Paeds · infectious-diseases
International adoption, immigration and refugee infection screening
Also known as Post-arrival health screen for migrant children · Refugee and asylum-seeker screening · Internationally adopted child screening · Immigrant child infection screen · Newcomer paediatric health assessment
Fellowship topic on the comprehensive infection screen for the three populations of migrant children — internationally adopted, immigrant, and refugee or asylum-seeking — anchored on the must-not-miss five (tuberculosis, HIV, hepatitis B, hepatitis C, parasitic and intestinal disease); the principle that a documented record is never trusted without re-verification in your own laboratory; the Australasian ASID/RHeANA framework and the United States CDC domestic examination guidance; the silent natural history of latent, chronic and vaccine-gap infections that makes screening the only route to early detection; the IGRA-versus-TST debate; the strongyloidiasis and schistosomiasis serology that is too often missed; the catch-up immunisation that follows on serological evidence; and the trauma-informed, interpreter-mediated, equity-grounded framing that turns a checklist into a medical home.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
S.C.R.E.E.N. — the six acts of the post-arrival assessment
Overview & Definition
Picture a four-year-old girl who has just arrived from an orphanage in a resource-limited country to join her adoptive family, sitting in your clinic looking well, with a thin folder of pre-adoption records in a language you do not read. The easy assumption is that she is healthy — and on the surface she is. The fellowship-level skill is to know that this is exactly the child in whom tuberculosis, chronic hepatitis B, HIV, and Strongyloides can sit silently for years, and that the single visit is the best — and sometimes only — chance to find them. The post-arrival infection screen is the structured, comprehensive assessment of a migrant child that targets these silent infections before they declare themselves. [1] [2]
The three populations share a logic but differ in detail. Internationally adopted children carry a higher burden of chronic viral hepatitis, tuberculosis and intestinal parasites than any routinely screened paediatric group, and their pre-adoption records are often sparse, untranslated, or unreliable. Immigrant children are often healthy but may have incomplete or undocumented vaccination and region-specific exposures. Refugee and asylum-seeking children are the most comprehensively screened group, because many high-income resettlement programmes run an overseas pre-departure examination followed by a domestic post-arrival assessment — yet even here the record is re-verified, never assumed. [3] [8]
What makes this a fellowship-level topic is that the dangerous infections are silent at the time of screening. Latent tuberculosis, chronic hepatitis B and C, and HIV produce no symptoms for years; Strongyloides can persist for decades; and a vaccine record can record doses that were never given or never took. The clinician is therefore screening not for illness but for future risk, and the discipline is to act on laboratory evidence rather than on the child's appearance or the paper in the folder. The reward is that almost everything found is treatable today, and the assessment opens a relationship that delivers the medical home. [7] [9]
Classification
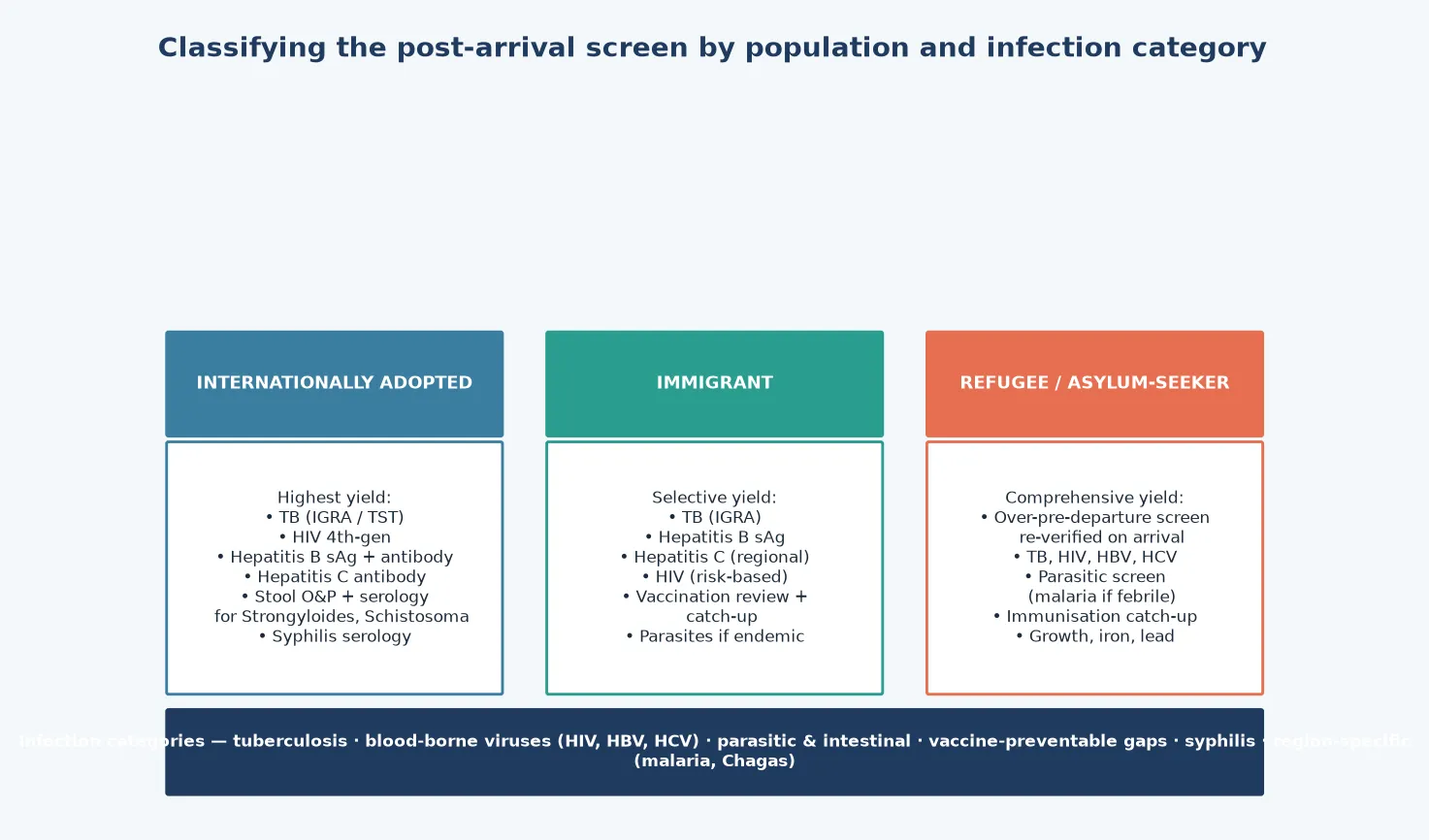
The most useful first classification is by population, because each group carries a recognisable risk profile that shapes the intensity and focus of the screen. The internationally adopted child has the highest pre-test probability of chronic hepatitis B, latent tuberculosis and intestinal parasites, and the lowest reliability of pre-adoption records — the screen is therefore comprehensive and assumes nothing. The immigrant child is often healthy but arrives with variable vaccination and region-specific exposure, so the screen is selective but always includes tuberculosis, hepatitis B and a vaccination review. The refugee or asylum-seeking child typically has both an overseas and a domestic record, and the post-arrival screen re-verifies the overseas findings, adds the conditions the overseas examination does not cover, and integrates mental-health and developmental assessment. [3] [8]
The second axis is the infection category, which organises the core panel. The must-not-miss five are tuberculosis (latent, by IGRA or tuberculin skin test), the blood-borne viruses (HIV, hepatitis B surface antigen, hepatitis C antibody), and the parasitic and intestinal diseases (Strongyloides and Schistosoma serology, stool ova, cysts and parasites). Around these sit the vaccine-preventable gaps (measles, rubella, diphtheria, tetanus, pertussis, polio, Haemophilus, pneumococcus, hepatitis B, varicella), syphilis serology, and the region-specific additions — a malaria film for the febrile recently arrived child, Chagas serology for the child from Latin America, and a blood-lead level for resettled refugee children. [4] [10]
The third axis is pre-arrival pathway, which determines what the clinician inherits. Some refugees arrive with a documented overseas pre-departure examination under a national resettlement programme; some arrive having had no pre-departure screen at all; internationally adopted children arrive with variable orphanage records. The Australasian ASID/RHeANA framework and the United States CDC domestic examination guidance both treat the overseas record as a starting point and require a full post-arrival re-assessment, because the overseas screen is necessarily limited and the child's circumstances may have changed. [9] [8]
The comprehensive post-arrival pathway
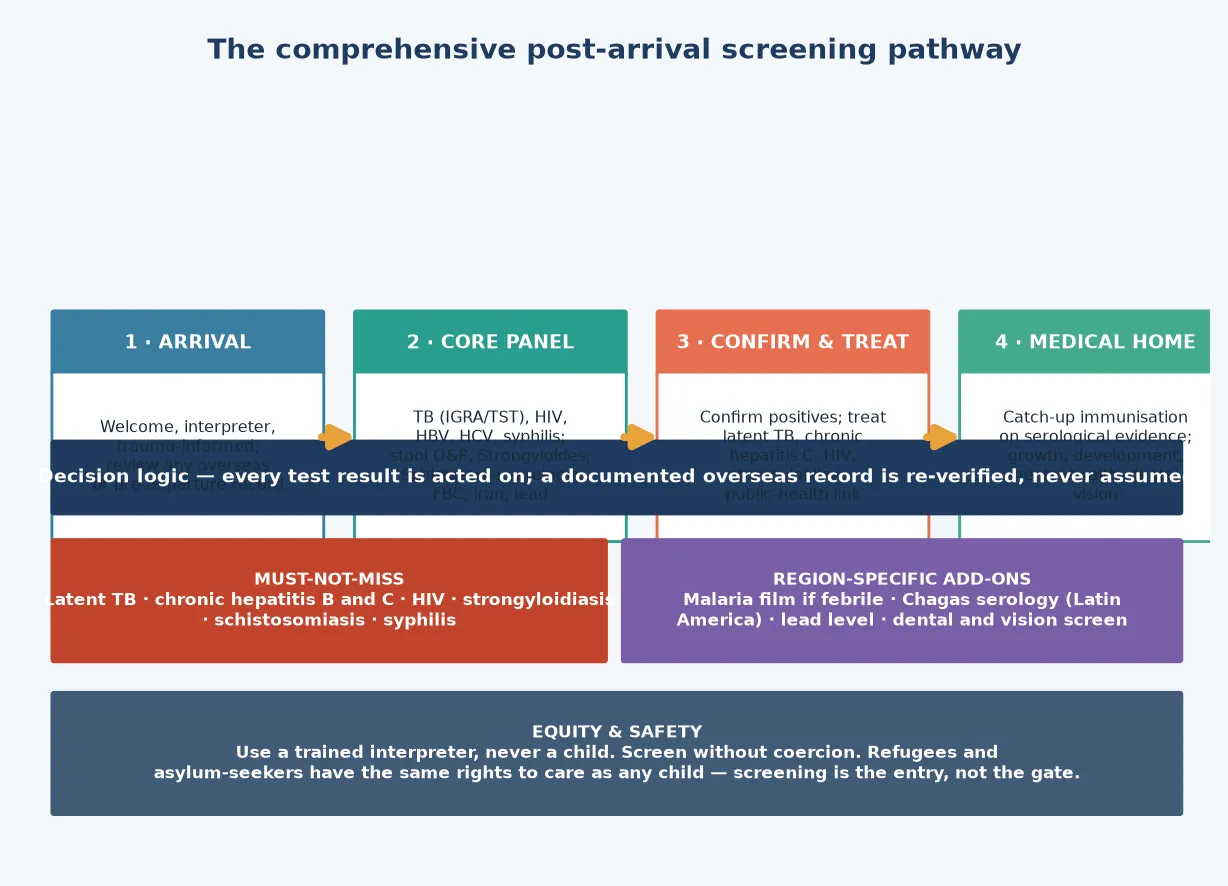
Arrival: welcome the family, use a trained interpreter, take a trauma-informed history, and review any overseas or pre-departure record as a hypothesis — not as fact.
Core panel: tuberculosis (IGRA or tuberculin skin test), HIV, hepatitis B surface antigen and antibody, hepatitis C antibody, syphilis; stool ova, cysts and parasites with Strongyloides and Schistosoma serology; full blood count, iron studies and a blood-lead level.
Confirm and treat: repeat any positive in your own laboratory, treat latent TB, chronic hepatitis C, HIV and strongyloidiasis, and link the family to public-health and infectious-diseases services.
Medical home: deliver catch-up immunisation on serological evidence, assess growth and development, support mental health, and arrange dental, vision and hearing care with an explicit follow-up plan.
Epidemiology & Risk Factors
The yield of post-arrival screening is high, and the evidence base is built on the systematic screening of large migrant cohorts. The foundational Hostetter study of internationally adopted children established that a structured medical evaluation detects infection in a substantial proportion of children who appear well on arrival, and every subsequent cohort has confirmed that the highest-yield conditions are tuberculosis, chronic hepatitis B, intestinal parasites and, in some regions, HIV. The probability of a specific finding tracks tightly with the country of origin, the type of institution or community the child came from, and the completeness of prior healthcare. [1] [2]
Tuberculosis is the single most common finding across all three populations. Latent tuberculosis infection is detected in roughly ten to twenty per cent of refugee and internationally adopted children in most large series, and the United States domestic-evaluation data on immigrant and refugee children showed that latent TB diagnosed overseas is frequently confirmed on post-arrival testing — which is why the post-arrival IGRA or tuberculin skin test is non-negotiable. Chronic hepatitis B surface antigen positivity is highest in internationally adopted children and in migrants from sub-Saharan Africa, East Asia and the Pacific, and chronic hepatitis C and HIV prevalence are lower but consequential when found. [11] [6]
Parasitic infection is the category most often under-screened and the one with the clearest single-dose treatment. Strongyloides stercoralis and Schistosoma species are endemic across much of the tropics and persist silently for decades; the United Kingdom and Australasian screening programmes both now recommend serology rather than stool alone, because stool microscopy has a low sensitivity for these chronic carriers. Refugee children also carry a higher burden of nutritional deficiency — iron-deficiency anaemia, vitamin B12 deficiency, and elevated blood-lead levels — and these are screened in parallel with the infection panel because they compound the effect of chronic disease on growth and development. [10] [7]
Risk is amplified by the type and duration of pre-arrival exposure. Children who lived in institutional care carry a higher burden of hepatitis B, scabies and intestinal parasites than those raised in families; children from rural or conflict-affected regions carry higher tuberculosis and parasite exposure; and children whose journey included periods in detention or unscreened transit carry additional risk of communicable disease and mental-health harm. The visiting-friends-and-relatives family and the unaccompanied minor are the groups most often missed by routine services, and a low threshold for a comprehensive screen is the structural defence. [8] [9]
Pathophysiology
Three converging mechanisms explain why migrant children carry undiagnosed infection, and each maps to a screening test and a treatable condition. Understanding the mechanism is what converts the screen from a checklist into a clinical act — you order the test because you can picture the disease it will find. [7]
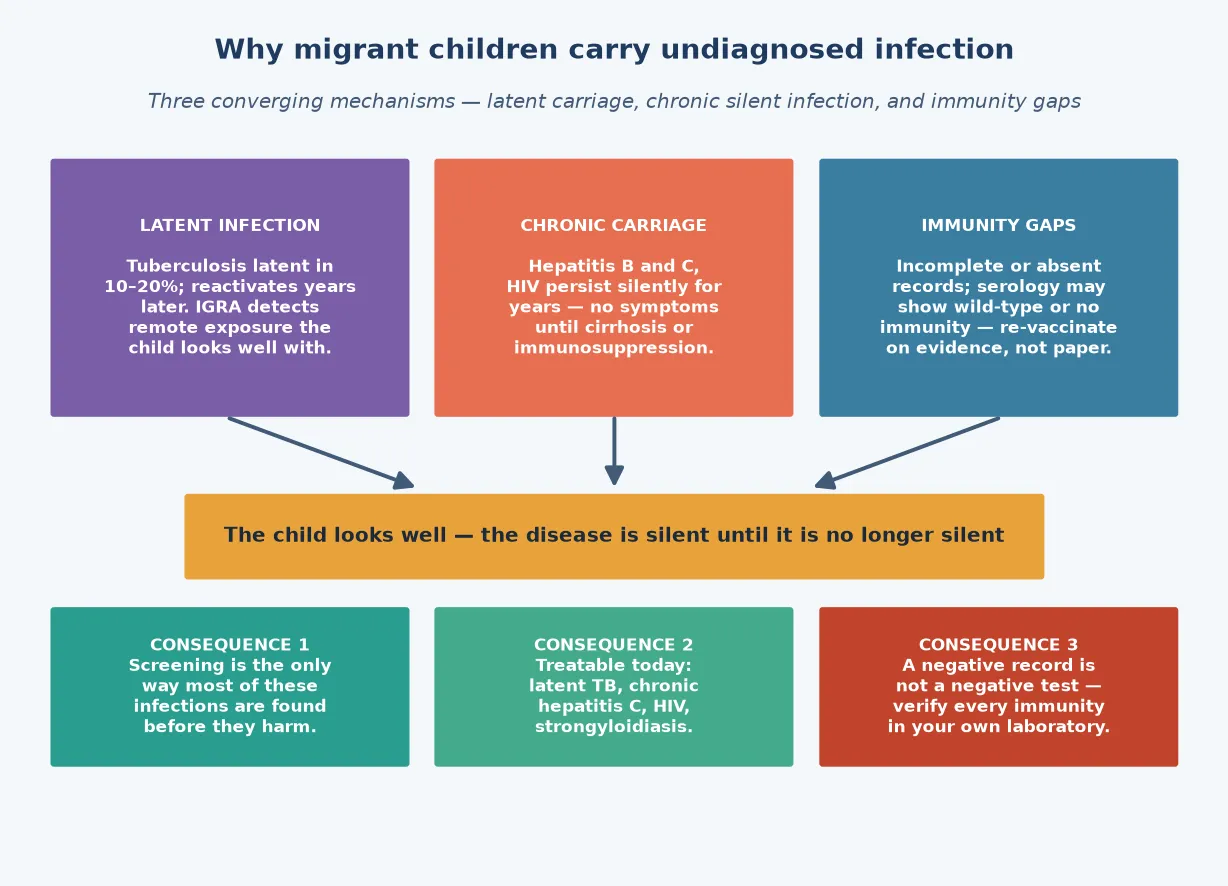
The first mechanism is latent infection, exemplified by tuberculosis. After primary infection the organism is contained by the cell-mediated immune response but not eradicated, and it can reactivate years to decades later — most often during adolescence, immunosuppression, or the physiological stress of resettlement. The interferon-gamma release assay (IGRA) and the tuberculin skin test detect this remote exposure by measuring the cell-mediated immune response, which is why a child with latent TB has a normal chest radiograph and looks entirely well. The point of screening is to find the latent case before it reactivates, because treating latent TB prevents the future infectious and destructive disease. [11] [9]
The second mechanism is chronic carriage, the silent persistence of a blood-borne virus or a tissue-dwelling parasite. Hepatitis B and C and HIV produce no symptoms for years; the liver inflammation of chronic hepatitis slowly progresses to cirrhosis and hepatocellular carcinoma, and the immunodeficiency of untreated HIV advances over a decade. Strongyloides stercoralis completes an auto-infection cycle that allows the worm to persist for fifty years or more, and the danger is hyperinfection — a catastrophic, often fatal dissemination — triggered by later corticosteroids, immunosuppression, or human T-lymphotropic virus co-infection. The point of screening is that all of these are treatable today: direct-acting antivirals cure chronic hepatitis C, antiretrovirals transform HIV into a chronic controlled condition, and ivermectin cures strongyloidiasis in a single course. [10] [8]
The third mechanism is the immunity gap, the difference between what a vaccine record says and what the child's immune system actually shows. Records may be incomplete, fabricated, lost in transit, or record doses given at the wrong interval or with a cold-chain break; some children have natural (wild-type) immunity and some have none. The serological approach — testing for antibodies to vaccine-preventable diseases and re-vaccinating those without immunity — closes this gap without over-vaccinating those already immune, and it is the standard for internationally adopted children whose records are least reliable. [4] [2]
Clinical Presentation
The clinical presentation that prompts screening is, in the great majority of cases, no presentation at all — the child looks well and has arrived for a routine post-arrival assessment. This is the central feature of the topic and the reason the screen is laboratory-led rather than symptom-led. The clinician does not wait for the child to declare disease; the clinician looks for the silent infection that the child is carrying asymptomatically. [3] [7]
The history that matters is the pre-arrival history: country and region of origin, type of care before arrival (institution, family, foster care, detention), the route and duration of any migration journey, any overseas or pre-departure medical examination and what it found, the vaccination record and its source, and the family's understanding of the child's health. For the internationally adopted child the adoption history — age at placement, growth and developmental milestones, and any known exposures — frames the screen; for the refugee child the exposure history, including time in camps or detention, frames the additional risks. [2] [8]
The examination is comprehensive rather than targeted, because the screen is the child's entry to care. Measure growth and plot it on appropriate references, examine the skin for scabies, lice and the stigmata of chronic liver disease, examine the abdomen for hepatosplenomegaly, listen to the heart for evidence of rheumatic or Chagas-related disease in the child from Latin America, and assess development and mental health. The child who is actually unwell — febrile, failing to thrive, or with organ-specific signs — is moved out of the screening pathway and into an acute assessment, because a febrile recently arrived child from a malaria-endemic region has malaria until a competent blood film proves otherwise. [9] [7]
Differential Diagnosis
The differential here is the differential of the abnormal screening result, not of a presenting symptom, and the skill is in interpreting each positive test correctly and confirming it before acting. A positive tuberculin skin test or IGRA raises latent tuberculosis infection, which must be distinguished from active tuberculosis by chest radiograph, symptom screen and — where indicated — sputum or gastric-aspirate sampling in the young child who cannot expectorate. A child with latent TB and a normal chest radiograph is treated for latent infection; a child with radiographic or symptomatic disease is treated for active TB and notified. [11] [9]
A positive hepatitis B surface antigen must be confirmed and the child assessed for chronicity (surface antigen positive beyond six months), viral markers (e-antigen and antibody, viral load), liver function and co-infection with hepatitis D, hepatitis C and HIV. A positive hepatitis C antibody is confirmed by a nucleic-acid test for hepatitis C RNA, because the antibody reflects exposure and only a viraemic child has chronic infection amenable to cure with direct-acting antivirals. A reactive HIV screen is confirmed with the age-appropriate algorithm, because maternal antibody persists in infants under eighteen months and the diagnostic test in that age group is HIV DNA or RNA PCR rather than serology. [8] [5]
A positive Strongyloides or Schistosoma serology is treated presumptively, because the serology reflects infection and chronic carriage carries the risk of future hyperinfection or chronic morbidity; stool microscopy is an adjunct for the load and for other parasites, not the gatekeeper for treatment. A low haemoglobin or ferritin raises iron-deficiency anaemia (common) and, in the right context, haemoglobinopathies such as thalassaemia or sickle-cell trait, which are common in migrants from the Mediterranean, Middle East, South Asia and sub-Saharan Africa. An elevated blood lead raises environmental lead exposure, which is over-represented in resettled refugee children and carries lifelong neurodevelopmental consequence. [10] [7]
Clinical & Bedside Assessment
The bedside assessment begins with the relationship, not the panel. Use a trained interpreter — never a child or a family member — because the pre-arrival history and the consent for screening depend on accurate communication, and because using a child to interpret for their family is both unsafe and a betrayal of the child's interest. Take a trauma-informed approach, recognising that many refugee and asylum-seeking families have experienced conflict, loss, detention or persecution, and that the clinical encounter may itself be a source of distress. The Australasian framework and the AAP guidance both frame screening as the entry to comprehensive, respectful care rather than a surveillance exercise. [9] [8]
The history establishes the country and region of origin, the pre-arrival living conditions, the migration route and duration, any overseas examination and its findings, the vaccination record and its provenance, the family's health concerns, and the child's growth, development and schooling. A dietary, dental and environmental history adds the nutritional and lead-exposure context, and a mental-health screen — using a validated tool in the family's language — addresses the often-invisible burden of trauma and adjustment disorder. Document the family's legal and resettlement status only insofar as it affects access to care, and never let documentation become a barrier to the screen. [3] [2]
The examination is comprehensive and unhurried. Measure and plot weight, height and head circumference on appropriate references, examine the skin, the abdomen for hepatosplenomegaly, the heart for rheumatic or Chagas-related disease, the respiratory system, and the ears, nose and throat. Assess developmental milestones formally in the young child and screen vision and hearing. The well-looking child proceeds to the core laboratory panel; the unwell or febrile child — especially the recently arrived child from a malaria-endemic region — is assessed acutely, with a malaria blood film sent on the same day and the broader screen deferred until the acute question is answered. [7] [11]
Investigations
The core panel is the spine of the screen, and every test on it is there because it finds a silent, treatable condition. For tuberculosis, the choice between an interferon-gamma release assay and a tuberculin skin test is governed by age, BCG status and local guideline: the IGRA is preferred in children two years and over because it is unaffected by BCG vaccination and requires a single visit, while the tuberculin skin test remains useful in young infants and where IGRA is unavailable. A positive test is followed by a chest radiograph and a symptom screen to distinguish latent from active disease. [11] [9]
For the blood-borne viruses, send a fourth-generation HIV antigen-antibody combination assay, a hepatitis B surface antigen with surface antibody and core antibody, and a hepatitis C antibody. Confirm every positive — hepatitis C antibody with a hepatitis C RNA nucleic-acid test, and HIV in the infant under eighteen months with HIV DNA or RNA PCR, because maternal antibody persists and a reactive serology in a young infant reflects exposure rather than infection. A syphilis serology (treponemal with a non-treponemal titre for activity) completes the blood-borne screen, because congenital and acquired syphilis are over-represented in some migrant cohorts. [4] [8]
For the parasitic screen, send stool for ova, cysts and parasites (ideally three samples to lift sensitivity) together with serology for Strongyloides stercoralis and, for children from endemic regions, Schistosoma species. Serology is the more sensitive test for the chronic tissue-dwelling parasites that stool microscopy misses, and a positive serology is treated presumptively. Add a full blood count with an eosinophil count — eosinophilia is a clue to tissue parasites — iron studies, and, for resettled refugee children, a blood-lead level. A malaria blood film is not part of the routine screen of the well afebrile child, but it is non-negotiable in any febrile recently arrived child from a malaria-endemic region. [10] [7]
The principle that governs every investigation is re-verification. A documented overseas vaccination, a pre-adoption serology, or a pre-departure tuberculosis test is a starting point, and the post-arrival panel repeats the tests that matter in your own laboratory. Vaccine immunity is checked serologically for the vaccine-preventable diseases where serology is reliable — hepatitis B, measles, rubella, varicella, and, where appropriate, mumps and tetanus — and the child is vaccinated on the evidence rather than on the record. This is the single behaviour that distinguishes a fellowship-level screen from a paperwork exercise. [4] [2]
Management — Resuscitation
The screen is overwhelmingly a routine and preventive encounter, and true resuscitation is the exception rather than the rule. The child who is acutely unwell on arrival — febrile, in shock, failing to thrive, or with organ-specific compromise — is moved out of the screening pathway and into an acute assessment, with the screen completed once the acute question is answered. The febrile recently arrived child from a malaria-endemic region is the prototypical exception: this child has falciparum malaria until a competent same-day blood film proves otherwise, and the screen is paused while the film and the acute workup proceed. [9] [7]
For the well child, the "resuscitation" phase is the safe set-up of the encounter: a trained interpreter booked, a trauma-informed approach, time allowed for a thorough history and examination, and consent taken for the comprehensive panel. Some children arrive malnourished, with iron-deficiency anaemia or, less commonly, severe acute malnutrition, and these are managed nutritionally alongside the screen rather than held back by it. A child with newly diagnosed HIV, chronic hepatitis B with decompensation, or active tuberculosis is referred immediately to paediatric infectious diseases and the relevant sub-specialty service, and public-health notification is completed where required. [8] [11]
The rare but serious acute presentation is the refugee or adopted child who arrives in, or develops, a vaccine-preventable illness — measles being the most consequential, because it is highly infectious and the under-immunised migrant child is a recognised source of outbreaks. Any child with a febrile rash illness consistent with measles is isolated, notified, and tested, and susceptible contacts are offered post-exposure prophylaxis. The structural lesson is that the immunity gap found at screening is also a public-health risk, which is why catch-up immunisation is part of the screen rather than a downstream task. [4] [8]
Management — Definitive & Stepwise
Definitive management runs in four lanes: confirm and treat the positives, deliver catch-up immunisation on serological evidence, address nutrition and growth, and build the medical home. The confirm-and-treat lane acts on every positive result. Latent tuberculosis is treated with the age-appropriate regimen — for example, three months of rifampicin plus isoniazid, four months of rifampicin, or six to nine months of isoniazid per the national guideline — after active disease has been excluded. Chronic hepatitis C in the child of treatment age is cured with direct-acting antivirals, chronic hepatitis B is assessed and monitored with or without antiviral therapy, HIV is referred for immediate antiretroviral therapy, and strongyloidiasis is treated with ivermectin and schistosomiasis with praziquantel. [11] [10]
The catch-up immunisation lane closes the immunity gap on evidence. After serology, the child without documented and serologically confirmed immunity is vaccinated on an accelerated catch-up schedule that respects minimum ages and intervals, and the child with evidence of immunity is not over-vaccinated. The schedule is built from the national immunisation programme, and the family is given a clear, dated record. Measles-containing vaccine is prioritised in outbreak-prone settings, and hepatitis B vaccine is given to the susceptible child alongside the household-contact assessment, because a hepatitis B surface-antigen-positive child places their unvaccinated household contacts at risk. [4] [8]
The nutrition and growth lane addresses the iron-deficiency anaemia, vitamin deficiencies and faltering growth that are common in migrant children, and re-plots growth on appropriate references over time to distinguish catch-up growth from underlying disease. The medical-home lane integrates mental-health support — many refugee and adopted children carry a burden of trauma, grief and adjustment difficulty that is invisible without a structured screen — dental, vision and hearing care, developmental assessment and school readiness, and an explicit follow-up plan with a named clinician. The screen succeeds when it becomes a relationship, not when it closes a checklist. [9] [2]
Specific Subtypes & Scenarios
The internationally adopted child carries the highest burden of chronic viral hepatitis and intestinal parasites of the three populations, and the pre-adoption record is the least reliable. The Hostetter study and its successors established the high yield of a structured evaluation, and the modern paediatric-clinics reviews by Eckerle and colleagues and by Abu-Shamsieh and Maw translate that evidence into the contemporary panel: tuberculosis by IGRA or tuberculin skin test, hepatitis B surface antigen with core antibody, hepatitis C antibody, HIV, syphilis, stool ova and parasites with Strongyloides serology, and serological vaccine-immunity testing. Growth, development and attachment are assessed in parallel, because the adoption is a developmental as well as an infectious transition. [1] [5]
The newly arrived refugee or asylum-seeking child is the most comprehensively screened group, because many high-income resettlement programmes run an overseas pre-departure examination followed by a domestic post-arrival assessment. The Australasian ASID/RHeANA guidance and the United States CDC domestic examination guidance both treat the overseas record as a starting point and require a full post-arrival re-assessment, and the Enhanced Health Interventions evaluation of the United States refugee programme showed measurable benefit from a structured overseas-and-domestic screening pathway. The refugee child also carries a higher burden of mental-health difficulty, nutritional deficiency and lead exposure, which are screened in parallel with infection. [9] [12]
The immigrant child is often healthy and arrives through family-reunion or skilled-migration pathways, and the screen is selective rather than comprehensive — but it always includes tuberculosis screening, a hepatitis B surface antigen, a vaccination review with serology where indicated, and a region-specific assessment. The visiting-friends-and-relatives family is the subgroup most often missed by routine services, because their children are usually born in the host country and their risk is acquired on return visits to the family's country of origin; the screen is an opportunity to deliver pre-travel advice for the next visit alongside the domestic assessment. [3] [8]
The febrile recently arrived child is the case that bridges this topic with the fever-in-the-returned-traveller framework. A refugee or migrant child who is febrile within weeks to months of arrival from a malaria-endemic region has falciparum malaria until a competent same-day blood film proves otherwise, and the broader screening panel is paused while the acute question is answered. The same child may also present with enteric fever, tuberculosis, or a vaccine-preventable illness acquired in transit, so the acute differential is held wide and the structured screen is completed once the acute illness is managed. [7] [9]
Complications & Pitfalls
The cardinal pitfall is trusting the overseas or pre-adoption record. Every mortality and morbidity review of missed chronic hepatitis B, untreated latent tuberculosis, and fatal Strongyloides hyperinfection in a migrant child returns to the same point: the clinician accepted a documented result at face value and did not re-verify it. The structural defence is to treat every record as a hypothesis, repeat the tests that matter in your own laboratory, and act on the evidence. [1] [4]
The second pitfall is stool-only parasite screening. Stool microscopy for ova, cysts and parasites has a low sensitivity for chronic Strongyloides and Schistosoma carriage, and a single negative stool does not exclude these infections. Serology is the more sensitive test and is now the standard in the Australasian and United Kingdom screening programmes; omitting it is the classic reason a treatable, potentially fatal infection is missed at the screen and presents years later as hyperinfection during immunosuppression. [10] [9]
The third pitfall is misinterpreting the HIV result in the young infant. Maternal antibody persists for up to eighteen months, so a reactive HIV serology in a young infant reflects exposure rather than infection, and the diagnostic test in that age group is an HIV DNA or RNA PCR. Treating a serology-positive infant as infected without PCR confirmation over-diagnoses, while dismissing the result misses the case — the age-appropriate algorithm resolves the ambiguity. [5] [8]
The fourth pitfall is vaccinating on the record rather than on the evidence. A vaccine record may be incomplete, fabricated, or record doses that did not take, and re-vaccinating the already-immune child is unnecessary while failing to vaccinate the non-immune child leaves the gap open. The serological approach — testing for antibody to the vaccine-preventable diseases where serology is reliable and vaccinating on the result — closes the gap correctly. The corollary pitfall is the under-immunised child who acquires measles on a return visit to a family country of origin and sparks an outbreak on return, which is why measles-containing catch-up vaccine is prioritised. [4] [2]
The fifth pitfall is failing to convert the screen into the medical home. A screen that finds the infections but does not deliver the treatment, the catch-up immunisation, the growth and developmental follow-up, and the mental-health support has detected disease without changing the outcome. The fellowship behaviour is to own the follow-up — a named clinician, a dated plan, and a relationship that delivers the comprehensive care the family is entitled to. [9] [8]
Prognosis & Disposition
The prognosis of the migrant child who receives a comprehensive, well-executed screen is excellent, because almost every condition found is treatable today. Latent tuberculosis treated with a short-course regimen prevents the future reactivation; chronic hepatitis C is cured with direct-acting antivirals; HIV is transformed by antiretrovirals into a chronic controlled condition; strongyloidiasis is cured with ivermectin; and the immunity gap is closed by catch-up immunisation. The Danish post-arrival screening data for internationally adopted children and the United States domestic-evaluation data for refugee children both show that the yield is high and the conditions found are manageable when the screen is complete. [6] [12]
The prognosis is determined less by the infections than by the social determinants that surround them. Growth faltering, developmental delay, mental-health difficulty, educational disruption, and the effects of detention or persecution all shape the child's longer-term trajectory, and the medical home is the structure that addresses these alongside the infections. The child whose screen is converted into a continuing relationship does better than the child whose screen is a one-off encounter, however thorough. [9] [8]
Disposition follows from the findings. The well child with a normal or manageable screen is followed in primary care with a dated plan for catch-up immunisation, growth monitoring, developmental assessment and mental-health support. The child with latent tuberculosis, chronic hepatitis B or C, HIV, or significant parasitic infection is co-managed with paediatric infectious diseases and the relevant sub-specialty. The child who is acutely unwell — febrile with possible malaria, or with a vaccine-preventable illness — is admitted or observed as the acute presentation dictates, with the screen completed thereafter. Every family is given a clear, interpreter-mediated summary and a named contact, because the screen is the entry to care, not the end of it. [7] [2]
Special Populations
The refugee and asylum-seeking child is the population most exposed to the social determinants that compound infection — displacement, detention, family separation, food insecurity and interrupted education. The Australasian and international guidance frames the screen as the entry to comprehensive, rights-based care, and the clinician holds a low threshold for mental-health, developmental and nutritional assessment alongside the infection panel. Detention is harmful to children, and the paediatrician's advocacy for community-based resettlement is part of the care, not separate from it. [9] [8]
The internationally adopted child carries the highest pre-test probability of chronic hepatitis B and intestinal parasites, and the adoption itself is a developmental transition that may involve attachment difficulty, growth faltering and developmental delay. The screen is integrated with a developmental and psychosocial assessment, and the family is supported through the adjustment period with clear information, a vaccination plan and a named clinician. The pre-adoption record is the least reliable of the three populations, so re-verification is at its most important here. [1] [5]
The unaccompanied or separated minor is a special case within the refugee population, because the young person arrives without a parent or guardian and may have experienced trafficking, exploitation or significant trauma. Consent and confidentiality are handled with particular care, the mental-health screen is prioritised, and the infectious screen is delivered alongside safeguarding and legal-status assessment. The young person's autonomy and dignity are respected throughout, and the screen is the entry to a service that continues beyond the medical encounter. [8] [7]
The immunocompromised child within a migrant family — for example, a child with HIV found at screen, or a child about to begin immunosuppressive therapy — converts several moderate risks into urgent ones. Strongyloides serology is non-negotiable before any corticosteroid or immunosuppression, because hyperinfection is fatal; latent TB treatment is expedited; and live vaccines are withheld or timed around the immunosuppression. The visiting-friends-and-relatives family and the rural or remote migrant family face access barriers to follow-up, so the screen is planned with the follow-up pathway built in from the start. [10] [11]
Evidence, Guidelines & Regional Differences
The evidence base rests on three pillars. The first is the landmark evaluation studies, beginning with the Hostetter study of the medical evaluation of internationally adopted children in the New England Journal of Medicine in 1991, which established the high yield of a structured evaluation, and the Miller review of caring for internationally adopted children in the same journal. The Stauffer, Kamat and Walker review unified the screening of immigrants, refugees and adoptees into a single framework, and the modern paediatric-clinics reviews by Barnett, Eckerle and colleagues, and Abu-Shamsieh and Maw update the panel and the evidence to the current era. [1] [8]
The second pillar is the cohort yield data, which quantifies the probability of each finding. The Nielsen study of infectious diseases detected by post-arrival screening of internationally adopted children in Denmark, the Shetty review of infectious diseases among refugee children, and the United States domestic-evaluation data on latent tuberculosis in immigrant and refugee children give the clinician a data-driven prior for the child in front of them. The Cinardo review of screening for neglected tropical diseases in refugee and asylum-seeker populations in the United Kingdom grounds the parasitic screen, and the Mitchell evaluation of enhanced health interventions for United States-bound refugees grounds the overseas-and-domestic pathway. [6] [12]
The third pillar is the guideline framework, which translates the evidence into practice. The Australasian Society for Infectious Diseases and Refugee Health Network of Australia recommendations — the ASID/RHeANA guidance, published in the Medical Journal of Australia — is the primary framework for the ANZ region and frames screening as a comprehensive, voluntary, post-arrival assessment for people of refugee-like background. The United States CDC domestic examination guidance and the AAP Red Book provide the parallel North American framework, and the national immunisation programmes translate the catch-up schedules. [9] [8]
Regional differences are real and decisional. In Australia and New Zealand, the ASID/RHeANA guidance shapes the post-arrival screen and is integrated with the national immunisation programme and the refugee-health network; in the United States, the CDC domestic examination follows an overseas pre-departure examination under the resettlement programme; in the United Kingdom and Europe, the post-arrival screen is shaped by the national health-service guidance and the neglected-tropical-disease screening reviews. The IGRA-versus-tuberculin-skin-test choice, the use of Strongyloides serology, and the blood-lead screening policy all vary by region, and the clinician applies the local framework while holding the universal principle: re-verify every record, screen for the must-not-miss five, and convert the screen into the medical home. [9] [10]
Exam Pearls
The post-arrival infection screen is an examination favourite because it rewards structured reasoning and equity-minded practice over factual recall. The single highest-yield behaviour is re-verification: never trust the overseas, pre-adoption or pre-departure record, repeat every serology in your own laboratory, and check vaccine immunity before re-vaccinating. [4] [8]
The must-not-miss five are tuberculosis (latent, by IGRA or tuberculin skin test, treated to prevent reactivation), hepatitis B (surface-antigen positive, assessed for chronicity and co-infection), hepatitis C (antibody positive with confirmed viraemia, curable with direct-acting antivirals), HIV (confirmed with the age-appropriate algorithm — PCR in the infant under eighteen months), and Strongyloides (serology positive, treated with ivermectin to prevent fatal future hyperinfection). For the orals and the long case, be ready to defend the IGRA-versus-skin-test choice, the stool-versus-serology choice for parasites, and the catch-up immunisation built on serological evidence. [9] [10]
The single most testable pitfall is stool-only parasite screening: a single negative stool does not exclude Strongyloides or Schistosoma, and serology is the standard because chronic carriage carries the risk of fatal hyperinfection during later immunosuppression. The febrile recently arrived child from a malaria-endemic region has falciparum malaria until a competent same-day blood film proves otherwise — the screen is paused, the film is sent, and the broader panel follows. And always use a trained interpreter, never a child, because the consent, the history and the trust all depend on accurate communication. [7] [11]
For the communication station, be ready to explain a positive hepatitis B or HIV result to a family through an interpreter, hold the safety net for the child discharged after a normal screen, and frame screening as the entry to a medical home rather than a surveillance exercise. The reward structure of the topic is that almost everything you find is treatable today, and the fellowship behaviour is to own the follow-up — a named clinician, a dated plan, and a relationship that delivers comprehensive, equitable, trauma-informed care to the migrant child and their family. [2] [9]
References
- [1]Hostetter MK; Iverson S; Thomas W; et al Medical evaluation of internationally adopted children. N Engl J Med, 1991.PMID 1649404
- [2]Miller LC Caring for internationally adopted children. N Engl J Med, 1999.PMID 10559456
- [3]Stauffer WM; Kamat D; Walker PF Screening of international immigrants, refugees, and adoptees. Prim Care, 2002.PMID 12687898
- [4]Barnett ED Immunizations and infectious disease screening for internationally adopted children. Pediatr Clin North Am, 2005.PMID 16154464
- [5]Eckerle JK; Howard CR; John CC Infections in internationally adopted children. Pediatr Clin North Am, 2013.PMID 23481113
- [6]Nielsen AV; Kjaergaard J; Pedersen TM; et al Infectious diseases detected by screening after arrival to Denmark in internationally adopted children. Acta Paediatr, 2020.PMID 31580515
- [7]Shetty AK Infectious Diseases among Refugee Children. Children (Basel), 2019.PMID 31783605
- [8]Abu-Shamsieh A; Maw S Pediatric Care for Immigrant, Refugee, and Internationally Adopted Children. Pediatr Clin North Am, 2022.PMID 34794672
- [9]Chaves NJ; Paxton GA; Biggs BA; et al The Australasian Society for Infectious Diseases and Refugee Health Network of Australia recommendations for health assessment for people from refugee-like backgrounds: an abridged outline. Med J Aust, 2017.PMID 28403765
- [10]Cinardo P; Farrant O; Gunn K; et al Screening for neglected tropical diseases and other infections in refugee and asylum-seeker populations in the United Kingdom. Ther Adv Infect Dis, 2022.PMID 35958977
- [11]Wang Z; Posey DL; Brostrom RJ; et al US Postarrival Evaluation of Immigrant and Refugee Children with Latent Tuberculosis Infection Diagnosed Overseas, 2007-2019. J Pediatr, 2022.PMID 35120982
- [12]Mitchell T; Lee D; Weinberg M; et al Impact of Enhanced Health Interventions for United States-Bound Refugees: Evaluating Best Practices in Migration Health. Am J Trop Med Hyg, 2018.PMID 29260657