing over several days. The healthy child is systemically well, and the lesion recurs at the same site because the same sensory nerve is involved. Recurrent disease is mild in the immunocompetent host, but frequent or severe recurrences, or recurrence in the immunocompromised, open the door to suppressive oral aciclovir. [1] [11]
The high-risk presentations are the ones that must not be missed. Neonatal HSV in the first four to six weeks of life presents with non-specific signs that overlap with bacterial sepsis — fever, lethargy, poor feeding, irritability — and is easily dismissed until a vesicle appears, a seizure occurs, or the liver fails. The three disease classes express themselves differently: skin-eye-mouth disease with vesicles, keratitis or mouth ulcers; central nervous system disease with lethargy and seizures; and disseminated disease with a sepsis-like illness, hepatitis, pneumonitis and coagulopathy. [2] [4]
Herpes simplex encephalitis presents with fever, altered consciousness, behavioural or personality change, and focal or generalised seizures, often with signs localising to the temporal lobe. It can declare itself subacutely over days, and the clinical pitfall is attributing the altered behaviour to a viral prodrome or a febrile delirium rather than to focal temporal-lobe disease. Eczema herpeticum presents as the rapid onset of painful, monomorphic, punched-out erosions scattered across eczematous skin, with fever, malaise and lymphadenopathy in an atopic child — a dermatological emergency. And HSV keratitis presents as a red, painful, watering eye with a dendritic ulcer on fluorescein staining. [8] [12]
The complications are part of the presentation because they often bring the child to care. The dehydrated child with gingivostomatitis arrives after days of poor intake. The neonate with disseminated HSV arrives in shock with hepatomegaly and bleeding. The child with encephalitis arrives confused and seizing. The child with eczema herpeticum arrives covered in erosions and systemically unwell. Recognising the syndrome at the first encounter sets the tempo of the response. [2] [3]
Differential Diagnosis
For the child with oral ulcers, the differential turns on the distribution, depth and systemic accompaniment. Herpangina and hand-foot-and-mouth disease, both caused by coxsackieviruses, produce discrete shallow ulcers on the posterior pharynx, soft palate and tonsillar pillars, with a briefer fever and a far less miserable child than gingivostomatitis. Aphthous stomatitis produces round, non-infectious ulcers without fever, usually on the movable oral mucosa. Oral candidiasis produces white plaques that scrape off rather than vesicles. The "anterior is HSV, posterior is coxsackie" rule resolves most cases at the bedside. [10] [1]
For the child with a vesicular rash, the differential includes varicella with its crops of all stages, impetigo with its honey-coloured crusts, contact dermatitis with its linear exposure pattern, and a bacterial superinfection of eczema. Eczema herpeticum is distinguished from bacterial eczema infection by the monomorphic, punched-out, painful erosions scattered across the eczematous skin, often with systemic upset out of proportion to the local findings. A child with atopic dermatitis and a rapidly worsening, painful, erosive rash has eczema herpeticum until proven otherwise. [12] [1]
For the febrile neonate, the differential that matters is the one that includes HSV. Bacterial sepsis and meningitis are the common framework, and enterovirus is a frequent mimic in the neonate, but neonatal HSV is the diagnosis that is missed because its early signs overlap with sepsis. A febrile, lethargic neonate in the first weeks of life, especially with a maternal history of genital HSV or a vesicle on the infant, earns HSV a place on the differential and a low threshold to investigate and treat. [2] [4]
For the child with encephalopathy and fever, herpes simplex encephalitis is the diagnosis that demands empirical treatment while others are excluded. Other viral encephalitides — enterovirus, arbovirus — autoimmune encephalitis, and metabolic or toxic encephalopathy all enter the differential, but the focal temporal-lobe presentation with fever and altered consciousness is treated as HSV until the CSF PCR returns. The cost of empirical aciclovir is low; the cost of a missed or delayed diagnosis is permanent neurological injury. [8] [2]
Clinical & Bedside Assessment
The assessment begins with a focused history built around the lesion and the host. For the child with gingivostomatitis, ask about oral intake, urine output and weight loss, because dehydration is the commonest reason for admission. For the neonate, establish the gestational age, the day of life, the maternal HSV history, the mode of delivery, the duration of rupture of membranes, and any skin, eye or mouth lesion on the infant. For the older child with encephalopathy, characterise the onset, the behavioural change and any seizure. [2] [10]
Establish the immune and atopic status precisely. Ask about atopic dermatitis, because it transforms a skin exposure into eczema herpeticum. Ask about chemotherapy, corticosteroids, transplantation and primary immunodeficiency, because these turn a self-limiting illness into a disseminated one. For the adolescent with genital disease, ask about sexual contacts, recent partners and any history of cold sores, because HSV-1 is now a recognised cause of genital herpes in young people. [1] [12]
Examine for the red flags that change disposition. In the child with gingivostomatitis, assess hydration — dry mucous membranes, sunken eyes, reduced skin turgor, capillary refill, and the wet-nappy count. In the neonate, examine the skin for vesicles, the eye for keratitis, and the nervous system for lethargy, irritability and seizures. In the older child, look for the focal neurological signs, the altered consciousness and the meningeal signs of encephalitis. In the atopic child, examine the distribution and character of the erosions. [3] [9]
Document the essentials that frame the response. Record the day of life, the presence and distribution of any lesion, the hydration status, and the neurological state. For the neonate, record the maternal history and the timeline of maternal lesions relative to delivery, because a primary maternal lesion near delivery is the highest-risk scenario. For the dehydrated child, record the weight, the intake and the urine output, so that rehydration can be tracked. A careful first encounter sets both the diagnosis and the trajectory of the illness. [2] [7]
Investigations
The diagnosis of primary gingivostomatitis in the typical case is clinical, and no test is needed. The combination of fever, a miserable child, painful anterior mouth ulcers, bleeding gums and cervical lymphadenopathy is sufficiently specific. Investigations are reserved for atypical presentations, severe or complicated disease, the neonate, and suspected central nervous system disease, where confirmation changes management. [10] [9]
When confirmation is needed, HSV PCR is the test of choice. For suspected herpes simplex encephalitis, send cerebrospinal fluid for HSV PCR, which is sensitive and specific, recognising that a very early sample can be falsely negative and that a repeat lumbar puncture is reasonable if the clinical picture persists. For suspected neonatal HSV, send surface swab PCR from the conjunctiva, oropharynx, rectum and any skin lesion, plus blood PCR, because the virus is often shed from multiple sites and a negative single swab does not exclude disease. [2] [8]
In Australia and Aotearoa New Zealand, CSF and surface PCR are the standard confirmatory tests for neonatal HSV and encephalitis. The Australian guidance and the equivalent New Zealand guidance set the maternal suppressive aciclovir pathway from 36 weeks, the caesarean recommendation for active genital lesions, and the structured assessment of the exposed neonate. Empirical high-dose intravenous aciclovir is started when neonatal HSV or encephalitis is plausible, before PCR returns. [1]
Type-specific serology has a limited role. It is most useful for epidemiology and for the pregnant woman whose genital HSV status is being assessed to plan suppression and mode of delivery. It is not the acute diagnostic tool, because antibody takes time to rise and does not distinguish old from new disease reliably at the bedside. In the pregnant adolescent with a first genital lesion, type-specific serology and PCR together frame the risk to the neonate. [1] [6]
For suspected herpes simplex encephalitis, the supportive bundle is as important as the PCR. A lumbar puncture — when safe — sends CSF for cell count (lymphocytic pleocytosis), protein (raised) and glucose (usually normal), alongside HSV PCR. An electroencephalogram may show periodic lateralised epileptiform discharges over a temporal lobe, and magnetic resonance imaging shows focal temporal-lobe signal change, often with haemorrhage. In suspected neonatal HSV, add liver function tests and a coagulation screen to detect hepatitis and disseminated intravascular coagulation, and a chest X-ray for pneumonitis. [8] [2]
For eczema herpeticum, confirm with a viral swab PCR of an erosion and send a bacterial swab to identify co-infection, because staphylococcal or streptococcal superinfection often accompanies the HSV. The investigation runs alongside, not instead of, the start of systemic aciclovir in the unwell child. [12] [1]
Management — Resuscitation
Resuscitation is about the high-risk or deteriorating host: the neonate with central nervous system or disseminated HSV, the child with herpes simplex encephalitis, and the child with severe eczema herpeticum. Each is a reason to admit, to monitor closely, and to start high-dose intravenous aciclovir promptly. The principle is that delaying antiviral therapy in the host who cannot contain the virus is the avoidable error, so the threshold to treat is low and the treatment is empirical. [2] [8]
Start high-dose intravenous aciclovir for neonatal HSV and for encephalitis without waiting for PCR when the clinical picture is compelling. The regimen is aciclovir 20 milligrams per kilogram per dose intravenously every eight hours, for fourteen days in skin-eye-mouth disease and for twenty-one days in central nervous system or disseminated disease. Intravenous rather than oral therapy achieves the central nervous system and tissue levels needed for these phenotypes, and hydration must be maintained to protect against aciclovir-induced nephrotoxicity. [8] [5]
Supportive care is the mainstay alongside antiviral therapy. In the dehydrated child with gingivostomatitis, give oral or intravenous rehydration, analgesia that is adequate to let the child drink, and attention to intake — because a child in pain will not drink, and a child who does not drink dehydrates. In neonatal disseminated disease, manage shock, coagulopathy and respiratory failure with fluids, blood products and ventilatory support as needed, and consult the paediatric intensive care unit early. [9] [4]
Manage seizures, airway and raised intracranial pressure in herpes simplex encephalitis directly, alongside the aciclovir. Anticonvulsants control seizures, and attention to airway, breathing and circulation supports the encephalopathic child. For eczema herpeticum, systemic aciclovir — oral if the child is well and the disease mild, intravenous if extensive, unwell or immunocompromised — is given with monitoring for dissemination and dermatology review. The common thread is that the high-risk host receives the treatment before the confirmation, not after. [8] [12]
Management — Definitive & Stepwise
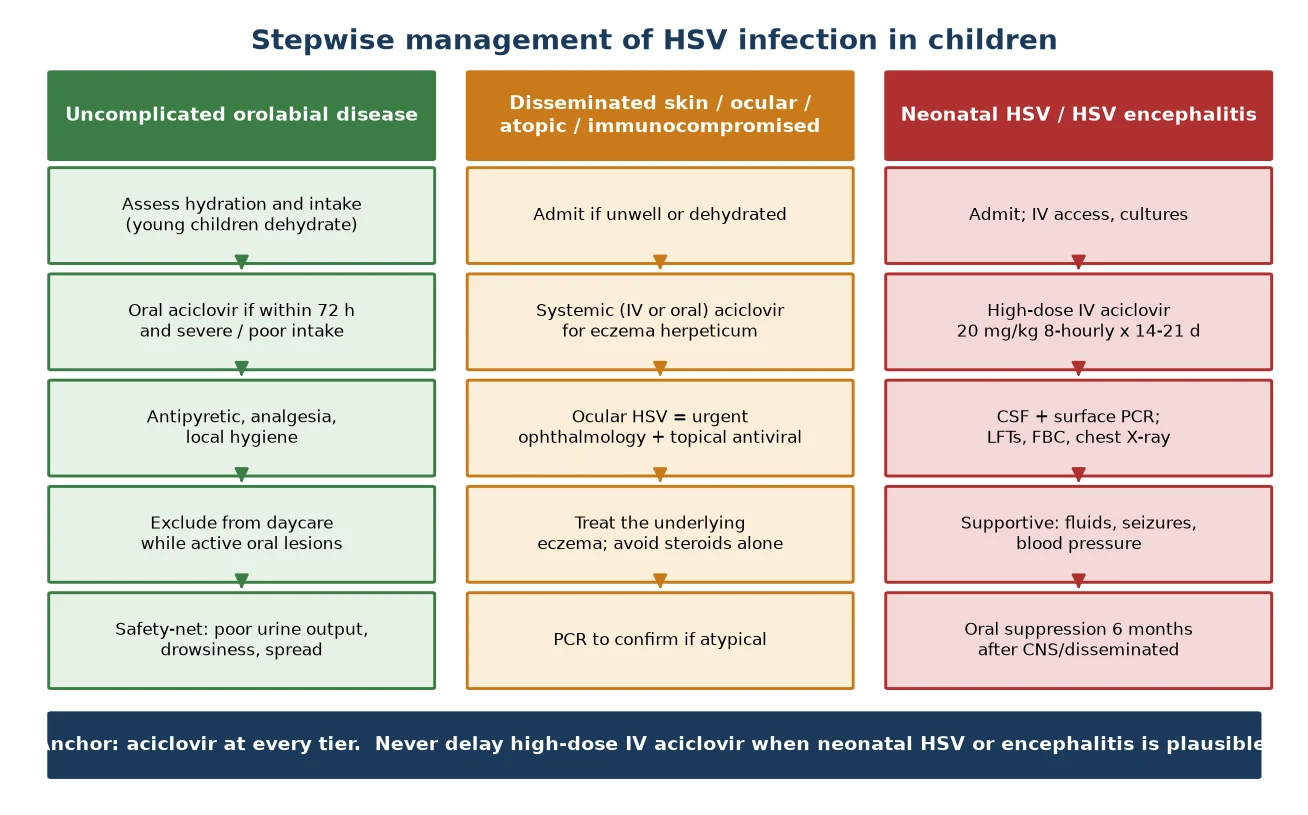
Definitive management is a stepwise pathway matched to the syndrome and the host-risk tier, with supportive care at one end, oral or intravenous aciclovir in the middle, and high-dose intravenous aciclovir at the other. The healthy child with uncomplicated orolabial disease receives supportive care with or without oral aciclovir; the atopic or immunocompromised child with cutaneous disease receives systemic aciclovir; and the neonate or the child with central nervous system disease receives high-dose intravenous aciclovir and post-treatment suppression. [1] [9]
The stepwise HSV pathway
Recognise the syndrome and set the host-risk tier at first contact: uncomplicated orolabial (supportive +/- oral aciclovir), cutaneous in the atopic or immunocompromised (systemic aciclovir), neonatal or CNS (high-dose IV aciclovir).
Primary gingivostomatitis: analgesia, hydration and local hygiene; consider oral aciclovir within 72 hours if severe or intake is poor; exclude from daycare while active oral lesions weep; safety-net for dehydration.
Eczema herpeticum: systemic aciclovir (oral if mild, IV if extensive or unwell); treat the underlying eczema; avoid topical calcineurin or steroid monotherapy during the acute HSV; review for dissemination.
Ocular HSV: urgent ophthalmology referral, topical antiviral (aciclovir ointment); never topical steroid without antiviral cover.
Neonatal HSV or encephalitis: admit, high-dose IV aciclovir 20 mg/kg 8-hourly for 14 days (SEM) or 21 days (CNS or disseminated); send CSF and surface PCR; maintain hydration; control seizures.
After neonatal CNS or disseminated disease: 6 months of oral aciclovir suppression to improve neurodevelopmental outcome, with neurodevelopmental and ophthalmology follow-up.
For the healthy child with primary gingivostomatitis, management is supportive and hydration-centred. Adequate analgesia — paracetamol, and sometimes a topical agent — lets the child drink, and oral or intravenous fluids restore hydration when intake has failed. Oral aciclovir has a defined role: the Amir et al. randomised trial and the Nasser et al. Cochrane review found that aciclovir started within seventy-two hours shortens the duration of illness and fever in primary gingivostomatitis, but the evidence to support routine use in every child is limited, and the decision is reserved for the severe presentation or the child whose intake is poor. [9] [11]
For recurrent herpes labialis, treatment is usually none at all, or a simple topical agent, in the healthy child. Oral aciclovir is reserved for frequent or severe recurrences or for the immunocompromised host, in whom suppressive therapy may be appropriate. The point is that recurrent disease is mild in the immunocompetent child and rarely warrants systemic therapy, while the immunocompromised host is the one for whom suppression transforms the clinical course. [1] [11]
For neonatal HSV and encephalitis, the regimen is high-dose intravenous aciclovir, twenty milligrams per kilogram per dose every eight hours, for fourteen days in skin-eye-mouth disease and twenty-one days in central nervous system or disseminated disease. After central nervous system or disseminated disease, six months of oral aciclovir suppression improves neurodevelopmental outcome, as the Kimberlin et al. New England Journal trial established. Hydration is maintained throughout to protect the kidneys, and the child is monitored for hepatitis, coagulopathy and pneumonitis. [5] [8]
For eczema herpeticum, systemic aciclovir is the anchor, oral for mild immunocompetent disease and intravenous for extensive, unwell or immunocompromised disease. The underlying eczema is treated to restore the skin barrier, but topical calcineurin inhibitors or topical steroid monotherapy are avoided during the acute HSV because they worsen the infection. Review for dissemination, and identify and treat any bacterial co-infection. For ocular HSV, urgent ophthalmology referral and topical antiviral are the core, and topical steroid is never given without antiviral cover because it promotes corneal ulceration. [12] [1]
Specific Subtypes & Scenarios
A young child with primary gingivostomatitis and dehydration. Assess intake and urine output, rehydrate orally or intravenously, give adequate analgesia, and consider oral aciclovir within seventy-two hours if the presentation is severe or intake is poor. Exclude from childcare while the oral lesions are active and weeping. The safety-net covers poor urine output, drowsiness and a spreading rash. Most children recover fully over ten to fourteen days. [9] [10]
A neonate with fever and lethargy in the first weeks of life. Hold HSV high on the differential, because neonatal HSV is missed when its early signs are attributed to bacterial sepsis. Send surface PCR swabs (conjunctiva, oropharynx, rectum, skin lesions), blood PCR, CSF PCR, liver function tests and coagulation, and start high-dose intravenous aciclovir while awaiting results if the picture is convincing. A febrile neonate with a vesicle, a seizure or hepatitis earns empirical aciclovir without hesitation. [2] [4]
A neonate with proven central nervous system or disseminated HSV. Give twenty-one days of high-dose intravenous aciclovir, followed by six months of oral aciclovir suppression, because suppression improves neurodevelopmental outcome after central nervous system or disseminated disease. Plan neurodevelopmental and ophthalmology follow-up, because the legacy of neonatal HSV is measured in long-term cognitive, motor and visual outcome. The prognosis is best for skin-eye-mouth disease and worst for disseminated disease. [5] [3]
A child with herpes simplex encephalitis. Start high-dose intravenous aciclovir for twenty-one days, confirm with CSF PCR, electroencephalogram and magnetic resonance imaging, and control seizures and raised intracranial pressure alongside the antiviral. The outcome depends on the level of consciousness at presentation and the delay to aciclovir, so treat before the PCR returns when the picture fits. Rehabilitation and prolonged follow-up address the cognitive and behavioural legacy of temporal-lobe injury. [8] [2]
A child with atopic dermatitis and a rapidly spreading erosive rash. This is eczema herpeticum, a dermatological emergency. Give systemic aciclovir — oral if mild and the child is well, intravenous if extensive, unwell or immunocompromised — confirm with a viral swab PCR, send a bacterial swab, treat the underlying eczema, and review for dissemination. Never treat with topical steroid alone, because that worsens the HSV. [12] [1]
An adolescent with genital HSV. Confirm with PCR, treat the episode with oral aciclovir, and counsel about transmission and the future risk to a neonate. For frequent recurrences, suppressive oral aciclovir reduces the frequency and the shedding. The adolescent who may become pregnant is the one for whom suppression and disclosure of HSV status matter most, because genital HSV in pregnancy is the gateway to neonatal disease. [1] [6]
Complications & Pitfalls
Dehydration is the commonest complication of primary gingivostomatitis, driven by pain and refusal to drink in the young child. The child who has stopped drinking arrives with a dry mouth, sunken eyes and reduced skin turgor, and needs rehydration, sometimes intravenous. The pitfall is focusing on the ulcer and missing the intake; the management is to assess hydration at every encounter and to admit when oral intake fails. [9] [10]
Neonatal HSV carries the heaviest burden of severe morbidity and mortality. Disseminated disease presents as a sepsis-like illness with hepatitis, pneumonitis and coagulopathy, and central nervous system disease presents with seizures and encephalopathy. The mortality and long-term neurodevelopmental disability remain substantial even with high-dose aciclovir, which is why early empirical treatment and post-treatment suppression are non-negotiable. The biggest pitfall is missing the diagnosis by attributing early signs to bacterial sepsis. [3] [4]
Herpes simplex encephalitis is the most devastating complication of HSV in the older child. The haemorrhagic, necrotising temporal-lobe process produces permanent neurological injury, and the outcome depends on the level of consciousness at presentation and the delay to aciclovir. The pitfall is attributing behavioural change to a viral prodrome or febrile delirium, or waiting for the PCR before treating. The correct approach is empirical high-dose aciclovir as soon as the picture is plausible. [8] [2]
Eczema herpeticum is the cutaneous emergency of HSV in the atopic child. Widespread, painful, monomorphic erosions across broken skin can disseminate and become secondarily infected, and the pitfall is treating the apparent eczema flare with more topical steroid. The correct response is to recognise the monomorphic punched-out erosions, stop the topical steroid, and give systemic aciclovir. HSV keratitis, likewise, is an ocular emergency: a dendritic ulcer on fluorescein staining threatens corneal scarring and vision loss, and topical steroid without antiviral cover worsens it. [12] [1]
The recurring pitfall across all severe HSV is delay. Delay in starting high-dose aciclovir for neonatal HSV, for encephalitis, and for eczema herpeticum is the single most avoidable source of harm, because outcome worsens with every hour. Risk-tier and syndrome recognition at the first encounter — setting the threshold to treat empirically in the neonate, the brain and the broken skin — is the safeguard. The healthy-child supportive default applied to these hosts is the dangerous error the fellowship examiner probes. [2] [8]
Prognosis & Disposition
Most healthy children with primary gingivostomatitis recover fully over ten to fourteen days, with morbidity driven by pain, poor intake and dehydration, and full recovery expected. The disposition is usually home management with adequate analgesia, a hydration plan and a clear safety-net, and admission reserved for the child whose oral intake has failed. Recurrent herpes labialis in the immunocompetent host is a mild nuisance that resolves over days. [10] [9]
The severe morbidity and the mortality are concentrated in the high-risk hosts. Neonatal disseminated and central nervous system disease carry the highest mortality and the most long-term neurodevelopmental disability, while skin-eye-mouth disease has the best prognosis when treated early. Herpes simplex encephalitis leaves a legacy of cognitive, behavioural and seizure burden that scales with the delay to treatment. This concentration of harm is why every management strategy and every prevention effort ultimately aims to protect the neonate and the brain. [3] [8]
Disposition follows the syndrome and the risk tier. Manage at home, with a hydration plan and follow-up, the healthy child with uncomplicated gingivostomatitis and good intake. Admit to the ward the dehydrated child, the child needing intravenous aciclovir for eczema herpeticum, and the neonate on treatment. Admit to the paediatric intensive care unit the neonate with disseminated disease and the child with encephalitis and raised intracranial pressure. The threshold for admitting a high-risk or deteriorating host is deliberately low. [2] [4]
At discharge, complete the antiviral course and the six months of oral suppression where indicated — after neonatal central nervous system or disseminated disease. Arrange neurodevelopmental and ophthalmology follow-up for the neonate, because the legacy of HSV is measured in long-term outcome. Give the family a clear safety-net for recurrence, deterioration, poor feeding or seizure. The discharge encounter is also a prevention opportunity: address the maternal-neonatal pathway for any future pregnancy, and counsel the adolescent about transmission. [5] [7]
The long-term consequence of primary HSV infection is lifelong latency with the possibility of recurrent disease at the original site. For most children this means the occasional cold sore; for the few who experience severe neonatal or central nervous system disease, it means a measured, watched recovery. Reinfection with a different strain is uncommon, and recurrence is reactivation of the latent original infection. [1] [8]
Special Populations
Neonates are the highest-risk group for severe HSV. The majority acquire the virus intrapartum from maternal genital HSV, and the immature immune system permits dissemination. They require high-dose intravenous aciclovir, surface and CSF PCR, a full duration of treatment, and six months of oral suppression after central nervous system or disseminated disease, with neurodevelopmental follow-up. A primary maternal genital infection near delivery is the highest-risk scenario and the one that drives the preventive pathway. [2] [6]
Pregnant adolescents and women with genital HSV carry a risk to the neonate that is reduced by prevention. Maternal suppressive aciclovir from 36 weeks reduces viral shedding and the risk of a lesion at delivery, and caesarean delivery is recommended when active genital lesions are present. The asymptomatic neonate exposed at delivery is managed by the structured Kimberlin-Baley pathway of the American Academy of Pediatrics, which sets the surveillance, sampling and empirical-treatment thresholds. Pre-conception counselling and suppressive therapy are the durable prevention. [7] [6]
Children with atopic dermatitis are at risk of eczema herpeticum, because the broken skin barrier invites HSV dissemination. Treat with systemic aciclovir and address the underlying eczema to restore the barrier, and avoid topical calcineurin or steroid monotherapy during the acute HSV. The family is taught to recognise the monomorphic punched-out erosions and to present early, because early aciclovir shortens the episode and prevents dissemination. [12] [1]
Immunocompromised children are at risk of severe, prolonged and recurrent HSV. The threshold for intravenous aciclovir and for suppressive therapy is lower, and aciclovir-resistant HSV is considered in refractory disease. These children depend on prevention around them, and household awareness of cold sore hygiene protects the immunocompromised child from a recurrent exposure. [1] [8]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children, and refugee, asylum-seeking and migrant families may face barriers to timely diagnosis, treatment and the maternal-neonatal prevention pathway. Ensure culturally safe, equitable access to PCR, aciclovir and follow-up, treat actively when disease is suspected, and use trained interpreters rather than family members. Disadvantage should never be the reason a neonatal HSV diagnosis is delayed or a maternal suppression pathway is missed. [2] [4]
Rural and remote neonates and children need timely access to PCR, aciclovir and retrieval, often through outreach and telehealth, because distance can delay the care that a sick neonate or an encephalopathic child cannot afford to wait for. The plan for a remote family accounts for what is locally available, and retrieval is mobilised early when a high-risk host deteriorates. [7] [2]
Evidence, Guidelines & Regional Differences
The comprehensive framing of HSV epidemiology, transmission and prevention is the Corey and Wald New England Journal review of maternal and neonatal HSV infections. It sets the biology of latency and reactivation, the maternal-primary-versus-recurrent transmission risk, and the rationale for suppressive therapy and caesarean delivery. It is the reference against which the clinical and preventive strategy is read. [1]
The evidence for oral aciclovir in primary gingivostomatitis rests on the Amir et al. randomised double-blind placebo-controlled trial, which showed that aciclovir started early shortens fever and illness, and on the Nasser et al. Cochrane review, which synthesised the limited evidence and found a role for early treatment in severe disease but insufficient evidence for routine use in every child. Together they frame the selective use of oral aciclovir in the severe or poorly-intaking child rather than a blanket recommendation. [9] [11]
Oral acyclovir suppression after neonatal HSV disease
Population: Randomised, placebo-controlled trial of infants who had completed parenteral aciclovir treatment for neonatal CNS or disseminated HSV disease, assigned to six months of oral aciclovir suppression versus placebo, with neurodevelopmental assessment at twelve months.
Key finding
Infants who received six months of oral acyclovir suppression had better neurodevelopmental outcomes at twelve months than those who received placebo, with improved Bayley mental-development scores. Neutropenia was a recognised side effect that required monitoring.
Practice change
Six months of oral aciclovir suppression after neonatal CNS or disseminated HSV disease improves neurodevelopmental outcome. This evidence underpins the post-treatment suppression that is now standard of care, with blood-count monitoring for neutropenia.
The contemporary synthesis of neonatal HSV diagnosis and management is set out in the Pinninti and Kimberlin, James and Kimberlin, and Samies, James and Kimberlin reviews. They describe the high-dose aciclovir regimen, the PCR-based diagnostic strategy, the three disease classes and their prognoses, and the post-treatment suppression, and they form the evidence base for the AAP Red Book neonatal HSV chapter. The James, Kimberlin and Whitley review of antiviral therapy for herpesvirus central nervous system infections frames the parallel management of neonatal HSV and herpes simplex encephalitis. [2] [8]
The structured neonatal exposure pathway is the Kimberlin and Baley guidance of the American Academy of Pediatrics, which sets the surveillance, sampling and empirical-treatment thresholds for the asymptomatic neonate born to a woman with active genital herpes lesions. It is the standard against which the exposed-neonate assessment is run, and it balances the cost of over-treatment against the catastrophe of a missed neonatal HSV. The Hsu et al. nationwide cohort describes the epidemiology of hospitalised eczema herpeticum in children, underlining its importance as a dermatological emergency. [7] [12]
The regional policy structure is consistent in principle and varies in detail. In ANZ, the Australian guidance and the New Zealand schedule set the maternal suppressive aciclovir pathway from 36 weeks, the caesarean recommendation for active genital lesions, and the structured exposed-neonate assessment, and empirical high-dose intravenous aciclovir is started when neonatal HSV or encephalitis is plausible. In the UK, the National Institute for Health and Care Excellence and the Green Book frame the maternal and neonatal management, and the Royal College of Paediatrics and Child Health guidance underlines the low threshold for empirical aciclovir in the febrile neonate. In the US, the American Academy of Pediatrics Red Book and the Centers for Disease Control and Prevention set the high-dose aciclovir regimen, the suppression and the Kimberlin-Baley exposed-neonate pathway. In Canada, the Canadian Paediatric Society and the Canadian guidelines deliver the equivalent strategy. The principle everywhere is that aciclovir is the anchor, and the maternal-neonatal pathway prevents the disease. [1] [7]
The controversies are real and active: the optimal threshold for HSV testing and empirical aciclovir in the febrile neonate, weighed against cost and resistance; the role of universal maternal HSV screening in pregnancy; the duration of suppression after neonatal disease; and the management of the asymptomatic neonate exposed at delivery. The defence against each is the same: a low threshold to test and treat the high-risk host, a structured maternal-neonatal pathway, and the recognition that the cost of a missed or delayed HSV is measured in lives and brains. [2] [8]
Exam Pearls
- HSV-1 causes most childhood orolabial and CNS disease; HSV-2 causes most genital and neonatal HSV — but HSV-1 neonatal disease is increasingly recognised. [1]
- The commonest primary HSV-1 presentation in children is acute herpetic gingivostomatitis — fever, painful anterior mouth ulcers, drooling, refusal to drink. [10]
- "Anterior is HSV, posterior is coxsackie" — gingivostomatitis strikes the gums and anterior mouth; herpangina strikes the posterior pharynx. [9]
- Neonatal HSV has three disease classes — skin-eye-mouth (best prognosis), CNS, disseminated (worst) — most acquired intrapartum from often-asymptomatic maternal genital HSV. [3]
- High-dose IV aciclovir for neonatal HSV and encephalitis: aciclovir 20 mg/kg/dose 8-hourly, for 14 days (SEM) or 21 days (CNS or disseminated), then 6 months oral suppression after CNS or disseminated disease. [8] [5]
- CSF HSV PCR is the diagnostic test for encephalitis; MRI shows temporal-lobe signal change and EEG shows periodic lateralised epileptiform discharges. [8]
- Eczema herpeticum is a dermatological emergency — monomorphic punched-out erosions in atopic skin, systemic aciclovir, never topical steroid alone. [12]
- Ocular HSV (dendritic keratitis) is a vision threat — urgent ophthalmology and topical antiviral; never topical steroid without antiviral cover. [1]
- Maternal suppressive aciclovir from 36 weeks and caesarean for active genital lesions reduce neonatal HSV; the asymptomatic exposed neonate is managed by the AAP Kimberlin-Baley pathway. [6] [7]
- Never delay high-dose IV aciclovir when neonatal HSV or encephalitis is plausible — outcome worsens with every hour of delay. [2] [8]
References
- [1]Corey L; Wald A Maternal and neonatal herpes simplex virus infections. N Engl J Med, 2009.PMID 19797284
- [2]Pinninti SG; Kimberlin DW Neonatal herpes simplex virus infections. Semin Perinatol, 2018.PMID 29544668
- [3]James SH; Kimberlin DW Neonatal Herpes Simplex Virus Infection. Infect Dis Clin North Am, 2015.PMID 26154662
- [4]Samies NL; James SH; Kimberlin DW Neonatal Herpes Simplex Virus Disease: Updates and Continued Challenges. Clin Perinatol, 2021.PMID 34030813
- [5]Kimberlin DW; Whitley RJ; Wan W; Powell DA; et al Oral acyclovir suppression and neurodevelopment after neonatal herpes. N Engl J Med, 2011.PMID 21991950
- [6]Pinninti SG; Kimberlin DW Preventing herpes simplex virus in the newborn. Clin Perinatol, 2014.PMID 25459782
- [7]Kimberlin DW; Baley J; Committee on Infectious Diseases; Committee on Fetus and Newborn Guidance on management of asymptomatic neonates born to women with active genital herpes lesions. Pediatrics, 2013.PMID 23359576
- [8]James SH; Kimberlin DW; Whitley RJ Antiviral therapy for herpesvirus central nervous system infections: neonatal herpes simplex virus infection, herpes simplex encephalitis, and congenital cytomegalovirus infection. Antiviral Res, 2009.PMID 19414035
- [9]Amir J; Harel L; Smetana Z; Varsano I Treatment of herpes simplex gingivostomatitis with aciclovir in children: a randomised double blind placebo controlled study. BMJ, 1997.PMID 9224082
- [10]Amir J; Harel L; Smetana Z; Varsano I The natural history of primary herpes simplex type 1 gingivostomatitis in children. Pediatr Dermatol, 1999.PMID 10469407
- [11]Nasser M; Fedorowicz Z; Khoshnevisan MH; Shahiri Tarestani M Acyclovir for treating primary herpetic gingivostomatitis. Cochrane Database Syst Rev, 2008.PMID 18843726
- [12]Hsu DY; Shinkai K; Silverberg JI Epidemiology of Eczema Herpeticum in Hospitalized U.S. Children: Analysis of a Nationwide Cohort. J Invest Dermatol, 2018.PMID 28927889