Paeds · infectious-diseases
Influenza and antiviral treatment
Also known as Seasonal influenza in children · Flu (paediatric) · Influenza A and B in children · Oseltamivir and baloxavir treatment of influenza · Paediatric influenza pneumonia and encephalopathy
Fellowship topic on influenza and antiviral treatment in children: the influenza A and B viruses and their seasonal epidemiology; abrupt febrile presentation and the atypical infant and high-risk presentations; viral and secondary bacterial pneumonia, encephalopathy and the other complications; PCR and rapid testing interpreted in context; stepwise management from supportive care of the hospitalised child through early oseltamivir and baloxavir, who to treat and when; post-exposure prophylaxis; and annual plus maternal vaccination as the prevention backbone — with ANZ, UK, US and Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
FLU — who you must treat, not wait on
Overview & Definition
Picture a three-year-old brought to the emergency department in mid-winter with a high fever, a dry cough and aching legs, who has been well until that morning. The suddenness is the clue — influenza does not creep in the way a common cold does, it arrives all at once. Recognising that pattern, and knowing when to escalate from reassurance to antiviral treatment, is the skill this topic builds. [2] [3]
Influenza is an acute infection of the respiratory tract caused by influenza A or B viruses (family Orthomyxoviridae), spread by respiratory droplets and by contact with contaminated surfaces. It causes recurrent seasonal winter epidemics and, periodically, pandemics. In older children and adults it is a self-limiting febrile illness; in infants and in children with chronic medical conditions it is a leading cause of hospitalisation, intensive-care admission and death. [2] [3]
The clinician's task has three parts. The first is to recognise influenza and triage severity — who can be managed at home and who is heading for the ward or the intensive-care unit. The second is to treat early with antivirals in the right patients, alongside supportive care and active management of complications. The third is prevention through annual vaccination, maternal vaccination and infection control, because the child who never reaches hospital is the child the immunisation programme has protected. [3] [10]
Classification
Sort influenza the way it presents at the bedside — by the infecting virus, then by the host and severity — because each axis changes the management. By virus, influenza A is subtyped by its surface glycoproteins, haemagglutinin (H) and neuraminidase (N), with A/H1N1 and A/H3N2 the circulating seasonal strains. Influenza B separates into two lineages, Victoria and Yamagata, and affects humans only. Influenza A undergoes both antigenic drift — small gradual changes that drive annual vaccine updates — and antigenic shift, the abrupt reassortment that can seed a pandemic; influenza B drifts only. [2] [3]
The second axis is the child in front of you. A healthy older child has an uncomplicated febrile illness. An infant under two, or any child with a high-risk condition, sits in a different risk stratum where the same virus is far more likely to cause pneumonia, dehydration, encephalopathy or respiratory failure. A fellowship answer that classifies only by virus and ignores the host-stratified risk misses the part that decides whether you treat, admit and escalate. [2] [4]
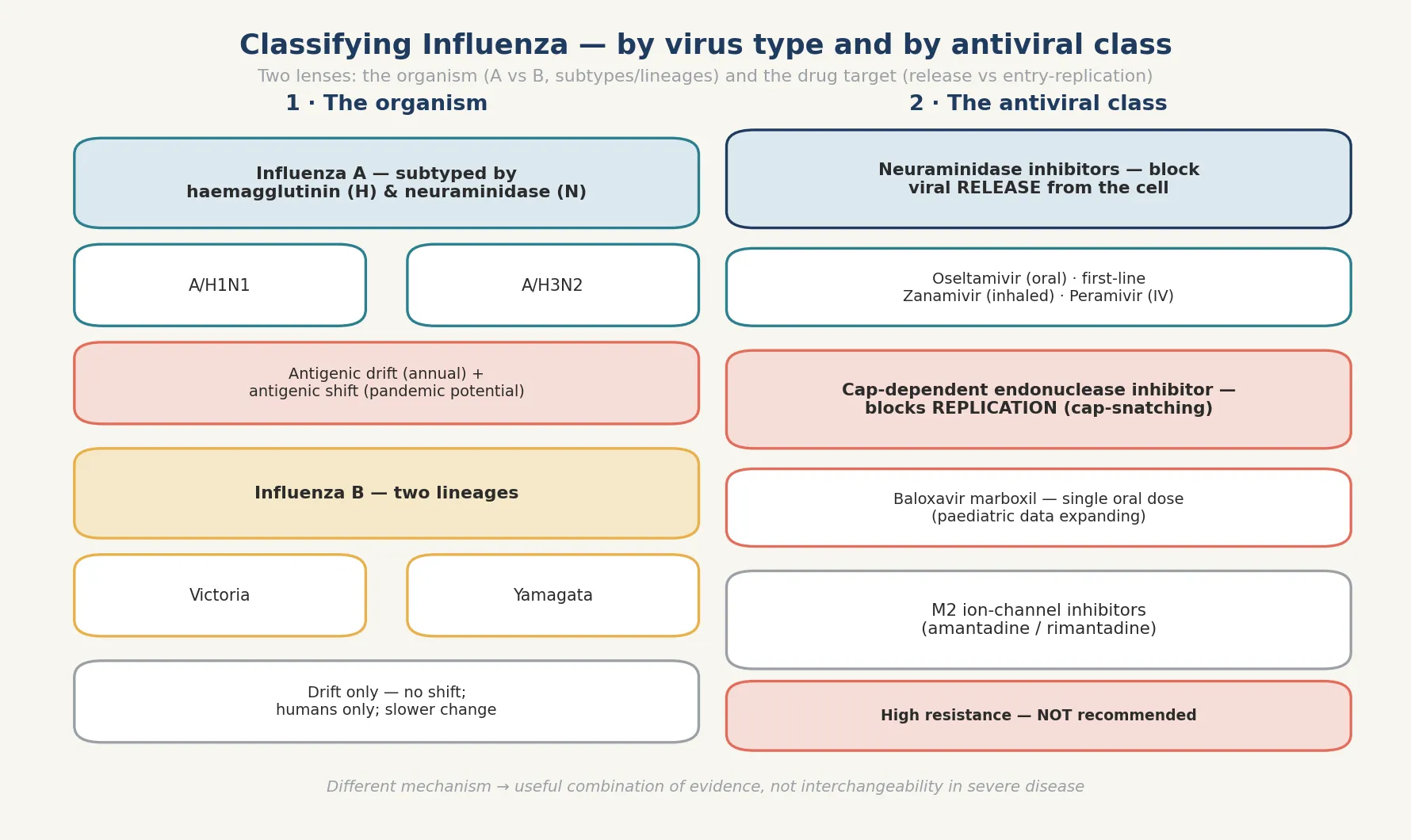
The third distinction, central to antiviral choice, is the drug target. Neuraminidase inhibitors — oseltamivir, zanamivir and peramivir — block the release of new virions from the infected cell. Baloxavir marboxil works one step earlier, blocking the viral cap-dependent endonuclease so the virus cannot hijack host messenger RNA to replicate. The older M2 ion-channel inhibitors, amantadine and rimantadine, are no longer used because high-level resistance is near-universal. Knowing which step each drug interrupts explains both their evidence and their use together. [7] [5]
Epidemiology & Risk Factors
Where does influenza sit, and whom does it hurt? It circulates every winter in temperate climates and year-round in the tropics, and children bear a disproportionate share of the burden — they have the highest attack rates, they shed virus for longer, and they are the engine of community transmission. Hospitalisation rates are highest in the very young and the very old; among children, those under two years carry the greatest risk. [3] [2]
The children who come to harm are a recognisable group. Infants under six months, who are too young to be fully vaccinated, depend on maternal antibody and the immunity of the people around them. Children with chronic lung disease (including asthma), congenital or acquired cardiac disease, neurologic and neurodevelopmental conditions, immunocompromise, metabolic and renal disease, and those on long-term aspirin therapy, all carry markedly higher risks of severe influenza. The 2009 H1N1 hospitalised-patient series from the United States showed how asthma, neurologic disease and immunocompromise dominated the risk profile of children admitted with pandemic influenza. [2] [4]
Mortality is concentrated in these high-risk children, but it is not confined to them — a striking feature of the seminal surveillance of influenza-associated deaths in children was how many of the children who died had been previously healthy. Secondary bacterial pneumonia, particularly with Staphylococcus aureus (including methicillin-resistant strains), Streptococcus pneumoniae and Haemophilus influenzae, drives much of the fatal deterioration. The Randolph et al. intensive-care series during the 2009 pandemic showed that a substantial proportion of critically ill children had no documented underlying condition, reinforcing that any child can become severely unwell. [3] [4]
Pathophysiology
Why does an acute respiratory virus produce pneumonia, encephalopathy and death? The answer lies in how influenza enters, replicates and damages the airway, and in the host factors that turn a nuisance into a threat. The virus is inhaled in droplets and its haemagglutinin binds sialic-acid receptors on ciliated respiratory epithelium, triggering endocytosis. Once inside, the viral polymerase uses a cap-snatching mechanism — stealing the capped ends of host messenger RNA — to transcribe its own genome and build new virions. [7] [5]
New virions then bud from the cell surface, and the viral neuraminidase cleaves the sialic-acid receptors so the virus can detach and spread to neighbouring cells. This release step is the target of the neuraminidase inhibitors, while baloxavir acts one step earlier on the cap-snatching endonuclease that enables replication. Epithelial cell death, inflammation and impaired mucociliary clearance follow, and the denuded airway becomes a fertile ground for secondary bacterial invasion. [7] [5]
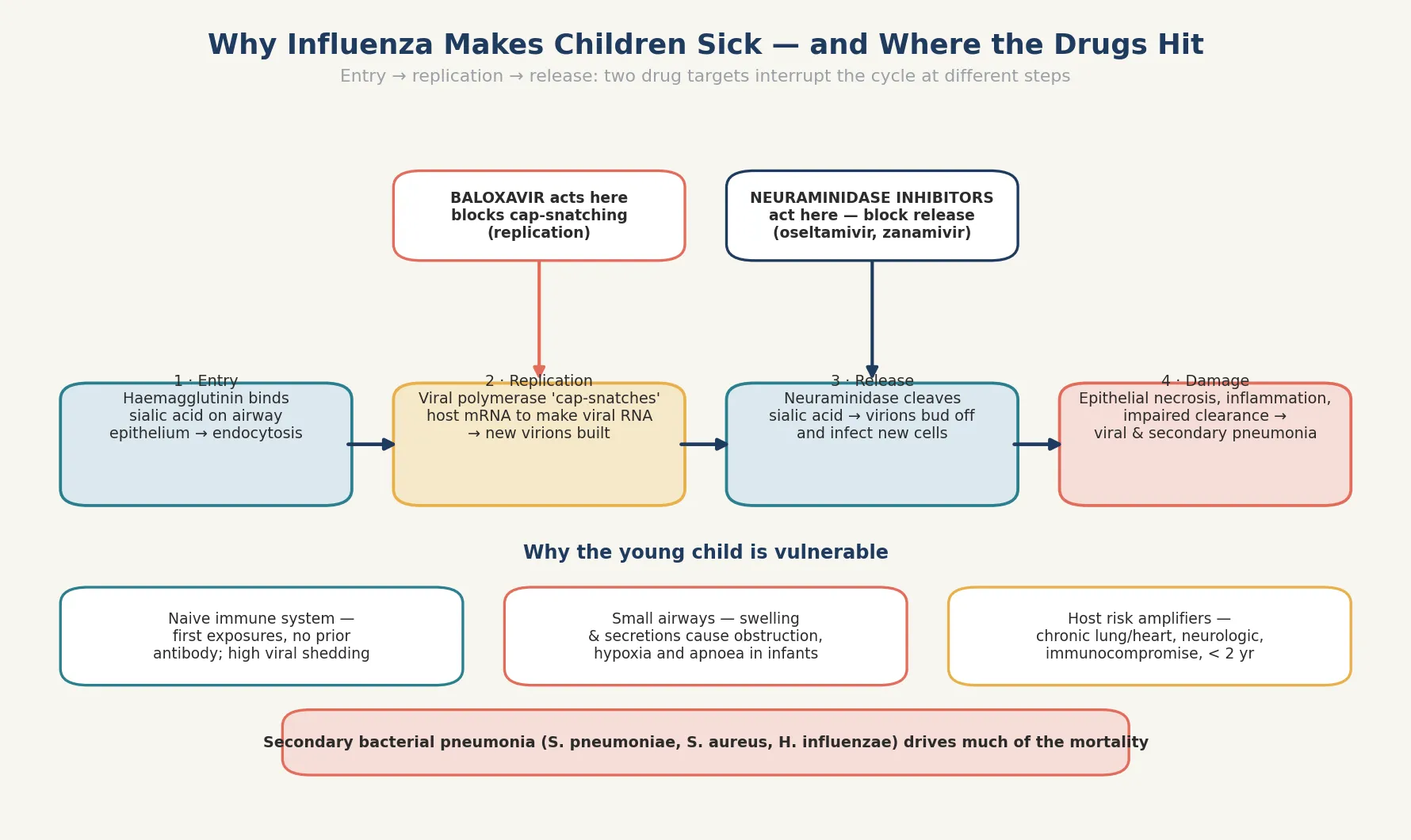
The young child is vulnerable for biological reasons. An infant's immune system is naive to influenza, so a first infection meets little pre-existing antibody and viral shedding is high. Small airways turn the same epithelial swelling and secretions that produce a cough in an adult into obstruction, hypoxia and apnoea in a baby. Host risk amplifiers — chronic lung or cardiac disease, neurologic impairment that weakens airway protection and secretion clearance, and immunocompromise — convert an ordinary febrile illness into respiratory failure, secondary pneumonia or encephalopathy. [4] [2]
Clinical Presentation
The classic picture in an older child is the abrupt onset that opens this topic. Within hours of appearing well, the child develops high fever, a dry cough, coryza, sore throat, headache, myalgia and marked fatigue. Gastrointestinal symptoms — vomiting, abdominal pain and diarrhoea — are far more common in children than in adults and may dominate the presentation. The contrast with the gradual, predominantly coryzal common cold is what makes the history so useful. [2] [3]
The infant presentation is the one that catches clinicians out. A baby under two may have no localising respiratory story at all: fever, poor feeding, irritability, lethargy, apnoea or a sepsis-like picture can be the whole illness. Influenza sits firmly in the differential of the febrile, unwell infant and of apparent life-threatening events, and a low threshold to test and treat is what prevents the catastrophic miss. [2] [4]
The complications are part of the presentation because they often bring the child to hospital. Viral pneumonia develops directly from influenza infection. Secondary bacterial pneumonia classically appears as deterioration after two to three days of initial improvement, with new fever, breathlessness and sepsis. Otitis media and asthma exacerbations are common. Influenza-associated encephalopathy — altered consciousness, seizures or behavioural change during the acute illness — is rare but rapidly progressive and carries a high mortality. Myocarditis presents as tachycardia out of proportion to fever, poor perfusion and hepatomegaly, and severe myositis may render a child unable to walk. [3] [4]
Differential Diagnosis
For the febrile child with cough in winter, the differential is broad. The common cold and other viral upper-respiratory infections begin gradually and run a milder, predominantly coryzal course. Respiratory syncytial virus bronchiolitis presents with wheeze, crackles and feeding difficulty, typically in younger infants. Mycoplasma pneumonia produces a more protracted, often atypical pneumonia in school-age children. Group A streptococcal pharyngitis causes fever and sore throat without the marked systemic myalgia and cough of influenza. [2] [3]
For the unwell infant with fever and respiratory signs, the dangerous differential takes over: sepsis and bacteraemia, urinary tract infection, bronchiolitis, pertussis, and pneumonia all overlap. The decisive point is that the unwell infant needs a sepsis-style workup and empiric treatment regardless of the eventual viral diagnosis, and that adding influenza PCR and early antivirals in season is part of that same protective instinct. [2] [4]
For the child who deteriorates after initial improvement, the differential is secondary bacterial pneumonia, sepsis from another focus, an influenza complication such as myocarditis or encephalopathy, and an alternative diagnosis such as aspiration or a missed foreign body. A new fever with worsening breathlessness after a few days of apparent recovery is secondary bacterial pneumonia until proven otherwise, and it warrants antibiotics that cover S. aureus, S. pneumoniae and H. influenzae. [3] [4]
Clinical & Bedside Assessment
Begin with a focused history built around the onset and the host. Ask about the tempo — the suddenness of the fever is itself a clue — and about cough, coryza, sore throat, myalgia, headache and gastrointestinal symptoms. Ask about feeding, urine output and alertness in the infant, and about any household or school contacts with influenza-like illness. Then establish the risk profile: age under two, chronic lung or cardiac disease, neurologic or neurodevelopmental conditions, immunocompromise, long-term aspirin, pregnancy in an adolescent, and vaccination status. [2] [3]
Examine for the red flags that change disposition. Assess work of breathing, oxygen saturation, recessions, grunting and the quality of air entry. Look for dehydration from poor feeding and fever, for the altered consciousness or seizures of encephalopathy, and for the tachycardia, poor perfusion and hepatomegaly of myocarditis. A child who cannot walk because of myositis, or who passes dark urine suggesting rhabdomyolysis, needs escalation. Re-assess the child who seemed stable, because the secondary deterioration of bacterial pneumonia is the classic late trap. [4] [3]
Document the public-health essentials that drive the response: symptom onset (for the 48-hour treatment window and for exclusion), school or childcare attendance, and the household contacts who may need prophylaxis. Influenza activity in the community frames the pre-test probability, so knowing whether the region is in epidemic changes how aggressively you test and treat. A careful contact and onset history at the first encounter prevents the late, disorganised public-health scramble. [2] [3]
Investigations
PCR is the confirmatory test that matters. A nasopharyngeal aspirate or flocked nasopharyngeal swab sent for influenza PCR (often as part of a respiratory-virus panel) is sensitive and specific, and it distinguishes influenza A from B and from the other winter viruses in the differential. PCR results guide isolation, antiviral decisions and the public-health response. The key principle is that a sick child should never wait for a PCR result before starting antivirals — a positive test later only confirms what the severity demanded up front. [2] [3]
Rapid antigen tests and point-of-care immunoassays are convenient but less sensitive than PCR, particularly outside peak viral shedding. A negative rapid test in a sick child does not exclude influenza, and the result should not be used to withhold antivirals or to abandon isolation when the clinical picture is convincing. Molecular point-of-care tests, where available, combine the speed of a rapid test with sensitivity close to laboratory PCR and are changing bedside decision-making. [2] [3]
In Australia and Aotearoa New Zealand, influenza is a nationally notifiable disease, and seasonal surveillance is coordinated through national and jurisdictional programmes. PCR on a nasopharyngeal swab or aspirate is the standard diagnostic test in hospital and for outbreak investigation; the Australian Immunisation Handbook (ATAGI) and the New Zealand immunisation schedule set the annual vaccine programme, the funded high-risk groups, and the public-health response including exclusion and prophylaxis. [2]
Supportive tests round out the workup as the picture demands. A full blood count may show a lymphopenia early in the illness but is non-specific. A chest X-ray is indicated when pneumonia is suspected — viral pneumonia shows bilateral infiltrates, while a lobar or pleural effusion pattern points toward secondary bacterial infection. Blood cultures, inflammatory markers and, in the encephalopathic child, neuroimaging and cerebrospinal-fluid analysis help to characterise the complication and to direct antibiotics. The unwell child needs continuous monitoring of oxygenation, work of breathing and conscious state. [4] [3]
Management — Resuscitation
Resuscitation is about the child who is deteriorating. The red flags are respiratory distress with hypoxia, dehydration, altered consciousness, the cardiovascular instability of myocarditis, and the secondary deterioration of bacterial pneumonia. Any child with these features needs admission, oxygen, fluid resuscitation if shock is present, and continuous monitoring. The threshold to admit an infant under two with influenza in winter is deliberately low. [4] [2]
Start antiviral treatment empirically in the sick child, regardless of the duration of symptoms. Oseltamivir, a five-day oral course dose-adjusted for weight and age, is first-line; in neonates and young infants, age-specific dosing established through pharmacokinetic studies supports its safe use even under two years of age. The principle is that severity, not the clock, drives treatment in the hospitalised child — waiting for confirmation or for the 48-hour window to close costs the sickest children the most. [1] [8]
Manage the complications actively. Viral pneumonia needs escalating respiratory support, up to and including high-flow nasal cannula, non-invasive ventilation or mechanical ventilation in the intensive-care unit. Suspected secondary bacterial pneumonia needs empirical antibiotics that cover S. aureus (including methicillin-resistant strains), S. pneumoniae and H. influenzae. Influenza-associated encephalopathy requires airway protection, seizure control and neuroprotective supportive care; myocarditis needs fluid restriction, inotropes and a low threshold for intensive-care involvement. [3] [4]
Maintain hydration and nutrition deliberately, because fever, tachypnoea and poor feeding deplete the sick child. Use oral repletion where tolerated, nasogastric feeds for the child who tires with feeding, and intravenous fluids for the dehydrated or shocked child. Place the child under droplet precautions throughout the admission, and complete the public-health essentials of notification, isolation and contact identification as part of the same resuscitation bundle. [4] [2]
Management — Definitive & Stepwise
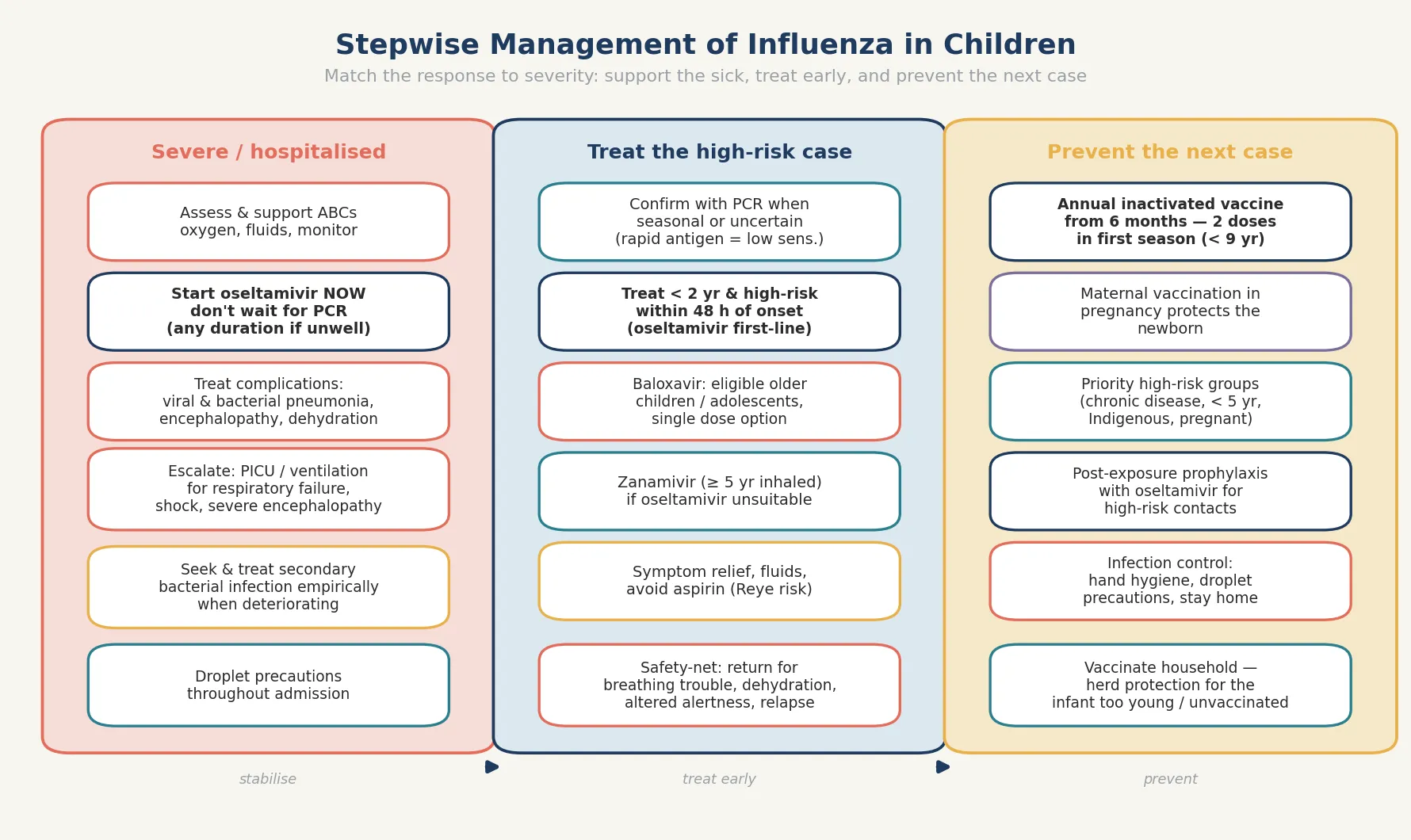
Definitive management is a stepwise pathway matched to severity and risk, with the individual antiviral at one end and the prevention programme at the other. The hospitalised or severe case gets early empiric oseltamivir and supportive care; the high-risk outpatient gets treatment within 48 hours; and the well, low-risk child gets symptomatic care, safety-netting and prevention through vaccination and hygiene. [2] [5]
The stepwise influenza pathway
Severe or hospitalised child: assess and support airway, breathing and circulation; give oxygen and fluids as needed; start oseltamivir empirically — do not wait for PCR.
High-risk or under-two outpatient: confirm with PCR when it changes management and start oseltamivir within 48 hours of onset; baloxavir is an option in eligible older children and adolescents.
Dose oseltamivir by weight and age for a five-day course; use age-specific dosing in neonates and young infants; choose zanamivir (inhaled, age-appropriate) or peramivir (intravenous) when oseltamivir is unsuitable.
Treat complications — viral pneumonia with respiratory support, secondary bacterial pneumonia with empirical antibiotics covering S. aureus and pneumococcus, encephalopathy and myocarditis with targeted supportive care.
Place under droplet precautions, notify where required, identify household and close contacts, and offer post-exposure prophylaxis to high-risk contacts.
Underpin everything with annual vaccination from six months (two doses in the first season), maternal vaccination in pregnancy, and household vaccination to protect the infant who is too young to be fully covered.
Oseltamivir is the first-line antiviral across age groups, given as a five-day oral course. The landmark trial in children showed that oseltamivir shortened the duration of illness and reduced the incidence of acute otitis media when given early, and a randomised trial in children aged one to three years found that early treatment shortened illness and reduced otitis media. Dose by weight and age; pharmacokinetic work in children under two years established safe, effective dosing for infants and neonates, which is why oseltamivir can be used even in the very young. [1] [6]
Baloxavir marboxil offers a different mechanism and the convenience of a single oral dose. The pivotal trial in adults and adolescents showed that baloxavir reduced viral shedding and shortened symptom duration, and a recent paediatric comparison from Japan reported favourable clinical and virologic outcomes of baloxavir compared with oseltamivir in children with influenza. Baloxavir is an option in eligible older children and adolescents, but oseltamivir remains the established first choice in severe disease and in the youngest infants, where the evidence base is deepest. [7] [9]
The decision to treat an uncomplicated child depends on risk and timing. Treat within 48 hours of onset for children under two years and for those with any high-risk condition, because the benefit of antivirals is greatest early. Treating an otherwise healthy older child within 48 hours can shorten illness and reduce household transmission, and is a reasonable shared decision when the family is keen. Outside that window, reserve antivirals for severe or complicated disease. [5] [6]
Specific Subtypes & Scenarios
A hospitalised child with influenza pneumonia. Admit, give oxygen and supportive respiratory care, start oseltamivir empirically and dose by weight, and monitor for escalation to high-flow nasal cannula or ventilation. Look continuously for the secondary bacterial pneumonia that signals deterioration, and add empirical antibiotics the moment a new fever, sepsis or a lobar infiltrate appears. [4] [3]
An infant under six months with influenza. Too young to be fully vaccinated, the infant depends on maternal antibody and household immunity. Admit the unwell infant, treat with oseltamivir using age-specific neonatal and infant dosing, support feeding and hydration, and monitor for apnoea. The household vaccination status and any opportunity for catch-up vaccination belong in the discharge plan. [8] [2]
A child with asthma or chronic lung disease. Influenza commonly triggers asthma exacerbations and can precipitate respiratory failure in the child with limited reserve. Treat early with oseltamivir, intensify the asthma management with bronchodilators and steroids, and have a low threshold for admission and respiratory support. [2] [4]
A child with neurologic or neurodevelopmental disease. Impaired airway protection, weak secretion clearance and aspiration risk make these children especially vulnerable to severe influenza and secondary pneumonia. Treat early, support the airway and secretions, and watch closely for encephalopathy superimposed on their baseline. [2] [3]
An immunocompromised child. Viral shedding is prolonged, resistance can emerge, and disease is more severe. Treat early, consider a longer antiviral course, monitor for oseltamivir resistance, and use intravenous zanamivir or peramivir when resistance or absorption is a concern. Prevention through household vaccination is central, because these children depend on the immunity of the people around them. [8] [2]
A pregnant adolescent. Pregnancy increases the risk of severe influenza, and influenza in pregnancy harms both mother and fetus. Treat early with oseltamivir, which is safe in pregnancy, and ensure the household and the mother are vaccinated. Maternal influenza vaccination in any future pregnancy will pass antibody to the next infant through the first months of life. [10] [11]
Complications & Pitfalls
Viral pneumonia is the direct severe complication of influenza, and secondary bacterial pneumonia is the classic killer. The pattern to fear is the child who improves for a day or two and then spikes a new fever with worsening breathlessness and sepsis — this is secondary bacterial pneumonia, most often S. aureus (including methicillin-resistant strains), S. pneumoniae or H. influenzae, and it needs empirical antibiotics immediately. Recognising this biphasic course and treating it early is one of the few things that genuinely changes the outcome of severe influenza. [3] [4]
Influenza-associated deaths in children — US 2003–2004
Population: US national surveillance of influenza-associated deaths among children during the 2003–2004 influenza season.
Key finding
A substantial proportion of the children who died had been previously healthy, and many deaths involved bacterial co-infection, particularly Staphylococcus aureus. The case-fatality data underscored that influenza is not always a benign illness in children.
Practice change
Take influenza seriously even in previously healthy children, watch for the biphasic deterioration of secondary bacterial pneumonia, and vaccinate broadly — mortality is not confined to those with obvious risk factors.
The central treatment pitfall is withholding antivirals while waiting for confirmation, or because more than 48 hours have passed. In the hospitalised, severe or high-risk child, severity governs the decision to treat — the clock matters most for the uncomplicated outpatient, not for the child who is already sick. A clinician who defers oseltamivir until the PCR returns loses the window in which antivirals help most. [1] [6]
A second pitfall is missing influenza-associated encephalopathy. Altered consciousness, seizures or behavioural change during influenza is not simply a febrile delirium — it may be a rapidly progressive encephalopathy with a high mortality, and it demands urgent assessment, neuroimaging and supportive care. Attributing a drowsy febrile child with influenza to "just a virus" closes the door on a diagnosis that can kill within hours. [3] [4]
A third pitfall is giving aspirin to a febrile child with influenza. Aspirin is avoided in children with viral febrile illness because of the association with Reye syndrome, and the antipyretic of choice is paracetamol or ibuprofen. A fourth pitfall is over-reliance on a negative rapid antigen test in a sick child — its lower sensitivity means a negative result cannot exclude influenza or justify withholding antivirals. [2] [3]
The final pitfall is forgetting prevention. Failing to vaccinate the child and the household, to isolate the hospitalised case, or to offer prophylaxis to a high-risk contact allows the next avoidable case — and the next avoidable death — to occur. The clinical encounter does not end when the child improves; it ends when the contacts are protected and the family is vaccinated. [10] [11]
Prognosis & Disposition
Most healthy older children recover fully within a week, though cough and fatigue may linger for weeks. For these patients the disposition is home management with symptomatic care, clear safety-netting for the warning signs, and reinforcement of vaccination. The morbidity in this group is driven less by danger than by disruption to sleep, school and family life. [2] [3]
The severe outcomes are concentrated in infants under two and in children with high-risk conditions, and the mortality is driven by viral pneumonia, secondary bacterial pneumonia, encephalopathy and myocarditis. This is the single most important prognostic fact in paediatric influenza, and it is why every prevention strategy — maternal vaccination, the annual schedule, household vaccination and early treatment of the sick child — ultimately aims to protect these groups. [3] [4]
Disposition follows severity. Admit to the ward the dehydrated child, the infant with poor feeding or moderate respiratory distress, and any high-risk child who needs observation; admit to the intensive-care unit the child with respiratory failure, shock, encephalopathy or myocarditis. Manage at home the stable, low-risk child with influenza whose feeding, hydration and oxygenation are preserved, provided the family understands the safety-net. [4] [2]
At discharge, complete the antiviral course, reinforce isolation until the child is afebrile and improving, give a clear safety-net for return — worsening breathing, dehydration, altered alertness, a new fever after improvement — and arrange vaccination for the child and the household. The discharge encounter is also a prevention opportunity, and a family vaccinated at this point is a family protected for the next season. [10] [11]
Special Populations
Infants under six months are too young to be fully vaccinated and depend on maternal antibody transferred in pregnancy and on the immunity of the people around them. Their atypical, sepsis-like presentation demands a low threshold to test, treat and admit, and maternal vaccination in pregnancy is the single most effective current protection for this age group. [10] [11]
Pregnant adolescents and women should receive influenza vaccination in pregnancy, because the pooled analysis of three randomised trials confirmed efficacy, protection of the infant and a favourable safety profile, and because maternal influenza immunisation reduces severe pneumonia in young infants. Vaccinating in pregnancy protects two people at once — the mother, who is herself at higher risk of severe influenza, and the newborn, through transplacentally transferred antibody. [10] [11]
Children with chronic medical conditions — chronic lung (including asthma), cardiac, neurologic or neurodevelopmental, immunocompromise, metabolic, renal, and those on long-term aspirin — carry the highest risk of severe influenza. Treat them early, watch them closely for complications, and prioritise them for annual vaccination and for post-exposure prophylaxis after a household contact. [2] [4]
Immunocompromised children may shed virus for longer, develop resistance to antivirals, and suffer more severe disease. Use early and sometimes extended antiviral treatment, monitor for resistance, and have intravenous options available. Household vaccination matters most for these children, who depend on the immunity of the people around them. [8] [2]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children, and refugee, asylum-seeking and migrant families bear a disproportionate burden of severe influenza and may face barriers to timely vaccination and care. Ensure culturally safe, equitable access to immunisation and treatment, use trained interpreters rather than family members, and treat actively when disease is suspected. Disadvantage should never be the reason an influenza diagnosis is delayed or a child is left unvaccinated. [2] [3]
Rural and remote children need timely access to diagnosis, antiviral treatment and escalation through outreach and telehealth, because distance can delay the care that a sick infant cannot afford to wait for. The plan for a remote family accounts for what is available locally, and retrieval is mobilised early when a child deteriorates. [4] [2]
Evidence, Guidelines & Regional Differences
The evidence for oseltamivir in children is anchored by the original treatment trial and the early-treatment trial in young children. The Whitley et al. trial established that oseltamivir shortened illness and reduced acute otitis media in children, and the Heinonen et al. randomised trial in children aged one to three years showed that early treatment shortened the illness and reduced otitis media. The adult meta-analysis by Dobson et al. confirmed that oseltamivir reduces symptom duration and lower-respiratory complications when started early, supporting the same principle in children. [1] [5]
The pharmacokinetic and dosing evidence for the youngest infants is set out in the Kimberlin et al. study, which established safe, effective oseltamivir dosing for children under two years and described the emergence of resistance. This evidence is what allows oseltamivir to be used with confidence even in neonates, where age-specific dosing matters most. [8] [1]
Baloxavir for uncomplicated influenza — CAPSTONE-1
Population: Adults and adolescents with uncomplicated influenza, randomised to baloxavir marboxil, oseltamivir or placebo within 48 hours of symptom onset.
Key finding
Baloxavir shortened the duration of symptoms and, compared with both oseltamivir and placebo, significantly reduced viral shedding after one day of treatment, reflecting its earlier mechanism of action on viral replication.
Practice change
Baloxavir is a single-dose oral option for eligible older children and adolescents; its faster virologic effect is attractive, but oseltamivir remains the evidence anchor for severe disease and for the youngest infants.
The baloxavir evidence in children is growing. The CAPSTONE-1 trial established baloxavir in adults and adolescents, and a recent paediatric comparison from Japan reported favourable clinical and virologic outcomes of baloxavir compared with oseltamivir in children with influenza. Baloxavir's single-dose convenience and rapid reduction in viral shedding are attractive, though the durability of the evidence and concerns about resistance mean oseltamivir remains first-line in severe disease and in the youngest infants. [7] [9]
The prevention evidence is anchored by the maternal-vaccination trials. The pooled analysis by Omer et al. of three randomised trials confirmed the efficacy of influenza vaccination in pregnancy, the duration of protection, the favourable birth outcomes and the protection of the infant; the separate analysis of the same trial network showed that maternal influenza immunisation reduced severe clinical pneumonia in young infants. Together they justify influenza vaccination in every pregnancy. [10] [11]
The regional policy structure is consistent in principle and varies in detail. In ANZ, influenza is nationally notifiable, the Australian Immunisation Handbook (ATAGI) and the New Zealand immunisation schedule fund the annual vaccine for high-risk groups and young children, and public-health units coordinate surveillance and the response to outbreaks and institutional spread. In the UK, the Green Book and UK Health Security Agency guidance direct the programme, with a strong emphasis on intranasal live-attenuated vaccine for children delivered through schools. In the US, the CDC and the American Academy of Pediatrics recommend universal annual vaccination from six months, two doses in the first season, and early antiviral treatment of hospitalised and high-risk children. In Canada, the Canadian Immunization Guide and provincial programmes deliver the equivalent strategy. In every region the principle is the same: vaccinate annually from six months, vaccinate in pregnancy, treat severe and high-risk children early, and protect the contacts around the vulnerable infant. [2] [3]
The controversies are active: the real-world magnitude of oseltamivir's benefit in uncomplicated children given its modest symptom reduction; the place of baloxavir relative to oseltamivir and the significance of baloxavir-emergent resistant variants; the optimal uptake of the annual childhood vaccine; and the inequities in vaccine access that leave some communities and infants unprotected. The defence against each is the same: high vaccination coverage, early antiviral treatment of the sick and high-risk child, active management of complications, and a public-health layer that does not stop at the bedside. [5] [9]
Exam Pearls
- Influenza is a droplet-spread seasonal virus — influenza A (H1N1, H3N2) and B (Victoria, Yamagata); onset is abrupt, with fever, cough, myalgia and fatigue. [2]
- Children under two and those with chronic lung, cardiac, neurologic or immune disease carry the highest risk; previously healthy children also die. [3] [4]
- In the infant, influenza can look like sepsis — fever, poor feeding, apnoea or lethargy; keep it in the differential of the unwell infant. [2]
- Confirm with PCR; rapid antigen tests have lower sensitivity, so a negative result does not exclude influenza in a sick child. [2]
- Start oseltamivir empirically in the hospitalised, severe or high-risk child — do not wait for PCR or for the 48-hour window. [1] [6]
- Oseltamivir is first-line (five-day oral course, dose by weight and age); zanamivir (inhaled) and peramivir (IV) are alternatives; baloxavir is a single-dose option in eligible older children. [7] [9]
- Treat within 48 hours for children under two and for high-risk conditions; outside that window, treat severe or complicated disease. [5] [6]
- Biphasic deterioration after initial improvement = secondary bacterial pneumonia (S. aureus, S. pneumoniae, H. influenzae) — add empirical antibiotics. [3]
- Watch for influenza-associated encephalopathy and myocarditis; do not dismiss a drowsy or tachycardic febrile child as "just a virus". [4]
- Avoid aspirin (Reye syndrome); use paracetamol or ibuprofen. [3]
- Prevention: annual inactivated vaccine from six months (two doses in the first season under nine years), maternal vaccination in pregnancy, and post-exposure prophylaxis for high-risk contacts. [10] [11]
- M2 inhibitors (amantadine, rimantadine) are not recommended because of near-universal resistance. [5]
References
- [1]Whitley RJ; Hayden FG; Reisinger KS; et al Oral oseltamivir treatment of influenza in children. Pediatr Infect Dis J, 2001.PMID 11224828
- [2]Jain S; Kamimoto L; Bramley AM; et al Hospitalized patients with 2009 H1N1 influenza in the United States, April-June 2009. N Engl J Med, 2009.PMID 19815859
- [3]Bhat N; Wright JG; Broder KR; et al Influenza-associated deaths among children in the United States, 2003-2004. N Engl J Med, 2005.PMID 16354892
- [4]Randolph AG; Vaughn F; Sullivan R; et al Critically ill children during the 2009-2010 influenza pandemic in the United States. Pediatrics, 2011.PMID 22065262
- [5]Dobson J; Whitley RJ; Pocock S; et al Oseltamivir treatment for influenza in adults: a meta-analysis of randomised controlled trials. Lancet, 2015.PMID 25640810
- [6]Heinonen S; Silvennoinen H; Lehtinen P; et al Early oseltamivir treatment of influenza in children 1-3 years of age: a randomized controlled trial. Clin Infect Dis, 2010.PMID 20815736
- [7]Hayden FG; Sugaya N; Hirotsu N; et al Baloxavir Marboxil for Uncomplicated Influenza in Adults and Adolescents. N Engl J Med, 2018.PMID 30184455
- [8]Kimberlin DW; Acosta EP; Prichard MN; et al Oseltamivir pharmacokinetics, dosing, and resistance among children aged <2 years with influenza. J Infect Dis, 2013.PMID 23230059
- [9]Ishiguro N; Morioka I; Nakano T; et al Clinical and Virologic Outcomes of Baloxavir Compared with Oseltamivir in Pediatric Patients with Influenza in Japan. Infect Dis Ther, 2025.PMID 40155497
- [10]Omer SB; Clark DR; Madhi SA; et al Efficacy, duration of protection, birth outcomes, and infant growth associated with influenza vaccination in pregnancy: a pooled analysis of three randomised controlled trials. Lancet Respir Med, 2020.PMID 32526188
- [11]Omer SB; Clark DR; Aqil AR; et al Maternal Influenza Immunization and Prevention of Severe Clinical Pneumonia in Young Infants: Analysis of Randomized Controlled Trials Conducted in Nepal, Mali and South Africa. Pediatr Infect Dis J, 2018.PMID 29443825