Paeds · infectious-diseases
HIV exposure and infection in children
Also known as Paediatric HIV · Perinatally-acquired HIV · Vertically-transmitted HIV in children · HIV-exposed infant (HEU) · Mother-to-child HIV transmission
Fellowship topic on HIV exposure and infection in children: mother-to-child transmission in utero, intrapartum and through breastfeeding and how combination ART compresses each; the PMTCT cascade from maternal ART (Option B+) through infant nevirapine prophylaxis to early infant PCR diagnosis; the distinction between HIV exposure and HIV infection (maternal IgG versus infant viraemia); rapid infant progression and the survival benefit of immediate ART; HIV DNA/RNA PCR as the diagnostic test under 18 months; cotrimoxazole prophylaxis and the prevention of Pneumocystis pneumonia; WHO clinical staging and CD4-based immunological staging; the HIV-exposed-uninfected infant; opportunistic infection, failure to thrive and HIV encephalopathy; feeding decisions, family testing and adolescent transition; and WHO, CDC, PENTA and ANZ/UK/US/Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Why the baby's antibody test is meaningless
Overview & Definition
Picture a six-week-old baby brought to clinic for the routine immunisation visit. The mother is HIV-positive and on antiretroviral therapy, her viral load was suppressed at delivery, and the baby received nevirapine for six weeks. A single antibody test on this baby would be positive — yet the baby may well be uninfected. The skill of the paediatrician is to hold exposure and infection apart, to test for the virus rather than the antibody, and to run the cascade that either confirms infection and starts treatment, or proves the baby is uninfected and closes the chapter. [7] [1]
Human immunodeficiency virus (HIV) in the child is almost always acquired vertically — from an HIV-positive mother during pregnancy, at delivery, or through breastfeeding. A smaller share is acquired through blood products, sexual contact, or, in adolescents, horizontal routes. The defining clinical fact is that exposure and infection are not the same: an HIV-exposed infant is born to a positive mother but may be uninfected, and only nucleic-acid testing can tell the two apart in the first 18 months of life. [4] [7]
The clinician's work runs on three layers. The acute layer recognises and treats the failing child — the infant with Pneumocystis pneumonia, the wasted toddler with chronic diarrhoea, the adolescent with advanced disease. The definitive layer diagnoses infection by PCR, starts ART immediately, and delivers cotrimoxazole, nutrition and opportunistic-infection care. The preventive layer runs the PMTCT cascade — maternal lifelong ART, an undetectable viral load, infant prophylaxis, safe feeding and structured follow-up — because the child who never acquires infection is the child the programme has protected. [1] [10]
Classification
Sort paediatric HIV the way it presents at the bedside — by whether the child is exposed or infected, by when the virus crossed from mother to child, and by how advanced the disease has become. The first axis is exposure versus infection. An HIV-exposed, uninfected infant (HEU) is born to an infected mother but has no detectable virus; an HIV-infected infant has virus confirmed by PCR; and an indeterminate infant has a borderline or unconfirmed early result that must be resolved by repeat testing. [7] [6]
The second axis is the timing of mother-to-child transmission. Virus may cross in utero in late pregnancy, during delivery through contact with maternal blood and secretions, or postpartum through breastfeeding. In an untreated mother the split is roughly 5–10% in utero, 10–20% intrapartum, and 5–20% through breastfeeding, and combination maternal ART plus infant prophylaxis compress each of these windows. The timing matters because it determines when a negative PCR becomes reliable and when follow-up must continue. [2] [3]
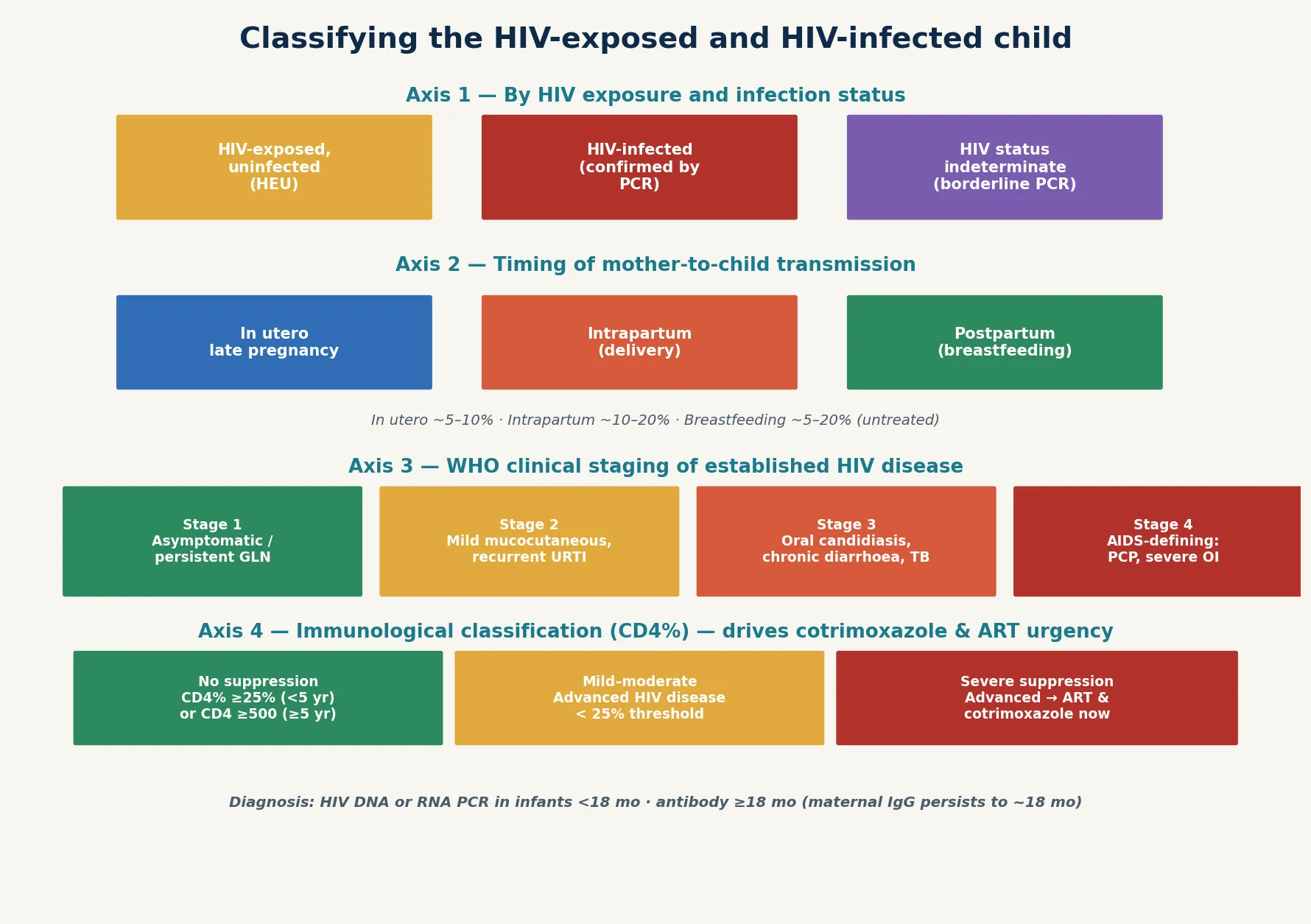
The third and fourth axes apply to the child with established disease. WHO clinical staging runs from stage 1 (asymptomatic or persistent generalised lymphadenopathy) through mild and moderate disease to stage 4 (AIDS-defining illness such as Pneumocystis pneumonia, severe recurrent infection or HIV encephalopathy). Immunological staging uses the CD4 percentage and absolute count, and together the two axes drive the urgency of cotrimoxazole prophylaxis and ART. Even under the current treat-all strategy, staging still frames prognosis and the risk of opportunistic infection. [8] [5]
Epidemiology & Risk Factors
Where does paediatric HIV sit, and who does it hurt? The global burden falls overwhelmingly on children in resource-limited settings, where the mother-to-child transmission rate without intervention is 25–45% in breastfeeding populations. In Australia and Aotearoa New Zealand the universal offer of antenatal HIV screening, combined with maternal ART and infant prophylaxis, has driven transmission to under 2%, and perinatally-acquired infection is now rare. Understanding who is at risk directs both acute care and prevention. [4] [7]
The dominant risk factor at the individual level is an unsuppressed maternal viral load at delivery. A mother who is not on ART, who started late in pregnancy, who has poor adherence, or who acquires HIV during pregnancy transmits far more readily than a fully suppressed mother. This single variable is the strongest predictor of transmission, and it is the reason the strategy is built around maternal viral suppression. [2] [3]
Infant and delivery factors raise transmission further. Prematurity, vaginal delivery with a high viral load, prolonged rupture of membranes, invasive obstetric procedures, and mixed (rather than exclusive replacement) feeding in the untreated setting all increase the chance the virus crosses. A baby born at the margin of the cascade — early, to a newly diagnosed or viraemic mother, with late prophylaxis — is the baby at greatest risk, and the one for whom a birth PCR and extended infant prophylaxis are most important. [7] [3]
Perinatally-infected infants progress far faster than adults. A pooled analysis of African cohorts found that roughly half of untreated, vertically-infected infants developed AIDS or died by two years of age, a trajectory far steeper than adult disease. This rapid progression is the biological justification for treating every infected infant immediately rather than waiting for clinical or immunological decline. [4] [1]
A growing population is the HIV-exposed-uninfected (HEU) infant. As PMTCT succeeds, the number of infected children falls and the number of exposed-uninfected children rises, and these infants carry higher infectious-morbidity and mortality than unexposed peers — a reflection of immune immaturity, prematurity, antiretroviral exposure and social determinants. The HEU child is not simply "well", and deserves the same thorough follow-up. [6] [9]
Pathophysiology
Why does a virus that infects a single cell type dismantle a child's entire immune defence? HIV is a retrovirus — principally HIV-1, with HIV-2 confined mainly to West Africa — whose envelope glycoprotein gp120 binds the CD4 receptor and a co-receptor (chiefly CCR5 in early infection) to enter CD4-positive T-lymphocytes, monocytes, macrophages and dendritic cells. Binding and entry are the first act of a lifelong infection. [8] [4]
Once inside, the virus uses its reverse transcriptase to copy RNA into DNA, and that proviral DNA integrates into the host genome. The infected cell becomes a permanent factory for new virus particles, which is why antiretrovirals control but do not cure infection — the integrated provirus persists. This integration is also why treatment, once started, is for life. [8] [10]
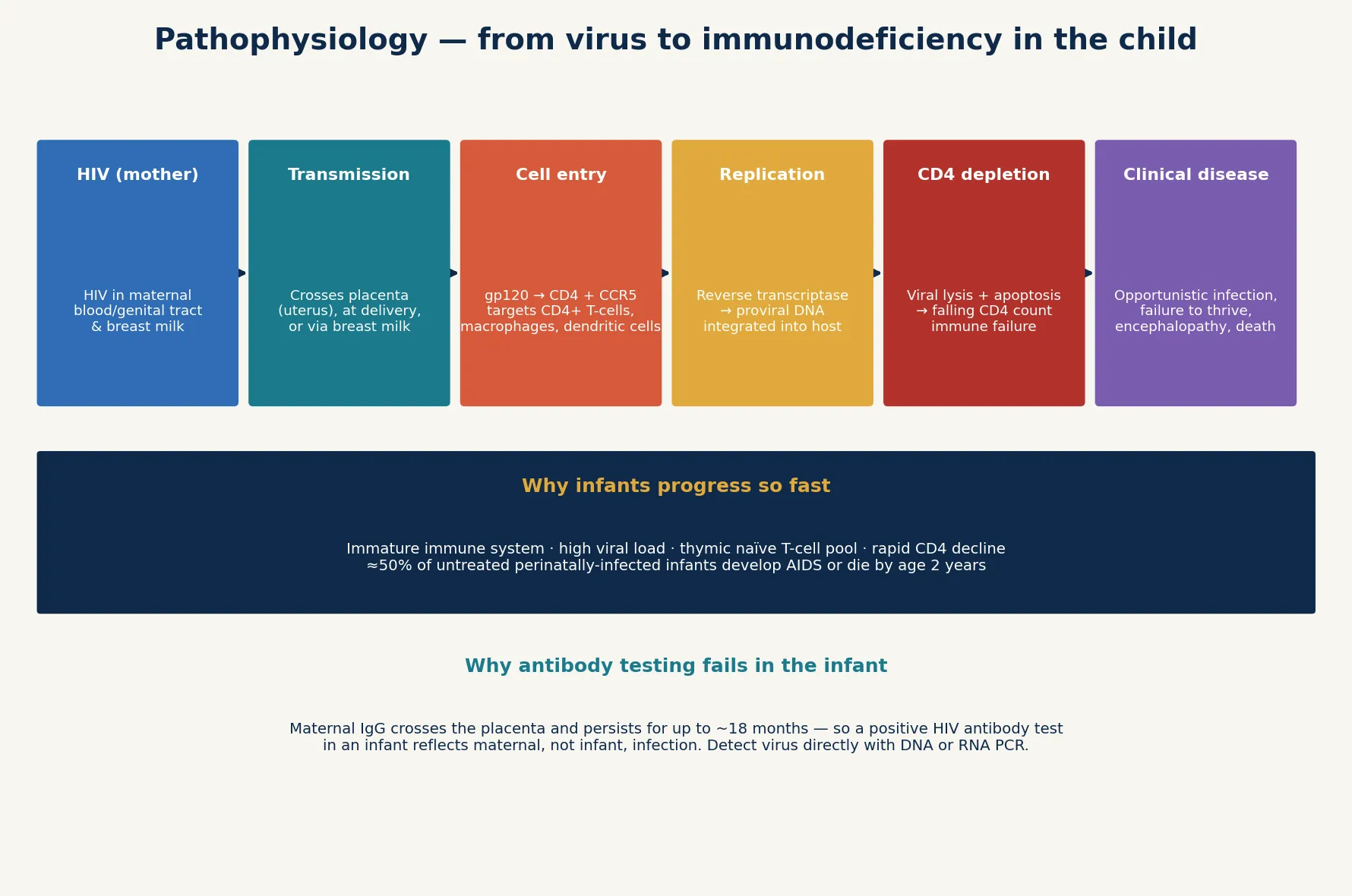
The clinical disease follows from progressive CD4-positive T-cell loss. Viral lysis, cell-to-cell fusion, apoptosis and immune-mediated killing together deplete the helper T-cell pool, so the child loses the capacity to mount the coordinated immune response that holds opportunistic organisms in check. The result is Pneumocystis pneumonia, chronic candidiasis, severe bacterial infection, chronic diarrhoea, failure to thrive, and HIV encephalopathy. [8] [4]
Infants progress faster than adults for biological reasons. The immature immune system, the large thymic pool of susceptible naïve T-cells, and a high viral set-point together drive a more rapid CD4 decline and earlier AIDS. The same virus that takes a decade to sicken an adult can sicken an infant within months, which is why the strategy treats infants at the moment of diagnosis rather than at a CD4 threshold. [4] [1]
The diagnostic consequence follows directly. Because maternal IgG crosses the placenta and persists in the infant's blood for up to 18 months, a positive HIV antibody test in a baby reflects the mother, not the child. To diagnose infection you must detect the virus itself — by HIV DNA or RNA PCR — and a single positive must be confirmed with a second sample before the child is labelled infected. Antibody testing becomes reliable only after maternal antibody has cleared, at around 18 months. [7] [8]
Clinical Presentation
The early infant presentation of perinatal HIV is often subtle and non-specific, which is exactly why it is missed. Failure to thrive despite adequate intake, chronic diarrhoea, recurrent bacterial infection, oral candidiasis that persists beyond infancy, generalised lymphadenopathy, hepatosplenomegaly and chronic parotitis are the quiet signs of a virus steadily dismantling the immune system. None is dramatic on its own, but together they form a pattern that should prompt a PCR. [8] [4]
The severe presentations are the ones that bring the undiagnosed child to acute care. Pneumocystis jirovecii pneumonia presents as a rapidly progressive, hypoxic interstitial pneumonia in an infant, classically aged three to six months, with tachypnoea, hypoxaemia and diffuse infiltrates but often a paucity of auscultatory findings. Severe bacterial infection or sepsis, chronic diarrhoea and wasting, and HIV encephalopathy with developmental delay, regression or loss of milestones are the other catastrophic modes of presentation. [8] [1]
The clinical triggers that should prompt testing of an untested or incompletely tested child are the pattern-recognition cues of paediatric HIV: failure to thrive despite adequate feeding, recurrent or severe infection, persistent oral candidiasis beyond infancy, chronic parotitis, lymphoid interstitial pneumonitis, and any atypical or severe opportunistic infection. In an older child, chronic skin disease, chronic diarrhoea and developmental delay complete the picture. [8] [7]
The HIV-exposed-uninfected infant presents differently — usually with recurrent minor infection, sequelae of prematurity, or feeding difficulty — and the trap is to attribute every illness to the exposure status. A HEU infant who is genuinely failing must still be investigated for non-HIV causes, and infection must still be actively excluded by PCR rather than assumed absent. [6] [7]
Differential Diagnosis
For the failing-to-thrive HIV-exposed infant, the differential spans inadequate intake, gastro-oesophageal reflux, malabsorption, chronic infection, and endocrine or metabolic disease — and HIV itself. The point of separation is the PCR: exposure alone does not cause failure to thrive, and a positive antibody test in an infant never establishes infection. The failing exposed infant is investigated for both HIV and the ordinary causes of poor growth. [7] [4]
For the child with recurrent or chronic infection, the differential is the immunodeficiency differential: primary immunodeficiency (combined immunodeficiency, antibody deficiency, complement defects), secondary immunodeficiency (malnutrition, malignancy, iatrogenic immunosuppression), and HIV. The maternal and exposure history and the PCR are decisive, because the patterns overlap and a child can have more than one problem at once. [8] [6]
For chronic diarrhoea and wasting, the differential includes chronic enteric infection (cryptosporidium, cytomegalovirus, mycobacterium avium complex), tuberculosis, coeliac disease, cystic fibrosis and HIV enteropathy. The exposure history, the PCR, and targeted stool and imaging studies separate them, and the wasted child often needs nutritional support while the workup proceeds. [8] [7]
Clinical & Bedside Assessment
The assessment begins with a focused history built around growth, feeding and infection. Plot the weight and length trajectory, ask about feeding type and tolerance, the stool pattern, and the frequency, type and severity of infections. Then establish the maternal and infant treatment history in detail: the mother's ART and viral load in pregnancy and at delivery, the mode of delivery, the infant's antiretroviral prophylaxis, the feeding choice, and every HIV PCR result with its date. The gap between exposure and confirmed infection is where errors occur, so this history must be precise. [7] [3]
Examine the child carefully for failure to thrive, opportunistic disease and the red flags of severe illness. Plot growth parameters, look for oral candidiasis, generalised lymphadenopathy, hepatosplenomegaly, chronic parotitis, skin disease and neurological signs, and assess the respiratory system for the distress and hypoxia that signal severe pneumonia. An exposed or infected infant can look deceptively well between illnesses, so the examination must be complete each visit. [8] [1]
Assess the acutely unwell infant for the time-critical emergencies. Severe hypoxic pneumonia raises Pneumocystis; sepsis and severe bacterial infection raise advanced immunodeficiency; dehydration and electrolyte disturbance complicate chronic diarrhoea; and neurological decline signals encephalopathy or an opportunistic central-nervous-system process. The child with advanced HIV can deteriorate rapidly, so the threshold for admission and aggressive workup is deliberately low. [8] [4]
Address the family and psychosocial frame at the bedside. The mother's own health and engagement in care, the partner and sibling testing status, the disclosure plan, the feeding decision, and the social and cultural context all shape adherence and follow-up. A technically correct plan fails if the family is not supported, so the bedside assessment extends deliberately into the social determinants of care. [6] [7]
Investigations
HIV DNA or RNA nucleic-acid testing (PCR) is the diagnostic test in infants under 18 months, because antibody is uninterpretable while maternal IgG persists. A positive result must be confirmed with a second PCR on a separate sample before the child is labelled infected, and a negative result early does not exclude infection acquired later through breastfeeding. The PCR is the single most important test in the exposed infant, and its timing is governed by the exposure and feeding context. [7] [8]
The standard schedule for early infant diagnosis is a PCR at four to six weeks of age, with a birth PCR added for high-risk infants (those born to unsuppressed or newly diagnosed mothers) and repeat testing at risk points through the breastfeeding period. A final HIV antibody test at 18–24 months confirms the exposed infant is uninfected after maternal antibody has cleared. The cascade is only complete when the last test is negative. [7] [3]
For the infected child, CD4 count and percentage and the HIV viral load (RNA) stage the immunosuppression, guide the urgency of cotrimoxazole and ART, and monitor the response to treatment. The goal of ART is viral load suppression to undetectable, and persistent viraemia signals adherence failure, resistance or both. A CD4 percentage below age-specific thresholds flags advanced disease and a higher opportunistic-infection risk. [5] [8]
In Australia and Aotearoa New Zealand, antenatal HIV screening is universally offered, and the ASHM (Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine) guidance directs the management of the exposed infant: HIV DNA/RNA PCR at birth where high-risk, at six weeks and at the appropriate interval after exposure ends, with a confirmatory antibody at 18–24 months. Cotrimoxazole prophylaxis begins at four to six weeks in infants whose infection has not been excluded, and specialist paediatric HIV services oversee ART. [7]
Targeted tests for opportunistic disease round out the workup as the clinical picture demands. A chest X-ray and, where available, induced sputum or nasopharyngeal wash investigate Pneumocystis; a tuberculosis workup is essential in endemic settings; stool studies address chronic diarrhoea; and blood culture, full blood count and lactate are sent where sepsis or drug toxicity is suspected. The laboratory workup follows the clinical question, not a fixed panel. [8] [4]
Management — Resuscitation
Resuscitation is about the acutely unwell HIV-exposed or infected infant, and the first emergency is severe hypoxic pneumonia. An infant with respiratory distress, hypoxaemia and diffuse infiltrates — born to an HIV-positive or untested mother — has Pneumocystis pneumonia until proven otherwise. Give supplemental oxygen, admit for monitoring, and start empiric high-dose co-trimoxazole with a corticosteroid for moderate–severe disease while the diagnosis is confirmed. Delay in starting treatment is the preventable cause of death. [8] [1]
Sepsis and severe bacterial infection are managed with broad-spectrum antibiotics guided by local resistance and culture, with the recognition that an immunodeficient child may be bacteraemic with an atypical or resistant organism. Dehydration and electrolyte disturbance from chronic diarrhoea are corrected with cautious rehydration, and the wasted or failing child receives nutritional support. The resuscitation bundle targets the immediate threats to life while the underlying diagnosis is secured. [8] [4]
Nutrition is part of resuscitation in the failing child, because failure to thrive is both a presentation and a driver of immune failure. High-energy feeding, treatment of oral and enteric infection, and nasogastric or specialist nutrition support rebuild the substrate the immune system needs to recover. A child who is malnourished and infected will not respond to ART alone, so nutrition runs in parallel with the acute medical treatment. [4] [8]
Once the infant is stable and the diagnosis is confirmed, start cotrimoxazole prophylaxis and antiretroviral therapy without delay. The survival benefit of early ART in infancy is large and time-sensitive, and the CHER trial showed that treating asymptomatic infants reduced mortality by roughly three-quarters. Waiting for clinical or immunological decline before treating is an obsolete and dangerous stance. [1] [5]
Management — Definitive & Stepwise
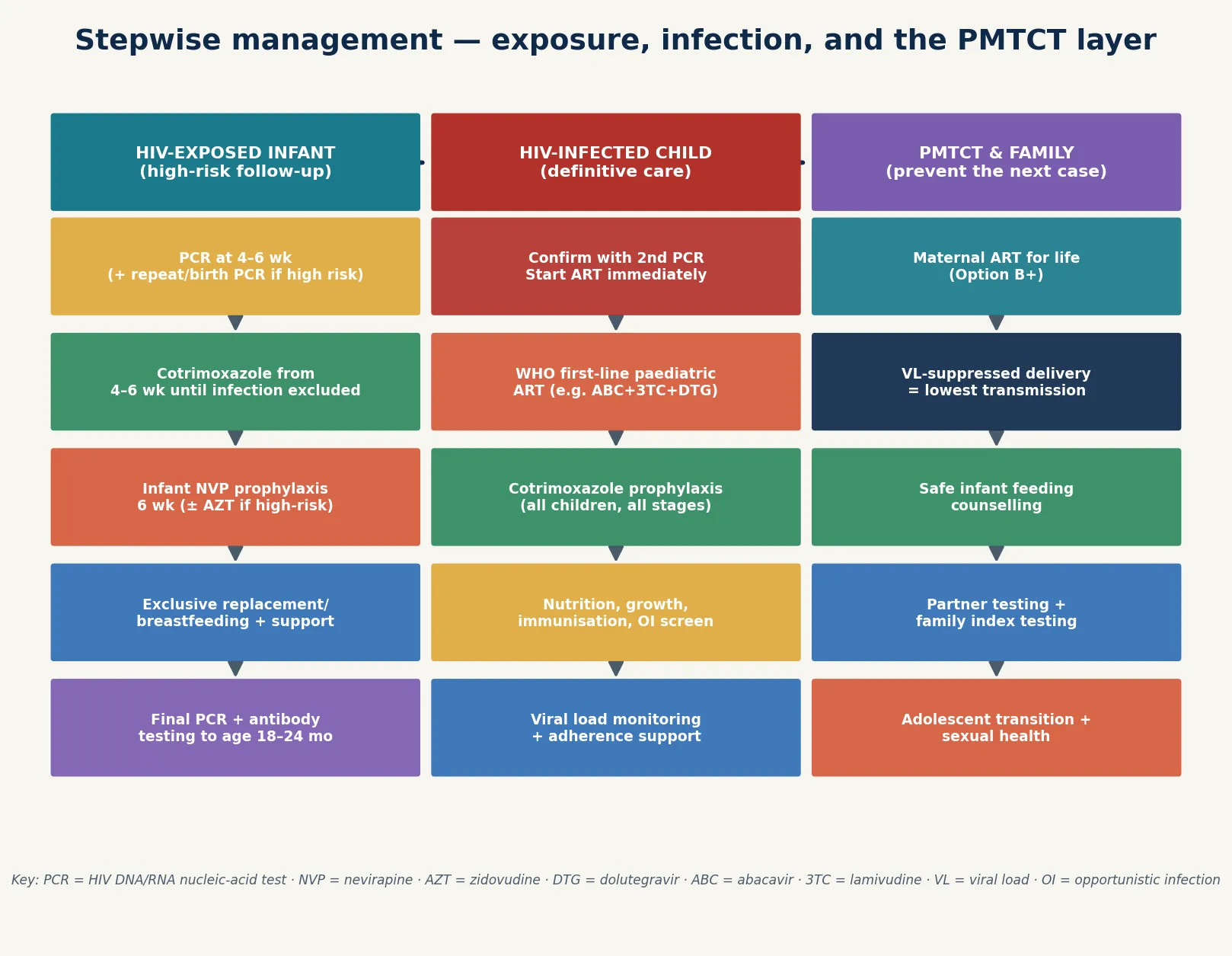
Definitive management is a stepwise pathway split between the HIV-exposed infant, the HIV-infected child, and the family and PMTCT layer that prevents the next case. The exposed infant receives prophylaxis and structured PCR follow-up; the infected child receives immediate ART, cotrimoxazole and comprehensive supportive care; and the family receives maternal ART, testing and counselling to close the cascade. [7] [10]
The stepwise HIV pathway
HIV-exposed infant: give nevirapine prophylaxis for six weeks (add zidovudine in high-risk infants), start cotrimoxazole at 4–6 weeks, and perform PCR at the scheduled timepoints.
Confirm or exclude infection: a positive PCR requires a second confirmatory sample; continue testing until exposure ends and a final antibody at 18–24 months is negative.
HIV-infected child: once infection is confirmed, start ART immediately — treat every infected child at any age and stage.
Add cotrimoxazole prophylaxis for all infected children and provide nutrition, immunisation, growth and opportunistic-infection care alongside the drugs.
Monitor the viral load to confirm suppression and detect failure; address adherence, toxicity and resistance promptly.
PMTCT and family: ensure the mother is on lifelong ART (Option B+) with a suppressed viral load, test partners and siblings, and plan adolescent transition early.
For the HIV-exposed infant, the pathway is prophylaxis plus surveillance. Infant nevirapine is given for six weeks, with zidovudine added in high-risk infants born to unsuppressed or newly diagnosed mothers. Cotrimoxazole begins at four to six weeks and continues until infection is excluded. PCR is performed at the scheduled timepoints, with a birth PCR for high-risk infants, and a final antibody test at 18–24 months confirms the child is uninfected once maternal antibody has cleared. [7] [3]
For the HIV-infected child, the pathway is immediate treatment plus comprehensive care. Infection confirmed, ART is started without delay using a WHO-recommended first-line paediatric regimen — an NRTI backbone such as abacavir and lamivudine plus a third agent such as an integrase inhibitor or a non-nucleoside — weight-based dosed and monitored by viral load. Cotrimoxazole prophylaxis is given to all infected children regardless of stage, and nutrition, immunisation, growth and opportunistic-infection care run in parallel. [5] [10]
For the family and the next pregnancy, the pathway is PMTCT and lifelong engagement. The mother is on lifelong ART (Option B+) with the aim of an undetectable viral load at delivery, which is the single strongest predictor of no transmission. Partners and siblings are offered testing and treatment, feeding is counselled to the setting, and the adolescent with vertically-acquired HIV is transitioned to adult care with attention to adherence, disclosure, mental and sexual health. The cascade is never finished while a single family member is outside it. [2] [3]
Specific Subtypes & Scenarios
An HIV-exposed infant with a positive PCR at six weeks. Confirm the result with a second PCR on a separate sample, start cotrimoxazole, and begin ART immediately once infection is confirmed. Do not wait for clinical staging or a CD4 result — the survival benefit of early treatment is in starting now. Counsel the family on the lifelong nature of treatment and arrange the supportive and monitoring framework. [1] [7]
An acutely hypoxic infant born to an unsuppressed HIV-positive mother. Suspect Pneumocystis pneumonia. Give oxygen, admit, and treat empirically with high-dose co-trimoxazole and a corticosteroid for moderate–severe disease while pursuing the diagnosis with a chest X-ray and, where available, induced sputum or nasopharyngeal wash. Start ART once the infant is stable, because controlling the virus is the definitive treatment of the immunodeficiency that allowed the PCP. [8] [1]
A breastfeeding HIV-positive mother newly diagnosed postpartum. Start maternal ART immediately, give the infant nevirapine prophylaxis, counsel on feeding in the local context, and arrange an early infant PCR. The postpartum diagnosis is a cascade emergency, because ongoing breastfeeding by an untreated viraemic mother is a high-transmission state, and the response must be prompt and coordinated. [3] [7]
An HIV-exposed-uninfected infant with recurrent infection. Confirm that infection is excluded with PCR and, when age-appropriate, a final negative antibody test, then investigate non-HIV causes of recurrent infection thoroughly. Do not assume that HEU status alone explains severe disease, because a HEU infant can still have a primary immunodeficiency, an anatomical problem, or another chronic illness. [6] [7]
An adolescent with vertically-acquired HIV transferring to adult care. Plan the transition early, years before the actual transfer. Address adherence, disclosure to the young person and to partners, mental health, sexual and reproductive health, and the practicalities of the adult service. The single most important goal is an undetectable viral load through the transfer, because disengagement and loss of suppression are the route back to AIDS. [6] [10]
A pregnant HIV-positive woman on effective ART with an undetectable viral load. Continue ART, plan delivery and infant prophylaxis, and reinforce the central fact: a suppressed maternal viral load is the strongest predictor of no transmission. In the high-income setting this woman has a better than 98% chance of an uninfected baby, and the role of the paediatric team is to complete the cascade — prophylaxis, PCR follow-up, feeding support — and to confirm that happy outcome. [2] [7]
Complications & Pitfalls
The serious complications of untreated paediatric HIV are the opportunistic diseases of profound immunodeficiency. Pneumocystis pneumonia is a leading cause of infant HIV mortality; other opportunistic infections include tuberculosis, chronic candidiasis, cytomegalovirus disease, and mycobacterium avium complex. Failure to thrive and wasting reflect both chronic infection and enteropathy, HIV encephalopathy causes developmental delay and regression, chronic diarrhoea depletes nutrition, cytopenias complicate advanced disease, and antiretroviral drugs carry their own toxicities — anaemia, lipodystrophy and mitochondrial toxicity among them. [8] [9]
The central diagnostic pitfall is using antibody testing to diagnose the infant. Maternal IgG crosses the placenta and persists for up to 18 months, so a positive antibody test in a baby is about the mother, not the child. Only nucleic-acid testing can confirm or exclude infection in the first year of life, and a clinician who acts on an antibody result in an infant will either overtreat an uninfected baby or miss an infected one. [7] [8]
A second pitfall is delaying ART in the confirmed infant while awaiting clinical staging or a CD4 count. The CHER trial showed that early treatment of asymptomatic infants reduced mortality by roughly three-quarters, and current guidance treats every infected child at any age and stage. Waiting for the child to sicken before treating is the error the evidence was designed to correct. [1] [5]
A third pitfall is missing Pneumocystis pneumonia in the hypoxic infant. PCP progresses rapidly, and the diagnosis is often clinical in the first instance. Empiric high-dose co-trimoxazole — with a corticosteroid for moderate–severe disease — should begin while the diagnostic workup proceeds, because waiting for confirmation costs lives in this age group. [8] [1]
A fourth pitfall is abandoning the HIV-exposed-uninfected infant after a negative early PCR. Late transmission through breastfeeding, and the persistence of maternal antibody, mean testing must continue until exposure ends and a final antibody is negative. The HEU infant who is lost to follow-up is the infant whose late-acquired infection is missed. [3] [7]
The final pitfall is stigma and confidentiality. A careless approach to disclosure, to testing of siblings and partners, or to the family's social context damages trust and drives disengagement from care. The clinical encounter is also a human encounter, and the family who feels respected stays engaged — which is, in the end, what keeps the virus suppressed and the child alive. [6] [7]
Prognosis & Disposition
Without ART, the prognosis of perinatally-acquired HIV is grim: roughly half of untreated infants are dead or have AIDS by two years of age. With immediate ART and sustained viral suppression, the prognosis is transformed — children who suppress virus and stay engaged in care survive into adulthood with near-normal life expectancy. The gap between these two outcomes is the entire justification for the cascade, and it is closed by treatment and adherence, not by anything more exotic. [4] [1]
With full PMTCT, mother-to-child transmission falls to under 2% in high-income settings, so the prognosis of the exposed but uninfected infant is overwhelmingly that of an uninfected child. The HEU infant does carry a modestly higher infectious-morbidity burden than an unexposed peer, but the dominant message to a supported family is that the baby is well, and the task is to confirm that status and close the chapter. [7] [6]
Disposition follows acuity. The acutely unwell infant with severe pneumonia, sepsis, dehydration or neurological decline is admitted and intensively supported; the stable exposed or infected child is managed in structured outpatient follow-up with a specialist paediatric HIV service. The threshold for admission in the sick exposed or infected infant is deliberately low, because the margin between stable and catastrophic is narrow in immunodeficiency. [8] [1]
The long-term disposition of the infected child is lifelong ART with viral-load monitoring and adherence support, cotrimoxazole where indicated, nutrition and growth surveillance, immunisation, and a planned transition to adult care in adolescence. The prognosis depends as much on engagement-in-care and viral suppression as on biology — the child who stays suppressed and connected to services does well, and disengagement is the route back to AIDS. [5] [6]
Special Populations
Infants and young children are the fastest progressors and the principal beneficiaries of early ART and cotrimoxazole. PCR-based diagnosis is mandatory under 18 months, and the untreated infant's trajectory toward AIDS within months — not years — is the fact that drives the urgency of the whole strategy. [1] [4]
HIV-exposed-uninfected (HEU) infants carry higher infectious-morbidity and mortality than unexposed infants, reflecting immune immaturity, prematurity, antiretroviral exposure and social determinants. They require thorough follow-up and should not be dismissed as simply "well", and a HEU infant who is genuinely failing is investigated for non-HIV causes alongside confirmation that infection is excluded. [6] [9]
Adolescents with vertically-acquired HIV face adherence, disclosure, mental-health and transition challenges. Plan the transfer to adult care early, address sexual and reproductive health, and keep the virus suppressed through the transition, because the disengaging adolescent is the patient most at risk of returning to AIDS. [6] [10]
Breastfeeding mothers and infants in resource-limited settings face a genuine balance: breastfeeding transmits virus in the untreated mother, yet replacement feeding may be unsafe or unavailable where clean water and reliable supply are not guaranteed. The strategy of maternal ART plus infant prophylaxis during breastfeeding is the compromise that protects the baby while preserving the benefits of breast milk. [2] [3]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children, and refugee, asylum-seeking and migrant families may face barriers to testing, treatment and follow-up. Ensure culturally safe, equitable access to PMTCT, ART and viral-load monitoring; use trained interpreters rather than family members; and address stigma and the social determinants that break the cascade. Disadvantage should never be the reason a child is left untested or untreated. [7] [6]
Rural and remote families need coordinated testing, ART supply, viral-load monitoring and retrieval through outreach and telehealth, because distance and logistics break the cascade if they are not deliberately managed. The plan for a remote family accounts for what is actually available locally and mobilises retrieval early when an infant deteriorates. [7] [8]
Evidence, Guidelines & Regional Differences
The landmark that transformed paediatric HIV was the CHER trial. Violari and colleagues showed that starting antiretroviral therapy in asymptomatic infants under twelve weeks — rather than waiting for clinical or immunological decline — reduced mortality by roughly 76% and HIV progression by 75%. The trial changed paediatric HIV from a staged to a treat-all strategy, and it is the single most important piece of evidence behind immediate ART for the infected infant. [1] [5]
The natural history that made the trial necessary was quantified by Newell and colleagues. Their pooled analysis of African cohorts showed that roughly half of untreated, vertically-infected infants developed AIDS or died by two years of age — a trajectory far steeper than adult disease, and the reason infants cannot wait. The evidence for postnatal prophylaxis comes from the BAN study, in which Chasela and Jamieson and colleagues showed that maternal or infant antiretrovirals during breastfeeding reduced postnatal transmission, informing the strategy that protects the breastfeeding infant. [4] [3]
CHER — Children with HIV Early Antiretroviral Therapy
Population: HIV-infected South African infants under 12 weeks of age, randomised to deferred ART (by CD4/clinical criteria) versus immediate ART, with a primary endpoint of mortality or HIV disease progression.
Key finding
Immediate ART in asymptomatic infants reduced mortality by about 76% and HIV progression by 75% compared with a deferred strategy — leading to early stopping of the deferred arm.
Practice change
Treat every infected infant as soon as infection is confirmed, at any age and stage; the survival benefit of early treatment in infancy is large and time-sensitive.
The guideline framework is consistent across regions. The WHO consolidated guidelines recommend ART for all children living with HIV and the Option B+ strategy of lifelong maternal ART. The PENTA 2016 guideline (Foster et al.) is the European paediatric analogue, recommending antiretroviral therapy for all children. In the United States, Havens and colleagues (Pediatrics 2009) and the CDC/NIH opportunistic-infection guidelines (Mofenson et al., MMWR 2009) direct the evaluation of the exposed infant and cotrimoxazole prophylaxis. In Australia and Aotearoa New Zealand, ASHM guidance directs antenatal screening and the exposed-infant pathway. [5] [7]
The HEU burden and the adolescent transition are framed by Slogrove and colleagues, who reviewed the global epidemiology of the HIV-exposed-uninfected child and the adolescent epidemic. Kacanek and colleagues contributed evidence on the neurodevelopmental outcomes of in-utero antiretroviral exposure, a question that matters to every family weighing treatment in pregnancy, and Barlow-Mosha and colleagues reviewed the benefits and risks of universal ART for children during implementation. [6] [9]
The controversies are real and active: the optimal balance of breastfeeding safety and replacement-feeding access in resource-limited settings; the place of newer agents such as dolutegravir in pregnancy and infancy; the long-term durability and toxicity of lifelong ART begun in childhood; and the equity gap that leaves some settings and families outside the cascade. The defence against each is the same: high coverage, prompt diagnosis, immediate treatment, cotrimoxazole, and a cascade that does not stop at the bedside. [10] [6]
Exam Pearls
- Diagnose infant HIV with DNA or RNA PCR — not antibody — because maternal IgG persists to ~18 months; confirm a positive PCR with a second sample. [7]
- Without PMTCT, mother-to-child transmission is 15–45% (higher in breastfeeding); with full PMTCT it falls below 2% in high-income settings. [4]
- Roughly half of untreated perinatally-infected infants are dead or have AIDS by age two — infants progress far faster than adults. [4]
- The CHER trial showed early ART in infants cut mortality by about 76% — treat every infected child now, at any age and stage. [1]
- Start cotrimoxazole prophylaxis at 4–6 weeks in exposed and infected infants; it prevents PCP and reduces mortality. [8]
- Pneumocystis pneumonia presents as hypoxic interstitial pneumonia at age 3–6 months — treat empirically with high-dose co-trimoxazole (and steroid for moderate–severe disease) while confirming. [8]
- The single strongest predictor of no vertical transmission is a maternal viral load that is undetectable at delivery — the backbone of Option B+. [2]
- Infant prophylaxis is nevirapine for six weeks (zidovudine added in high-risk infants); continue testing to a final negative antibody at 18–24 months. [7]
- HIV-exposed-uninfected (HEU) infants carry higher morbidity than unexposed infants — do not dismiss them as simply "well". [6]
- Plan adolescent transition early: adherence, disclosure, mental and sexual health, and viral suppression through the transfer to adult care. [6]
References
- [1]Violari A; Cotton MF; Gibb DM; Babiker AG; et al Early antiretroviral therapy and mortality among HIV-infected infants. N Engl J Med, 2008.PMID 19020325
- [2]Chasela CS; Hudleston MJ; Jamieson DJ; Kayira D; et al Maternal or infant antiretroviral drugs to reduce HIV-1 transmission. N Engl J Med, 2010.PMID 20554982
- [3]Jamieson DJ; Chasela CS; Hudleston MG; King CC; et al Maternal and infant antiretroviral regimens to prevent postnatal HIV-1 transmission: 48-week follow-up of the BAN randomised controlled trial. Lancet, 2012.PMID 22541418
- [4]Newell ML; Coovadia H; Cortina-Borja M; Rollins N; et al Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet, 2004.PMID 15464184
- [5]Foster C; Pace M; Kaye S; Hopkins E; et al Paediatric European Network for Treatment of AIDS Treatment Guideline 2016 update: antiretroviral therapy recommended for all children living with HIV. HIV Med, 2017.PMID 27385585
- [6]Slogrove AL; Mahy M; Armstrong A; Davies MA Living and dying to be counted: What we know about the epidemiology of the global adolescent HIV epidemic. J Int AIDS Soc, 2017.PMID 28530036
- [7]Havens PL; Mofenson LM; American Academy of Pediatrics Committee on Pediatric AIDS Evaluation and management of the infant exposed to HIV-1 in the United States. Pediatrics, 2009.PMID 19117880
- [8]Mofenson LM; Brady MT; Danner SP; Dominguez KL; et al Guidelines for the Prevention and Treatment of Opportunistic Infections among HIV-exposed and HIV-infected children. MMWR Recomm Rep, 2009.PMID 19730409
- [9]Kacanek D; Huo Y; Laskey B; Mellins CA; et al Pediatric Neurodevelopmental Functioning After In Utero Exposure to Triple-NRTI vs. Dual-NRTI + PI ART in a Randomized Trial, Botswana. J Acquir Immune Defic Syndr, 2018.PMID 30015793
- [10]Barlow-Mosha L; Angelidou K; Lindsey JC; Archary M; et al Universal antiretroviral therapy for HIV-infected children: a review of the benefits and risks to consider during implementation. J Int AIDS Soc, 2017.PMID 28691434