Paeds · infectious-diseases
Malaria in children
Also known as Falciparum malaria · Cerebral malaria · Severe malaria · Plasmodium falciparum infection · Imported malaria
Fellowship guide to malaria in children: Plasmodium species and severe falciparum disease, the cyclical fever and pathophysiology of cytoadherence and sequestration, the time-critical recognition of severe malaria in a returning traveller, blood film and rapid diagnostic test interpretation, intravenous artesunate for severe disease with fluid and transfusion support, artemisinin-combination therapy for uncomplicated infection, post-artesunate haemolysis, and the RTS,S vaccine.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Malaria is a mosquito-borne parasitic illness caused by Plasmodium protozoa and transmitted by the bite of an infected female Anopheles mosquito. In children it ranges from a self-limiting febrile illness to a rapidly fatal multisystem disease, and the difference between the two is the single most important judgement a clinician makes. Any febrile child who has been in a malaria-endemic area must be presumed to have malaria until the blood film proves otherwise. [1]
The parasite that dominates severe disease and death is Plasmodium falciparum, which kills through cytoadherence and sequestration of infected red cells in the microvasculature of the brain and other organs. The other species, vivax, ovale, malariae, and the zoonotic knowlesi, cause significant illness but are rarely as lethal, and vivax and ovale carry the added burden of relapse from dormant liver stages called hypnozoites. Recognising the species and the severity drives every treatment decision. [1]
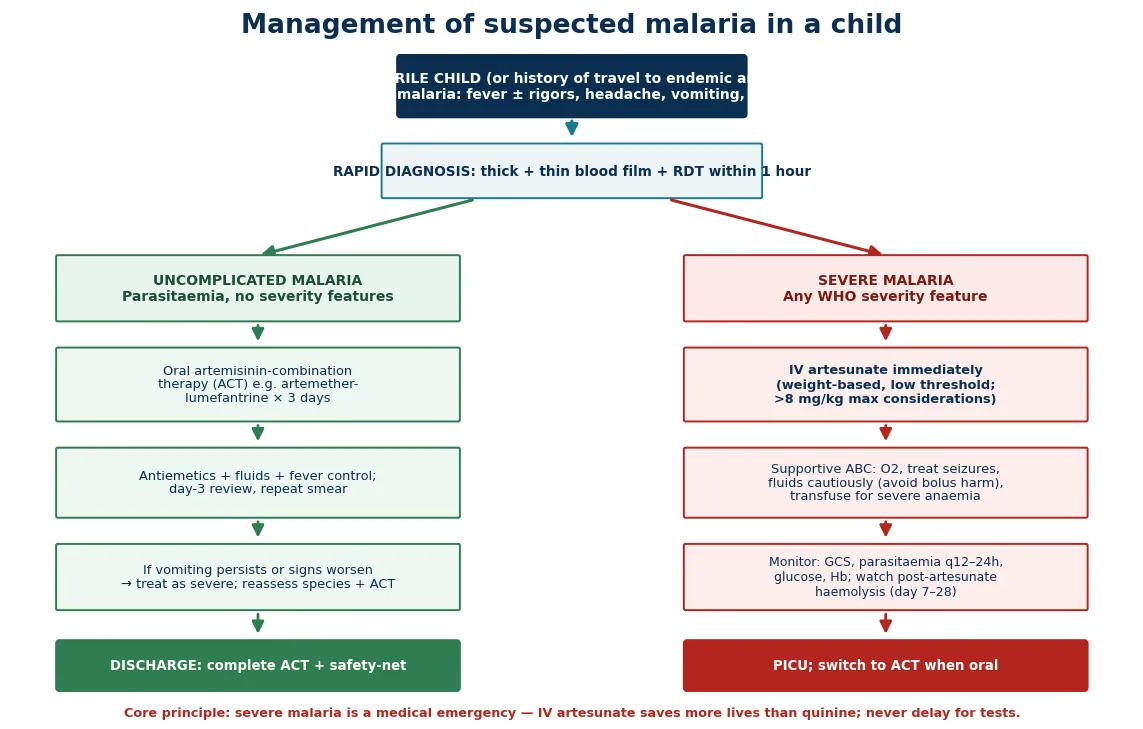
The cardinal principle is speed. Severe falciparum malaria is a medical emergency in which every hour of delay in giving intravenous artesunate measurably increases mortality, so blood films and rapid tests must never postpone the first dose in a sick child. In Australia and New Zealand malaria is almost always imported through travel, which makes a travel history the hinge of the whole encounter. [2]
Classification
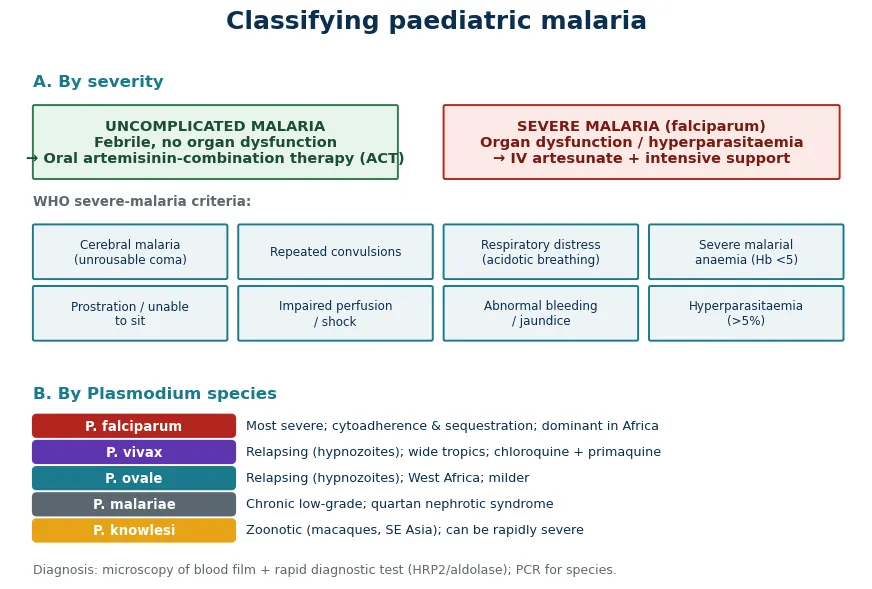
The clinical classification that changes management is the split between uncomplicated and severe malaria. A child with fever and parasitaemia but no organ dysfunction has uncomplicated disease and is treated with oral therapy. A child with any World Health Organization severity feature, whether cerebral malaria with impaired consciousness, repeated convulsions, respiratory distress, severe anaemia, prostration, shock, abnormal bleeding, jaundice, or a high parasitaemia, has severe disease and needs intravenous artesunate and intensive support. [1]
The species classification refines prognosis and treatment. Falciparum causes the great majority of severe cases through cytoadherence and sequestration. Vivax and ovale produce dormant liver hypnozoites that relapse weeks to years later, so they need an additional radical-cure drug. Malariae runs a chronic low-grade course linked to the nephrotic syndrome, and knowlesi, acquired from macaque monkeys in Southeast Asia, can multiply rapidly and behave like falciparum. [1]
[1] [1]Epidemiology & Risk Factors
Malaria remains one of the largest killers of children in the world, with the heaviest burden in sub-Saharan Africa. Insecticide-treated nets, indoor residual spraying, and artemisinin-combination therapy have roughly halved the clinical burden over fifteen years, yet hundreds of thousands of African children under five still die of falciparum malaria each year. Young children in endemic areas carry most of the mortality because they have not yet acquired the partial immunity that comes with repeated exposure. [5]
In the highest-burden regions, the prevalence of falciparum infection in children aged two to ten fell by about half between 2000 and 2015 as control measures scaled up, and the estimated rate of clinical cases fell in parallel. Even so, transmission persists across the tropics, and the disease remains common wherever the Anopheles vector and the parasite coexist. The gains are fragile and can reverse if control efforts slacken or if drug resistance spreads. [5]
The dominant risk factor for severe disease in any setting is a lack of immunity, which is precisely the situation of the non-immune traveller or the young infant in an endemic area. Children born to non-immune parents, migrants and refugees returning from visits to their country of origin, and unimmunised or unprotected travellers all carry high risk. Pregnancy, asplenia, and immunosuppression amplify susceptibility and severity, and glucose-6-phosphate dehydrogenase deficiency shapes the choice of radical cure because primaquine can cause haemolysis. [1]
Pathophysiology
The life cycle of the malaria parasite begins when an infected female Anopheles mosquito injects sporozoites during a blood meal. Sporozoites travel to the liver and invade hepatocytes, where they multiply silently over one to two weeks before releasing merozoites into the bloodstream. In vivax and ovale infection, some parasites remain dormant in the liver as hypnozoites and cause relapses long after the first illness. [1]
Merozoites infect red blood cells and begin the erythrocytic cycle, maturing from ring forms to trophozoites and then to schizonts, which rupture the red cell and release a fresh wave of merozoites. This synchronous rupture of red cells drives the cyclical fever that characterises malaria, though the pattern is often blurred in children. Some parasites differentiate into gametocytes, which infect a new mosquito and sustain transmission. [1]
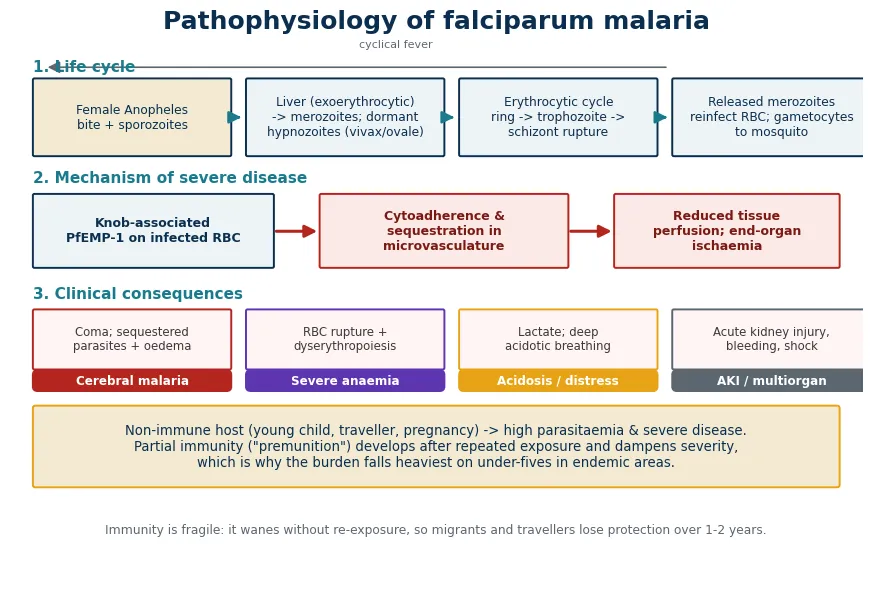
The distinguishing and lethal feature of falciparum is cytoadherence. Infected red cells display parasite proteins, chiefly PfEMP-1, on knob-like protrusions that stick them to the lining of small blood vessels. The sequestered parasites obstruct blood flow, escape clearance by the spleen, and provoke local inflammation and endothelial dysfunction. The result is microvascular obstruction in the brain, gut, kidney, and placenta, which underlies cerebral malaria, acidosis, renal failure, and the other features of severe disease. [6]
The consequences of this microvascular obstruction drive both the clinical syndrome and the complications. In the brain, sequestered parasites and surrounding oedema produce the impaired consciousness and seizures of cerebral malaria. Mass rupture of red cells, alongside impaired red cell production, produces severe malarial anaemia. Tissue hypoperfusion generates lactate and the deep sighing acidotic breathing that is a marker of a high mortality risk. [6]
Clinical Presentation
The classical presentation of malaria is fever, often with rigors or chills, headache, and vomiting, but in children the picture is frequently non-specific. Fever may be continuous rather than the textbook tertian or quartan pattern, and infants may show only irritability, poor feeding, lethargy, or refusing to drink. Pallor, jaundice, and splenomegaly are useful signs when present, and thrombocytopenia is so consistent that a normal platelet count should prompt doubt about the diagnosis. [1]
The features that mark severe disease, and that must be actively sought, are the World Health Organization severity criteria. These include impaired consciousness, prostration with inability to sit or drink, repeated convulsions, deep sighing acidotic breathing, severe pallor, haemoglobinuria with dark urine, spontaneous bleeding, shock, and jaundice. Any one of these in a parasitaemic child converts the diagnosis to severe malaria and dictates intravenous artesunate. [1]
Cerebral malaria specifically presents as impaired consciousness that can progress to unrousable coma, with or without seizures. In a young child, assess the conscious level with the Blantyre coma scale rather than the Glasgow scale. Deep breathing, a weak pulse, cold peripheries, and delayed capillary refill signal shock or acidosis, and dark red or black urine points to massive haemolysis. A child who is prostrate, unable to localise pain, or breathing deeply is a child who needs artesunate now. [6]
Severity features to seek at the bedside
Impaired consciousness or Blantyre coma scale below three
Repeated or prolonged convulsions
Deep sighing acidotic breathing or respiratory distress
Severe pallor or haemoglobinuria (dark urine)
Prostration: unable to sit, stand, or drink
Shock, abnormal bleeding, or jaundice
Parasitaemia above two per cent in a non-immune child
Differential Diagnosis
The differential diagnosis of fever in a returning traveller is broad, and malaria sits at its centre because it is the most rapidly fatal. The other travel-related infections to consider are typhoid, dengue and other arboviruses, rickettsial infection, leptospirosis, schistosomiasis, and viral haemorrhagic fevers. Non-travel causes such as pneumonia, urinary tract infection, meningitis, and sepsis remain common and can coexist with malaria. [1]
Several conditions mimic the complications of severe malaria and must be distinguished. A haemolytic crisis from glucose-6-phosphate dehydrogenase deficiency, sickle cell disease, or an autoimmune haemolysis can reproduce the anaemia and jaundice of malaria. Encephalitis, meningitis, and febrile convulsions mimic the cerebral presentation, and septic shock can mimic the cardiovascular compromise of severe disease. Bacterial co-infection is common in severe malaria and may itself be the cause of shock or deterioration. [1]
The recurring error is to anchor on a viral illness or a benign diagnosis such as gastroenteritis in a febrile child with a travel history, and to omit the blood film. Any child with fever and relevant travel who deteriorates, who develops altered consciousness, or who fails to improve must be reassessed for malaria and for bacterial co-infection, because the cost of a missed diagnosis is high and the test is cheap and fast. [2]
Clinical & Bedside Assessment
Begin every assessment with an overall judgement of how sick the child is, using the paediatric assessment triangle of appearance, work of breathing, and circulation. A child who is drowsy, breathing deeply, or poorly perfused needs immediate resuscitation and the blood film organised in parallel. Measure temperature, heart rate, respiratory rate, blood pressure, capillary refill, and oxygen saturation, and check a fingerprick or point-of-care glucose immediately because hypoglycaemia is common and treatable. [2]
Take a focused exposure history while the team works. Ask exactly where the child has travelled or lived, whether overnight or rural stays occurred, the dates of travel relative to symptom onset, whether chemoprophylaxis was taken and how reliably, and whether insecticide-treated nets were used. Malaria can present months after exposure, particularly vivax, so a travel history within the preceding three months, and longer for relapsing species, must be elicited. [1]
Perform a full examination looking specifically for the severity features. Assess the conscious level with the Blantyre coma scale in pre-verbal children or the Glasgow coma scale in older children, look for neck stiffness to exclude meningitis, and examine for pallor, jaundice, and the size of the spleen and liver. Count the respiratory rate and characterise the breathing, because deep sighing respirations signal metabolic acidosis, and look for bleeding and petechiae. A rapid, focused examination that finds any severity feature sets the whole management pathway in motion. [1]
Investigations
The definitive investigation is the blood film, and it must be requested the moment malaria is suspected. A thick film concentrates parasites and is the most sensitive test, while a thin film allows species identification and parasite density counting. A single negative film does not exclude malaria, particularly in partially treated or non-immune children, so repeat films every twelve to twenty-four hours for two to three samples if suspicion persists. [1]
Rapid diagnostic tests detect parasite antigens and give a result in minutes. The histidine-rich protein 2 test is highly sensitive for falciparum and is the cornerstone of point-of-care diagnosis, while lactate dehydrogenase or aldolase tests detect non-falciparum species. A rapid test does not quantify parasitaemia, so a blood film is still needed for species confirmation and density once the diagnosis is made. [1]
Send baseline bloods alongside the film. A full blood count typically shows anaemia and thrombocytopenia, and a blood gas, lactate, glucose, urea, creatinine, electrolytes, and bilirubin define the severity of organ involvement. A blood culture is warranted in any sick child because bacterial co-infection is common in severe malaria. Polymerase chain reaction is the most sensitive and specific test and is useful for species confirmation and for detecting mixed infections, though it is not used for acute decisions. [1]
Management — Resuscitation
A child with severe malaria needs immediate resuscitation using an airway, breathing, circulation approach. Secure the airway and give high-flow oxygen for hypoxia, respiratory distress, or a falling conscious level, and establish intravenous or intraosseous access within minutes rather than prolonging the hunt for a peripheral line. Check and treat hypoglycaemia at once, because sick children with falciparum malaria are prone to low blood glucose and the empirical bolus is safer than missing it. [2]
Fluid management in severe malaria is deliberately cautious. Large boluses of isotonic crystalloid were shown in the FEAST trial to increase mortality in African children with severe febrile illness and impaired perfusion, including malaria, so resuscitation relies on small, reassessed boluses only for clear shock, and on maintenance fluids to keep the child euvolaemic. Avoid hypotonic fluids, watch for pulmonary oedema, and transfuse packed red cells for severe malarial anaemia. [4]
Resuscitation sequence for severe malaria
Assess airway, breathing, circulation and give high-flow oxygen
Establish intravenous or intraosseous access within minutes
Check fingerprick glucose and treat hypoglycaemia
Take blood film, rapid diagnostic test, cultures, and baseline bloods
Give intravenous artesunate immediately for any severity feature
Give small reassessed fluid boluses only for clear shock, avoid large boluses
The single most important drug intervention is intravenous artesunate, given the moment a severity feature is recognised and before the parasite density is known. Artesunate is faster to act than quinine, clears parasites more quickly, and has fewer side effects, and the large randomised trials in both Asian adults and African children showed a substantial survival advantage. Convulsions are treated with benzodiazepines, and severe anaemia with transfusion, while the team prepares for paediatric intensive care. [2]
Management — Definitive & Stepwise
Severe malaria is treated with intravenous artesunate at 2.4 mg per kilogram given intravenously at diagnosis and then at 12 and 24 hours, followed by a dose once daily until the child can swallow. Each dose is given as a slow intravenous injection over minutes, and treatment continues until oral therapy is tolerated, at which point a full oral artemisinin-combination therapy course completes the regimen. Intramuscular artesunate is used when intravenous access is impossible or during retrieval. [2]
The evidence for artesunate over quinine is among the strongest in tropical medicine. The SEAQUAMAT trial in severe Asian malaria and the AQUAMAT trial in African children both showed that artesunate reduced mortality by about a quarter relative to quinine, with the benefit clearest in the youngest and sickest children. Quinine is now reserved for genuine artesunate shortage, and even then it requires a loading dose and careful cardiac and glucose monitoring. [3]
AQUAMAT: artesunate vs quinine in African children
Population: 5,425 African children under 15 years with severe falciparum malaria
Key finding
Intravenous artesunate reduced mortality by 22 per cent compared with quinine in African children with severe falciparum malaria, with a relative risk of death of 0.78 and a number needed to treat of about 41.
Uncomplicated falciparum malaria is treated with an oral artemisinin-combination therapy for three days. Artemether-lumefantrine is the most widely used regimen and is taken over three days, with the option of dihydroartemisinin-piperaquine or artesunate-amodiaquine where local resistance patterns allow. The child is reviewed on day three for clinical response and a repeat smear to confirm falling parasitaemia, and treatment failure prompts a switch to a second-line combination. [1]
For vivax and ovale malaria, treat the blood stage with chloroquine where the parasite is sensitive, or with an artemisinin-combination therapy in chloroquine-resistant regions, and add a radical cure with primaquine to eradicate liver hypnozoites and prevent relapse. Check glucose-6-phosphate dehydrogenase status before giving primaquine, because deficient children risk severe haemolysis, and tafenoquine offers a single-dose alternative in suitable patients. Knowlesi and chloroquine-resistant species are managed as for falciparum with an artemisinin-combination therapy. [1]
Antimalarial by disease severity and species
Specific Subtypes & Scenarios
Cerebral malaria is the archetype of severe disease and the scenario examiners test most relentlessly. It presents as impaired consciousness progressing to coma, often with seizures and abnormal posturing, in a child with falciparum parasitaemia. The management is intravenous artesunate, airway protection, seizure control, careful fluids, and correction of hypoglycaemia, with paediatric intensive care for ventilation if the coma deepens. Even with optimal treatment, cerebral malaria kills around one in ten children and leaves many survivors with neurological sequelae. [6]
Severe malarial anaemia presents with profound pallor, dyspnoea, and heart failure in a child with high parasitaemia, and it results from the rupture of infected red cells combined with impaired production of new red cells. Transfusion of packed red cells is the life-saving intervention, guided by the severity of anaemia and the presence of respiratory distress or cardiac compromise, and it is given alongside artesunate. Recovery of haemoglobin takes weeks, and folate supplementation supports marrow recovery. [7]
Vivax malaria carries the particular problem of relapse. The blood-stage illness responds to chloroquine or an artemisinin-combination therapy, but dormant liver hypnozoites re-emerge weeks to months later and cause repeated febrile episodes unless primaquine is given. Children returning from Papua New Guinea or South Asia often relapse, so a documented vivax infection must be followed by a radical cure after glucose-6-phosphate dehydrogenase testing. [1]
Knowlesi malaria, acquired from macaque monkeys in the forests of Southeast Asia, can behave like falciparum with high parasitaemia and rapid deterioration. A child returning from Malaysia or nearby regions with a blood film showing parasites that look like malariae but with a high density should be treated as having knowlesi and managed with an artemisinin-combination therapy, escalating to intravenous artesunate if severity features appear. [11]
Artesunate
Dose
2.4 mg/kg IV at 0, 12 and 24 hours, then once daily
Complications & Pitfalls
The mortality of treated cerebral malaria is around ten to twenty per cent, and survivors carry a substantial burden of neurological sequelae including epilepsy, motor deficits, cognitive impairment, behavioural problems, and blindness or deafness. Severe malarial anaemia also carries significant mortality, particularly in young children with co-existing malnutrition or bacterial infection. These outcomes drive the emphasis on early artesunate and on intensive support. [6]
A distinctive and often-missed complication is post-artesunate delayed haemolysis, which occurs in non-immune travellers and children treated with intravenous artesunate. Between one and four weeks after treatment, a previously recovering child develops falling haemoglobin with haemolysis, sometimes requiring transfusion. Every child given intravenous artesunate needs follow-up blood counts in the weeks after discharge so that this delayed complication is caught rather than missed. [8]
Acute complications also include hypoglycaemia, pulmonary oedema and the acute respiratory distress syndrome, acute kidney injury, blackwater fever with massive haemolysis, disseminated intravascular coagulation, and bacterial co-infection or septicaemia. The major clinical pitfalls are failing to take a travel history, accepting a single negative film, delaying artesunate while awaiting results, giving large fluid boluses, and forgetting to arrange follow-up for post-artesunate haemolysis. [1]
Prognosis & Disposition
The two determinants of outcome are the speed of starting artesunate and the severity at presentation. Children treated promptly for uncomplicated malaria recover fully within days and have an excellent prognosis, while those who present with deep coma, respiratory distress, or very high parasitaemia face the highest mortality. Falciparum carries the worst prognosis of the species, and non-immune children and infants fare worse than semi-immune older children in endemic areas. [2]
After cerebral malaria, survivors need structured developmental and neurological follow-up because epilepsy, cognitive impairment, and motor deficits may emerge over months. Hearing and vision should be checked, and children with identified deficits referred for early intervention and rehabilitation. The family needs honest counselling about prognosis and a clear plan for surveillance, because the consequences of an unrecognised late seizure or developmental regression are significant. [6]
Disposition requires that the child is clinically stable, afebrile, tolerating oral therapy, and showing a falling parasitaemia on repeat smears. Every child treated for severe malaria needs follow-up to monitor haemoglobin in light of the risk of post-artesunate haemolysis, and families receive a written safety-net explaining warning signs and when to re-present. Public health notification of the case is routine, and any co-travellers with fever should be assessed. [8]
Special Populations
Non-immune travellers and the children of migrants returning to visit family in endemic areas are the classic ANZ paediatric malaria patients. Their lack of partial immunity means a given parasitaemia carries a higher risk of severe disease than in a child living in an endemic area, so a lower threshold for intravenous artesunate applies. Adherence to chemoprophylaxis is often incomplete in travellers, and a careful prophylaxis history is part of every assessment. [1]
Infants and young children carry the highest mortality from severe malaria in endemic areas because they have not yet acquired immunity, and they present with non-specific signs that are easy to dismiss. Pregnancy adds risk for both mother and fetus, with a higher parasite density, more severe anaemia, and the possibility of congenital or perinatal malaria in the newborn of a parasitaemic mother. Asplenic and immunocompromised children are at risk of overwhelming infection with any of the species. [1]
In Indigenous and remote communities, particularly those near the Torres Strait and in regions with travel links to Papua New Guinea, access to blood films and to intravenous artesunate can be delayed by distance, which makes clear retrieval pathways and culturally safe, well-explained care essential. Migrant and refugee families may have incomplete prophylaxis, language barriers, and exposure to organisms uncommon in the host country. In all these groups, the key is to assume malaria in any febrile child with relevant exposure and to treat early. [1]
[9]Evidence, Guidelines & Regional Differences
The World Health Organization guidelines for malaria establish intravenous artesunate as the first-line treatment of severe falciparum malaria in children and adults, and oral artemisinin-combination therapy as the treatment of uncomplicated disease. These recommendations rest on the SEAQUAMAT and AQUAMAT trials, which together showed that artesunate reduces mortality by about a quarter relative to quinine, and on a large body of observational evidence on diagnostics and supportive care. [3]
The FEAST trial reshaped fluid management in severe malaria. It showed that bolus fluid resuscitation increased mortality in African children with severe febrile illness and impaired perfusion, many of whom had malaria, and it ended the routine use of large saline boluses in these children. Current practice is to give fluids cautiously, using small reassessed boluses only for clear shock and maintenance fluids to maintain euvolaemia. [4]
[4]Two live controversies shape contemporary practice. The first is emerging artemisinin resistance, first recognised in the Greater Mekong subregion and now characterised by slow parasite clearance and specific genetic markers, which threatens the efficacy of artemisinin-combination therapy and drives surveillance and regimen adaptation. The second is the rollout of the RTS,S malaria vaccine, which provides partial protection against falciparum in children in moderate-to-high transmission areas and adds a new tool to existing control measures. [12]
Exam Pearls
Severe malaria severity features
References
- [1]White NJ Malaria. Lancet, 2014.PMID 23953767
- [2]Dondorp AM Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, randomised trial. Lancet, 2010.PMID 21062666
- [3]Dondorp A Artesunate versus quinine for treatment of severe falciparum malaria: a randomised trial. Lancet, 2005.PMID 16125588
- [4]Maitland K Mortality after fluid bolus in African children with severe infection. N Engl J Med, 2011.PMID 21615299
- [5]Bhatt S The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature, 2015.PMID 26375008
- [6]Newton CR Pathophysiology of fatal falciparum malaria in African children. Am J Trop Med Hyg, 1998.PMID 9598460
- [7]Calis JC Severe anemia in Malawian children. Malawi Med J, 2016.PMID 27895843
- [8]Jaita S Post-Artesunate Delayed Hemolysis: A Review of Current Evidence. Trop Med Infect Dis, 2023.PMID 36668956
- [9]Syed YY RTS,S/AS01 malaria vaccine (Mosquirix): a profile of its use. Drugs Ther Perspect, 2022.PMID 36093265
- [10]Guerra Mendoza Y Safety profile of the RTS,S/AS01 malaria vaccine in infants and children: additional data from a phase III randomized controlled trial in sub-Saharan Africa. Hum Vaccin Immunother, 2019.PMID 31012786
- [11]Barber BE Plasmodium knowlesi malaria in children. Emerg Infect Dis, 2011.PMID 21529389
- [12]Nayak S Population genomics and transcriptomics of Plasmodium falciparum in Cambodia and Vietnam uncover key components of the artemisinin resistance genetic background. Nat Commun, 2024.PMID 39639029