Paeds · infectious-diseases
Infections in immunocompromised children
Also known as Febrile neutropenia · Opportunistic infection in children · Infection in the cancer or transplant child · Immunocompromised host infection · Overwhelming post-splenectomy infection
A fellowship-depth approach to infections in immunocompromised children: classify the immune-defect type and its signature organisms, understand why fever and signs are blunted, run the immunocompromised-fever threat gate first, deliver empiric therapy within 60 minutes, and manage organism-specific syndromes from fever-and-neutropenia through Pneumocystis, invasive fungal disease, CMV, adenovirus, central-line sepsis and overwhelming post-splenectomy infection.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A registrar hands you a child on chemotherapy who has spiked a fever at home. The child looks well, is playing on the bed, and the temperature is only 38.1 °C. The trap is to be reassured. The whole principle of this topic is that the missing immune compartment — whether neutrophils, T-cells, antibody, or spleen — removes the early-warning system that tells you a normal host is sick. Height of fever correlates poorly with serious bacterial infection even in immunocompetent children, and the relationship is weaker still when the inflammatory response itself is disabled. [4]
This page owns the approach to infections in immunocompromised children. It sits beside the sister pages on paediatric sepsis, fever by age and immune status, fungal infections, EBV and CMV, and antimicrobial stewardship. Those pages take the organism-specific depth; this page builds the unifying framework a fellowship candidate must defend at viva. [1] [14]
W.E.A.K. H.O.S.T.
Overview & Definition
An immunocompromised child is one whose immune system cannot mount the response a normal host would mount to the same organism. The compromise may be inherited, as in primary immunodeficiency; acquired, as in chemotherapy-induced neutropenia or HIV; iatrogenic, as in post-transplant immunosuppression; or structural, as in asplenia or the presence of an indwelling central venous catheter. What unites these children is a shared clinical problem: the usual signs of infection — fever, localising pain, pus, an inflammatory wall — are blunted or absent, so the window between treatable infection and overwhelming sepsis narrows. [1]
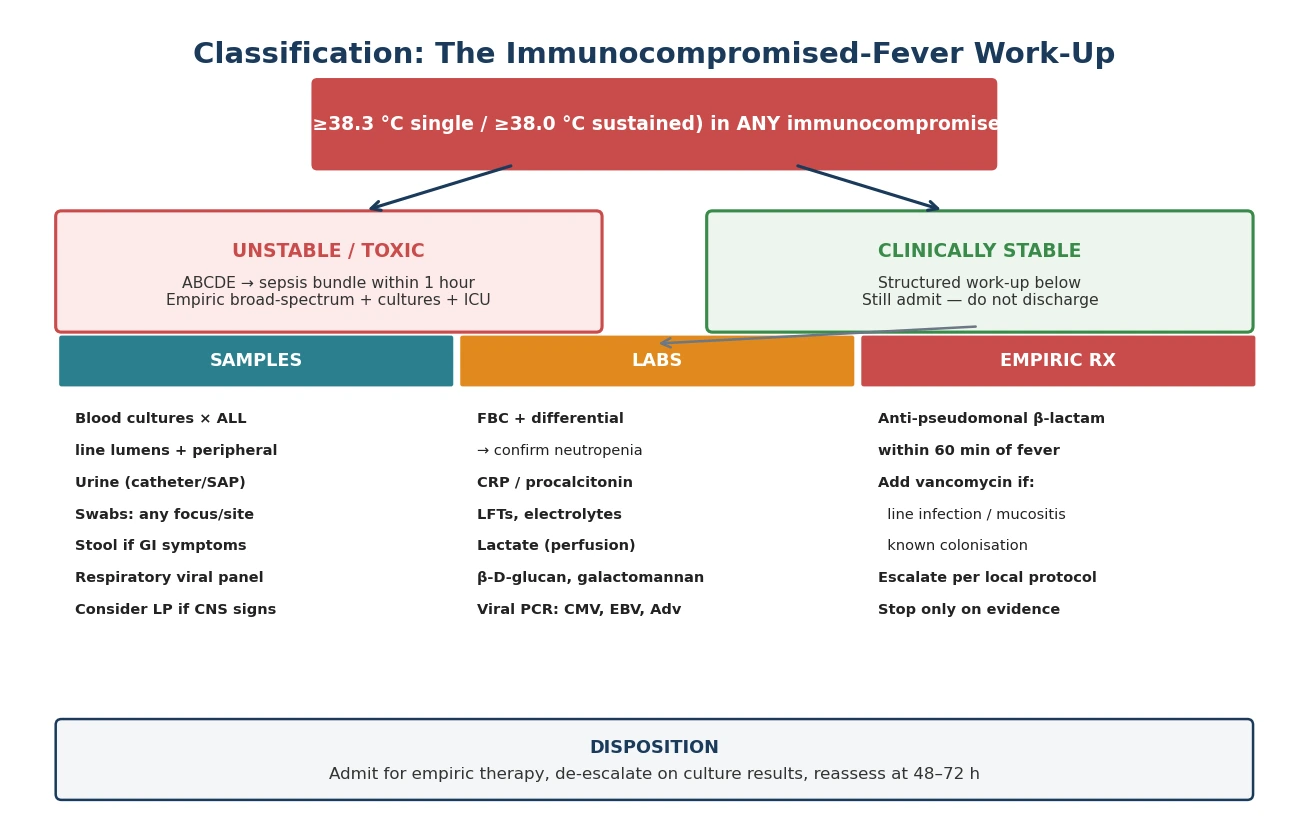
Fever in the immunocompromised host is defined operationally, not arbitrarily. In the febrile-neutropenia pathway, fever is a single oral or tympanic reading at or above 38.3 °C, or two readings at or above 38.0 °C taken at least an hour apart. Neutropenia — an absolute neutrophil count below 0.5 × 10⁹/L, or below 1.0 × 10⁹/L with an expected fall — is the qualifier that converts a febrile child into a febrile-neutropenic emergency. The definition matters because the threshold triggers an entire pathway that does not wait for proof of infection. [1]
Classification
The most useful classification for the bedside is by which immune compartment is missing, because each compartment fails against a predictable set of organisms. The four categories — neutropenic, T-cell defective, humoral defective, and device or mucosal barrier compromised — overlap in real patients (a child on day 10 post-HSCT has all four), but they organise your differential and your empiric therapy. [1] [14]
Immune-defect categories and their signature organisms
A second axis — the post-HSCT timeline — re-classifies risk in stem-cell transplant recipients. Srinivasan and colleagues mapped how bacterial, fungal, and viral infections cluster across the pre-engraftment, early (day 0 to 100), and late (beyond day 100) periods. The neutropenia dominates the first period, acute graft-versus-host disease and its immunosuppression dominate the second, and chronic graft-versus-host disease with slow immune reconstitution dominates the third. [14]
Why this matters: key numbers
Epidemiology & Risk Factors
Infection remains a leading cause of non-relapse mortality in paediatric oncology and stem-cell transplant recipients despite modern prophylaxis. The risk is concentrated in the periods of deepest immune suppression: induction and consolidation chemotherapy for leukaemia, the pre-engraftment neutropenic window after HSCT, and the treatment of graft-versus-host disease with corticosteroids and calcineurin inhibitors. [1] [14]
Central venous catheters are the single largest modifiable risk factor for bloodstream infection in this population. Bavare's recent paediatric review describes how biofilm formation on the catheter surface, repeated line access for therapy and blood sampling, and the loss of skin barrier integrity converge to produce central-line-associated bloodstream infection. The attributable harm is substantial — prolonged admission, line removal, missed chemotherapy cycles, and excess mortality. [11]
Risk factors and how they raise infection risk
Primary immunodeficiency syndromes are rarer but critical to recognise because they present with recurrent, severe, or unusual infections that should prompt immunological referral rather than another round of empirical antibiotics. Severe combined immunodeficiency presents in infancy with failure to thrive, chronic diarrhoea, and opportunistic infection; chronic granulomatous disease presents with recurrent abscesses and lymphadenitis from catalase-positive organisms; agammaglobulinaemia produces recurrent sinopulmonary infection with encapsulated bacteria. [14]
Pathophysiology
In the normal host, infection follows a predictable cascade. Neutrophils and macrophages engulf and kill invading organisms within minutes; cytokines such as interleukin-1, interleukin-6, and tumour necrosis factor-alpha reset the hypothalamic set-point to generate fever; antibody and T-cell responses then clear the organism and provide memory. Fever, localising pain, erythema, and pus are the visible signs that this cascade is working. [4]
The immunocompromised host breaks this cascade at different points depending on the missing compartment, and the clinical consequence is the same each time: the warning signs are lost. Remove the neutrophils, and gram-negative organisms multiply unchecked with no pus and little localising pain. Remove the T-cells, and intracellular opportunists — Pneumocystis, CMV, mycobacteria — establish tissue-invasive disease that the host cannot wall off. Remove the antibody or the spleen, and encapsulated bacteria replicate in the bloodstream faster than the reticuloendothelial system can clear them. [1] [14]
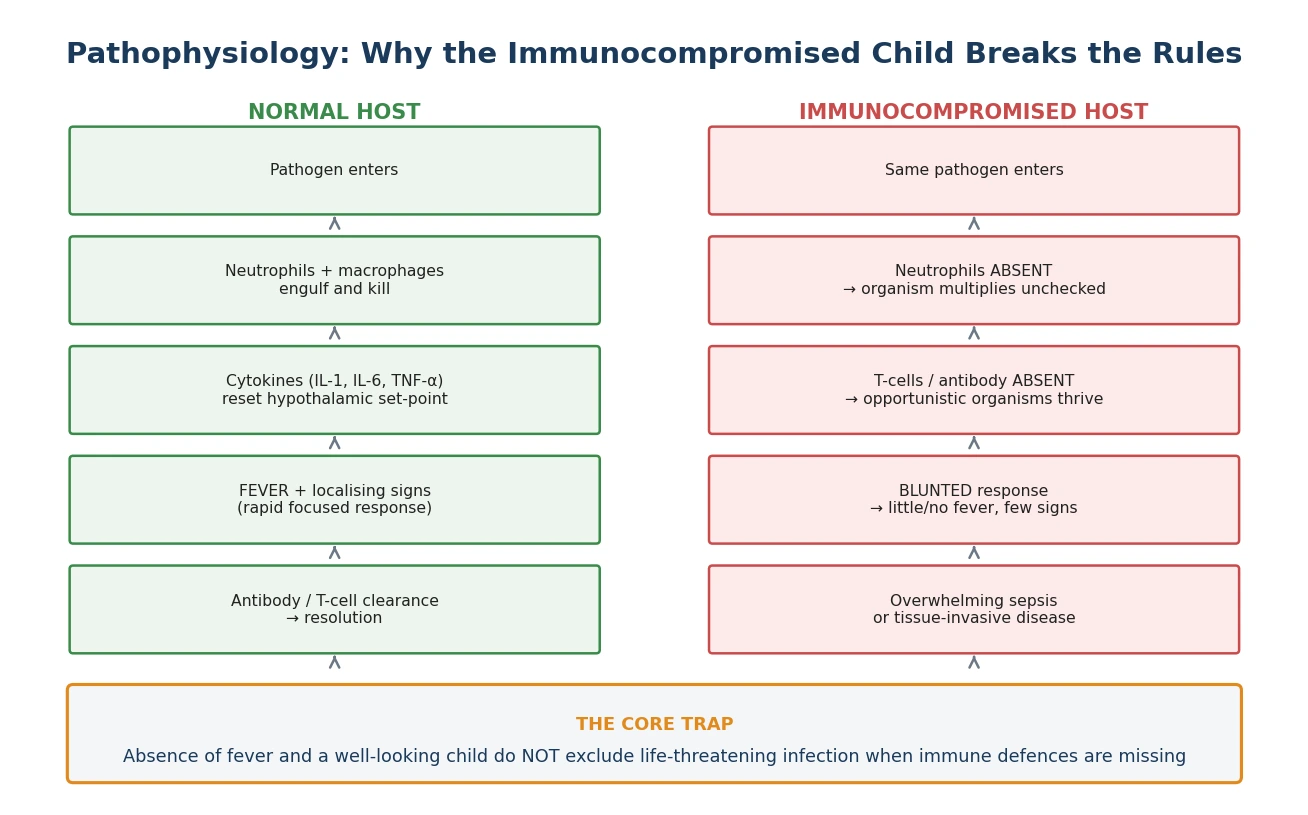
The blunted inflammatory response is the central trap. De and colleagues confirmed that body temperature lacks accuracy for detecting serious bacterial infection even in immunocompetent febrile children; in the immunocompromised child the relationship is weaker still. Hypothermia, rather than fever, can be the presentation of sepsis in the neutropenic or transplant host. A child who is afebrile but tachypnoeic, or who has simply become less interactive than their chronically-ill baseline, may have overwhelming infection. The corollary that drives management is simple: you cannot use the clinical appearance to defer investigation or therapy in these children. [4]
Central venous catheters add a mechanical pathophysiology. Organisms gain access along the catheter tract from the skin, or seed the intraluminal surface during line manipulation, and then form a biofilm that is resistant both to neutrophil killing and to antibiotic penetration. Once a biofilm is established, systemic therapy alone may fail and line removal becomes necessary. Gut mucosal disruption — from chemotherapy mucositis or graft-versus-host disease — provides a parallel translocation route for enteric gram-negatives, enterococci, and Candida. [11]
Clinical Presentation
The febrile neutropenic child most often presents with fever alone, or with vague non-specific symptoms that would be dismissed in an immunocompetent host — mild lethargy, reduced oral intake, a single loose stool, or a slightly raised respiratory rate. The child may look entirely well and be playing at the moment of assessment. The discipline of this topic is to act on the fever and the immune status, not on the appearance. [1]
Atypical presentations are the rule, not the exception. Hypothermia in a neutropenic or transplant child is a sepsis sign until proven otherwise. Subtle confusion, a fall in baseline interaction, or isolated tachypnoea may be the only clue. Pain or erythema at a central-line exit site is a line infection until cultures prove otherwise, even when the child is afebrile. Perianal pain or cellulitis in a neutropenic child signals a surgical emergency that needs broad empiric cover because the neutrophil response that would normally localise the infection is absent. [11]
In Australian and New Zealand practice, retrieval networks move immunocompromised children from rural and remote centres to tertiary oncology and transplant services. The first dose of empiric therapy should be given before and during retrieval; waiting for transfer without treatment is a recognised cause of preventable death. Telehealth links between rural centres and oncology teams help with early risk decisions. [1]
Organism-specific presentations follow the immune-defect pattern. Pneumocystis pneumonia classically produces hypoxaemia that is disproportionate to the chest auscultation findings — the child is desaturating but the chest sounds clear, and the picture worsens rapidly over hours. Invasive aspergillosis declares itself as persistent fever despite broad-spectrum antibiotics, with new pulmonary nodules on imaging, sinus pain, or cutaneous lesions; a halo sign or air-crescent sign on chest CT suggests angioinvasive disease. Invasive candidiasis may produce a new fever, skin nodules, or endophthalmitis in the persistently neutropenic child. [6] [10]
Differential Diagnosis
The differential in the febrile immunocompromised child is deliberately broad, because the missing immune compartment opens the door to organisms a normal host would never acquire. Gram-negative bacteraemia — especially Pseudomonas aeruginosa — is the immediate life-threat that empiric therapy is designed to cover. Gram-positive line infections, invasive fungal disease, viral reactivation, and opportunistic pneumonia must all stay open simultaneously, and the work-up is structured to sample for all of them at once. [1]
Non-infectious causes must also sit in the differential, because treating them as infection wastes time and exposes the child to unnecessary therapy. Drug fever, blood-product transfusion reaction, leukaemic or post-transplant lymphoproliferative infiltration, graft-versus-host disease, cytokine release, and haemophagocytic lymphohistiocytosis can all produce fever that mimics infection. The distinguishing features are the tempo, the response to anti-infective therapy, and the specific syndrome — but the default in the unstable or early-presentation child is always to treat as infection first and revise later. [1] [14]
Differential by immune-defect type — must-not-miss organisms
Clinical & Bedside Assessment
The first-impression assessment is the threat gate and it overrides everything else. The paediatric assessment triangle — appearance, work of breathing, and circulation to skin — identifies the toxic or shocked child within seconds. Any derangement sends the child straight to the sepsis bundle: oxygen, intravenous access, fluid boluses, early vasoactives, and empiric therapy within the hour, with PICU involvement from the outset. [2] [3]
In the clinically stable child, the focused examination is directed at the high-yield sites that the immunocompromised host cannot localise on their own. Examine the central-line exit site and tunnel for erythema, swelling, tenderness, or discharge. Inspect the perianal area for cellulitis or fissure — this is easy to miss and changes the empiric therapy. Examine the oral mucosa for mucositis, the skin for embolic or fungal lesions, the sinuses for tenderness, and perform fundoscopy where invasive candidiasis is suspected. Caregiver concern that the child has changed from their chronically-ill baseline is data, not anxiety, and should escalate the assessment. [4] [11]
The focused immunocompromised-fever examination (5 high-yield sites)
The problem representation that follows a complete assessment names the immune-defect type and commits to the emergency pathway. A useful synthesis is: "This is a six-year-old with ALL on maintenance therapy, now profoundly neutropenic with fever at 38.5 °C and a clean line site — this is febrile neutropenia and I am activating the pathway now." That sentence commits you to cultures, empiric therapy, and admission, regardless of how well the child looks. [1]
Investigations
The investigation bundle is taken in parallel, not sequentially, because empiric therapy must not wait for results. Blood cultures are drawn from every lumen of a central venous catheter and from a separate peripheral site — the paired comparison tells you whether the line is the source. A full blood count with differential confirms the current neutrophil depth; a count from days ago is not acceptable because counts fall quickly during chemotherapy. CRP and procalcitonin are supportive but never gate the decision to treat. Lactate assesses perfusion and occult shock. [1] [11]
Targeted investigations follow the clinical leads and the immune-defect pattern. Urine is sent by catheter or suprapubic aspirate, never by bag, in the immunocompromised child. Stool is sent if there are gastrointestinal symptoms. A respiratory viral panel is taken if there are respiratory signs, because viral infections in the transplant host can be as dangerous as bacterial sepsis. Beta-D-glucan and galactomannan are sent when invasive fungal disease is suspected; viral PCR panels for CMV, EBV, and adenovirus are sent in the transplant host. [6] [13]
A lumbar puncture is not routine in febrile neutropenia, but it is indicated when there are central nervous system signs — altered consciousness, meningism, seizures, or a new focal deficit. It is contraindicated in the unstable child until resuscitation is complete, and in the thrombocytopenic child until the platelet count is corrected. Where focal neurological signs are present, imaging must precede the lumbar puncture. [1]
Imaging is directed by the clinical question. A chest radiograph is the first step in the child with respiratory signs, but a normal radiograph does not exclude Pneumocystis or early invasive fungal disease — high-resolution or contrast chest CT is more sensitive for the nodular, halo, and crescent signs of fungal infection. Sinus CT is indicated when invasive fungal sinusitis is suspected. Abdominal ultrasound or CT is indicated for typhlitis, hepatosplenic candidiasis, or a suspected intra-abdominal focus. [6] [10]
Management — Resuscitation
The unstable immunocompromised child is managed with the paediatric sepsis bundle. The Surviving Sepsis Campaign 2020 (paediatric) guideline and the Phoenix sepsis criteria provide the operational framework: within the first hour, obtain access, take cultures, give a fluid bolus of 10 to 20 mL/kg of isotonic crystalloid, start empiric broad-spectrum therapy, and add early vasoactives — peripheral adrenaline or noradrenaline — if shock persists after the first fluid bolus. PICU is involved from the outset, not as a last resort. [2] [3]
First-hour sepsis bundle for the immunocompromised child
Recognise: any fever (or hypothermia) in a neutropenic, transplant, asplenic, or primary-immunodeficiency child is sepsis until proven otherwise
Access: intravenous or intraosseous within minutes; draw blood cultures from every line lumen and a peripheral site before antibiotics
Resuscitate: oxygen for hypoxaemia or shock; 10–20 mL/kg isotonic crystalloid bolus, reassess after each
Empiric therapy: anti-pseudomonal beta-lactam within 60 minutes of fever recognition
Add vasoactives early: peripheral adrenaline or noradrenaline if shock persists after the first fluid bolus
Escalate: PICU, oncology or transplant team, infectious diseases and microbiology — simultaneously, not sequentially
The principle that overrides every nuance is this: appearance is not a gate. The well-looking neutropenic child gets the same empiric therapy as the toxic one, because the neutrophil compartment that would produce visible toxicity is absent. Waiting for the child to look unwell before treating is the single most dangerous error in this topic. [1] [4]
Management — Definitive & Stepwise
Definitive management follows the empiric start and is shaped by the immune-defect type, the culture and PCR results, and the clinical course. The 2023 international fever-and-neutropenia guideline sets the framework: empiric monotherapy with an anti-pseudomonal beta-lactam is standard; a second gram-negative agent or gram-positive cover is added in specific circumstances; and antifungal escalation is considered for persistent fever. [1]
Empiric gram-positive cover — with vancomycin or another agent — is added when there is clinical or microbiological evidence of a line infection, severe mucositis, known colonisation with resistant organisms, haemodynamic instability, or a soft-tissue or skin focus. It is not added routinely to every febrile-neutropenic child, because routine addition has not improved outcomes and broadens toxicity and resistance. [1]
Empiric anti-pseudomonal beta-lactam (febrile neutropenia)
Dose
Agent, dose, route, frequency and duration are set by the local oncology or transplant protocol and must be confirmed against current local guidelines before administration
Antifungal escalation is considered when fever persists despite four or more days of broad-spectrum antibacterial therapy. The ECIL-8 paediatric invasive fungal disease guideline and the global candidiasis guideline inform the choice between mould-active triazoles (voriconazole, posaconazole, isavuconazole), echinocandins, and liposomal amphotericin B, guided by galactomannan and beta-D-glucan results, imaging findings, and the child's organ function. [6] [7]
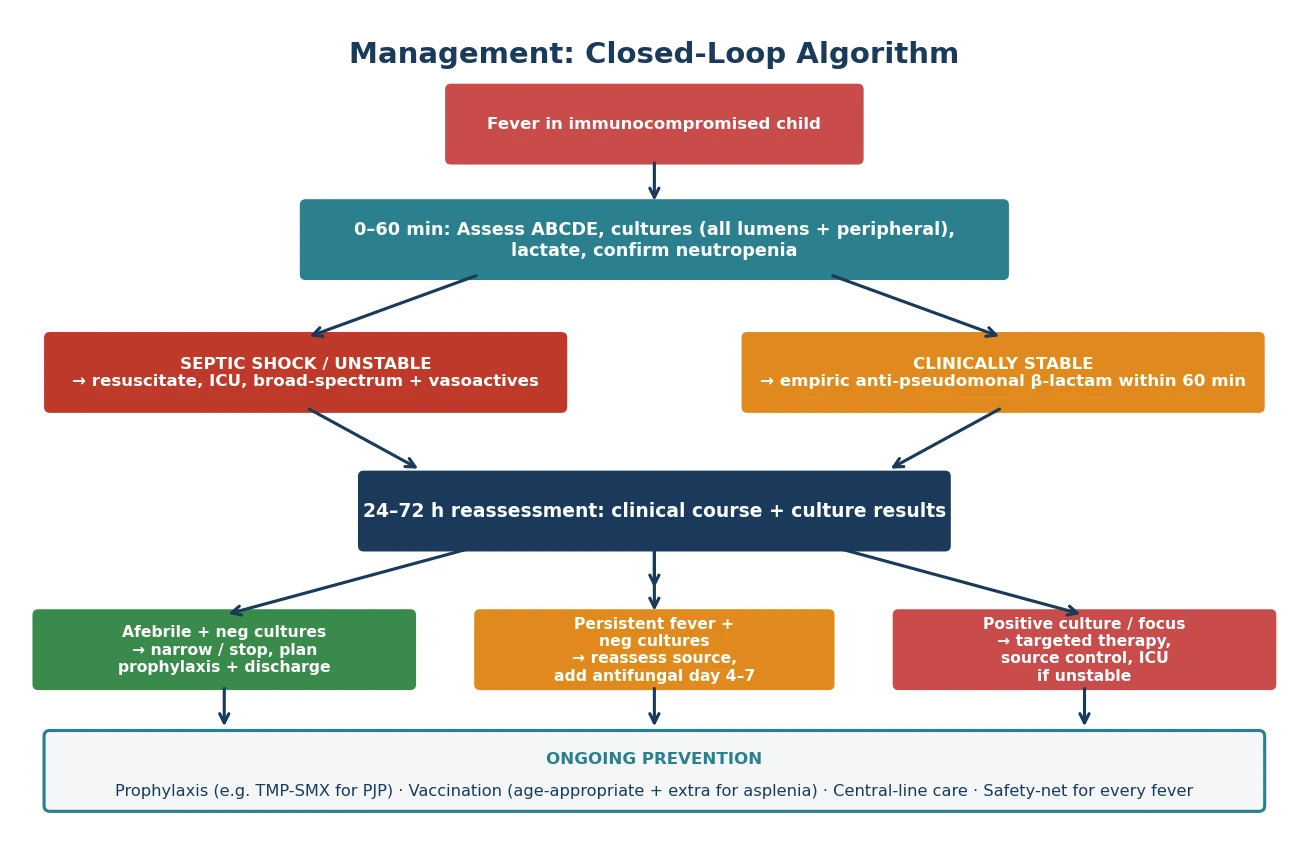
De-escalation is the discipline of narrowing therapy as evidence accrues. When a focus and organism are identified, therapy is narrowed to the most targeted effective agent. When cultures remain negative and the child defervesces, therapy is stopped at the protocol-defined interval — continued broad-spectrum therapy in the afebrile, culture-negative child adds toxicity and resistance without benefit. When fever persists with negative cultures, the source is actively re-sought with imaging, repeat biomarkers, and a reconsideration of the differential. [1]
Prophylaxis prevents the common opportunistic infections and is a core management responsibility. Trimethoprim-sulfamethoxazole prophylaxis against Pneumocystis is standard for children receiving chemotherapy, after HSCT, and on prolonged high-dose corticosteroids; the ECIL guideline confirms its effectiveness in haematological malignancy and stem-cell transplant recipients. Antiviral prophylaxis (for example, with a nucleoside analogue active against herpesviruses) and antifungal prophylaxis are layered on according to the transplant phase and the underlying disease. [8] [9]
Specific Subtypes & Scenarios
Fever and neutropenia in paediatric oncology
The 2023 guideline (Lehrnbecher) is the single most important operational document for this scenario. It defines the fever and neutropenia thresholds, mandates empiric anti-pseudomonal therapy within 60 minutes, sets the indications for gram-positive cover, and addresses the controversial question of outpatient management in selected low-risk children. The low-risk pathway — where a child is stable, culture-negative at 48 hours, without a focus, and meets protocol-defined criteria — may allow step-down to oral or outpatient therapy, but only under a structured programme with reliable follow-up. [1]
Pneumocystis jirovecii pneumonia
Pneumocystis pneumonia is the archetypal T-cell-defect infection. It presents with progressive dyspnoea, hypoxaemia disproportionate to the chest findings, and a rapidly worsening picture over hours to days. The chest radiograph may be normal or show bilateral perihilar infiltrates; a normal radiograph does not exclude the diagnosis. Diagnosis rests on respiratory sampling with immunofluorescence or PCR. Treatment is high-dose trimethoprim-sulfamethoxazole, with adjunctive corticosteroids for moderate-to-severe hypoxaemia, and the ECIL prophylaxis guideline confirms that routine trimethoprim-sulfamethoxazole prophylaxis prevents most cases in at-risk groups. [8]
Invasive aspergillosis and candidiasis
Invasive aspergillosis is suspected in the persistently febrile neutropenic child with new pulmonary nodules, a halo sign or air-crescent sign on chest CT, sinus involvement, or cutaneous lesions. Galactomannan testing on serum or bronchoalveolar lavage supports the diagnosis. Hsu and colleagues describe the paediatric treatment challenges — voriconazole is the first-line agent, with therapeutic drug monitoring essential because of variable pharmacokinetics in children, and alternatives including liposomal amphotericin B and isavuconazole. The global candidiasis guideline addresses invasive candidiasis, where echinocandins and liposomal amphotericin B are central, guided by species and susceptibility. [6] [7] [10]
CMV in solid-organ and stem-cell transplant
Cytomegalovirus is one of the most important opportunistic pathogens in transplantation. The third international consensus guideline for solid-organ transplant (Kotton) sets out the preemptive and prophylactic strategies: quantitative CMV PCR monitoring with preemptive therapy when viral replication is detected, versus universal prophylaxis in the early post-transplant period. Treatment of established disease uses intravenous ganciclovir or oral valganciclovir, with resistance managed by specialist transplant-infectious-disease teams. In stem-cell transplant, CMV reactivation occurs predominantly in the early to late period and is monitored with serial PCR. [9] [14]
Adenovirus in HSCT
Adenovirus can cause disseminated disease — hepatitis, pneumonitis, enteritis, and encephalitis — in the allogeneic HSCT recipient, particularly in the context of T-cell-depleted grafts and graft-versus-host disease. Cesaro and colleagues describe how serial quantitative PCR monitoring allows preemptive intervention before end-organ disease develops. Cidofovir and brincidofovir are the antiviral agents with activity against adenovirus, used in transplant protocols when viraemia rises or end-organ disease appears; the reduction of immunosuppression, where possible, is central to control. [13]
Central-line-associated bloodstream infection
Central-line infection is diagnosed when the same organism grows from the line and peripheral cultures, or when the line culture turns positive much earlier than the peripheral (a positive differential-time-to-positivity). Coagulase-negative staphylococci are the commonest organisms, but Staphylococcus aureus, enterococci, gram-negatives, and Candida species all occur. Line salvage with systemic therapy and an antibiotic or ethanol lock may succeed for uncomplicated coagulase-negative staphylococcal infection, but Bavare's review makes clear that line removal is required for tunnel infection, port-pocket abscess, persistent bacteraemia, septic thrombophlebitis, endocarditis, or any S. aureus, Pseudomonas, or Candida line infection. [11]
Overwhelming post-splenectomy infection
The asplenic or hyposplenic child — anatomically splenectomised, or functionally hyposplenic from sickle cell disease — cannot clear encapsulated bacteria from the bloodstream. Overwhelming post-splenectomy infection is the feared outcome: a well-looking child with fever who progresses to septic shock and death within hours. Lee's review of infection prevention in asplenia sets out the three-part prevention pathway — vaccination against pneumococcus, meningococcus, and Haemophilus influenzae type b; penicillin prophylaxis, especially in young children; and a written, rehearsed fever action plan that tells the family to present immediately for any fever. Every fever in an asplenic child is an emergency on the same footing as febrile neutropenia. [12]
Complications & Pitfalls
The classic errors cluster around two themes: trusting appearance, and delaying therapy for investigation. The well-looking neutropenic child who is sent home, the child whose empiric therapy is withheld until cultures are taken in a distant department, the line-lumen culture that is omitted, and the failure to reassess at 48 to 72 hours are all recognised, preventable causes of death. The discipline of this topic is to act on the fever and the immune status immediately. [1]
Antifungal and antiviral therapy carry their own toxicity. Amphotericin B causes nephrotoxicity and electrolyte disturbance; voriconazole causes hepatotoxicity, neurotoxicity, and photosensitivity, and requires therapeutic drug monitoring; ganciclovir causes marrow suppression and nephrotoxicity. These toxicities compound the toxicity of the underlying chemotherapy or transplant immunosuppression, and they are the reason that prophylaxis is targeted rather than universal. [6] [10]
Line-management decisions are a frequent source of error. Leaving an infected line in place too long risks persistent bacteraemia, endocarditis, and septic thrombophlebitis; removing a salvageable line unnecessarily subjects the child to anaesthesia and the loss of venous access that may be hard to replace. The decision is governed by the organism, the presence of tunnel or pocket involvement, the response to therapy, and the persistence of bacteraemia. [11]
Missing Pneumocystis or invasive fungal disease because the initial chest radiograph was normal is a recurring pitfall. The discipline is to pursue imaging — high-resolution or contrast chest CT — when the clinical suspicion is high, and to treat empirically for Pneumocystis in the hypoxaemic T-cell-defective child while the diagnostic work-up proceeds. Immune reconstitution inflammatory syndrome and engraftment syndrome can masquerade as infection during the post-transplant recovery, producing fever and pulmonary infiltrates as the immune system recovers, and they require specialist transplant-team distinction from relapsing infection. [8] [10]
Prognosis & Disposition
Outcome in febrile neutropenia is determined by four factors: the time to antibiotic, the virulence of the organism, the depth and duration of neutropenia, and the status of the underlying disease. Prompt empiric therapy has the largest single effect, and it is the factor most under the clinician's control. Pseudomonas bacteraemia and invasive fungal disease carry the highest mortality. [1]
Admission is the default for every febrile neutropenic, transplant, and asplenic child. The 2023 guideline addresses the controversial question of outpatient or step-down management: selected low-risk children — clinically stable, culture-negative at 48 hours, without a focus, meeting protocol-defined criteria, and with reliable follow-up — may be managed in a structured outpatient programme. This is never a default for the unstable, the deeply neutropenic, the child with a comorbid focus, or the child whose family cannot return immediately. [1]
The safety-net for any discharged immunocompromised child must be specific and rehearsed. The family is told to return immediately for any fever, any new pain or rash, any breathing difficulty, or any parental concern that the child is worse. For the asplenic child, the fever action plan is explicit: any fever is an emergency, present immediately, state the asplenia, and expect empiric therapy within the hour. [12]
Follow-up coordinates the oncology or transplant team, infection prevention, prophylaxis adherence, and vaccination catch-up. Prophylaxis adherence is a common failure point, especially in adolescents, and it should be checked at every contact. Vaccination catch-up after chemotherapy or transplant follows a specialist schedule, because live vaccines are contraindicated during active immunosuppression and additional vaccines are needed for the asplenic child. [8] [12]
Special Populations
The neonate or infant who is also immunocompromised is doubly high-risk. A febrile neonate on chemotherapy, or a transplant recipient in early infancy, combines the immature immunity that already places neonates at high risk of serious bacterial infection with the added deficit of treatment. The work-up is the full neonatal septic bundle plus the immunocompromised-fever pathway, and the threshold for PICU involvement is lower. [5]
Primary immunodeficiency syndromes change the organism spectrum and the prophylaxis strategy. Severe combined immunodeficiency requires isolation and urgent referral for haematopoietic stem cell rescue; chronic granulomatous disease requires antibacterial and antifungal prophylaxis against catalase-positive organisms; agammaglobulinaemia and common variable immunodeficiency require immunoglobulin replacement and vigilance for enteroviral meningoencephalitis. The clue is recurrent, severe, or unusual infection, and the response is immunological referral rather than another empirical antibiotic course. [14]
Asplenia and functional hyposplenism — from sickle cell disease, hereditary spherocytosis, or surgical splenectomy — require a dedicated prevention pathway. Lee's review sets out the three pillars: age-appropriate plus additional vaccination against pneumococcus, meningococcus, and Haemophilus influenzae type b; penicillin prophylaxis, especially in children under five years and for the first years after splenectomy; and a written, rehearsed fever action plan. Sickle cell disease adds functional hyposplenism early in life, so the pathway begins in infancy. [12]
Solid-organ transplant recipients differ from HSCT recipients in timeline and organism risk. The SOT child is never neutropenic to the same degree, but is on lifelong calcineurin-inhibitor-based immunosuppression, with the highest opportunistic-infection risk in the first six months and ongoing risk for the life of the graft. The HSCT child passes through a neutropenic pre-engraftment period, an early graft-versus-host-disease period, and a late reconstitution period, with different organisms in each. [9] [14]
Transplant timelines compared
Evidence, Guidelines & Regional Differences
The evidence base is anchored by a set of consensus guidelines that a fellowship candidate must be able to name. The 2023 international fever-and-neutropenia guideline (Lehrnbecher) governs the oncology and HSCT fever pathway. The ECIL-8 paediatric invasive fungal disease guideline (Groll) governs fungal diagnosis, prevention, and treatment in children with cancer or post-HSCT. The ECIL PJP prophylaxis guideline (Maertens) and the global candidiasis guideline (Cornely) address organism-specific prevention and management. The CMV consensus guideline for solid-organ transplant (Kotton) sets the preemptive and prophylactic strategy. The Surviving Sepsis Campaign 2020 (paediatric) guideline (Weiss) and the Phoenix sepsis criteria (Schlapbach) govern the sepsis bundle. [1] [3] [6] [7] [8] [9]
The live controversies are three. First, the routine addition of empirical gram-positive cover to every febrile-neutropenic regimen: the evidence does not support routine addition, and the practice broadens toxicity and resistance without improving outcomes, so gram-positive cover is reserved for specific indications. Second, outpatient management of low-risk febrile neutropenia: structured programmes in selected centres show safety, but the eligibility criteria are strict and the approach is not generalisable to every setting. Third, the choice between universal antifungal prophylaxis and a preemptive biomarker-driven strategy in the high-risk transplant period: the decision depends on the underlying disease, the local epidemiology, and the centre's experience. [1] [6]
ANZ and Canadian pathways follow the same international consensus but adapt empiric-agent choice to local antibiograms and to the rural and remote retrieval context. The principle — empiric anti-pseudomonal therapy within 60 minutes and admission — is invariant across regions; the specific agent varies. [1]
Biomarkers — CRP, procalcitonin, galactomannan, beta-D-glucan — are supportive but never gate the initial decision. Their evidence base is strongest for galactomannan in invasive aspergillosis and weakest for CRP and procalcitonin as triage tools in the febrile-neutropenic child. They inform escalation and de-escalation once the initial pathway is underway, not the decision to start it. [6]
Exam Pearls
The organism-defect pairings are the classic written-exam stems, and they should be automatic. Neutropenia pairs with Pseudomonas aeruginosa. T-cell defect pairs with Pneumocystis jirovecii and CMV. Humoral defect and asplenia pair with encapsulated bacteria — Streptococcus pneumoniae, Haemophilus influenzae type b, Neisseria meningitidis. A central venous catheter pairs with coagulase-negative staphylococci and Candida. Chronic granulomatous disease pairs with catalase-positive organisms such as Staphylococcus aureus, Serratia, and Aspergillus. [1] [12] [14]
The frequently misremembered facts, corrected: the single-reading fever threshold in neutropenia is 38.3 °C, not 38.0 °C; the sustained threshold is two readings at or above 38.0 °C at least an hour apart. Gram-positive cover is not added to every febrile-neutropenic regimen — it is reserved for line infection, mucositis, known colonisation, or instability. Empiric therapy is given within 60 minutes, not after cultures return. A normal chest radiograph does not exclude Pneumocystis or invasive fungal disease. [1]
Vaccination rules in the immunocompromised child are a recurring short-case and communication station. Live vaccines — measles-mumps-rubella, varicella, rotavirus, live-attenuated influenza, BCG — are contraindicated during chemotherapy and during high-level post-transplant immunosuppression. The asplenic child needs additional vaccination against pneumococcus, meningococcus (including serogroup B), and Haemophilus influenzae type b, on top of the routine schedule. Vaccination catch-up after chemotherapy or transplant follows a specialist schedule, timed to immune reconstitution. [12]
References
- [1]Lehrnbecher T Guideline for the Management of Fever and Neutropenia in Pediatric Patients With Cancer and Hematopoietic Cell Transplantation Recipients: 2023 Update. Journal of clinical oncology, 2023.PMID 36689694
- [2]Schlapbach LJ International Consensus Criteria for Pediatric Sepsis and Septic Shock. JAMA, 2024.PMID 38245889
- [3]Weiss SL Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026. Pediatric critical care medicine, 2026.PMID 41869844
- [4]De S Lack of Accuracy of Body Temperature for Detecting Serious Bacterial Infection in Febrile Episodes. The Pediatric infectious disease journal, 2015.PMID 26065864
- [5]Biondi EA Prevalence of Bacteremia and Bacterial Meningitis in Febrile Neonates and Infants in the Second Month of Life: A Systematic Review and Meta-analysis. JAMA network open, 2019.PMID 30901044
- [6]Groll AH 8th European Conference on Infections in Leukaemia: 2020 guidelines for the diagnosis, prevention, and treatment of invasive fungal diseases in paediatric patients with cancer or post-haematopoietic cell transplantation. The Lancet. Oncology, 2021.PMID 33811813
- [7]Cornely OA Global guideline for the diagnosis and management of candidiasis: an initiative of the ECMM in cooperation with ISHAM and ASM. The Lancet. Infectious diseases, 2025.PMID 39956121
- [8]Maertens J ECIL guidelines for preventing Pneumocystis jirovecii pneumonia in patients with haematological malignancies and stem cell transplant recipients. The Journal of antimicrobial chemotherapy, 2016.PMID 27550992
- [9]Kotton CN The Third International Consensus Guidelines on the Management of Cytomegalovirus in Solid-organ Transplantation. Transplantation, 2018.PMID 29596116
- [10]Hsu AJ Challenges in the Treatment of Invasive Aspergillosis in Immunocompromised Children. Antimicrobial agents and chemotherapy, 2022.PMID 35766509
- [11]Bavare AC Central Line-Associated Bloodstream Infections in Pediatrics: A Review. Pediatrics in review, 2025.PMID 40875258
- [12]Lee GM Preventing infections in children and adults with asplenia. Hematology. American Society of Hematology. Education Program, 2020.PMID 33275684
- [13]Cesaro S Adenovirus infection in allogeneic hematopoietic cell transplantation. Transplant infectious disease, 2023.PMID 37846850
- [14]Srinivasan A Timeline, epidemiology, and risk factors for bacterial, fungal, and viral infections in children and adolescents after allogeneic hematopoietic stem cell transplantation. Biology of blood and marrow transplantation, 2013.PMID 22922523