Paeds · infectious-diseases
Infection prevention, isolation and outbreak management
Also known as Infection prevention and control (IPC) · Standard and transmission-based precautions · Isolation and cohorting · Healthcare-associated infection prevention · Outbreak investigation and management
Fellowship topic on infection prevention, isolation and outbreak management in the paediatric healthcare setting: the chain of infection and where every IPC measure breaks it; standard precautions applied to every child; transmission-based precautions — contact, droplet and airborne — matched to the organism; the WHO 'My 5 Moments' of hand hygiene; personal protective equipment, isolation, cohorting and single-room use; the device-related healthcare-associated infections (CLABSI, VAP, CAUTI, SSI) and their bundle prevention; paediatric and NICU-specific risks including immature skin, parental presence, shared equipment and toy pools; outbreak recognition, case definition, epidemic-curve construction, source investigation, communication and control; multidrug-resistant organism containment; surveillance, antimicrobial stewardship and the regional guideline landscape (WHO, CDC/HICPAC, ACSQHC, NHS, SHEA). Designed for the candidate who must think like a clinician and a system operator at once.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Standard precautions are for everyone — always
Overview & Definition
Picture a four-bed bay on a paediatric ward in winter. Two children have bronchiolitis, one has a central line for chemotherapy, and the fourth is a returned traveller with fever and a rash not yet diagnosed. Within hours, a vomit-and-diarrhoea illness sweeps the bay, the oncology child spikes a line infection, and the question on everyone's lips is "should the rashy child have been placed elsewhere?" This is the daily reality of infection prevention and control, and the difference between a contained problem and a ward-wide outbreak is decided at exactly these moments. [6] [4]
Infection prevention and control is the discipline and the practice of preventing harm to patients, staff and visitors from transmissible organisms in the healthcare setting. In its modern form it binds together hand hygiene, personal protective equipment, isolation and cohorting, environmental hygiene, surveillance, antimicrobial stewardship and outbreak management into a single safety system. The aim is not to eliminate every microbe — that is impossible — but to ensure that a pathogen does not move from where it belongs to where it can hurt a vulnerable child. [1] [3]
Why does paediatric IPC deserve its own page? Children bring three features that change the calculus. First, their skin, mucosa and immune systems are immature, especially in neonates, so a small inoculum becomes a serious infection. Second, they are handled constantly — by parents, siblings, play therapists, students and many staff — and they share toys, equipment and waiting spaces, multiplying the surfaces a pathogen can ride on. Third, the highest-risk hosts are concentrated in specific units: the premature neonate with a central line in the NICU, the oncology patient with neutropenia, the technology-dependent child with a tracheostomy. A single lapse that an adult ward might shrug off can devastate these patients. [5] [7]
The clinician's job splits into two halves that must run together. The reactive half responds to the infectious child in front of you — choosing the right precautions, isolating early, placing the line bundle. The proactive half runs the system — auditing hand hygiene, surveilling for clusters, designing bundles, and preparing for the outbreak that is always one missed case away. Fellowship answers that cover only the bedside miss the system, and those that cover only the system miss the child; the best cover both. [4] [7]
Classification
Classify IPC the way you use it at the bedside: first by the tier of precautions, then by the route of transmission, and finally by the type of healthcare-associated infection you are trying to prevent. The tiered model is the backbone. Standard precautions are the baseline applied to every patient regardless of diagnosis, because history and examination cannot reliably identify everyone who is infectious. When a specific organism is known or suspected, transmission-based precautions are added on top, chosen to match how that organism travels between people. [4] [3]
At the bedside you match the precaution to how the organism actually travels between children, and examiners expect you to pair each route with its examples and its equipment. Contact precautions — gown and gloves, ideally a single room or cohort — cover organisms that spread by direct touch or via the shared environment: MRSA, VRE, norovirus, RSV, C. difficile, scabies and impetigo. Droplet precautions — surgical mask and spacing of about a metre — cover organisms carried in large respiratory droplets: influenza, pertussis, mumps, Group A streptococcus and (classically) meningococcal disease. Airborne precautions — a fit-checked particulate respirator such as N95 or P2 and a negative-pressure room — cover organisms that ride small-particle nuclei that drift on air currents: measles, pulmonary tuberculosis, varicella and disseminated herpes zoster. [4] [5]
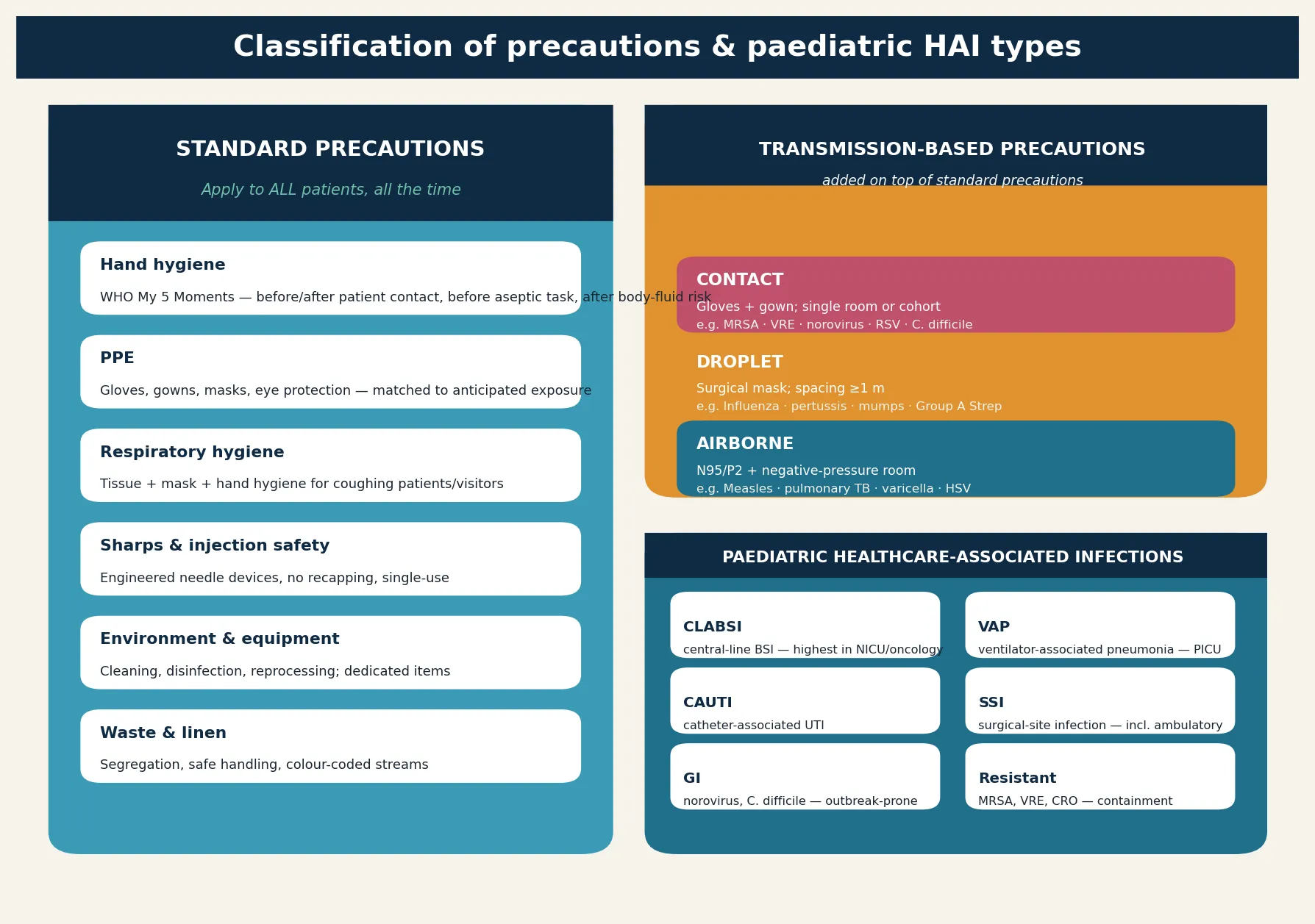
The third axis is the device-related infection, because each has its own prevention bundle. A central-line-associated bloodstream infection (CLABSI) arises when skin organisms track along or through a line into the bloodstream — the largest preventable HAI burden in the NICU and a leading killer in oncology. Ventilator-associated pneumonia (VAP) follows aspiration of contaminated secretions around the endotracheal tube. Catheter-associated urinary tract infection (CAUTI) and surgical-site infection (SSI) — including infections after day-case and ambulatory surgery — complete the set. Classifying by device matters because each bundle names the precise checklist that prevents it, and the fellowship candidate who reaches for "antibiotics" instead of "the bundle" has reached for the wrong tool. [5] [10] [9]
Epidemiology & Risk Factors
How common are healthcare-associated infections, and who pays the price? The Magill multistate point-prevalence survey of US acute-care hospitals found that about one in twenty-five hospitalised patients had at least one healthcare-associated infection on the day of survey, with pneumonia, gastrointestinal illness, urinary tract and bloodstream infections heading the list. For children — and especially for neonates in intensive care — the device-related infections dominate, and they are largely preventable. Knowing the burden tells you where to direct effort. [6] [7]
The dominant risk factors cluster around the device and the host. Anything that breaches the skin or mucosa — a central or peripheral line, a urinary catheter, an endotracheal tube, a surgical wound — creates a portal of entry and a surface for biofilm. The longer a device stays, the higher the risk, which is why daily review of line necessity and prompt removal sit at the centre of every bundle. A large NICU analysis confirmed that central-line days, gestational age and parenteral nutrition are among the strongest predictors of healthcare-associated bloodstream infection in neonates. [10] [5]
Host vulnerability magnifies risk at both ends of childhood. The very preterm neonate has thin skin, an immature immune system and, often, a central line for life-sustaining nutrition; the oncology patient is neutropenic and line-dependent; the technology-dependent child with a tracheostomy or long-term ventilation lives with a chronic portal of entry. These are the patients in whom a single environmental lapse becomes a bloodstream infection, and for whom bundle reliability is non-negotiable. [5] [7]
Behavioural and environmental risk factors complete the picture. Poor hand-hygiene compliance, shared or inadequately reprocessed equipment, overcrowding and understaffing, toy pools that are not cleaned, and the constant traffic of family members all raise transmission. Outbreaks of viral respiratory infection in NICUs — including RSV, influenza, parainfluenza and SARS-CoV-2 — are a recurring threat, and the SHEA NICU white paper on preventing viral respiratory infections sets out the cohorting, screening and visitor-control measures that contain them. [8] [4]
Pathophysiology
Why does a pathogen move from one child to the next, and where can you stop it? The answer is the chain of infection: six links, each of which can be broken. The infectious agent is the organism itself. Its reservoir is where it normally lives — the skin, the gut, the respiratory tract, a piece of equipment, or even a staff member. The portal of exit is the route by which it leaves the reservoir: respiratory secretions, faeces, blood, wound drainage. The mode of transmission is how it travels — contact, droplet, airborne, a common vehicle such as contaminated fluid, or a vector. The portal of entry is how it enters the next host: mucous membranes, broken skin, a device or line. And the susceptible host is the child whose defences cannot withstand the inoculum. [4] [1]
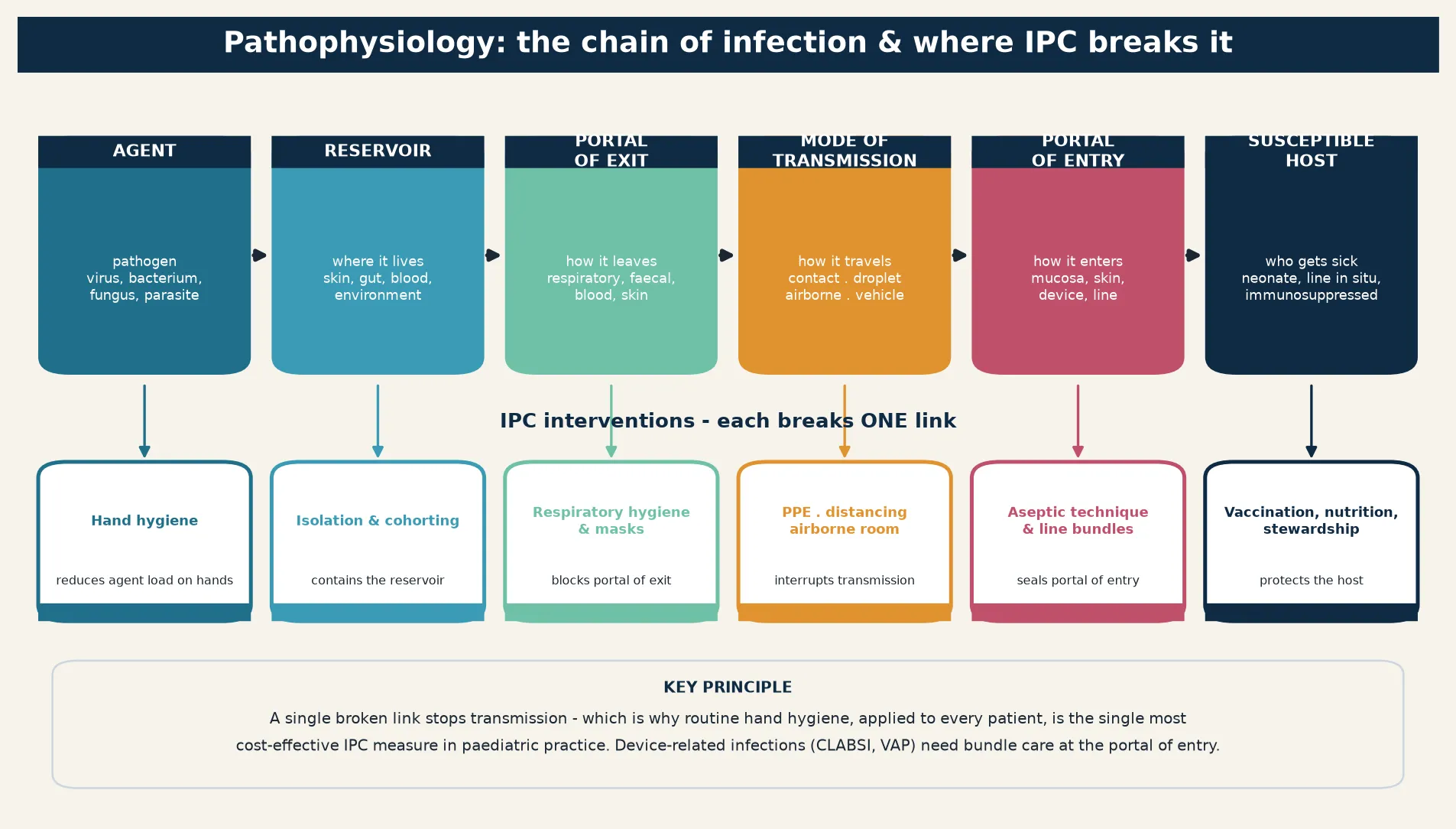
The teaching point of the chain is that each link is an opportunity, and each precaution maps to a specific link. Hand hygiene lowers the agent load on hands and interrupts transmission through the contact route. Isolation and cohorting contain the reservoir. Respiratory hygiene and masks block the portal of exit. PPE, distancing and negative-pressure rooms interrupt the mode of transmission. Aseptic technique and device bundles seal the portal of entry. Vaccination, nutrition and antimicrobial stewardship protect the susceptible host. When a candidate maps an intervention to its link, they stop memorising rules and start reasoning about transmission. [1] [3]
Device-related infection has its own mini-pathophysiology that the bundles target directly. A central line is a foreign body that skin organisms such as coagulase-negative staphylococci can colonise, forming a biofilm at the catheter tip or along the intraluminal surface; from there they seed the bloodstream. The CLABSI bundle attacks each step — maximal sterile barrier and chlorhexidine preparation at insertion, optimal site selection, daily review of necessity, scrub-the-hub access care, and prompt removal. VAP follows the same logic: contaminated oropharyngeal secretions pool above the endotracheal cuff and slip past into the lung, and the bundle — head-of-bed elevation, oral care, sedation holds and daily extubation assessment — addresses each. [5] [10]
The paediatric twist is that the susceptible host is often the most fragile link. A premature neonate's skin is thin and easily damaged, so even adhesive dressings and tape become portals of entry; an immature immune system clears organisms poorly; and a single line may be the only access for life-sustaining nutrition and cannot simply be removed. This is why NICU IPC tolerates no compromise on bundles, and why the same lapse that an adult ward might absorb can be lethal on a neonatal unit. [5] [8]
Clinical Presentation
How does a healthcare-associated infection declare itself, and how does an outbreak show up on the ward? A device-related infection presents as new fever, rigors or clinical deterioration localised to the device. A child with a central line who develops fever, chills or new entry-site inflammation, especially around line access or during a flush, has a CLABSI until proven otherwise — and the decision to draw blood cultures, including a peripheral culture and a culture through the line, and to weigh source control should happen promptly. New respiratory deterioration in a ventilated child raises VAP; cloudy urine or systemic upset with a catheter raises CAUTI; and wound erythema, discharge or dehiscence after surgery raises an SSI, including after day-case procedures. [6] [9]
An outbreak presents as a signal — a cluster of cases above the expected baseline. Three or more cases of norovirus gastroenteritis in a bay over forty-eight hours, a sudden rise in CLABSI on one shift pattern, or two cases of the same resistant organism on a ward are all signals. The art is in recognising the signal early, before it becomes a ward-wide event, and in resisting the temptation to dismiss the first cases as coincidence. The clinician who notices that "this is the third child with this organism this week" is the one who triggers the response in time. [4] [8]
Gastrointestinal outbreaks have a distinctive tempo. Norovirus hits hard and fast — explosive vomiting and diarrhoea that propagates across patients, staff and visitors within a day or two, and which alcohol-based hand rub alone does not control because it is relatively resistant; soap-and-water hand washing and environmental cleaning with bleach-based agents are required. Clostridioides difficile presents with diarrhoea after antibiotic exposure, and a cluster on a ward raises the question of cross-transmission and antibiotic stewardship. Recognising the pattern drives the right containment. [4] [7]
Viral respiratory outbreaks in the NICU present more subtly and more dangerously. A neonate with new apnoea, feed intolerance, recurrent desaturation or unexplained temperature instability during the RSV or influenza season may have acquired the virus on the unit, and a single case should prompt screening and cohorting of exposed infants. The SHEA NICU white paper frames these as preventable events: cohorting of cases and exposed infants, restriction of ill staff and visitors, and reinforcement of hand hygiene and PPE. [8] [5]
Differential Diagnosis
For the hospitalised child with new fever, the differential turns on whether the source is community-acquired, healthcare-associated or non-infectious. A new fever on day five of admission, in a child with a central line, points toward a healthcare-associated bloodstream infection; the same fever on day one of admission more often reflects the presenting illness. Non-infectious causes — drug fever, a transfusion reaction, postoperative inflammatory response, or a missed line thrombosis — must not be forgotten, because treating them as infection means unnecessary antibiotics and continued risk. The disciplined approach is to sample before treating, weigh device removal, and keep the differential open. [6] [7]
For the cluster or outbreak, the differential is the cause itself. A gastroenteritis cluster is usually norovirus but could be a foodborne event, rotavirus, adenovirus, or even C. difficile related to antibiotic pressure. A respiratory cluster on a ward or in a NICU ranges across RSV, influenza, parainfluenza, rhinovirus, human metapneumovirus and SARS-CoV-2 — and the management (cohorting, screening, visitor restriction) is similar for all, but the protection of the most vulnerable infants is the constant. A rise in device infections may be a true cluster, a surveillance artefact, or a pseudo-outbreak from contaminated specimens or reagents — a distinction that laboratory and epidemiological investigation resolves. [4] [8]
For the individual infectious presentation, the organism-specific differential matters because it sets the isolation category. A fever-and-rash presentation could be measles (airborne), varicella (airborne and contact), meningococcal disease (droplet), a viral exanthem (standard or contact), or Kawasaki disease (no isolation at all). A purulent wound could be a sensitive organism on standard precautions or MRSA on contact precautions. Choosing the wrong isolation category — too low and you spread the organism, too high and you isolate a non-infectious child — is a common and consequential error. [4] [5]
Clinical & Bedside Assessment
The bedside assessment begins with a moment of triage: does this child need isolation now, on arrival, before the diagnosis is settled? The safe default is to isolate early on the clinical suspicion rather than wait for confirmation, because the cost of isolating a child who turns out not to be infectious is far lower than the cost of missing one who is. Ask about the rash and fever, the cough with an unimmunised household, the diarrhoea and vomiting with a ward outbreak in progress, the recent travel, and the immune status. A child in whom a high-consequence infection is plausible — measles, pulmonary TB, a viral haemorrhagic fever, a resistant organism — goes straight into the appropriate precautions. [4] [5]
Assess the device as deliberately as you assess the child. When was the central line placed, by whom, and under what barrier conditions? Is the entry site clean and dry, and is the dressing intact? How many lumens, how often are they accessed, and is "scrub the hub" actually happening? Is the urinary catheter still needed today, and what is the plan to remove it? Is the child on the lowest effective ventilator settings with daily sedation holds and extubation assessment? Each device is a standing invitation to infection, and the bundle is the daily defence. [5] [10]
Document the IPC essentials at the bedside so the system can act. Record the onset and nature of any suspected cluster, the bay and bed numbers, the staff and visitors involved, and the specimens sent. For a notifiable disease, confirm that notification has been triggered. For a device infection, capture the line days and bundle documentation. These details feed surveillance and outbreak investigation, and the encounter where they are captured is the encounter where the next case is prevented. [4] [7]
Assess the family's needs as part of the IPC plan, because isolation changes a family's experience of the hospital. A child in a single room may be frightened and alone; parents may be limited in their visits; siblings may be excluded; and the explanation of why isolation is necessary must be honest, calm and free of stigma. For children with disability or neurodiversity, for Aboriginal and Torres Strait Islander and Māori families, and for migrant and refugee families, the isolation plan must be communicated with cultural safety, through trained interpreters where needed, so that IPC does not become a barrier to compassionate, equitable care. [7] [8]
Investigations
The investigations split into two streams: diagnosing the individual child, and investigating the cluster. For the individual, send blood cultures before antibiotics whenever possible — a peripheral culture and a culture drawn through each accessible line lumen — to localise the source and guide source control. Send respiratory samples for the relevant viral panel in season, wound swabs or aspirates for culture, stool for norovirus, rotavirus, adenovirus and C. difficile testing as the picture demands, and consider molecular typing for resistant organisms. The principle is to sample early and broadly, because a sample taken after empirical antibiotics is far less useful. [6] [5]
For the cluster or outbreak, the investigation is epidemiological as much as microbiological. Construct a case definition — who counts as a case, by clinical and time-and-place criteria — and apply it both retrospectively and prospectively. Build a line list of every case with onset, location, organism, device, staff and risk factors. Draw the epidemic curve, plotting cases over time, because its shape reveals the mode of spread: a point-source outbreak rises and falls sharply, while propagating outbreaks stagger over time as person-to-person transmission continues. Combine the curve with a review of the environment, equipment, practices and staffing to identify the source and the mode. [4] [8]
Surveillance underpins both streams and is itself an investigation of the system. Ongoing measurement of device-associated infection rates, hand-hygiene compliance, resistant-organism acquisition and notifiable-disease notifications allows a cluster to be seen against a known baseline. The fellowship candidate should name surveillance as the early-warning system that turns "this feels like a lot of cases" into "the rate is two standard deviations above baseline" — and should know that without a baseline, an outbreak cannot be confirmed. [7] [4]
In Australia and Aotearoa New Zealand, IPC practice is governed by the Australian Commission on Safety and Quality in Health Care (ACSQHC) national standards, the NHMRC infection-control guidance, and state and territory public-health legislation for notifiable diseases. Hand-hygiene compliance is audited nationally and fed back to units, and the Aotearoa New Zealand standards set equivalent expectations. The same principles — standard and transmission-based precautions, device bundles, surveillance and outbreak response — apply, with local variation in notification pathways and isolation-room infrastructure.
Management — Resuscitation
Resuscitation in IPC is about the high-consequence presentation and the deteriorating child, handled with the right protection in place. When a child with a suspected high-transmission infection arrives — measles, pulmonary TB, a viral haemorrhagic fever, a new resistant organism — the immediate priority is to place them in the correct precautions without delay, while preserving rapid access to airway, breathing and circulation care. Senior decision-making, early isolation in a single negative-pressure room where airborne spread is possible, and minimisation of staff exposure come first; the diagnosis can be refined afterwards. [4] [5]
For the device-related infection that causes physiological collapse, resuscitation follows paediatric sepsis principles with IPC woven through it. Recognise the septic child, give oxygen and fluid boluses, take cultures including line cultures before antibiotics, give broad-spectrum therapy promptly, and address the source — which often means deciding with the team whether to remove or exchange the central line. Source control is part of resuscitation in device-related sepsis, and a line that has caused a bloodstream infection is frequently part of the problem and part of the cure when it is removed. [6] [10]
For the outbreak in progress, the resuscitation equivalent is containment: act on suspicion, do not wait for confirmation. Close the affected bay, stop new admissions, isolate and cohort cases and their exposed contacts, reinforce hand hygiene and PPE, restrict ill staff and visitors, and clean the environment with the right agents. The instinct to wait for laboratory confirmation before acting is the instinct that lets an outbreak double in size; containment is cheapest and most effective at the very first signal. [4] [8]
Throughout, protect the staff and the family. Fit-check respirators where airborne spread is possible, ensure correct donning and especially doffing of PPE, and arrange for the sickest child to be cared for by the smallest necessary team. Communicate clearly with the family about what is happening and why, and never let IPC become an excuse to withhold compassionate, family-centred care. [5] [8]
Management — Definitive & Stepwise
Definitive management is a layered, stepwise system: standard precautions as the universal base, transmission-based precautions added to the specific organism, device bundles that prevent the highest-impact infections, environmental and equipment hygiene, surveillance, and a structured outbreak response. The candidate who presents IPC as a system — rather than a list of disconnected rules — is the one who can apply it under pressure. [4] [1]
The stepwise IPC system at the bedside
Apply standard precautions to every patient, every time — hand hygiene at the WHO 5 Moments, task-matched PPE, respiratory hygiene, sharps and waste safety, environmental cleaning.
Add transmission-based precautions matched to the organism: contact (gown and gloves) for MRSA, norovirus, RSV, C. difficile; droplet (surgical mask) for influenza and pertussis; airborne (N95/P2 and negative pressure) for measles, pulmonary TB and varicella.
Isolate early on suspicion in a single room or cohort; never wait for confirmation before containing a high-consequence organism or an outbreak signal.
Run the device bundles daily — maximal-barrier insertion and daily line necessity review for CLABSI, head-of-bed elevation and sedation holds for VAP, daily catheter review for CAUTI, and perioperative bundles for SSI.
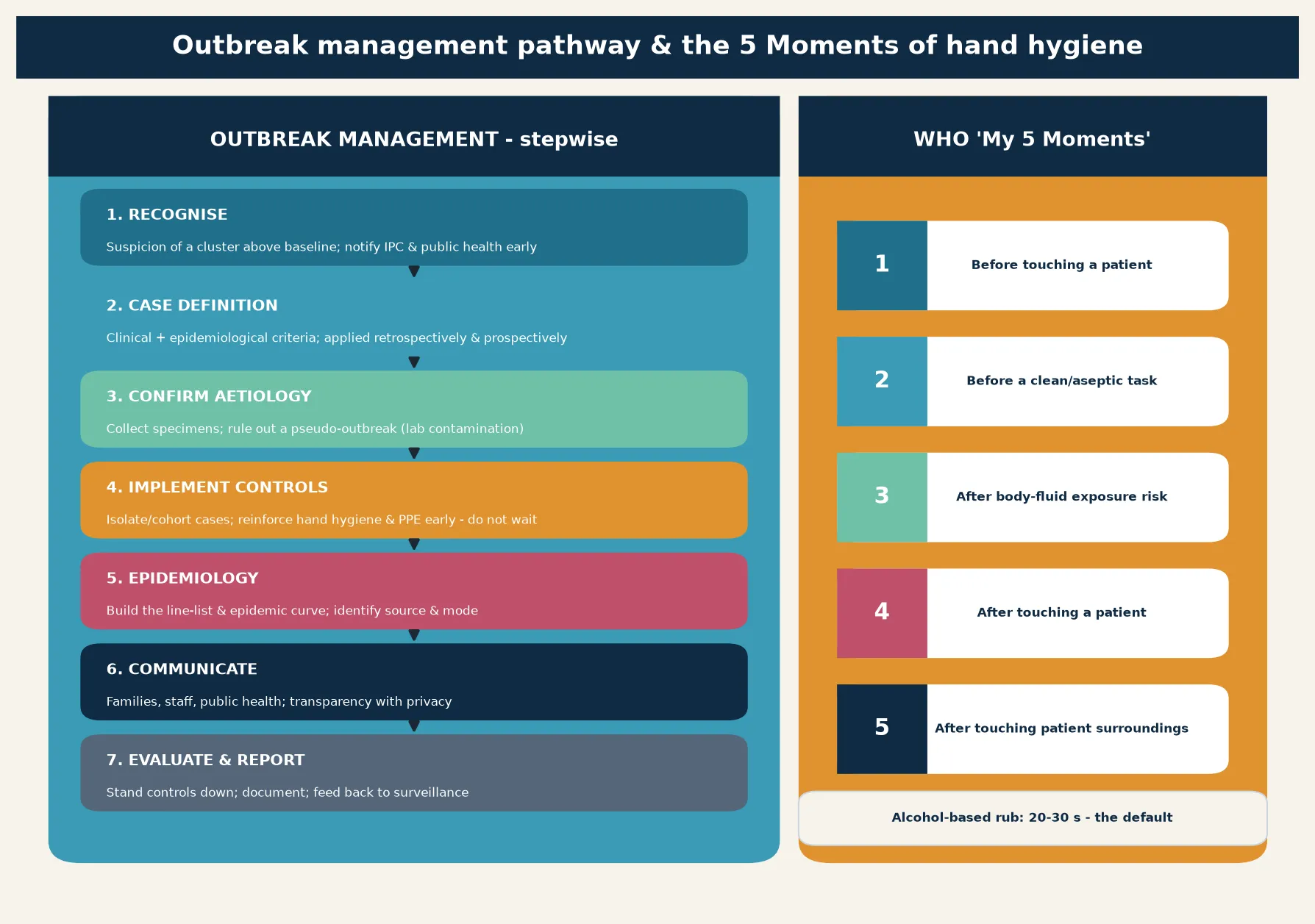
When cases cluster above baseline, treat it as an outbreak: recognise, set a case definition, confirm the aetiology, implement controls, build the epidemic curve, communicate and evaluate.
Link IPC to antimicrobial stewardship, surveillance and vaccination — the measures that protect the susceptible host and slow resistance.
Hand hygiene is the keystone, and the WHO "My 5 Moments for Hand Hygiene" is the framework: before touching a patient, before a clean or aseptic task, after body-fluid exposure risk, after touching a patient, and after touching patient surroundings. Alcohol-based hand rub is the default for routine decontamination, taking twenty to thirty seconds and acting rapidly on most pathogens; soap and water is required when hands are visibly soiled and specifically after caring for a patient with suspected or confirmed norovirus or C. difficile, against which alcohol is less reliable. The Allegranzi and Pittet review of hand hygiene's role in HAI prevention anchors the evidence that improving compliance lowers infection rates, and the WHO and CDC guidelines operationalise the practice. [1] [3] [2]
Transmission-based precautions are deployed once an organism is known or suspected, and they are removed once the risk has passed or been treated. The logistics — single room versus cohort, dedicated equipment, signage, the duration of isolation, the negative-pressure requirement for airborne spread — are details an examiner probes, and so are the pitfalls: a child with a droplet illness incorrectly placed in only a surgical mask when airborne spread is possible, or a contact-precautions child whose room equipment is carried out and reused. Cohorting is the pragmatic NICU and ward solution when single rooms are scarce: group cases together, group exposed contacts together, and staff them with dedicated teams. [4] [8]
Device bundles convert aspiration into reliability. The CLABSI bundle — hand hygiene, maximal sterile barrier and chlorhexidine skin preparation at insertion, optimal site selection, daily review of line necessity with prompt removal, and scrub-the-hub access care — is the single best-studied paediatric IPC intervention, and the Polin AAP NICU guidance and the NICU bloodstream-infection epidemiology underline why it matters most where lines are life-sustaining. The VAP, CAUTI and SSI bundles follow the same logic, and the Yokoe compendium of strategies to prevent healthcare-associated infections organises them into a single acute-care reference. Prevention here is process, not pharmacology. [5] [4] [10]
Specific Subtypes & Scenarios
A NICU viral respiratory outbreak (RSV, influenza, parainfluenza, SARS-CoV-2). The premature infant is the most susceptible host, and a single case on the unit is an emergency. Cohort cases and exposed infants, screen contacts, restrict ill staff and visitors, reinforce hand hygiene and PPE, and consider unit closure to new admissions. The SHEA NICU white paper on preventing viral respiratory infections sets out these practical measures and frames them as both feasible and essential. [8] [5]
A central-line bloodstream infection in an oncology or NICU patient. Draw cultures peripherally and through the line, start appropriate empirical therapy, and decide with the team on line removal or exchange — often the infected line must come out for source control. Review the bundle: was the barrier sterile at insertion, is the site cared for, is necessity reviewed daily, is the hub scrubbed? Feed the case back into the unit's CLABSI surveillance and improvement work. [10] [5]
A norovirus gastroenteritis outbreak on the ward. Close the bay, isolate and cohort, switch to soap-and-water hand washing (alcohol rub is insufficient), and clean with a bleach-based agent. Exclude affected staff, restrict movement, and communicate with families and the IPC team. Expect propagation within twenty-four to forty-eight hours if controls are delayed, and stand controls down only after the defined period without new cases. [4] [6]
A multidrug-resistant organism — MRSA, VRE, or a carbapenem-resistant Enterobacterales. Place on contact precautions in a single room or cohort, use dedicated equipment, screen contacts as the local policy directs, and link the event to antimicrobial stewardship because resistance is driven by antibiotic pressure. Decolonisation has a role for some organisms in some settings, but containment and stewardship are the durable answers. [7] [4]
A vaccine-preventable disease on the ward — measles or varicella. Act immediately: place the case on airborne (and, for varicella, contact) precautions, identify every susceptible contact, offer post-exposure prophylaxis or vaccination where indicated, and exclude susceptible staff. These events are high-consequence because the unprotected neonate, oncology patient or pregnant contact is in the same building. The speed of the response determines its success. [5] [4]
A surgical-site infection after ambulatory or day-case surgery. Most paediatric surgery is now ambulatory, and the Gerber study of infections after paediatric ambulatory surgery showed that SSIs occur after day-case procedures too, with identifiable risk factors. Perioperative bundles — timing and choice of prophylaxis, skin preparation, glycaemic and temperature control, and sterile technique — apply as much to the day-case as to the inpatient theatre. [9] [4]
Complications & Pitfalls
The gravest complication is preventable harm to a vulnerable child — a CLABSI in a neonate, a viral pneumonia in an oncology patient, a measles exposure of an unimmunised infant — and the fellowship candidate should frame every HAI as a failure of a system that should have prevented it. The Magill prevalence data and the NICU bloodstream-infection epidemiology are the evidence that the burden is real and concentrated in the patients who can least afford it. [6] [10]
The central pitfall is waiting for confirmation before acting. The clinician who requires a positive PCR before isolating a measles-suspect child, or a typed organism before closing a bay, has already allowed transmission. The correct reflex is to isolate on suspicion and to stand down when the risk is excluded. Containment is cheapest at the first signal and most expensive once an outbreak is established. [4] [8]
A second pitfall is mismatching the precaution to the route. Placing a measles case on droplet precautions instead of airborne, or a norovirus case on standard precautions, lets the organism travel the route you failed to block. The remedy is to know the route for each common organism and to escalate the precaution upward when in doubt. Equally, over-isolation — isolating a non-infectious child on full contact precautions — wastes single-room capacity, stigmatises the family, and erodes trust in the system. [5] [4]
A third pitfall is neglecting the device. A line left in "just in case", a catheter not reviewed today, or a ventilator bundle delivered inconsistently is the everyday origin of a CLABSI, a CAUTI or a VAP. The bundles work only when they are reliable, and reliability is a daily discipline. Reaching for antibiotics instead of the bundle treats the symptom and perpetuates the cause. [5] [10]
A fourth pitfall is the human one: PPE worn incorrectly, especially doffed in a way that contaminates the wearer; hand hygiene skipped between tasks; and the assumption that gloves substitute for hand hygiene. Gloves are worn for the task and removed promptly, and hand hygiene follows every removal. The behavioural dimension — auditing compliance, feeding it back, and building a just culture in which staff can speak up — is as important as the technical one. [1] [3]
The final pitfall is treating IPC as the IPC team's problem. The team advises and coordinates, but the practices that prevent transmission happen at the bedside, on every shift, in every encounter. A culture that delegates IPC upward is the culture that lets clusters grow; a culture in which every clinician owns the bundle, the hand-hygiene moment and the early signal is the culture that contains them. [4] [7]
Prognosis & Disposition
Most healthcare-associated infections, recognised and treated promptly, resolve — but the patients who acquire them are the patients least able to tolerate the setback, and the morbidity, length of stay and cost are substantial. The prognosis is worst where the device and the host conspire: the very-low-birthweight neonate with a CLABSI, the neutropenic oncology patient with a line infection, the chronically ventilated child with VAP. For these patients, prevention is treatment, and the best disposition is the one that never became necessary. [6] [10]
Disposition follows the clinical state and the transmission risk. Admit or escalate the deteriorating child; manage the stable device-related infection with cultures, antibiotics and bundle review; and discharge the child whose isolation criteria are met. The decision to remove a child from isolation is a defined one — symptoms resolved for the required period, or criteria such as a negative test at the right interval — and the candidate should know the standing-down rules for common organisms rather than leaving the child isolated indefinitely. [4] [5]
At discharge, complete the bundle documentation, feed the case into surveillance, finish any contact tracing, and give the family a clear plan — including return precautions and, where relevant, the vaccination or stewardship conversation that prevents the next event. The discharge encounter is also a prevention opportunity, because the family who understands why their child needed isolation is the family who supports the system next time. [7] [4]
For the outbreak, disposition is the controlled stand-down: no new cases for the defined period, the environment cleaned, the cohort dispersed, the staff returned, and the event documented and reported. A well-managed outbreak ends with a debrief and a quality-improvement action — because the outbreak that is not learned from is the outbreak that recurs. [4] [8]
Special Populations
Neonates, especially in the NICU, carry the highest HAI burden because their skin, immune systems and devices concentrate the risk. The CLABSI bundle, unit-wide hand hygiene, minimal line handling, human-milk feeding where possible, and rigorous viral-respiratory containment are the NICU-specific defences, and the Polin AAP guidance and the SHEA NICU white paper are the references an examiner expects you to name. [5] [8]
Children with cancer and the immunocompromised depend on line-bundle reliability, protective isolation during neutropenia, vaccination of their household contacts, and prompt investigation of any new fever. They are the patients in whom a community-acquired virus becomes a life-threatening illness, and in whom antimicrobial stewardship must balance prophylaxis against resistance. [7] [10]
Technology-dependent children — those with tracheostomies, long-term ventilation, enteral feeds or indwelling catheters — live with chronic portals of entry. Their care plans must embed IPC into the home and the community as well as the hospital, with clear guidance on equipment cleaning, hand hygiene and recognition of infection. [5] [4]
Children with disability or neurodiversity may find isolation, PPE-clad staff and changes to routine especially distressing. Adapt the IPC plan to the child — familiar carers, sensory-friendly communication, time off isolation where clinically safe — so that infection control does not become trauma, and so the family remains a partner in care. [7] [8]
Aboriginal and Torres Strait Islander, Māori and other Indigenous children, and migrant, refugee and asylum-seeking families may face barriers to understanding and engaging with isolation. Provide culturally safe care, use trained interpreters rather than family members, and ensure that IPC does not compound existing inequity. Disadvantage must never be the reason a child acquires a preventable infection or is isolated without explanation. [4] [7]
Rural and remote children are cared for in smaller units with fewer single rooms and less on-site IPC capacity, and retrieval adds a layer of transmission risk. Plan for what is locally feasible, use telehealth to link IPC expertise, and escalate early — because a small unit cannot absorb an outbreak the way a large one can. [4] [8]
Evidence, Guidelines & Regional Differences
The global foundation is the World Health Organization's guidelines on hand hygiene in health care, which codified the "My 5 Moments" framework and the multimodal improvement strategy, and the Pittet consensus paper that set out their recommendations. The Allegranzi and Pittet review of hand hygiene's role in HAI prevention summarises the evidence that improving compliance lowers infection, and the Boyce and Pittet CDC/HICPAC guideline operationalised the practice for US healthcare. These are the documents a fellowship candidate should be able to cite by principle. [1] [3] [2]
Multistate point-prevalence survey of healthcare-associated infections
Population: A large point-prevalence survey across US acute-care hospitals, measuring the burden of healthcare-associated infections, their types and associated pathogens.
Key finding
About one in twenty-five hospitalised patients had a healthcare-associated infection on the survey day, with pneumonia and gastrointestinal infections leading; device-related and resistant-organism infections were prominent.
Practice change
The HAI burden is real, measurable and concentrated in device-bearing and vulnerable patients — which is why surveillance, bundles and standardised precautions are justified across every unit.
The prevention strategies are organised in the Yokoe compendium of strategies to prevent healthcare-associated infections in acute care hospitals, which presents the evidence-based recommendations for each HAI type as practical bundles. The paediatric- and NICU-specific evidence is set out in the Polin AAP guidance on NICU HAI prevention, the SHEA NICU white paper on viral respiratory infection prevention, the Coffin pediatric research priorities paper, and the Gerber ambulatory-surgery infection study — together defining what is known and where the gaps remain. [4] [5] [8] [9]
The regional policy structures are consistent in principle and varied in detail. In ANZ, the ACSQHC national standards and the NHMRC infection-control guidance govern practice, with national hand-hygiene auditing and notifiable-disease legislation defining the response. In the UK, NHS England and UK Health Security Agency guidance, with the code of practice on HAI prevention, set the framework. In the US, the CDC and HICPAC guidelines, with state-based reporting requirements, direct practice. In Canada, the Public Health Agency and provincial standards deliver the equivalent system. Everywhere the principle is the same: standard precautions for all, transmission-based precautions matched to the organism, device bundles, surveillance, and a structured outbreak response. [2] [4]
The controversies are active and important. How best to balance single-room capacity against cohorting when demand outstrips infrastructure; how far to screen and decolonise for resistant organisms; how to make bundles reliable under staffing pressure; how to integrate antimicrobial stewardship with IPC so that each reinforces the other; and how to ensure that isolation never becomes a vehicle for inequity or family exclusion. The defence against each is the same system thinking — surveillance, audit, feedback, just culture, and the willingness to act on the first signal. [7] [1]
Exam Pearls
- Standard precautions apply to every patient, every time — hand hygiene at the WHO 5 Moments, task-matched PPE, respiratory hygiene, sharps and waste safety, environmental cleaning. The dangerous patient is the one not yet identified. [3] [4]
- Transmission-based precautions are layered on top: contact (gown + gloves; MRSA, VRE, norovirus, RSV, C. difficile), droplet (surgical mask; influenza, pertussis), airborne (N95/P2 + negative pressure; measles, pulmonary TB, varicella). [4] [5]
- The chain of infection has six links — agent, reservoir, portal of exit, transmission, portal of entry, susceptible host — and every IPC measure breaks one link. [1] [4]
- Hand hygiene is the single most effective measure; alcohol rub is the default (20–30 s), but use soap and water for norovirus and C. difficile. [3] [1]
- Device infections are prevented by bundles, not antibiotics: CLABSI (maximal barrier, chlorhexidine, daily line review, scrub the hub), VAP (head-of-bed elevation, oral care, sedation holds), CAUTI (daily catheter review), SSI (perioperative bundle). [5] [4]
- CLABSI is the largest preventable HAI burden in the NICU — line days, gestational age and parenteral nutrition are the strongest risk factors. [10] [5]
- Isolate early on suspicion; do not wait for confirmation — containment is cheapest at the first signal. [4] [8]
- Outbreak response: recognise → case definition → confirm aetiology → implement controls → epidemic curve and line-list → communicate → evaluate and report. [4] [6]
- Norovirus needs soap-and-water hand washing and bleach cleaning — alcohol rub alone is insufficient. [4]
- Link IPC to stewardship, surveillance and vaccination — the measures that protect the susceptible host and slow resistance. [7] [4]
References
- [1]Allegranzi B; Pittet D Role of hand hygiene in healthcare-associated infection prevention. J Hosp Infect, 2009.PMID 19720430
- [2]Boyce JM; Pittet D; Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. MMWR Recomm Rep, 2002.PMID 12418624
- [3]Pittet D; Allegranzi B; Boyce J; WHO World Alliance for Patient Safety First Global Patient Safety Challenge Core Group of Experts The World Health Organization Guidelines on Hand Hygiene in Health Care and their consensus recommendations. Infect Control Hosp Epidemiol, 2009.PMID 19508124
- [4]Yokoe DS; Mermel LA; Anderson DJ; Arias KM; et al A compendium of strategies to prevent healthcare-associated infections in acute care hospitals. Infect Control Hosp Epidemiol, 2008.PMID 18840084
- [5]Polin RA; Denson S; Brady MT; Committee on Fetus and Newborn; Committee on Infectious Diseases Strategies for prevention of health care-associated infections in the NICU. Pediatrics, 2012.PMID 22451712
- [6]Magill SS; Edwards JR; Bamberg W; Beldavs ZG; et al Multistate point-prevalence survey of health care-associated infections. N Engl J Med, 2014.PMID 24670166
- [7]Coffin SE; Milstone AM; Zaoutis TE; Gerber JS; et al Pediatric research priorities in healthcare-associated infections and antimicrobial stewardship. Infect Control Hosp Epidemiol, 2021.PMID 33239122
- [8]Thampi N; Smith C; Mac S; Papenburg J; et al SHEA NICU white paper series: Practical approaches for the prevention of viral respiratory infections. Infect Control Hosp Epidemiol, 2024.PMID 37877172
- [9]Gerber JS; Zerr DM; Guthrie KA; Thomas ID; et al Infections after pediatric ambulatory surgery: Incidence and risk factors. Infect Control Hosp Epidemiol, 2019.PMID 30698133
- [10]Johnson J; Smith A; Martinez K; Reynolds S; et al Risk Factors for Health Care-Associated Bloodstream Infections in NICUs. JAMA Netw Open, 2025.PMID 40131271